
Abstract
Introduction
ADHD is a neurodevelopmental disorder characterized by high and consistent levels of inattention, hyperactivity, and impulsivity that are present before the age of 12 years. These symptoms lead to functional impairment across multiple settings, including home, school, and peer relationships. ADHD has also been shown to have long-term adverse effects on academic performance, vocational success, and social-emotional development (American Psychiatric Association [APA], 2013).
Although ADHD is a disorder usually diagnosed in children, about 15% of the patients retain the full diagnosis by the age of 25 years, with a further 50% in partial remission, indicating that around two thirds of children with ADHD continue to have impairing levels of ADHD symptoms as adults (S. J. J. Kooij et al., 2010). A recent international meta-analysis estimated the global prevalence of ADHD in adulthood to be 2.8%, ranging from 0.6% to 7.3%, depending on the country’s income level (Fayyad et al., 2017).
Comorbidity with other psychiatric disorders is frequent in patients affected by adult ADHD, ranging from 50% to 75% (Kessler, Akiskal, et al., 2006; Piñeiro-Dieguez, Balanzá-Martínez, García-García, Soler-López, & The CAT Study Group, 2016). Patients with ADHD suffer, on average, from three other psychiatric disorders (J. J. S. Kooij et al., 2012).
The prevalence of ADHD in adult patients with major depressive disorder has been estimated to be of 9.4% in the United States (Kessler, Adler, et al., 2006), while comorbidity in bipolar disorder has been reported to be about 9.5% (Nierenberg et al., 2005). The prevalence of ADHD in patients with anxiety disorders seems to be even higher, ranging from 7% to 35% depending on the observed population (Chao et al., 2008; Van Ameringen, Mancini, Simpson, & Patterson, 2011). A recent review reported a prevalence of comorbidity between ADHD and personality disorders ranging from 10% to 75% (Matthies & Philipsen, 2016). Studies conducted in patients with substance use disorders show a prevalence of ADHD in this population ranging from 20% to 30% (Goossensen et al., 2006; Schubiner et al., 2000; Wilens, 2007).
ADHD in adults also appears to be related with sleep disorders (Gau et al., 2007; Veen, Kooij, Boonstra, Gordijn, & Someren, 2010). Considering previous literature, the prevalence of adult ADHD comorbidity across the different psychiatric disorders can range from 10% to 20% (Almeida Montes, Hernández García, & Ricardo-Garcell, 2007; Nylander, Holmqvist, Gustafson, & Gillberg, 2009; Prathibha & Maurice, 2011). A recent and carefully conducted cross-sectional study investigating the presence of ADHD in adult psychiatric nonpsychotic outpatients from Austria, Belgium, Denmark, Germany, The Netherlands, Spain, Sweden, and the United Kingdom found the prevalence to be of 15.8% according to Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) criteria or 17.4% according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) criteria (Deberdt et al., 2015). Other authors report that, on average, one out of five adult psychiatric patients may suffer from ADHD (J. J. S. Kooij, 2013).
Despite the relatively high prevalence of ADHD in the adult psychiatric population, many patients still do not receive proper diagnostic assessment, even when they are routinely followed and treated by a specialist for other disorders (Ginsberg, Quintero, Anand, Casillas, & Upadhyaya, 2014). Considering that currently available treatments show established efficacy, as attested by the high effect sizes reported in literature (De Crescenzo, Cortese, Adamo, & Janiri, 2017), raising awareness and improving diagnostic precision and scientific knowledge of adult ADHD are features of important clinical relevance (Geffen & Forster, 2018).
Appropriate resources for diagnosis are especially lacking in Europe, where therapeutic protocols and molecules approved for treatment of adult ADHD also are scarce (Ramos-Quiroga, Montoya, Kutzelnigg, Deberdt, & Sobanski, 2013). Compared with other European high-income countries, Italy shows a considerably lower rate of adult ADHD diagnosis, probably due to an even more important lack of specific clinician’s knowledge, as attested from nationally representative data (Fayyad et al., 2017).
The aims of this study were to obtain a preliminary evaluation of the prevalence of ADHD in a large sample of Italian adult outpatients and to compare sociodemographic and clinical variables of psychiatric patients with and without a diagnosis of adult ADHD.
Method
Sample and Procedures
All patients accessing two outpatient services of the University Department of Mental Health of the Brescia Spedali Civili Hospital (Italy) in the period between November 2015 and March 2017 were invited to participate in this cross-sectional observational study. Patients who accepted to participate signed a written informed consent form.
