
Abstract
Keywords
It is well known that attention deficit/hyperactivity disorder (ADHD) is a major childhood psychiatric disorder, which is characterized by a persistent and developmentally inappropriate pattern of inattention, hyperactivity, and/or impulsivity (American Psychiatric Association, 2013). According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.), ADHD is categorized as a “neurodevelopmental disorder”; it was formerly classified under the “disorders usually first diagnosed in infancy, childhood, or adolescence” section, given that it is a chronic, life-long condition unlike many other psychiatric disorders (American Psychiatric Association, 2013).
ADHD affects many areas of one’s life including academic performance, social functioning, occupational functioning, and overall quality of life across the life span (Bagwell, Molina, Pelham, & Hoza, 2001; Mannuzza & Klein, 2000; Matza, Swensen, Flood, Secnik, & Leidy, 2004; Sawyer et al., 2002). Given the broad and long-term impact of ADHD, it is likely to have enormous economic implications for children, families, and society. According to a recent review on economic burden of ADHD, children with ADHD had higher medical costs than matched controls (the difference ranged from US$503 to 1,343) or nonmatched controls (the difference ranged from US$207 to 1,560), due to increased number of hospitalizations, primary care office visits, outpatient mental health visits, and pharmacy refills (Guevara, Lozano, Wickizer, Mell, & Gephart, 2001; Matza, Paramore, & Prasad, 2005). However, as available published studies have mostly been conducted in Western countries, particularly in the United States, they cannot be readily generalized to other cultural, social, and health care environments.
The Global Burden of Disease Study (GBD 2010) reported that the burden of mental and substance use disorders increased by 37% between 1990 and 2010. These disorders have become the leading global cause of all nonfatal burden of disease, as they are mainly composed of years lived with disability (YLDs) rather than years lived of life lost (YLLs; Whiteford et al., 2013). Given that 40% of the world’s population are aged less than 25 years, it is therefore particularly significant that GBD 2010 included ADHD in their scope. They reported that ADHD accounted for 491,500 YLDs/disability-adjusted life years (DALYs) and 0.02% of the total 2.49 billion all-cause global DALYs (Erskine et al., 2014; United Nations, 2011).
Recently, the Korean Burden of Disease Study 2012 (KoBD 2012) reported that the burden of mental and substance use disorders was 945,391 DALYs and accounted for 6.2% of the total burden of disease, ranking seventh (Lim, Lee, & Park, 2016). However, it is still insufficient to obtain accurate computation on the burden of individual mental disorder.
Therefore, we estimated the national burden and economic costs of ADHD on medical care utilization and updated disability weight and explored characteristics of this burden, with respect to age and sex, using representative health statistics and health insurance data from 2012.
Method
Data Source
The National Health Insurance Service (NHIS) is a single national administrative body in the Republic of Korea (ROK) that covers approximately 97% of the entire population. Therefore, the database managed by the NHIS includes medical information, which is representative of the entire Korean population who received health care services at a medical institution (Kwon, 2009). We used NHIS claims data from January 1 to December 31 in 2012, to estimate the prevalence rates, hospital use, and medical expenditure resulting from ADHD for Korean people aged 19 years or younger. We limited the age of the study cohort because the NHIS coverage of adult ADHD treatment was not approved at the time of 2012.
Case Definition
The International Classification of Disease (ICD)-10 code F90 was used to identify ADHD cases. ADHD cases were extracted based on a primary and first additional diagnosis in the claims data and confirmed when a policyholder made at least one hospitalization or at least three outpatient claims during 2012.
Prevalence Rates of ADHD
The prevalence rate of ADHD was defined as the total number of ADHD cases divided by the registered population of Korean residents in 2012, which was provided by the KOrean Statistical Information Services (KOSIS), a national statistical database operated by Statistics Korea.
