
Abstract
Introduction
Sleep/circadian rhythm problems are among the most frequent medical conditions associated with ADHD, a disorder characterized by a persistent and impairing pattern of inattention, hyperactivity, and impulsivity (Cassoff, Wiebe, & Gruber, 2012; Um, Hong, & Jeong, 2017).
Many case-control and cross-sectional studies have reported an association between ADHD and short sleep duration, great difficulty in falling asleep, great frequency of nocturnal awakenings, sleep problems/dysfunctions, and late sleep-time preferences (Cassoff et al., 2012; Coogan & McGowan, 2017; Díaz-Román, Mitchell, & Cortese, 2018; Hvolby, 2015; Um et al., 2017). Few longitudinal studies have assessed the role of sleep duration and sleep problems as an early ADHD predictor (Armstrong, Ruttle, Klein, Essex, & Benca, 2014; Gregory, Agnew-Blais, Matthews, Moffitt, & Arseneault, 2017; Scott et al., 2013; Steinsbekk & Wichstrom, 2015; Tso et al., 2019; Williams & Sciberras, 2016) as well as the effect of some important sleep measures such as daytime sleep duration or restless sleep (Cortese, Faraone, Konofal, & Lecendreux, 2009; Díaz-Román, Hita-Yáñez, & Buela-Casal, 2016).
Shorter total sleep duration and more nocturnal awakenings at 5, 6, and 9 years of age were associated with ADHD at ages 7 to 9 years in the Avon Longitudinal Study of Parents and Children (ALSPAC) cohort (Scott et al., 2013). In another population-based study, moderate to severe sleep problems from 2 to 7 years of age were associated with hyperactivity/inattention symptoms from 8 to 9 years (Williams & Sciberras, 2016). Recently, a Chinese population-based cohort study reported an association between early sleep deprivation and an elevated risk of ADHD in middle childhood (Tso et al., 2019). However, there is great variability in how previous studies have selected and used confounding variables for adjustment in multivariable analyses when assessing the effect of sleep on ADHD. Many important theoretical variables, such as socioeconomic, maternal/pregnancy, and birth-related factors, are not included in the models; thus, findings may be hampered by confounding factors.
Moreover, most studies evaluate sleep variables at specific and single time points. In this sense, the long-term effect of sleep duration in early life and its changes with respect to several time points are largely unknown. Analyses considering changes in sleep duration over time have only been carried out by Scott et al. (2013) and Armstrong et al. (2014). According to the former, a reduction in sleep duration from 3 to 5 years of age increased the risk of ADHD (Scott et al., 2013). Armstrong et al. (2014) observed that the persistence of insomnia at both 4.5 and 9 years was associated with ADHD symptoms at 9 years, and the persistence of movements during sleep was associated with ADHD symptomatology at 9 and 18 years of age (Armstrong et al., 2014). Studies evaluating sleep trajectories as a predictor of ADHD can provide meaningful information about the link between both traits; however, they are scarce in the literature.
Another important issue related to sleep problems in ADHD is the presence of psychiatric comorbidities (Díaz-Román et al., 2018). Sleep problems are associated with both internalizing and externalizing problems in childhood and adolescence and can also predict other mental health outcomes (Sadeh, Tikotzky, & Kahn, 2014). For example, the cohort study cited above found that persistent insomnia was also associated with both depression and externalizing symptoms at age 9 years and both anxiety and externalizing symptoms at age 18 years (Armstrong et al., 2014). In review studies, other circadian and sleep problems have been associated with several emotional and behavioral conditions in addition to ADHD, such as depression, anxiety, risk-taking, and aggression (Brown et al., 2018; Sadeh et al., 2014; Zee, Attarian, & Videnovic, 2013). Therefore, we cannot assure that sleep problems are specific to ADHD. For instance, although sleep problems were recognized as being related to ADHD according to observational epidemiologic studies, they were removed from the ADHD diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994; Cortese, 2015) due to the need for more well-conducted studies in the field assessing the specificity of the association.
Considering the current exposed pitfalls of the association between sleep characteristics and ADHD and the lack of birth cohort studies with a considerable sample size (Cortese et al., 2009; Díaz-Román et al., 2016), this study has the following aims: (a) to investigate the effect of sleep duration and sleep problems at 12, 24, and 48 months on ADHD at 11 years of age in a Brazilian population-based birth cohort; (b) to investigate the effect of 3-point (12, 24, and 48 months of age) sleep duration trajectories on the same outcome; and (c) to evaluate the specificity of the effect on ADHD and hyperactivity/inattention problems, testing the effect of sleep variables over other mental disorders.
