
Abstract
Recent World Mental Health Survey data suggested that only 1% of adults in China suffered from ADHD (Fayyad et al., 2017), contrasting sharply with the global adult ADHD prevalence figure of 4.4% (Fayyad et al., 2007). In fact, reported prevalence figures of ADHD in Chinese children were substantially higher in the range of 4% to 6% (Zheng & Zheng, 2015), while a school-based study in Hong Kong reported 8.9% of the Chinese schoolboys to suffer from the condition (Leung et al., 1996). These findings may suggest ADHD in Chinese communities to have lower adulthood persistence or have better adulthood outcomes. As such, ADHD in the Chinese may appear to be a less serious condition than that known in the West, possibly consistent with the fact that common comorbidities of adult ADHD, such as depression, alcoholism, and other substance use are also less common in Chinese than Western people (Lee et al., 2009; Shen et al., 2006). Given the high adulthood persistence rate (60%-70%) of ADHD found in Western clinical prospective studies (Biederman et al., 2006; Biederman et al., 2012), examination of the apparent discrepancy in Chinese versus Western adulthood outcomes of clinical cohorts of childhood ADHD may shed light on the etiology and cross-cultural validity of adult ADHD.
Before we accept the above possibility that adult ADHD is a somewhat Western “culture-bound” pathology, several issues deserve attention. First, there has been no published Chinese longitudinal data on adulthood ADHD persistence in clinical or population samples. Second, mental disorders such as depression and substance use have become increasingly common in Chinese communities (Huang et al., 2016). Third, owing to limited treatment resources, under-treatment of children with ADHD in Chinese communities is common (Fayyad et al., 2017; Zheng & Zheng, 2015). This should increase rather than diminish adult persistence. These considerations suggest that the prevalence of adult ADHD in China could have been underestimated. In the West, adult ADHD leads to significant occupational and social role impairment, criminal behavior (Barkley, Fischer, Smallish, & Fletcher, 2006; Biederman et al., 1996; Kessler et al., 2006; Klein, 1991; Mannuzza, Klein, Bessler, Malloy, & LaPadula, 1998), as well as psychiatric comorbidity (Biederman et al., 2012). If 4.4% of the 1.4 billion Chinese population had adult ADHD as in the West, over 50 million adults in China could be suffering from ADHD but have yet to receive proper treatment.
To examine the persistence of childhood-diagnosed ADHD in a Hong Kong Chinese clinical sample, we comprehensively recruited and systematically assessed a sample of children aged 6 to 12 who were clinically diagnosed with ADHD in 2002-2005 in four major children’s mental health services in Hong Kong to examine their current early-adulthood clinical symptomatology and diagnostic subtypes including inattention and hyperactivity/impulsivity, and the impact of adulthood persistence of ADHD on psychiatric comorbidity, functional impairment and social outcomes.
Method
Procedures
Recruitment began after ethical approval from the Clinical Research Ethics Committee of the Hong Kong New Territories East cluster, Hong Kong West cluster, and Kowloon West cluster hospitals. After initial record search for diagnostic compatibility, addresses and/or telephone numbers of the included patients were retrieved with the following methods:
i. Directly from case records
ii. Two parallel computer databases of the Hong Kong Hospital Authority, which is the only public hospital service provider in Hong Kong. The databases allow access to address and telephone numbers of the patient or next-of-kin as of the patient’s latest public hospital attendance across the territory in Hong Kong. All participants were then contacted by phone at least 5 times with each phone number availed, at different times of the day/week. Text messages were sent to those who did not respond to the phone calls, failing which letters were sent to most updated addresses available from computer records. To compare respondent and nonrespondent characteristics, an electronic Chinese version of the Adult ADHD Self-Report Scale (ASRS; Yeh, Gau, Kessler, & Wu, 2008) for self-rating of current ADHD symptom severity was given to all respondents as well as those who either declined the interview or were unavailable for research interview, but agreed to complete the electronic screening.
Participants
We consecutively identified all clinic attendances of 6- to 12-year-old (Klein et al., 2012) Chinese children in years 2002 to 2003 to four tertiary-referral Child and Adolescent’s Mental Health Centers in Hong Kong who had at least reached the age of 18 by the date of recruitment (up to November 2017) (see Figure 1). Five hundred sixty patient records had clinical diagnosis entered on the registry of Diagnostic and Statistical Manual of Mental Disorders (DSM)-ADHD or International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) Hyperkinetic Disorder at baseline and further evidenced by case records showing (a) diagnosis made by a specialist child psychiatrist, (b) inattention or hyperactivity reported by both parents and teachers (Adler & Spencer, 2004), and (c) evidence of functional impairment, for example, underachievement, behavioral problems, and disciplinary consequences. We excluded those who did not have any Chinese parents (n = 3), those whose hospital record showed evidence of mental retardation (n = 29), childhood autism requiring special school placement (n = 23), major sensorimotor handicap (paralysis, deafness or blindness; n = 2), and those who were adopted children as their developmental history may be incomplete (n = 0) (Biederman et al., 2006; Biederman et al., 2012; Klein et al., 2012). Finally, those who were able to make valid informed written consent were recruited for follow-up assessment (n = 499).