The eligibility criteria were (a) age of 18 or older, (b) patient capable of reading and understanding the administered tests, and (c) patient capable of reading and understanding the written informed consent form.
The exclusion criteria were (a) age of 70 or older, (b) diagnosis of intellectual disability, and (c) diagnosis of mental disorder related to general medical condition.
All patients received a unique identification code to maintain data anonymity and patient confidentiality. All precautions were taken for the management of sensitive data, and participants were not given monetary compensation for their involvement.
The administration of psychiatric assessment scales is routinely performed in our services according to the Department rules. In particular, all patients agreeing to participate in this study were assessed using the Mini-International Neuropsychiatric Interview (MINI Plus, Version 5.0.0; Sheehan et al., 1998) to confirm the main psychiatric diagnosis and evaluate comorbidity. All patients were also administered the Adult ADHD self-report Scale Symptoms Checklist (ASRS-V 1.1) Short Form (Kessler et al., 2005) and a questionnaire designed to collect sociodemographic and clinical features. Trained psychiatrists then tested all patients with positive ASRS-V 1.1 using the Diagnostic Interview for ADHD in Adults (DIVA 2.0; J. J. S. Kooij, 2013) to confirm adult ADHD diagnosis according to DSM-IV-TR criteria (APA, 2000). Patients who tested positive both on the ASRS-V 1.1 and the DIVA 2.0 were included in the “ADHD positive” group, whereas patients who tested negative to the ASRS-V 1.1 or who were positive on the screener but negative to the DIVA 2.0 interview were included in the “ADHD negative” group.
Assessment Tools
The MINI Plus Version 5.0.0 is designed as a brief structured interview that could be used to diagnose Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) psychiatric disorders. It has demonstrated its validity and reliability in comparison with other more complex tools (van Vliet & de Beurs, 2007). In the present study, the interview was administered to all enrolled patients to confirm their main clinical psychiatric diagnosis and to identify and diagnose potential comorbidity.
The ASRS-V 1.1 is a self-administered, internationally validated (Kessler et al., 2007) screening tool for adult ADHD developed by the World Health Organization. It consists of an 18-item checklist concerning adult ADHD symptoms as reported in the DSM-IV-TR. Six of these items, four concerning attention deficit symptoms and two concerning hyperactivity/impulsivity symptoms, have shown greater sensitivity and can be used as a separate screening tool, also known as ASRS-V 1.1 Short Form. Patients indicate the frequency of occurrence for each item, from 0 (never) to 4 (very often): The test can be considered positive when four or more answers are above the cutoff value. A positive screening test cannot be considered sufficient to diagnose adult ADHD, but it indicates that further diagnostic investigation is required.
The DIVA 2.0 is a validated (Ramos-Quiroga et al., 2016) structured interview for the assessment of adult ADHD according to the diagnostic criteria of the DSM-IV-TR. It consists of 18 questions (nine concerning inattentive symptoms and nine about hyperactivity/impulsivity) investigating ADHD symptoms as reported in the DSM-IV-TR. Each question is followed by concrete examples, for both childhood and adulthood, to help the patient to recognize symptoms in his or her everyday life. The DIVA interview also investigates the impact of ADHD symptoms on patient’s functioning, considering different areas. The DIVA interview should also be completed with additional data, such as the patient’s school reports, and conducted in the presence of a family member, to better evaluate the presence of ADHD symptoms during childhood and the age of onset of the disorder. This additional information is necessary to perform the retrospective evaluation required for diagnosing ADHD in adults.
Statistical Analysis
All computations were performed using the IBM SPSS Statistics (Version 22.0, IBM Corporation, Armonk, NY, USA). Comparisons were performed using the Pearson’s χ2 test for categorical variables. Mean differences in continuous variables were evaluated using the independent samples t test. A p value of .05 was used to define statistical significance.