Estimation of YLDs (Prevalence-Based DALY) of ADHD
DALY is a summary measure of population health; the DALY of ADHD was calculated to estimate the burden of ADHD. The DALY aggregates the total burden of disease into a single measure in units of healthy life lost, by combining YLD due to morbidity and YLL due to premature mortality. In the present study, a prevalence-based approach was used to calculate the DALYs of ADHD. Therefore, estimated YLD describes current health losses arising from either incident or prevalent cases of ADHD in 2012. The following formula was used to calculate YLD: YLDs = Prevalence (sequela) × Disability Weight (health state) (Yoon et al., 2016). The disability weight of ADHD in the South Korean population was developed as 0.470 in the previous study (Ock, Ahn, Yoon, & Jo, 2016).
Estimation of the Economic Burden of ADHD
The economic burden of ADHD was estimated based on the societal perspective. Societal costs include direct medical costs, direct nonmedical costs, and indirect costs caused by a disease (Kim et al., 2013). The costs resulting from ADHD were estimated using a prevalence-based approach, which measured the costs caused by either new or preexisting cases of ADHD in 2012.
Direct medical costs cover insured and uninsured medical costs incurred as a result of treating ADHD. NHIS claims data were used to calculate NHI-covered outpatient and inpatient medical costs. Uninsured medical costs were estimated using the ratio of the NHI-covered medical costs to noncovered medical costs which was provided by the NHIS (Seo et al., 2012).
Direct nonmedical costs include transportation costs and caregiver costs. Transportation costs associated with ADHD were defined as the products of the number of outpatient visits and hospitalizations with the average roundtrip transportation costs. The average roundtrip transportation costs were US$2.169 per outpatient visit and US$20.246 per hospitalization according to Korean Health Panel data (Seo et al., 2014).
The caregiver costs for inpatient care were calculated by multiplying the number of hospitalization days by the average daily caregiver cost (Kim, Lee, Park, Lee & Oh, 2016). To calculate the caregiver costs for outpatient visits, however, one third of the number of outpatient visits were multiplied by the average daily caregiver cost, because the number of hours spent for an outpatient visit was considered as one third of the caregiver’s working hours.
Indirect costs include lost productivity from disability and premature death associated with ADHD. Indirect costs were estimated using the human capital approach (Drummond, Sculpher, Torrance, O’Brien, & Stoddart, 2005). Because we assumed that patients aged 19 years or younger would not be working, the productivity loss was defined as zero. In addition, because there were no deaths from ADHD, the productivity loss due to premature deaths was defined as zero as well.
The total economic burden of ADHD was calculated by adding the direct and indirect costs of ADHD. All estimated costs were converted from Korean won (KRW) to US$ using the average exchange rate in 2012 (US$1 = 1,126.76 KRW; “Statistics Korea,” 2014).
Ethics Statement
The current study was performed as a part of the KoBD 2012 (Yoon et al., 2016) and was funded by the Ministry of Health and Welfare. The study was approved by the Korea University Institutional Review Board, No. 1040548-KU-IRB-13-164-A-1(E-A-1). Informed consent was waived by the board.
Results
Approximately 96% of the ADHD patients were 19 years or younger; patients aged 10 to 19 years accounted for 67.76% of all cases. Table 1 outlines the epidemiologic characteristics of patients with ADHD aged 19 years or younger in Korea. In 2012, a total of 69,353 people in South Korea experienced at least one hospitalization or at least three outpatient visits for the treatment of ADHD. The estimated prevalence rate of ADHD was 6.18 persons per 1,000 people. The prevalence of ADHD was 3.53 times higher (9.39 vs. 2.66 per 1,000 population) in boys than in girls.
Attention Deficit/Hyperactivity Disorder prevalence Rates Per 1,000 Population in Koreans Aged 19 or Younger in 2012—Data Grouped by Sex.

Because there were no deaths from ADHD, YLL was zero for all age and sex groups. The burden of ADHD in 2012 as measured by the prevalence-based approach was 32,605 DALYs (Table 2). Male patients (25,901 DALYs) had greater burden from ADHD than female patients (6,704 DALYs). The group aged 10 to 19 years accounted for the higher burden (71.0%) of the total DALYs compared with the group aged 0 to 9 years (29.0%).