Method
Sample
The 2004 Pelotas Birth Cohort is a population-based longitudinal study conducted with hospital childbirths in the southern Brazilian city of Pelotas. Among the 4,263 live births, 4,231 mothers agreed to participate in the study. For the current analyses, twin births and children with neurodevelopmental impairments due to genetic syndromes were excluded. We included data from children visited at ages 12, 24, and 48 months and at 11 years. The follow-up rates during these visits were 94.3%, 93.5%, 92.0%, and 86.6%, respectively (Santos et al., 2011; Santos et al., 2014). At the 11-year follow-up, 92 participants potentially eligible for the study were not included due to death. All data were collected by trained interviewers.
ADHD
At the 11-year follow-up, trained psychologists applied the Development and Well-Being Assessment (DAWBA; Goodman, Ford, Richards, Gatward, & Meltzer, 2000) to mothers and caregivers to assess ADHD and other mental health disorders. ADHD was evaluated by a specific DAWBA section consisting of 31 closed- and open-ended questions. For the final classification, two independent and experienced mental health professionals assessed all of the responses. Cases were defined according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) criteria, as were other mental disorders. The DAWBA was adapted and has been validated for the Brazilian population aged between 4 and 16 years (Fleitlich-Bilyk & Goodman, 2004).
Sleep Behavior (Exposures of Interest)
Nighttime sleep duration
Maternal reports of children’s sleep behavior were collected at 12, 24, and 48 months. To assess children’s bed and wake times in the past 2 weeks, mothers were asked the following questions: “In the last two weeks, at what time did your child go to bed at night?” and “At what time did the child wake up in the morning?” In addition to bedtime, mothers were asked about how long it took the child to fall asleep (sleep latency). Mothers were also asked about night awakenings: “In the last 2 weeks, did the child wake up during night?” If they responded yes to this question, we asked, “How many nights in the last two weeks?” and “How often each night?” We calculated nighttime sleep duration by discounting the latency and the wake time after sleep onset. The mean wake time after sleep onset was calculated by multiplying the average number of nocturnal awakenings in the last 2 weeks by the estimated time the child was awake in each event at each time point. The duration of each nocturnal awakening was based on data from the Sleep Trial, carried out with a subsample of the Pelotas 2015 Birth Cohort Study, which included all the children born in Pelotas in 2015 (Santos et al., 2016). Sleep duration, objectively measured by actigraphy, during that trial showed that each nighttime awakening lasted an average of 22 min at 12 months and 7 min at 24 months of age. Given that no local data on the duration of night awakenings at 48 months was available, we assigned 7 min to each.
Daytime sleep duration
Mothers were also asked, “In the last 2 weeks, approximately how many naps did the child take during the day?” and “Approximately how long did each nap last?” We multiplied these two variables to calculate daytime sleep duration.
Total sleep duration
Sleep duration over the 24-hr period (total sleep duration) was calculated by adding the nighttime and daytime sleep duration variables. In this study, sleep durations ranging between 3 and 20 hr per day were considered plausible values. Values out of this range, as assessed manually by two specialized analysts, were considered outliers and were excluded from analyses (N = 13).
Total sleep duration trajectories from 12 to 48 months (short sleepers, typical sleepers, and longer sleepers) were also built. A semiparametric, group-based approach was used to identify the different patterns of total sleep duration reported by mothers from 12 to 48 months of age. This is a specialized form of finite mixture modeling designed to identify rather than assume groups or clusters of individuals following similar developmental trajectories (Nagin, 2005; Nagin & Tremblay, 2005). A polynomial function was used to model the relationship between total sleep duration and age. The models were estimated with the Stata procedure “traj” (B. L. Jones & Nagin, 2012). A logistic model was used to fit the data. The choice of the number and shape of trajectories was based not only on the best fit of the model (maximum Bayesian information criterion [BIC]) but also on the interpretability of the obtained trajectories (Nagin, 2005). Individuals with missing information were not excluded from the model due to trajectory modeling ability based on lost data manipulation groups using maximum likelihood estimation. However, total sleep duration trajectories were created considering only individuals with at least two time points of total sleep data and those with outcome data at 11 years (n = 3,376) to obtain more plausible trajectories.
Sleep disturbances
Sleep disturbance variables were intended to indicate behaviors that may increase the risk of future sleep problems. The following variables collected at the 24- and 48-month follow-ups were employed: The child has trouble going to sleep (yes/no), the child has nightmares/night terrors (yes/no), and the child has restless sleep (yes/no). These variables were already reported as good indicators of sleep problems in infancy in previous studies (Netsi et al., 2017; O’Connor et al., 2007).