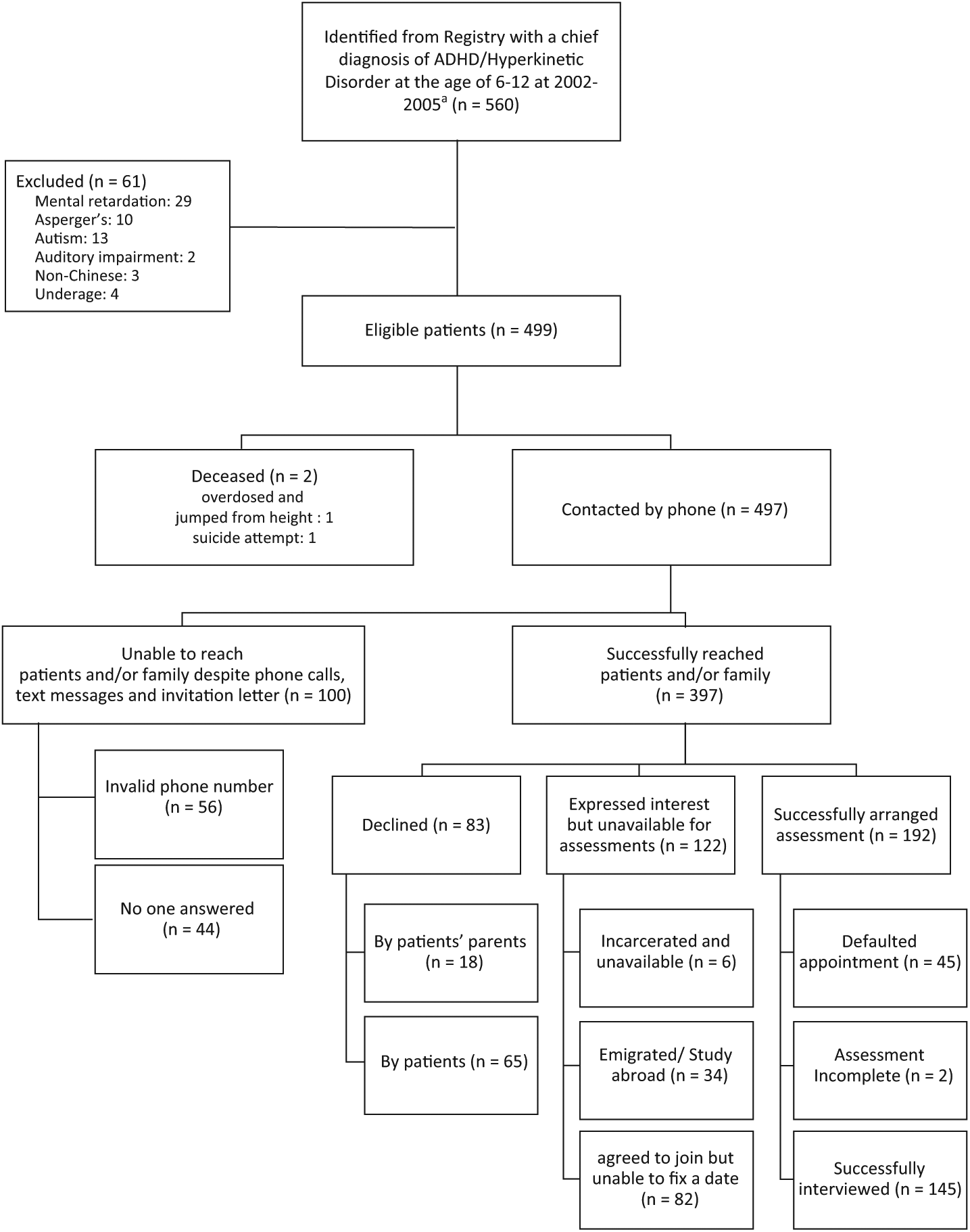
Recruitment flowchart.
Successful phone contact was made with 397 patients or their parents. Eighty-three declined (16.6%), of which 18 were by the parents who refused for investigators to contact the patients for further recruitment procedures. Three hundred fourteen (62.9%) expressed interest to participate in the study. We were unable to schedule research interviews for 122 of these participants, 82 of which were unable to commit into any scheduled slots despite continued expression of interest in the study. Six of them were incarcerated according to their parents. We were able to successfully visit one of them in prison, who expressed interest in further participation in the study, but owing to regulatory difficulties research interview could not be conducted, and all six have remained in prison at the time of writing. Thirty-four were studying abroad and have not been able to return to Hong Kong to attend research interviews up till the time of writing.
We were able to schedule assessments for 192 participants, of which 45 did not turn up, two did not complete ADHD Clinical Diagnostic Scale (ACDS) assessments (one arrived late and was not able to complete assessment, or further schedule an appointment; the other came for first half of the assessment, but became incarcerated since). Eventually, 145 were successfully interviewed for adulthood ADHD persistence. Participation rate was therefore 29% (145/499).