Prevalence-Based Disability-Adjusted Life Years of Disease Due to Attention Deficit Hyperactivity Disorder in Koreans Aged 19 or Younger in 2012.

Note. YLLs = years lived of life lost; YLDs = years lived with disability.
Table 3 presents the health care utilization characteristics of patients aged 19 years or younger with ADHD in Korea. On average, patients with ADHD had 9.07 outpatient visits in 2012. The mean number of outpatient visits for the 0- to 9-year age group was higher than that for the 10- to 19-year age group (9.93 vs. 8.72). Furthermore, the mean number of outpatient visits for male patients was higher than that for female patients (9.32 vs. 8.09).
Outpatient Visits and Inpatient Admissions Due to Attention Deficit Hyperactivity Disorder in Koreans Aged 19 or Younger—Grouped According to Age and Sex.
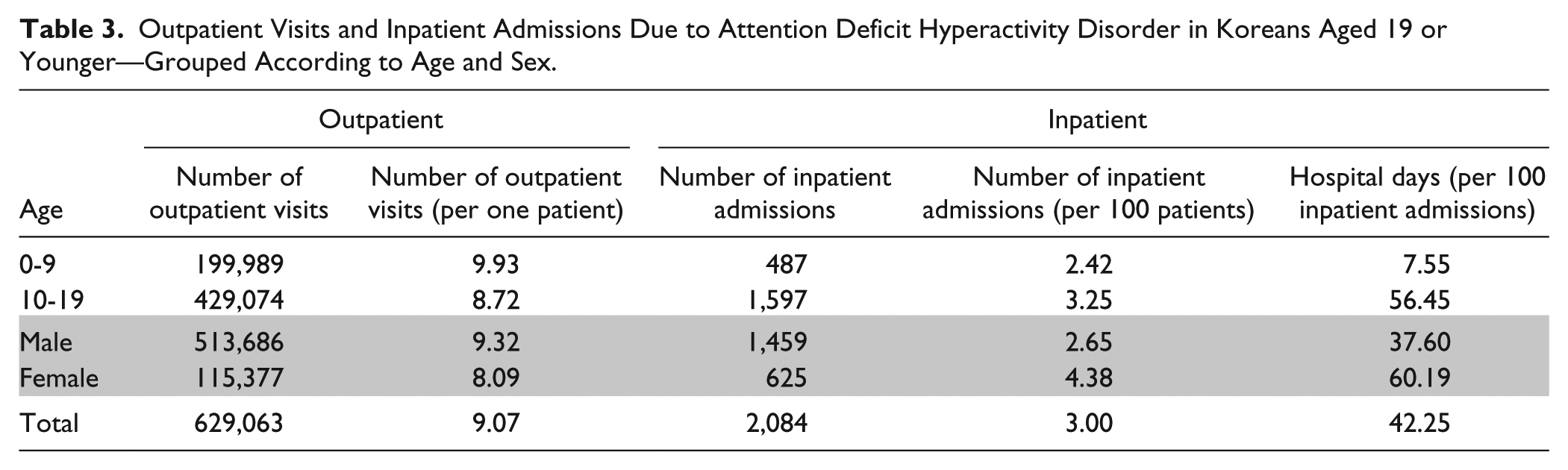
The mean number of hospitalizations per 100 patients was 3.00, with a higher number of hospitalization observed among those aged 10 to 19 years (3.25 per 100 patients). The mean number of hospitalizations per 100 patients for female patients (4.38) was higher than that for male patients (2.65). The mean duration of hospitalization per 100 patients was 42.25 days, with a longer duration observed among those aged 10 to 19 years (56.45). The mean durations of hospitalization per 100 patients were 37.60 days for male patients and 60.19 days for female patient (Table 3).