Potential Confounding Factors
The following covariates, collected at the perinatal study (cohort baseline), were used for adjustment in multivariable analyses: wealth index (continuous score), maternal schooling (complete years), maternal age (complete years), maternal marital status (single or married/living with someone), maternal skin color (White, Black, or Other—including Brown, Yellow, or Indigenous), parity (number of previous live births or stillbirths, categorized as <2 and ≥2), maternal alcohol (yes/no) and tobacco (yes/no) use in pregnancy, maternal reported nervous or depression symptoms in pregnancy (yes/no), C-section (yes/no), child sex (male/female), birth weight (evaluated by calibrated electronic scale), and gestational age (considering <37 weeks as preterm birth).
The wealth index (an indicator of material living standards) considers the possession of durable consumer goods (e.g., television, car, computer, and stoves) and household characteristics (e.g., number of toilets) and is constructed through principal components analysis. For our analyses, the first component was selected and categorized in quintiles (Barros & Victora, 2005). Continuous variables were maintained in their original form for multiple regression models, and when we used these variables to describe our sample, we categorized them for a better comprehension.
Data Analysis
All analyses were conducted using Stata software (Version 14.0) and a significance level of 5%. We describe variables with a normal distribution using the mean and standard deviation (SD). For numerical variables with asymmetric distribution, we used medians and interquartile range (IQR), and for nominal variables, we used percentages. Bivariate analyses (chi-square tests and t tests, depending on the type of variables) were conducted to explore the relationship between sleep exposures and ADHD at different time points. Crude and adjusted logistic regression models were used to assess the strength of the association between sleep variables and ADHD at 11 years, independently of confounding factors, to test our Hypotheses 1 and 2:
We also conducted a complementary analysis to test whether sleep duration and problems would be specific to ADHD:
Secondary Analysis
As a secondary analysis, we assessed inattention/hyperactivity problems evaluated by the Strengths and Difficulties Questionnaire (SDQ) as a secondary outcome. The SDQ is a screening questionnaire applied with the DAWBA, and it measures 25 psychological attributes divided into five scales: Inattention/Hyperactivity Symptoms, Conduct Problems, Emotional Symptoms, Peer Relationship Problems, and Prosocial Behavior. The questionnaire was adapted and previously validated for the Brazilian population of children and teenagers aged between 4 and 16 years (Fleitlich-Bilyk & Goodman, 2004). We used the cutoff points established for the Brazilian population to categorize the screening for inattention/hyperactivity problems (≥7) and total emotional/behavior difficulties (≥17). To test a hypothesis of a specificity effect, we created a variable with three categories, namely, “no other emotional/behavior difficulty,” “inattention/hyperactivity problems,” and “another emotional/behavior difficulty,” and used the same models described above.
Ethics
The study protocol and all follow-ups of the 2004 Pelotas Birth Cohort Study were approved by the Medical Ethics Committee of the Federal University of Pelotas, which is affiliated with the Brazilian National Commission for Research Ethics (Comissão Nacional de Ética em Pesquisa). Written informed consent was obtained from the mothers or legal guardians of the adolescents. At the 11-year follow-up, adolescents also signed an informed consent form.
Results
Following the eligibility criteria, 111 participants (84 twins and 27 with syndromic cases) were excluded from this study. A total of 3,466 participants were included in the analysis, yielding a response rate of 86.05% for mental health outcomes at the 11-year follow-up among the 4,028 living and eligible participants. A total of 144 adolescents were diagnosed with ADHD using the DAWBA (4.0%). Approximately half of our sample were boys (51.7%) and were born by C-section (44.8%). The prevalence of low birth weight and prematurity was 8% and 13%, respectively. Mothers were mostly married (80.5%) and had White skin color (73.2%) and two or more children (60.4%). Although 26.8% of mothers smoked during pregnancy, few reported alcohol consumption during this period (3.2%). Approximately 25% of the mothers reported being depressed or nervous during pregnancy (Table 1). Children not included in the sample due to missing data were from poorer and less educated mothers. Mothers in the analyzed sample were older than those not included (≥35 years old, 13.9% vs. 9.6%, respectively) and less depressive than the nonrespondents (24.0% vs. 30.1%, respectively) (Table 1).
Comparison of Maternal and Birth-Related Characteristics Between 2004 Pelotas Birth Cohort Participants Included and Not Included in Analyses Due to Missing Data.