Results
Sample Characteristics
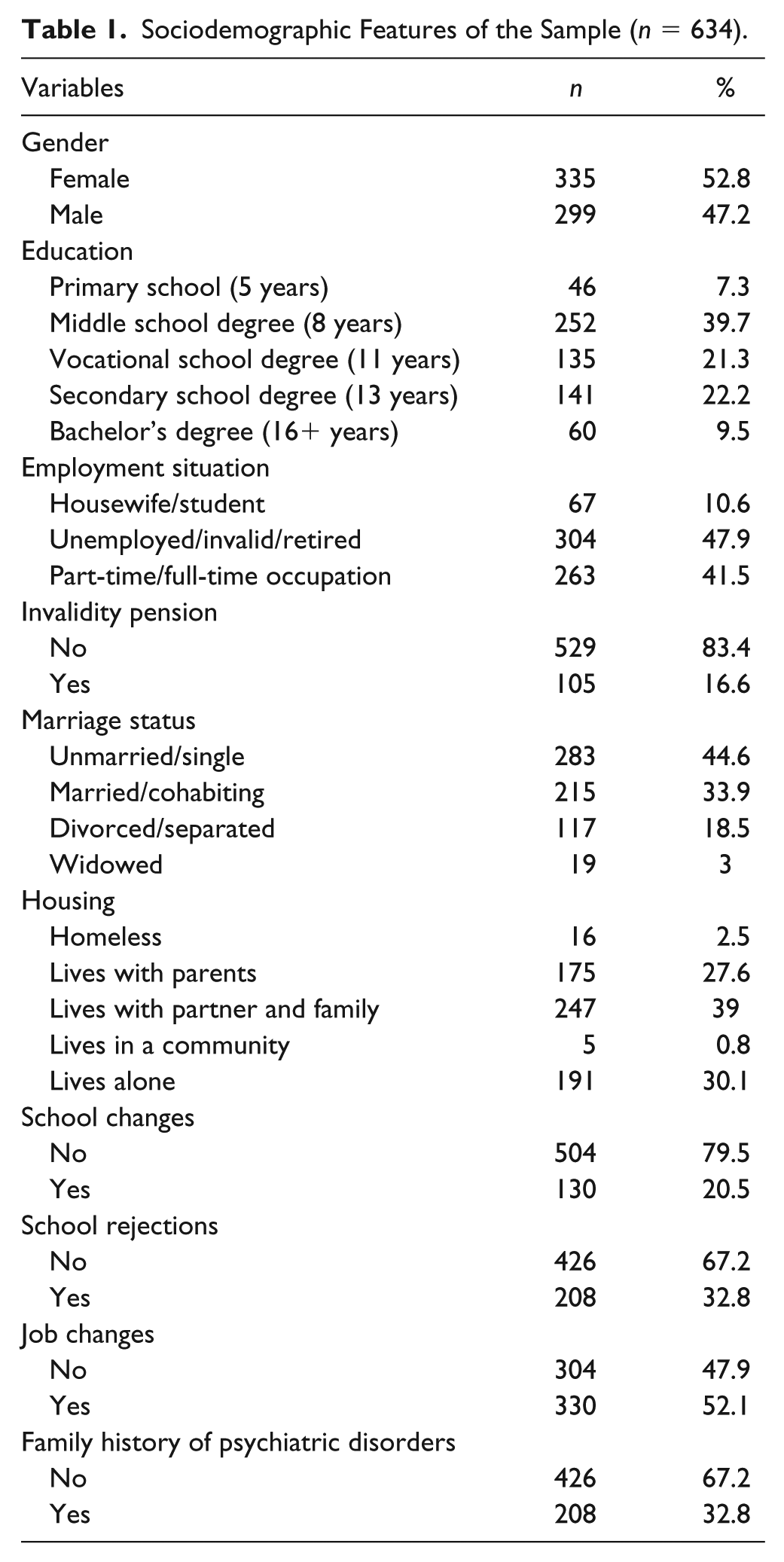
A total of 634 patients accepted to participate in the study. There were 335 (52.8%) female and 229 (47.2%) male participants. The mean age of the sample was 47.2 years (SD ± 12).
The sociodemographic characteristics of the sample are reported in Table 1.
Sociodemographic Features of the Sample (n = 634).
The clinical characteristics of the sample are listed in Table 2.
Clinical Features of the Sample (n = 634).