Table 4 shows the economic burden of ADHD among Koreans based on the direct and indirect costs in 2012. The total burden was US$47.75 million, which accounted for approximately 0.004% of the Korean gross domestic product (GDP) in 2012. Outpatient medical cost accounted for the biggest portion of direct costs (53.36%), followed by uninsured medical cost (19.22%), caregiver cost (19.04%), transportation cost (5.10%), and inpatient medical cost (3.28%). Indirect costs were calculated as the sum of work-loss costs and lost future income due to ADHD-related deaths; both costs were identified as US$0.
Economic Burden of Disease Due to Attention Deficit Hyperactivity Disorder in Koreans Aged 19 or Younger in 2012.
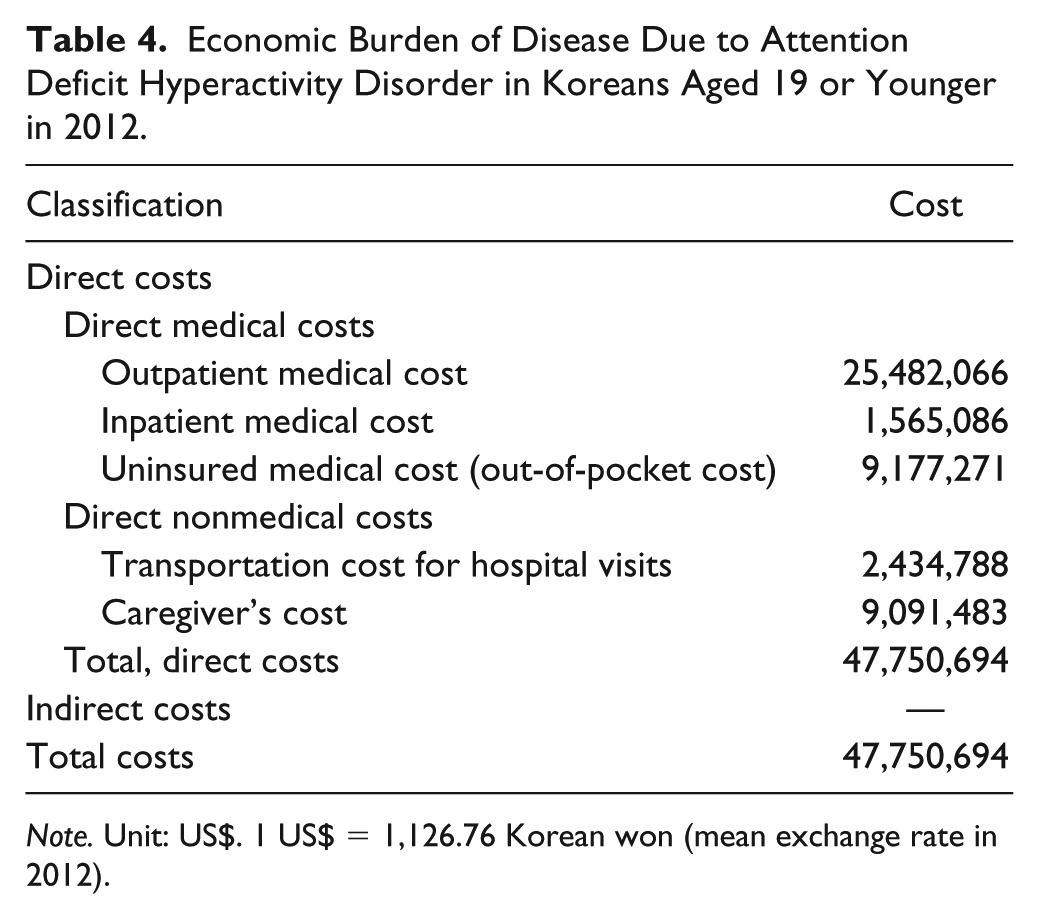
Note. Unit: US$. 1 US$ = 1,126.76 Korean won (mean exchange rate in 2012).
Table 5 outlines the economic burden of ADHD, according to each age group. The economic burden of inpatient care was US$3.25 million (6.80% of the total cost), compared with US$44.50 million (93.20%) for outpatient care. The majority of economic burden was observed among patients aged 10 to 19 years, with a total amount of US$34.26 million. The economic burden of ADHD-related hospitalization among patients aged 10 to 19 years was US$3.05 million and the cost of outpatient care was US$31.20 million. The average treatment cost per capita due to ADHD was US$688.52.