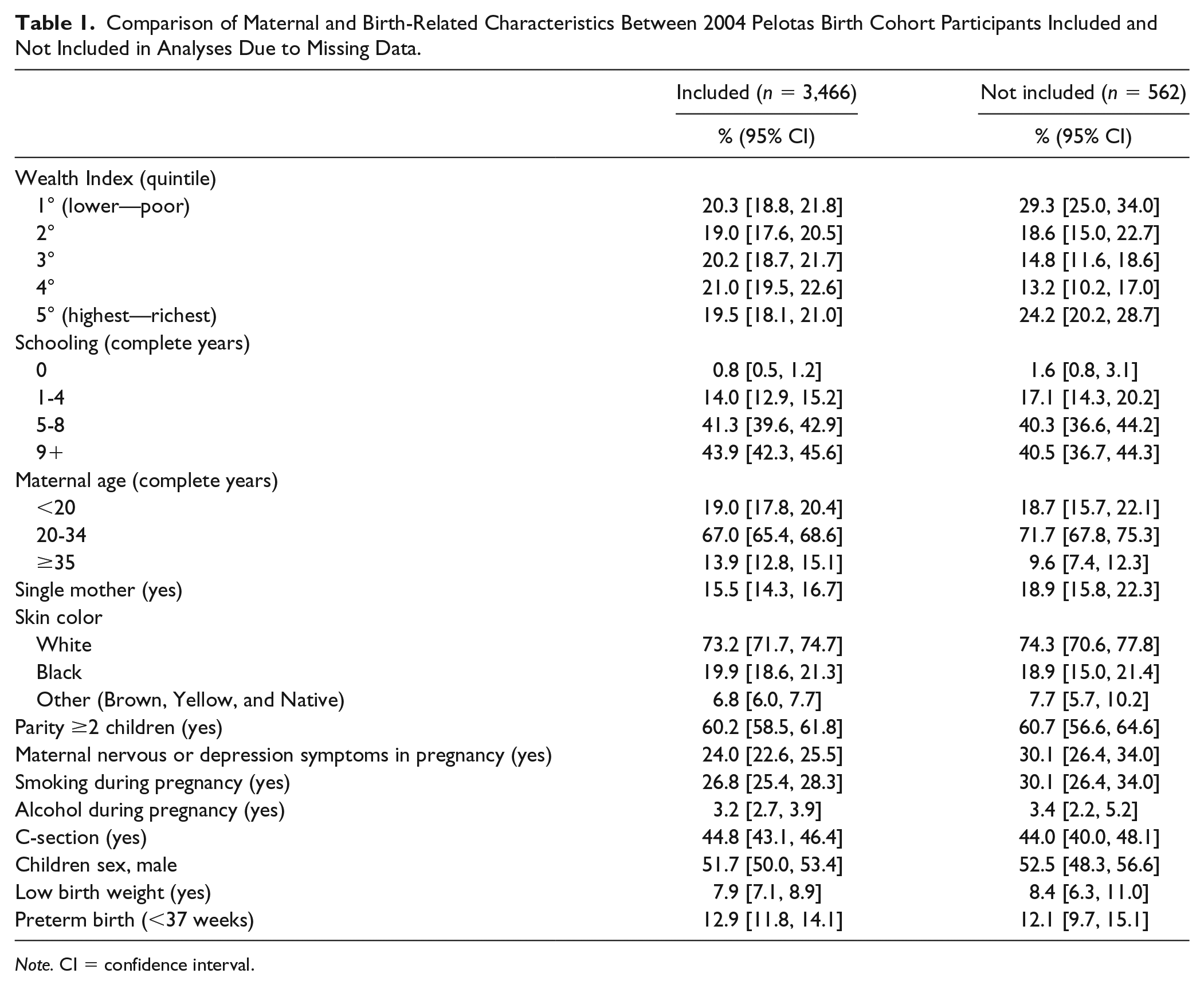
Note. CI = confidence interval.
Sleep Variables Description
Table 2 presents the descriptive statistics for the sleep variables. As age increases, the mean for total sleep duration decreases, and the mean for nighttime sleep duration increases. Daytime sleep duration had an asymmetric distribution, and the median also decreased as age increased. The frequency of sleep problems decreased as age increased for the overall sample, except for restless sleep in the ADHD groups.
Sleep Variables for the Whole Sample of the 2004 Pelotas Birth Cohort (Pelotas, Brazil), Stratified According to ADHD Status at 11 Years of Age.