Assessments
Childhood baseline data including age, sex, school year, special education, family constitution, immigration status, diagnoses, comorbidities, and drug prescription records, province of origin and/or birth, and family and family socioeconomic variables—parents’ age, sex, educational attainment, occupation at the time of intake—were documented.
Early Adulthood Outcome Assessment
The Adult ACDS v1.2 (Lara et al., 2009), a semistructured interview for retrospective assessment of all DSM childhood ADHD symptoms followed by an expanded assessment of recent (12-month) adult ADHD symptoms including nine DSM Criterion A symptoms of inattention and nine hyperactivity/impulsivity symptoms, along with 14 non-DSM symptoms relevant to adult ADHD clinical manifestations, were validated and used for adult ADHD assessment (Biederman, Petty, Clarke, Lomedico, & Faraone, 2011). For the Chinese validation, two-way translation was made with endorsement by the original authors to Chinese understandable to both Mandarin and Cantonese speakers, by two separate and independent mental health professionals fluent in both Chinese and English. Before arriving on a finalized version, the working translated version were tested with five adults under clinical care with ADHD to test and improve comprehensibility of the wordings used. An independent panel of academic psychiatrists examined the back-translated instrument for semantic and content equivalence with the original instrument. All interviewers received clinical training as well as training on the administration of the ACDS v1.2 by a representative panel of psychiatrists experienced in adult and childhood ADHD diagnosis. Each trained interviewer completed five practice interviews where symptom ratings agree with those of trainers before formal interview took place. For assessing childhood symptomatology and severity and early adulthood ADHD diagnosis, each participant was interviewed individually, supplemented by a parent interview using the ACDS v1.2 for
a. Current 1-year Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) diagnosis and severity of ADHD by enquiring on developmentally sensitive areas of ADHD symptomatology.
b. Retrospective childhood ADHD diagnosis and severity using the childhood-ADHD module of the ACDS v1.2.
To assess the reliability of the adult module of the Chinese version of ACDS v1.2, 20 participant–parent pairs were separately interviewed by a panel of two specialist psychiatrists blind to ACDS results for assessing criterion validity for ADHD assessment. We found complete ACDS-clinician agreement in current ADHD diagnosis. The panel of clinician experts and academic psychiatrists examined and reviewed the ADHD diagnostic data with the interviewers to resolve ambiguities and discrepancies, and further in-depth clinical interviews with the participant–parent pairs as indicated, before adult-persistent ADHD was confirmed. Monthly calibration meetings were held to prevent rater drift.
Semistructured psychiatric diagnostic assessment was made by trained clinician interviewers blind to the results of current ADHD symptomatology using the validated Chinese-bilingual version of the Structured Clinical Interview for DSM Mental Disorders (So et al., 2003), for lifetime and current diagnoses of Affective disorders, Schizophrenia, Anxiety, and phobic disorders, Substance use disorders, and Eating disorders.
We measured role impairment with the official validated Chinese version of the World Health Organization (WHO) Disability Assessment Schedule (DAS; Chwastiak & Von Korff, 2003). This measure assesses the frequency and intensity of difficulties experienced over the past 30 days in each of three areas of basic functioning—mobility (e.g., walking a mile), self-care (e.g., getting dressed), and cognition (e.g., remembering to do important things)—and three areas of instrumental functioning—time out of role (i.e., number of days totally unable to carry out normal daily activities and number of days of cutting back on amount done or time spent on daily activities), productive role performance (e.g., cutting back on quality of work), and social role performance (e.g., controlling emotions when around other people). WHO-DAS 2.0 data were scored based on item response theory (IRT) with an algorithm (available from WHO) that determines a summary score by differentially weighting the items and levels of severity. Population norms were derived from general population samples from 10 countries (including China). WHO-DAS 2.0 has been shown to be cross-culturally stable showing a similar two-level factor structure across the 19 countries where it was tested.
Socio-Demographic, Occupational, and Educational Outcomes
Parents’ and the participant’s educational attainment, occupation and monthly income, and experience of expulsion from school and work were documented on a standardized list. All these information was confirmed with the patients and parents during the interview. Adverse behavioral/social outcomes, including criminal offense, involvement in fights, violence leading to personal injury with or without criminal consequences, theft, felony requiring conviction, and financial problems, such as failure to settle bills, owing debts, inability to save up to pay for debts, teenage parenthood, were documented from direct interview with parents and patients.
Statistical Analysis
SPSS v24.0 was used for statistical analysis. Baseline socio-demographic data and number of participants who could be traced and those who could not be traced, as well as those included and excluded from the study based on case note perusal, were compared using Pearson’s chi-square tests for binary variables and t tests for dimensional variables. All p values are two-tailed. Fisher’s exact test were used where appropriate. For nonparametric data, Mann–Whitney U test was used to delineate group differences. The primary outcome measure in this study was current 6-month prevalence of persistent ADHD (including full and subthreshold ADHD) in the ADHD follow-up group with 95% confidence interval (CI) of the proportion, weighted for age and sex distribution in the study population. To assess the psychiatric status of persistent ADHD at early adulthood, we used logistic regression models to compare ADHD-persistent and nonpersistent participants on the lifetime prevalence of each disorder at follow-up. Simple statistics, such as Pearson’s chi-square tests, t tests, ANOVAs, and Pearson correlation analyses, were used to compare differences in comorbidity, and socioeconomic variables between those with persistent ADHD against nonpersistent ADHD. Owing to the nonparametric nature of the WHO-DAS IRT scores, univariate comparisons of WHO-DAS role impairment scores in persistent and remitted ADHD participants were performed with Mann–Whitney U test. Bootstrapped linear regression was performed to identify independent predictors of WHO-DAS role impairment scores.