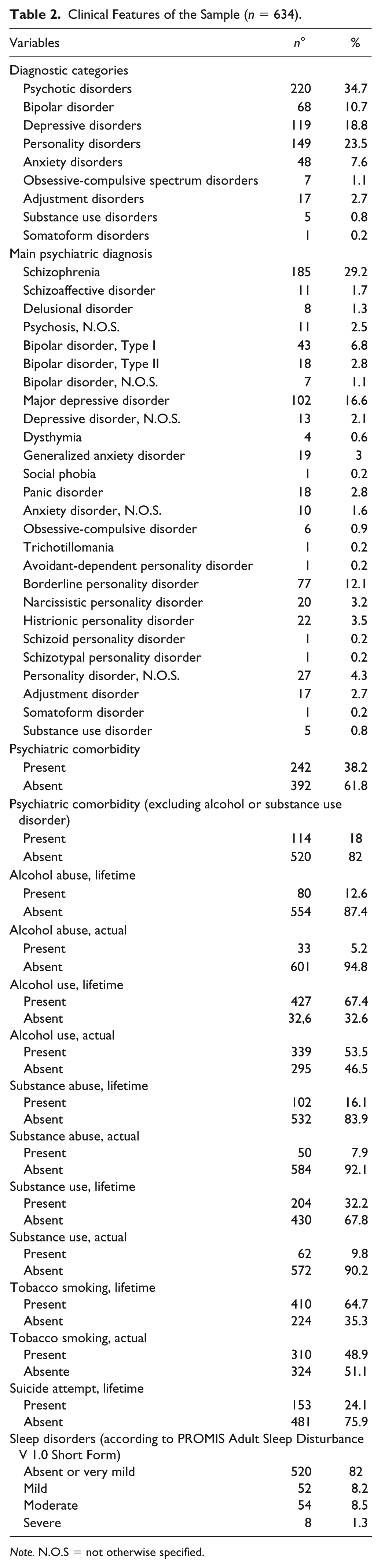
Note. N.O.S = not otherwise specified.
Prevalence of Adult ADHD
Of the total patients’ sample, 81 (12.8%) tested positive while 553 (87.2%) resulted negative on the ASRS-V 1.1 Short Form. After performing the DIVA 2.0 interview, 44 (6.9%) of the total sample met the diagnostic criteria for adult ADHD and were therefore included in the “ADHD positive” group, while 590 (93.1%) tested negative and were included in the “ADHD negative” group.
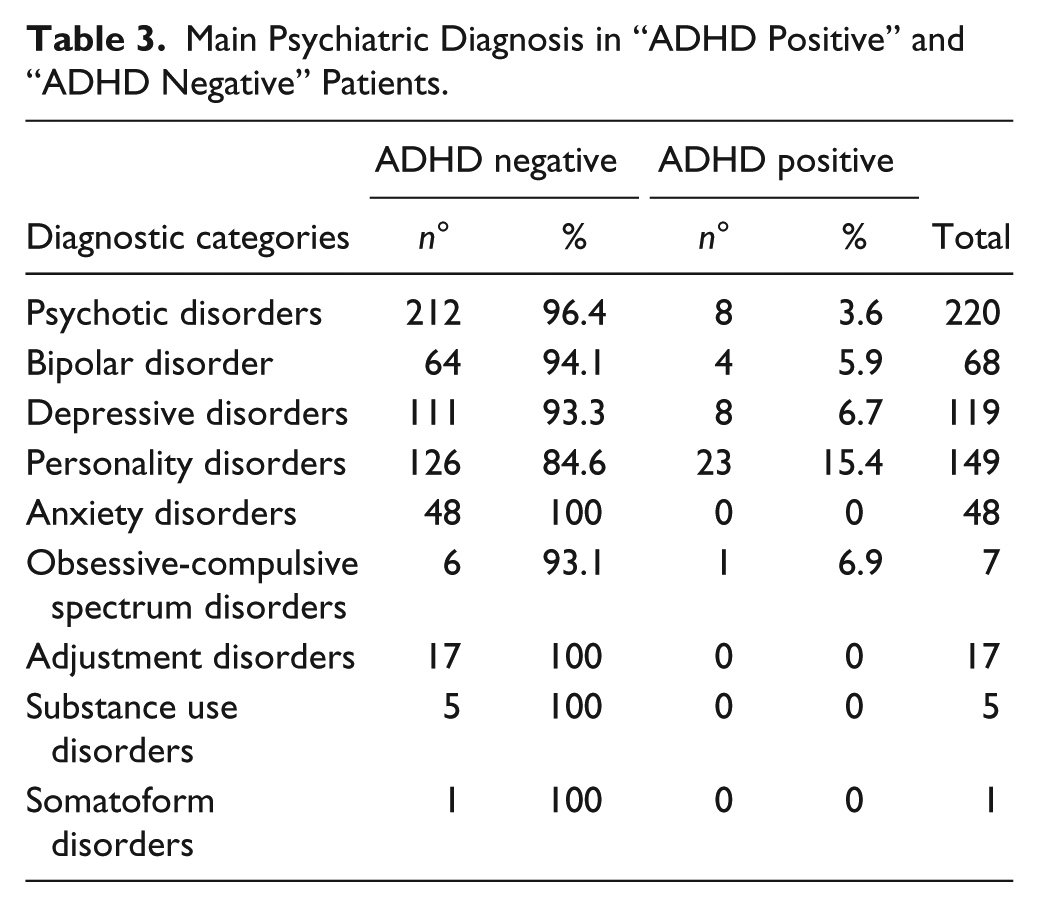
The main psychiatric diagnoses of “ADHD positive” and “ADHD negative” groups are shown in Table 3.