Economic Burden of Disease Due to Attention Deficit Hyperactivity Disorder in Koreans Aged 19 or Younger in 2012—Grouped by Age.
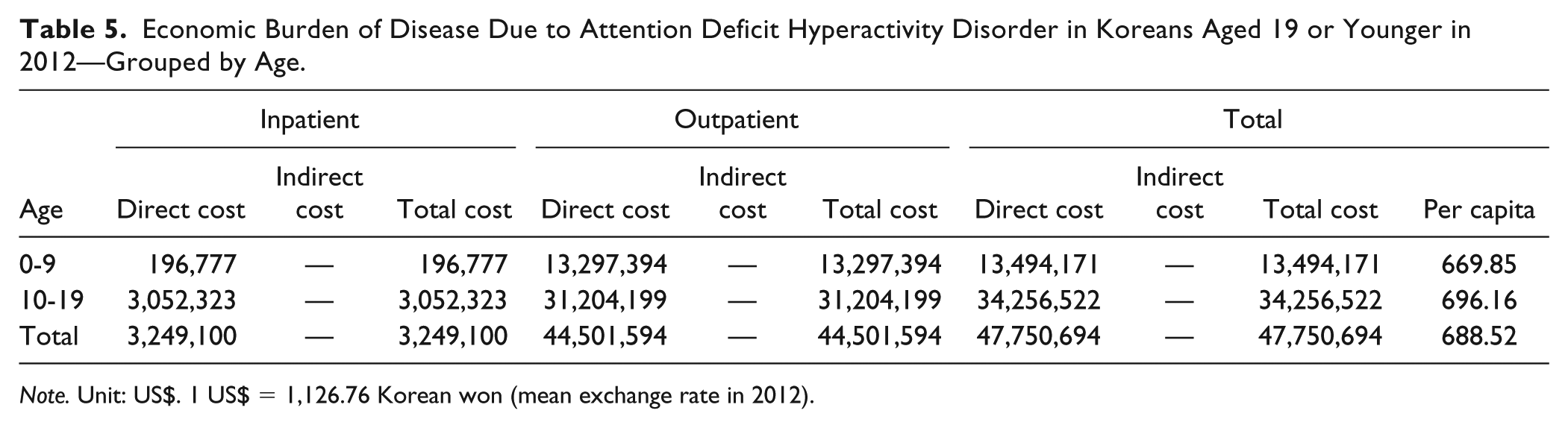
Note. Unit: US$. 1 US$ = 1,126.76 Korean won (mean exchange rate in 2012).
Discussion
A growing body of literature has demonstrated that ADHD places a substantial socioeconomic burden on the individual patient as well as on society. However, there is no representative published study on ADHD in Korea. Therefore, the present study is significant; as to our knowledge, it is the first to measure the DALY and economic burden on individuals with ADHD, using national representative data, that is, NHIS claims data.
ADHD contributed a total 32,605 YLDs/DALYs to the burden of disease in Korea. Considering that total burden of mental and substance use disorder in the 0- to 19-year age group is 112,566 (Lim et al., 2016), it is very high occupancy rate, accounting for 28.9%. In 2012, the burden of mental and substance use disorder in Korea was 1,860 DALYs per 100,000 people (945,391 DALYs) and accounted for 6.2% of the total burden of disease. These diseases, which were the seventh greatest contributor, were more responsible for the total burden of disease than digestive diseases, transport injuries, HIV/AIDS, and tuberculosis (Yoon et al., 2016). According to recent findings, worldwide mental and substance use disorder was the fifth leading disorder category for global DALYs accounting for 183.9 million DALYs and 7.5% of total disease burden in 2010 (Whiteford et al., 2013). According to the GBD in 2010, ADHD was responsible for 0.06% of total YLDs and 0.02% of total DALYs (491,500 YLDs/DALYs) globally (Erskine et al., 2014). Thus, our findings corroborated with previous results. For mental and substance use disorder, YLD accounts for 98.5% (Lim et al., 2016). Although there was apparently no contribution of YLLs, with deaths in people with ADHD were coded to the physical cause of death and suicide was coded under the injuries under self-harm category, our findings demonstrated that ADHD significantly contributes to the burden of disease in Korea.