Results
Two participants were deceased. Both were male and in the age group of 20 to 24 at the time of death. According to hospital records, one jumped from height while intoxicated with illicit substances, the other committed suicide by drug overdose. Crude mortality rate was 2/499 = 0.004. According to Hong Kong Census and Statistics Department (2016) data, age/sex specific mortality ratio of male aged 20 to 24 in 2015 was 0.0004. Standardized mortality ratio was therefore = 10% to 1 (95% CI = [3.10, 18.48]) (Census & Statistics Department, 2016). Six of the eligible pool of 499 participants were imprisoned at the time of recruitment.
One hundred forty-five patients (29% of 499) completed current ADHD assessments. Their mean age at the time of assessment was 22.18 (18.11-27.9), mean duration of follow-up being 14.9 years (Figure 1). About 84% were male, and 78.6% had received medications for ADHD by age of 12. Nonresponders (n = 352) had similar gender distribution but were significantly older and more likely to have received medication prescription in childhood compared with the responders (n = 147). We invited all potential participants who declined or were not able to schedule an interview (n = 205) to complete an online version of the ASRS sent to their mobile phone by text messenger. Only half of them consented to receive the questionnaire (n = 103), and only 24 responses were received. Their ASRS scores did not significantly differ from those of the successfully interviewed respondents (28.0 vs. 31.9, p = .15; Table 1).
Comparison of Characteristics Between Respondents and Nonrespondents.
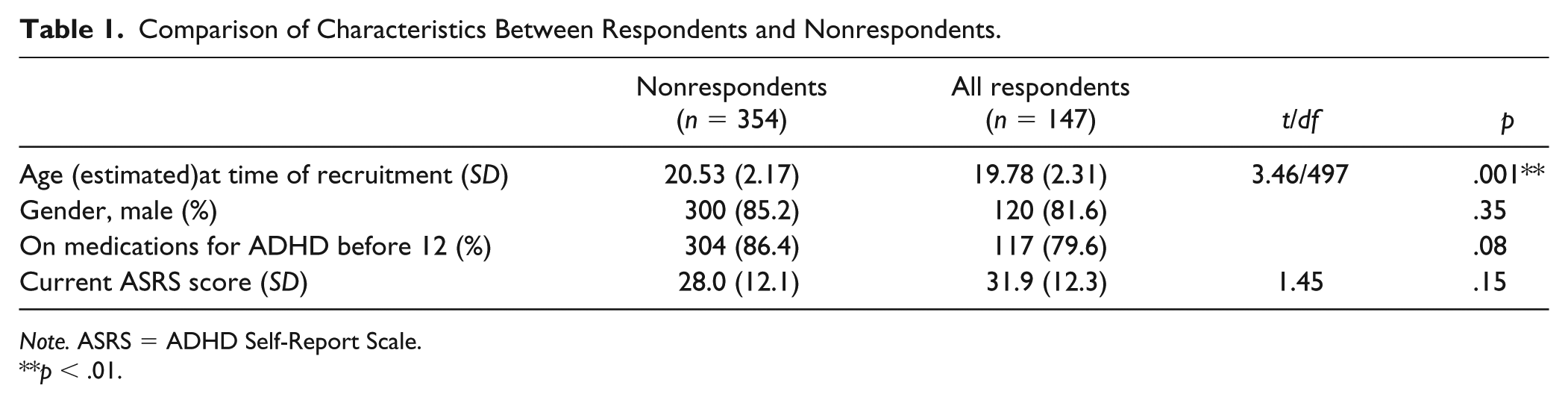
Note. ASRS = ADHD Self-Report Scale.
p < .01.
ADHD Persistence
After weighting for age and sex distribution of nonrespondents, 83.1% (121 of 145) participants currently met DSM-5 criteria for ADHD. Fifty-three (36.8%) met the criteria for ADHD-inattentive subtype, five (3.3%) met criteria for hyperactivity/impulsivity subtype, and 62 (43%) met criteria for combined subtype.
Treatment and Medication History
Median age of first psychiatric appointment was 7, and median age of last appointment was 15 (see Table 2). Participants on average received approximately 8 years (95.17 months) of outpatient psychiatric service for ADHD. Persistent ADHD participants were more likely to stay in care than those who remitted. However, whereas 75.8% of the persistent ADHD participants continued to receive outpatient care after age of 12, only 31.7% continued to receive care past the age of 18. Persistent ADHD participants had on average been out of care for 6.84 years already.
Sociodemographic Data, Treatment History, and Social Outcomes of Remitted and Persistent ADHD.