Main Psychiatric Diagnosis in “ADHD Positive” and “ADHD Negative” Patients.
Comparison Between “ADHD Positive” and “ADHD Negative” Groups
The comparisons for sociodemographic features between the groups of “ADHD positive” and “ADHD negative” patients are reported in Table 4.
Comparison for Sociodemographic Features Between Groups.
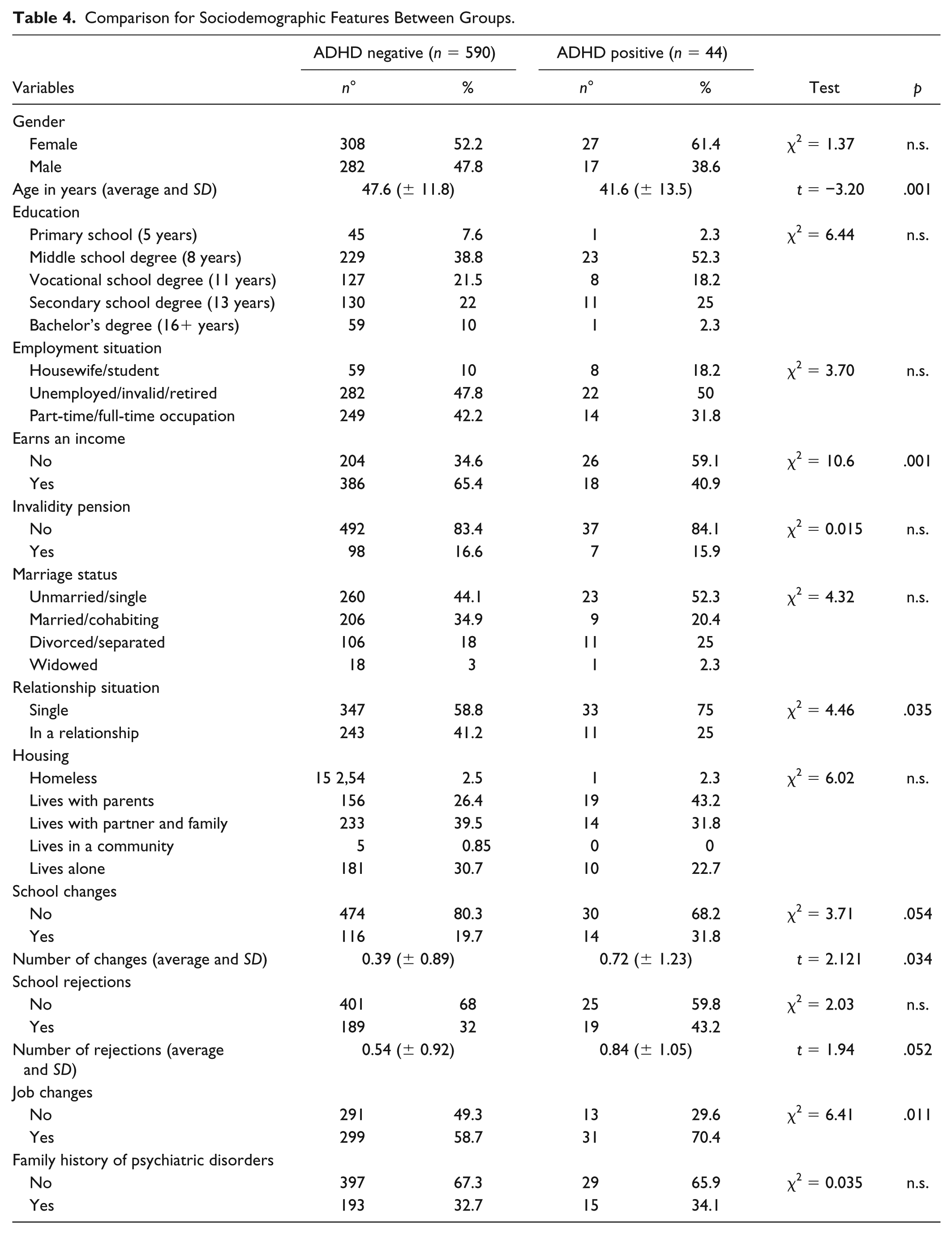
“ADHD positive” were younger (41.6 ± 13.5 years) than “ADHD negative” patients (47.6 ± 11.8 years) at the time of evaluation (p = .001).