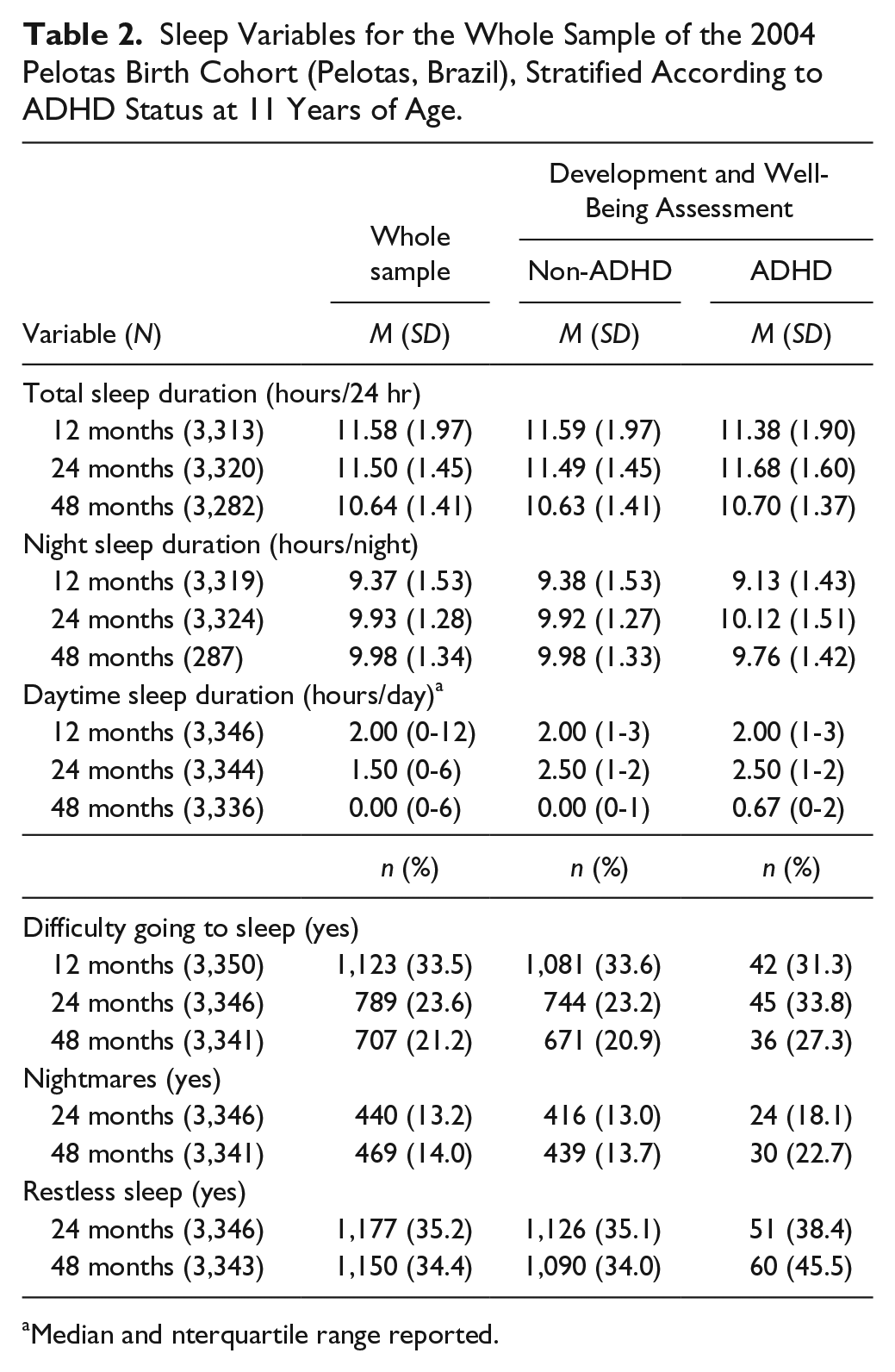
Median and nterquartile range reported.
For the total sleep trajectories, data were used from 3,376 participants. Trajectories were constructed with quadratic models and showed an adequate average posterior probability (more than 70% for each trajectory; Supplemental Table S1). We obtained three groups, namely, longer sleepers (12.8%), typical sleepers (79.0%), and shorter sleepers (8.2%), and their differences seem to be more important at the beginning of life (Supplemental Figure S1). Family wealth index (p = .014), schooling (p < .001), depression during pregnancy (p = .003), smoking during pregnancy (p = .016), and other sleep variables (all p values <.05) were associated with the trajectory groups, thus making these groups more plausible.
Total Sleep Duration Trajectories, Sleep Duration Variables, and ADHD
Total sleep duration trajectories were not associated with ADHD (Table 3). With respect to individual sleep duration variables, only longer daytime sleep duration at 48 months was associated with a higher odds of ADHD at 11 years old (odds ratio [OR] = 1.28, 95% confidence interval [CI] = [1.06, 1.53]). The other sleep duration variables were not associated with ADHD in the adjusted model (Table 4). The SDQ results also showed a lack of association for most of the sleep duration variables in the adjusted model. Only a marginal association was observed between short nighttime sleep at 48 months and inattention/hyperactivity problems (Supplemental Table S2).
Association Between Early Life Total Sleep Duration Trajectory Groups and ADHD, as Assessed by the Development and Well-Being Assessment, at 11 Years of Age in the 2004 Pelotas Birth Cohort.

Note. OR = odds ratio; CI = confidence interval.
Unadjusted analysis.
Maternal and birth-related characteristics adjustment: family wealth index, maternal age, maternal schooling, maternal marital status, maternal skin color, parity, alcohol intake and smoking during pregnancy, maternal nervous or depression symptoms in pregnancy, gestational age, C-section, child sex, and birth weight.