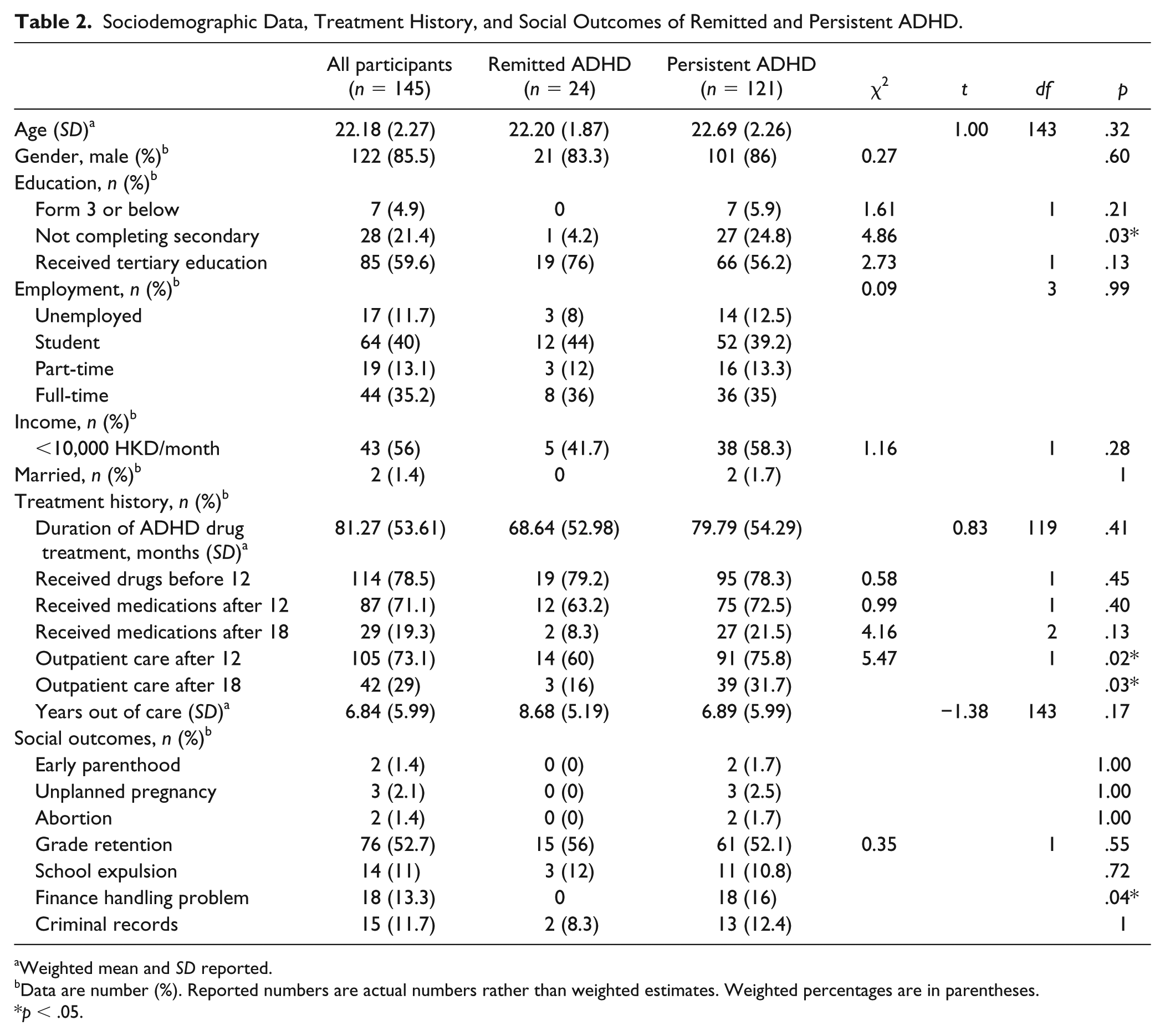
Weighted mean and SD reported.
Data are number (%). Reported numbers are actual numbers rather than weighted estimates. Weighted percentages are in parentheses.
p < .05.
Over 78.3% of all participants had received medications for ADHD before the age of 12, mainly methylphenidate and a minority received atomoxetine. They on average received 6.5 years of drug treatment. Median age of commencement and discontinuation of prescription were 9 years and 15 years, respectively. Only 31.7% of persistent ADHD participants received drug treatment past age of 18, not significantly higher than those without ADHD persistence.
Social Outcomes
All but two of the participants were single. Academically, about half had experienced grade retention, one tenth were expelled from school. Roughly one fifth were unable to complete secondary school education. About 39.2% were currently students, and 12.5% were currently unemployed. About 5.9% of the persistent ADHD participants received education up to Form 3 or below, slightly higher than the 4.76% of young adults in the Hong Kong population (age group 20-29; Census & Statistics Department, the Government of the Hong Kong Special Administrative Region, 2017b). One tenth of the participants reported criminal history, substantially higher than the arrest rate of 0.67% (age group 21-29; Census & Statistics Department, the Government of the Hong Kong Special Administrative Region, 2017a) in the Hong Kong population. Although there are no comparable population-level statistics, 16% in our participants reported significant difficulties handling financial problems. Fewer than one tenth reported adverse family outcomes such as early parenthood, unplanned pregnancy, and abortion.