Although no significant difference emerged concerning the employment status, the two groups showed a significantly different capacity of independently earning an income: Only 18/44 (40.9%) of the “ADHD positive” group independently earned money, as compared with 386/590 (65.4%) of the “ADHD negative” patients (p = .001).
The two groups differed also in relationship status: 33/44 of the “ADHD positive” group (75%) compared with only 347/590 of the “ADHD negative” patients (58.8%) were single (p = .035).
As for changes in scholastic institutions, a significant difference was found between the two groups concerning average number of school changes, with a higher rate of changes in the “ADHD positive” group (0.72 ± 1.23) compared with the “ADHD negative” group (0.39 ± 0.89; p = .034).
Finally, a significant difference emerged concerning job changes: In particular, 31/44 of the “ADHD positive” patients (70.5%) had changed job at least once in their life, while this happened only in 299/590 of “ADHD negative” patients (50.7%; p = .011).
The comparison of clinical features between the two groups is reported in Table 5.
Comparison for Clinical Features Between Groups.
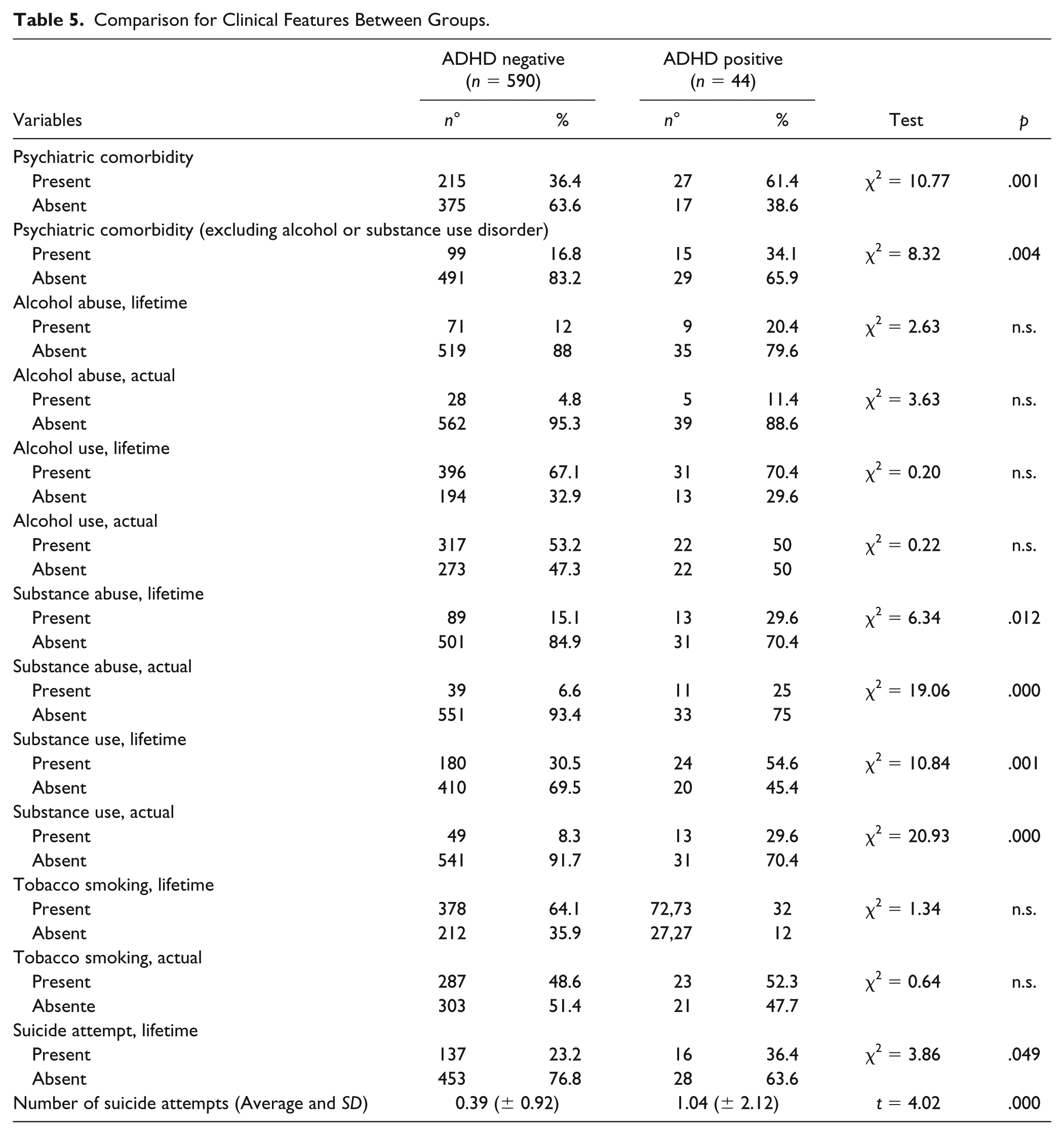
The two groups showed a highly significant difference concerning the presence of multiple psychiatric comorbidity: 27/44 of “ADHD positive” patients (61.4%) showed multiple comorbidity (i.e., two psychiatric disorders other than adult ADHD) while only 215/590 of “ADHD negative” patients (36.4%) showed comorbidity (p = .001). This difference remains significative even excluding the comorbidity with substance use disorders (p = .004).
No differences emerged between the two groups concerning present and lifetime alcohol use and abuse. Conversely, various differences emerged concerning the use and abuse of illegal substances. “ADHD positive” patients showed higher substance use, both current (29.6% vs. 8.3%, p < .001) and lifetime (54.6% vs. 30.5%, p = .001). Even considering the diagnosis of substance abuse, “ADHD positive” patients showed a higher prevalence, both present (25% vs. 6.6%, p < .001) and lifetime (29.6% vs. 15%, p = .012) compared with “ADHD negative” patients.
Another difference was observed for the history of suicidal attempts: 16/44 (36.3%) of “ADHD positive” patients attempted suicide at least once during their lifetime, compared with 137/590 (23.2%) of “ADHD negative” patients (p = .049). Moreover, the mean number of suicidal attempts was significantly higher in the “ADHD positive” group (1.04 vs. 0.39, p < .001).