In our study, the economic burden of ADHD was estimated at US$47,750,694, which amounts to 53,803,571,971.44 KRW (1 US$ = 1,126.76 KRW, mean exchange rate in 2012).
It amounts to 0.004% to 2012 GDP (1,377,813,395,600,000 KRW [US$1,222.81 billion]) in Korea. The economic burden of this study was only inclusive of direct and indirect medical expenses. Considering the characteristics of ADHD, additional costs, such as cost to families (Cussen, Sciberras, Ukoumunne, & Efron, 2012; Swensen et al., 2003), cost of comorbidities (Balázs, Győri, Horváth, Mészáros, & Szentiványi, 2018; Burd, Klug, Coumbe, & Kerbeshian, 2003), accidents (Swensen et al., 2004), criminality (Matza, Paramore, & Prasad, 2005), or loss of work (Birnbaum et al., 2005), are also expected. Furthermore, the chronicity of ADHD is another issue that must be mentioned. With the continuing impact of ADHD in adulthood, the additional economic costs of adults with ADHD need to be considered (Secnik, Swensen, & Lage, 2005). In recent review with this perspective, which was conducted in the United States, the overall national annual incremental costs of ADHD ranged from US$143 to 266 billion (Doshi et al., 2012). Further studies in Korea are needed to estimate the incremental education expenses, spillover costs borne by the family members, or productivity and income losses in adult patients. Compared with the incremental cost of US$949.24 (Gupte-Singh, Singh, & Lawson, 2017), the result of our study was estimated as only US$688.52, which might be related to the low patient payment expenses in Korean medical system.
ADHD is mainly recognized in children and adolescents. Thus, the timely assessment and regular monitoring may help curtail the high socioeconomic expenditures associated with this condition, including high comorbidities.
A few limitations in the present study must be noted. First, we acquired data from a secondary database, that is, the NHIS claims database, rather than from medical records. It is precisely the treatment prevalence–based burden of disease. Furthermore, we did not consider neither psychiatric nor physical comorbid disorders. Therefore, questions regarding variations of diagnostic validity and comorbidity information across hospitals may be raised. However, there were no significant differences between the present study and previously published papers on the prevalence of ADHD (Hong, Kwack, et al., 2014; Hong, Lee, et al., 2014). To ensure accuracy, we additionally used the number of hospitalizations and frequency of outpatient visits. Another limitation is that we used data from the population aged 0 to 19 years, instead of assessing all age groups, because the NHIS coverage only applied to the child and adolescent population. Thus, these results may not accurately reflect the population aged 20+ years. Since September 2016, the NHIS coverage was extended to the adult population. According to recently published review, an incremental increase in the costs associated with ADHD is expected (Doshi et al., 2012). The economic cost and DALY of ADHD in the adult population remains to be investigated in further studies.
Despite the limitations, however, the present study on ADHD burden and economic cost is a major milestone in the recognition of its impact on the population. ADHD accounts for a large proportion of the total burden of disease and economic costs, given that the majority of its burden occurs within childhood, as opposed to other causes of burden that occur across the life span. The substantial number of YLDs/DALYs and economic costs emphasize the necessity of investigating the financial implications of this burden and the need for policy makers to appropriately resource the prevention and early intervention of mental disorders affecting childhood.
Footnotes
Authors’ Note
I-H.O. and H.P. contributed equally to this study. Bomi Park is now affiliated with National Cancer Control Institute, National Cancer Center, Goyang, Korea.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Korean Health Technology R&D Project, Ministry of Health and Welfare, Republic of Korea (number of study: HI13C0729).