Significantly more persistent ADHD participants failed to complete secondary school education (24.8% vs. 4.2%, p = .03) and reported significant problems handling financial matters (p = .04) compared with those who remitted. All other adverse social outcomes appeared more frequent in persistent compared with remitted ADHD participants but the differences did not reach statistical significance.
Psychiatric Comorbidities
About 45.5% of the participants met the criteria for a lifetime psychiatric diagnosis (Table 3). About 29.9% had a depressive illness, 3.7% had a bipolar disorder, and 27.6% met criteria for an anxiety disorder. Four patients had alcohol use disorder. None met criteria for substance use disorders, eating disorders, or nonaffective psychoses. Persistent ADHD participants were significantly more likely to suffer from a comorbid mental disorder (49.5% vs. 22.7%, p = .02) and among all mental disorders, depressive disorder (33.3% vs. 9.1%, p = .02).
Psychiatric Comorbidity in Remitted and Persistent ADHD.
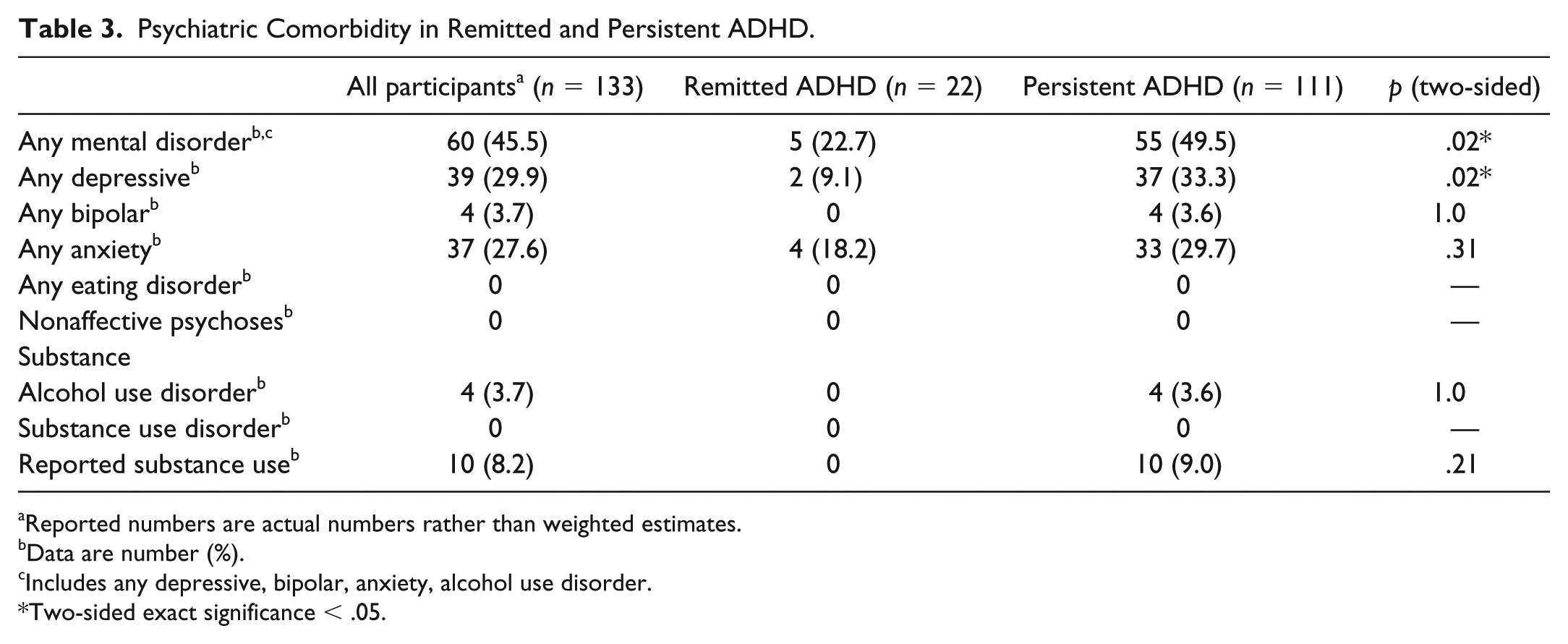
Reported numbers are actual numbers rather than weighted estimates.
Data are number (%).
Includes any depressive, bipolar, anxiety, alcohol use disorder.
Two-sided exact significance < .05.
Role Impairment
Persistent ADHD participants had significantly increased impairment in various domains of life as measured with the WHO-DAS, including understanding and communicating, getting around, getting along with people, life activities, participation in society, and overall scores (equivalent to 78th population percentile versus 65th population percentile in nonpersistent participants; Tables 4 and 5). In all of these domains combined, subtype individuals had significant increase in impairment compared with remitted participants, while inattentive subtype participants had significant increase in impairment only in understanding and communication, getting along with people, life activities, and overall score. In a bootstrapped linear regression model adjusted for age, gender, and education level, current ADHD (p = .003) and history of mental disorders (p = .004) independently predicted current WHO-DAS scores.