Association Between Sleep Variables and ADHD, as Assessed by the Development and Well-Being Assessment, at 11 Years of Age in the 2004 Pelotas Birth Cohort.
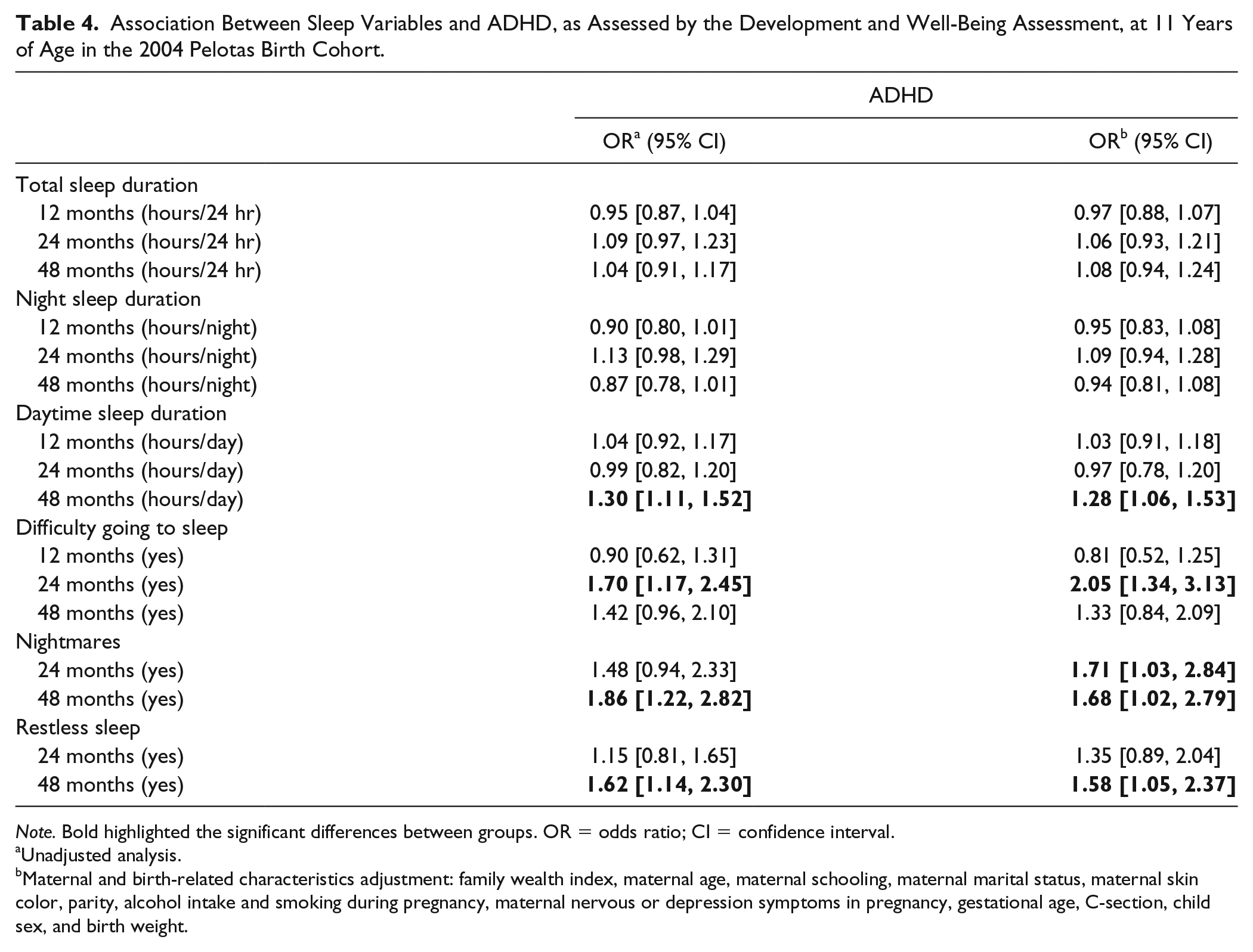
Note. Bold highlighted the significant differences between groups. OR = odds ratio; CI = confidence interval.
Unadjusted analysis.
Maternal and birth-related characteristics adjustment: family wealth index, maternal age, maternal schooling, maternal marital status, maternal skin color, parity, alcohol intake and smoking during pregnancy, maternal nervous or depression symptoms in pregnancy, gestational age, C-section, child sex, and birth weight.
Sleep Problems and ADHD
Overall, most of the sleep problem variables were associated with ADHD after adjustment for covariates (Table 4). The risk of having ADHD was greater among those who presented difficulty in going to sleep at 24 months (OR = 2.05, 95% CI = [1.34, 3.13]), those who had restless sleep at 48 months (OR = 1.58, 95% CI = [1.05, 2.37]), and those who had nightmares at both 24 months (OR = 1.70, 95% CI = [1.28, 2.25]) and 48 months (OR = 1.60, 95% CI = [1.21, 2.12]) (Table 4). In the SDQ assessment, difficulty going to sleep at 24 months and having nightmares and restless sleep at both 24 and 48 months were associated with inattention/hyperactivity problems after adjustment for covariates (Supplemental Table S2).