Discussion
Data obtained from the present study show a prevalence of adult ADHD of 6.9% in the total sample of outpatients with various psychiatric diagnoses. Previous literature shows a slightly higher prevalence in the psychiatric outpatient population, ranging from 10% to 20% (Deberdt et al., 2015; J. J. S. Kooij, 2013). This can probably be due to the careful diagnostic evaluation performed on our sample, comprised both of a validated screening test (Kessler et al., 2007) and a validated diagnostic interview (Ramos-Quiroga et al., 2016). Despite this conservative evaluation, the prevalence of ADHD in the sample remains high and largely comparable to those reported in previous studies.
The “ADHD positive” patients in our sample are younger than the “ADHD negative” ones. This finding is consistent with the available literature, which reports a decrease in the severity of symptoms, especially those related to hyperactivity, as the patients get older (Biederman, Mick, & Faraone, 2000; Evans et al., 2013). Some authors suggest also an increasing difficulty with aging in remembering the core symptoms of ADHD, especially those concerning attention deficit, present during childhood and first adolescence (J. J. S. Kooij, 2013). For this reason, to obtain a careful diagnostic evaluation, the presence of supplemental information, such as previous school reports and the presence of a close relative during the diagnostic interview (as required by the DIVA), is of great importance.
The sample analysis showed no statistically significant difference in school achievement between “ADHD positive” and “ADHD negative” patients. This finding could be explained by the presence in the sample of a co-occurrent psychiatric diagnosis; in fact, psychiatric patients achieve, on average, a lower educational level than the general population (Breslau, Lane, Sampson, & Kessler, 2008). However, the analysis of whole data including rejections and school changes does show differences between the two groups, confirming previous findings (Murphy, Barkley, & Bush, 2002). It could be hypothesized that ADHD patients may decide more frequently to change school for a less challenging one, a strategy that may allow to reduce the attentive burden and general stress levels enough to obtain a degree otherwise not obtainable.