Impairment Across Six Domains in WHO Disability Assessment Schedule Between Remitted and Persistent ADHD, and Combined and Inattentive Subtypes.
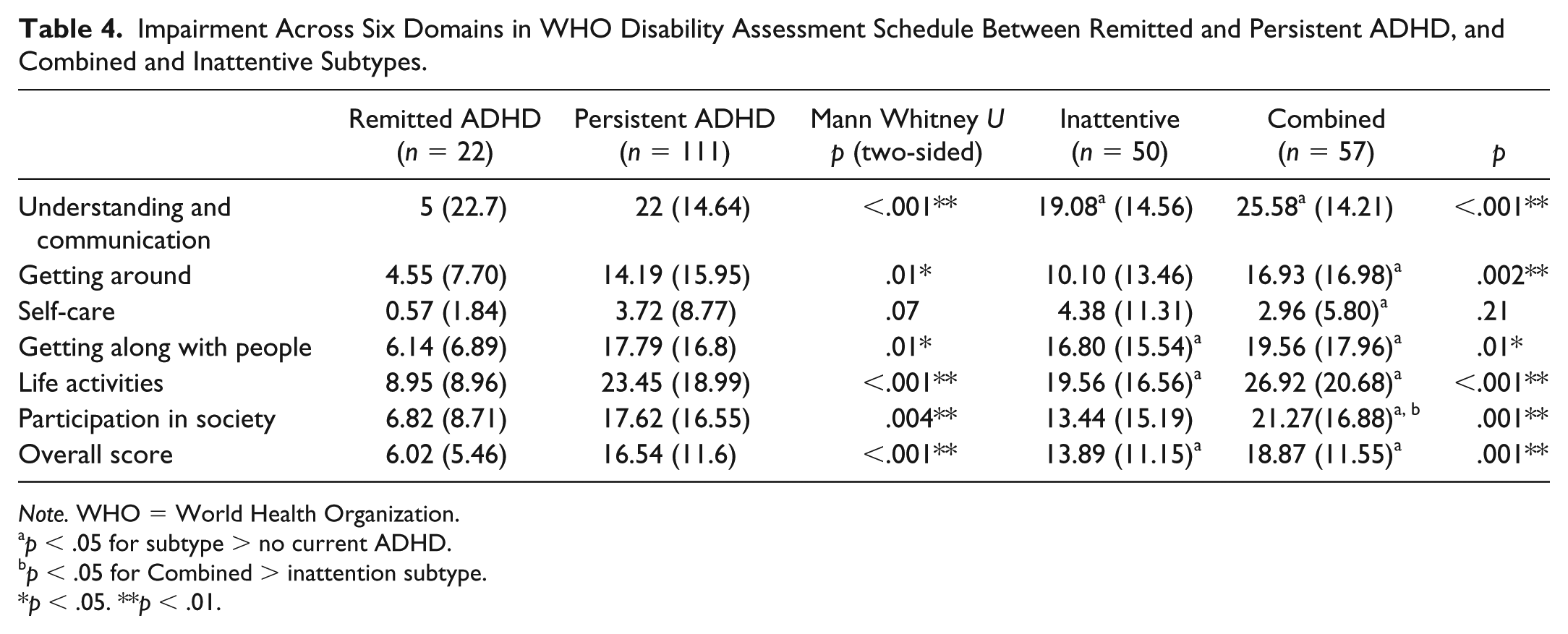
Note. WHO = World Health Organization.
p < .05 for subtype > no current ADHD.
p < .05 for Combined > inattention subtype.
p < .05. **p < .01.
Bootstrapped Linear Regression of the Association Between ADHD Persistence, Any Mental Disorder and Basic Sociodemographic Data, and WHO-DAS.

Note. Dependent variable: WHO-DAS overall complex scoring score. CI = confidence interval; WHO-DAS = World Health Organization Disability Assessment Schedule.
p < .01.
Discussion
Our study has several limitations. First, we were only able to successfully interview 29% of the target sample. Respondents were slightly younger on average but just as likely to have received medication treatment before 12, suggesting similar childhood illness severity. The high persistence rate of ADHD found in the recruited sample may be attributable to participant-derived sampling bias, where participants with less severe ADHD-related problems may be less likely to participate in the study. Note, however, that only 83 (16.6%) declined, and we were able to get in touch with a further 122 (24.4%) participants and their parents who had expressed interest in joining the study but repeatedly failed to turn up for appointments despite numerous attempts at rescheduling. Without proper clinical assessment, it would be difficult to speculate how time management difficulties common to ADHD patients and other illness-related behaviors may explain the scheduling difficulties and refusal to participate in the study (Kessler et al., 2006). It was unfortunate that we were unable to obtain ASRS ratings from more nonrespondents, but the ASRS scores obtained did not suggest any difference in ADHD symptom severity between those who were successfully interviewed. Second, we were unable to provide prospective and structured assessment of ADHD symptoms, impairment, comorbidities, and functioning at earlier time points during adolescence. This precluded a more accurate estimate of the chronology of key ADHD symptoms and related impairments throughout adolescence, where critical changes in psychopathology, family influences, and academic challenges may have occurred. We were also unable to examine the adulthood impact of childhood ADHD severity and other clinical variables in lieu of prospective data collection in the childhood phase. Third, we could only identify children whose ADHD diagnoses were entered in the hospital registry and with compatible childhood symptoms documented in the case records. We would not be able to access those with milder or subthreshold ADHD that escaped clinical attention, especially when presenting with a non-ADHD primary diagnosis such as Major Depressive Disorder. Finally, we did not seek ratings from employers (Barkley et al., 2006), owing to fear of stigma and participants’ concerns consequences about disclosure. This may have led to underestimation of functioning impairment in the work place.