Specificity Analysis
According to the DAWBA, 86.8% of the sample presented no psychopathology, while 9.2% had any other mental disorder (despite ADHD). The multinomial logistic regression showed that there was no association between sleep duration and other mental problems at any point after adjustment (Table 5 and Supplemental Table S3). On the contrary, sleep problem variables were associated with the presence of other mental issues in the adjusted model. Having difficulty going to sleep at the 24-month follow-up, having restless sleep at the same age, and having nightmares at the 24- and 48-month follow-ups were risk factors for having other mental disorders compared with typical development (Table 5). We also observed the association between having any other mental condition and difficulty going to sleep at 24 months and nightmares at 24 and 48 months, with respect to the SDQ outcome (Supplemental Table S4). The results observed for the ADHD group in the multinomial analyses were virtually the same as those found in the main analyses. They were omitted from the main text to facilitate the presentation of the data, but they are shown in Supplemental Table S4.
Association Between Sleep Variables and Any Mental Disorders Other Than ADHD, as Evaluated by the DAWBA, at 11 Years of Age in the 2004 Pelotas Birth Cohort Using Multinomial Logistic Regression.

Note. DAWBA = Development and Well-Being Assessment; OR = odds ratio; CI = confidence interval.
Unadjusted analysis.
Maternal and birth-related characteristics adjustment: family wealth index, maternal age, maternal schooling, maternal marital status, maternal skin color, parity, alcohol intake and smoking during pregnancy, maternal nervous or depression symptoms in pregnancy, gestational age, C-section, child sex, and birth weight; bold highlighted the significant differences between groups. The results including the ADHD group are shown in Supplemental Table S4.
Discussion
Our findings showed a consistent association between sleep problems at 24 and 48 months of age and ADHD in the beginning of adolescence. Regarding sleep duration variables, no consistent association was found with ADHD, although some variables at specific follow-up points were associated with ADHD after adjustment. The long-term sleep duration effect assessed using trajectories was also not associated with ADHD. We also showed that sleep problems may be common to different psychiatric disorders, not only to ADHD.
Our results suggest that sleep disturbances in early life may be more important for ADHD than sleep duration. The associations between ADHD and difficulty going to sleep (Armstrong et al., 2014; Craig, Weiss, Hudec, & Gibbins, 2017; Steinsbekk & Wichstrom, 2015), nightmares (Grünwald & Schlarb, 2017), and restless sleep (Armstrong et al., 2014; Cortese et al., 2005; Sadeh, Pergamin, & Bar-Haim, 2006) have been reported in the literature, which is in accordance with our findings. On the contrary, several studies have suggested an important role of sleep duration in this disorder (Cassoff et al., 2012; Coogan & McGowan, 2017; Scott et al., 2013). We should highlight that our unadjusted analyses showed an association between total sleep duration and ADHD, as has been reported previously. However, most of the sleep duration associations were highly marginal and/or lost significance after adjustment for maternal and birth-related factors, suggesting that this association may result from confounding. This pattern was also observed when we tested the trajectories. The effect did not remain significant after the adjustment, indicating that the trajectories (longitudinal construct) are also not the most important factors in future ADHD. Indeed, although the literature shows the association between sleep duration and ADHD, most of the previous studies presented no adjusted analyses or utilized an insufficient/inadequate control method (Scott et al., 2013; Williams & Sciberras, 2016). Although we cannot rule out the potential role of unfavorable sleep–wake behavior or variability in sleep schedules, which have already been reported in ADHD (Craig et al., 2017; Scott et al., 2013; Thoma et al., 2018), for the few associations observed for shorter nocturnal and greater daytime sleep duration at 48 months, confounding seems to be an important issue in the current literature. Future studies should more thoroughly explore this issue to report adequate estimates.