Compared with “ADHD negative” patients, “ADHD positive” participants are less likely to have a personal income; this finding may represent the consequence of the presence of both inattentive and behavioral symptoms in the workplace, which often lead to poor organization, failure in time managing, and relational difficulties both with peers and with superiors (Sarkis, 2014). The data concerning patients’ working status have also been confirmed through the comparison between the number of job changes in the two groups: “ADHD positive” patients show a less stable working condition, with no less than 70% changing job at least once during their life.
Although no difference in marital status was found between the two groups, a statistically significant difference was found concerning relationship status: In particular, most “ADHD positive” patients are single, a result in line with previous literature findings (Asherson et al., 2012).
In our sample, adult ADHD was diagnosed in 6.7% of patients with depressive disorders; in particular, 4.9% of patients with major depressive disorder were included in the “ADHD positive group.” This prevalence is somehow lower than that reported in the international literature (Kessler, Adler, et al., 2006), a finding that can be explained again with the strict diagnostic process adopted. The same consideration could be made for patients with bipolar disorder: In our sample, 5.9% were included in the “ADHD positive” group, a prevalence again slightly lower than that previously reported (Nierenberg et al., 2005). Among patients with a diagnosis of personality disorder, 15.4% were included in the “ADHD positive group”; the prevalence of ADHD rises to 23.4% if only borderline personality disorder is considered, confirming the relevance of this comorbidity (Matthies & Philipsen, 2016). The prevalence of ADHD in patients diagnosed with schizophrenia was only 3.6%. In fact, previous findings reported that comorbidity of ADHD and schizophrenia in adults is not a typical feature and is therefore underresearched (Donev et al., 2011).
Concerning clinical features, the “ADHD positive” group includes a higher rate of people with multiple psychiatric comorbidity; this difference remains statistically significant after excluding the diagnosis of substance or alcohol use disorder. This result is consistent with previous literature, which shows the presence of one or more psychiatric comorbidities in 50% to 75% of adult ADHD patients (Piñeiro-Dieguez et al., 2016), and an average number of three psychiatric comorbidities in adult patients suffering from ADHD (Fayyad et al., 2017).
The study indicates a more frequent presence of substance use and abuse, both current and lifetime, in “ADHD positive” patients. This result is in line with previous findings, which showed a 50% prevalence of substance use disorders in adult participants with ADHD (Biederman, Wilens, Mick, Faraone, & Spencer, 1998; Wilens, Biederman, Mick, Faraone, & Spencer, 1997).
“ADHD positive” patients showed a higher number of lifetime suicide attempts; this finding is also in line with previous literature findings, which report a correlation between ADHD diagnosis, both in childhood and in adult life, suicide attempts, and life-threatening self-harm (Furczyk & Thome, 2014).
Our findings confirm the high prevalence of ADHD comorbidity in the adult psychiatric population in Italy, comparable to that of other high-income countries (Deberdt et al., 2015). The presence of ADHD leads to significant impairment in many areas of functioning, as shown by more frequent changes of school and jobs, lower rates of patients earning an income, and higher rates of being single. Our results also suggest a worse outcome in ADHD patients, with a higher rate of multiple psychiatric comorbidity, of substance use and abuse, and of self-harmful behavior.
Assessing ADHD comorbidity could have an important impact on managing these patients in the everyday clinical practice, as ADHD is a condition that shows a good response to specific treatment (De Crescenzo et al., 2017). Considering the short time required to administer the ASRS-V 1.1 Short Form and its good reliability as a screening tool for adult ADHD (Kessler et al., 2007), its use could be recommended as a routine in the evaluation of psychiatric outpatients, even if they are followed for another psychiatric condition. This could allow to recognize in which cases further investigation is required for this frequently undiagnosed disorder and therefore to achieve a better global evaluation of the patient.
Conclusion
We found a prevalence of ADHD in adult psychiatric outpatients in an Italian psychiatric department comparable to that found in many other high-income countries.
Many clinical correlates of the diagnosis were detected, including difficulties in relevant functional areas, such as education, work and relationship status, the prevalence of comorbidities, and self-harmful behavior, in line with previous literature obtained in other countries.
These findings indicate the importance of implementing specific knowledge on this topic in clinicians and professionals, an unmet diagnostic need in Europe and especially in Italy.
Future research should focus on confirming these data in larger samples obtained from multicenter studies. Moreover, the impact of a concomitant diagnosis of ADHD in the treatment of the primary psychiatric diagnosis and that of the treatment of ADHD in these patients have to be further assessed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.