Nevertheless, our findings were important because we showed that Chinese children who received a diagnosis of ADHD in the clinic, like their Western counterparts (Biederman et al., 2012), have a high risk of suffering from persistent symptoms in adulthood. The vast majority of our participants with persistent ADHD met criteria for the inattentive subtype, half of whom also meeting criteria for hyperactive/impulsivity subtype, consistent with Western findings of inattention as the most persistent and probably core deficit in ADHD. Similar to Western findings, ADHD persistence was also associated with increased affective comorbidity (Biederman et al., 2012; Klein, 1991), both independently predicting impairment in broad areas of functioning (Klein, 1991).
We found that ADHD persistence in our cohort was associated with poorer academic outcomes, namely, noncompletion of secondary school studies, school expulsion, and grade retention, similar to those reported in the West (Barkley et al., 2006; Biederman et al., 1996; Kessler et al., 2006; Klein, 1991; Mannuzza et al., 1998). The high rate of reported criminal history compared with the local population, as well as problems in financial self-management also appeared consistent with Western data (Barkley et al., 2006). These broad cross-national similarities in ADHD outcomes support the universality and validity of adult persistence of inattention as a core feature of ADHD that predicts impairment and psychiatric comorbidity. The significant morbidity and adverse socio-educational outcomes may also reflect the diverse health care and social welfare needs incurred from ADHD persistence in young adults.
The lower rates of teenage or unplanned pregnancy and substance use (Barkley et al., 2006; Biederman et al., 1996; Kessler et al., 2006; Klein, 1991; Mannuzza et al., 1998) appeared consistent with previous reports of lower rates of teenage pregnancy (10 in 1,000 in Hong Kong vs. 57 in 1,000 15- to 19-year-old females in the United States; Sedgh, Finer, Bankole, Eilers, & Singh, 2015) and substance use in Hong Kong adolescents (Lau, Kim, & Tsui, 2005) and ADHD patients (Lam & Ho, 2010). However, our recruited sample could have under-represented people with substance use problems, who may have more chaotic lifestyles and therefore more difficult to engage in the study.
Of concern is the finding that most participants with persistent ADHD had ceased to receive care. This is relevant to not only China but also many areas in the world, where child mental health services deliver care only up to the age of 18 when transition to generic adult psychiatric service would occur. Discontinuation of care may occur owing to lack of resource provisions and training for general adult psychiatrists in the clinical assessment and management of ADHD in adulthood, as well as lack of awareness about the nature of ADHD, related impairments and salience of continued treatment on the part of patients and their caregivers.
In summary, cross-national adulthood persistence of ADHD, especially attention deficit, is supported by our clinical data on Chinese participants in Hong Kong with those of the clinical cohorts in the West. Although we still lack population-based cohort data, it is likely that the prevalence of adult ADHD in Chinese communities was previously underestimated (Fayyad et al., 2017). Further research effort should go into prospective measurement of childhood predictors of persistence and impairments in different national samples, as well as cross-national comparison of middle and later adulthood outcomes related to ADHD.
Footnotes
Acknowledgements
The authors would like to thank all the young men and women and their parents for participating in this study, and colleagues in the various sites—Candi Leung, Daphne Ng, Harriet Tang, Marina Wong, Shelly Leung, Veronica Chow and Katy Wong, for their contribution with conducting this study.
Author Contributions
Arthur D. P. Mak contributed in the conception and design of study, research interviews and blind clinical reappraisal, analysis, and write-up; Alicia K. W. Chan contributed in conducting research interviews and data collection and analysis; Phyllis K. L. Chan contributed with the site logistics, study conception, advice on analysis, and manuscript approval; C. P. Tang contributed in the recruitment logistics, clinical diagnoses, and manuscript approval; Kelly Lai contributed in advice on logistics and clinical assessment and support of recruitment logistics; Sheila Wong did the analysis, data management, manuscript preparation, and revision; Patrick Leung contributed in the study conception, advice on ADHD Clinical Diagnostic Scale (ACDS) analysis, and advice on manuscript; S. F. Hung contributed in the study conception, progress monitoring, project management, and analysis; Linda C. W. Lam contributed in the study logistics and design, progress monitoring, and editing of manuscript; and Sing Lee contributed with the conception and design of study and clinical reappraisal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from Health and Medical Research Fund (12130681) of the Government of Hong Kong Special Administrative Region.