The differential roles of sleep duration and problems with ADHD still need to be clarified in terms of mechanisms. The current hypotheses that explain the link between sleep issues and ADHD are mainly based on the impairment of the prefrontal cortex and frontal functions, dopamine neurotransmission, and circadian rhythm control (Cassoff et al., 2012; Um et al., 2017). An impact of sleep quality and duration on brain executive control and emotional information processing has already been observed (Sadeh et al., 2014; Um et al., 2017; Wright, Lowry, & LeBourgeois, 2012), which may explain the neurobehavioral, neurocognitive, and functional manifestations of ADHD symptomatology (Lunsford-Avery, Krystal, & Kollins, 2016; Mahone & Denckla, 2017; Pievsky & McGrath, 2018). Moreover, both executive functions and sleep are regulated by prefrontal cortex function and dopaminergic activity (Cassoff et al., 2012; Mahone & Denckla, 2017; Wright et al., 2012; Zee et al., 2013), providing a mechanism linking both traits. Impairment in synaptic plasticity, an increase in hippocampal oxidative stress, and the facilitation of neuronal loss were already observed in response to sleep deprivation, which affect neurocognitive function and provide similar symptomatology to ADHD (Um et al., 2017). Other sleep conditions, however, do not have a clear underlying pathway. Recently, genome-wide association studies have indicated that the genetic markers of insomnia and sleep duration are not the same (S. E. Jones et al., 2016), although a negative genetic correlation between the traits was observed (Jansen et al., 2018; Lane et al., 2017). In this sense, it is necessary to understand the biological pathways affected by sleep disturbances and sleep duration to comprehend their relationship with ADHD etiology.
The lack of specificity observed in our study of the effects of sleep problems on ADHD suggests that sleep problems could not be considered early markers or endophenotypes of ADHD as a unique mental condition and a means of early detection, as has been stated in the literature (Sadeh et al., 2014; Um et al., 2017; Williams & Sciberras, 2016). On the contrary, Williams and Sciberras (2016) highlighted that sleep problems in children with and without ADHD precede emotional dysregulation, and even though early sleep problems are not a specific marker of ADHD, treating these sleep problems may contribute to reduced attentional dysfunction and prevent ADHD as well as other mental conditions. Importantly, sleep problems are also reported in adults with ADHD (Díaz-Román et al., 2018), suggesting that the association observed here may be persistent across development. Therefore, we can consider sleep problems an important issue in ADHD, even when there is no specific effect observed. Detecting and treating precociously may be an important issue in preventing or attenuating ADHD symptoms.
Our results should be interpreted in the context of some limitations. First, we do not have data on sleep at 11 years and ADHD evaluation (or a proxy) at 48 months, making it impossible to test other hypotheses, such as the bidirectional relation, as other studies have mentioned (Gregory et al., 2017; Steinsbekk & Wichstrom, 2015), and the potential causality of sleep problems on ADHD. However, a clinical trial found that the effect of its intervention on ADHD symptoms was mediated through improved sleep problems in the intervention group (Hiscock et al., 2015), indicating that even when ADHD symptoms may bring forth sleep problems, sleep hygiene interventions may be an alternative/complementary treatment to ADHD. With respect to the trajectory, it is important to highlight that the trajectory of our longer trajectory group is longer compared with our own data (Nagin & Tremblay, 2005) but not compared with the recommended sleep time at 24 and 48 months. In other words, children in this group sleep more than the recommended amount only during the 12 months, and after this point, they sleep the recommended amount of time (Hirshkowitz et al., 2015). However, the observed sleep trajectory is very similar to the pattern reported by other studies in the sleep field (Bathory & Tomopoulos, 2017), indicating that there are persistent groups of shorter, longer, and typical sleepers, with the differences decreasing with increasing age, enhancing the reliability of our findings. Moreover, although there is a difference between respondents and nonrespondents, which may be considered a limitation, the response rate is high, and only a few differences were observed. Finally, both sleep and mental health outcomes are evaluated only by mothers’ reports, which may have an impact on the prevalence, as caregivers’ perceptions may affect their reports. However, in population-based studies, especially in this age range, parental reports are the most feasible. In addition, most of the studies also evaluated the exposure and outcome by maternal report, providing us with more comparability.
Nevertheless, we focused on sleep and ADHD data in a large population-based birth cohort in Brazil, including assessments at several time points during childhood and a high follow-up rate, which are study characteristics that are still lacking in the literature (Cortese, 2015; Cortese et al., 2005; Lunsford-Avery et al., 2016; Um et al., 2017). Moreover, we administered a comprehensively validated diagnosis instrument on all cohort participants to detect ADHD cases (Fleitlich-Bilyk & Goodman, 2004), which is an important addition to the current literature (Cortese et al., 2009; Díaz-Román et al., 2016). These points can be considered strengths of our data; no previous study has performed this type of comprehensive analysis. We used this robust methodology to explore the effect of each follow-up time point as well as the total sleep duration trajectory effect on ADHD. We also addressed possible maternal and child confounders, which have not been thoroughly studied previously. Furthermore, the specificity analysis adds important information to the literature.
Finally, our findings indicate that sleep problems in early life may be more important than sleep duration for the ADHD etiology. The results of the specificity analyses suggest that sleep disturbances may be considered as a common early marker of psychiatric disorders in general and not only a marker of ADHD. This study shows that the relationship between sleep/circadian rhythms and ADHD may be more complex than previously shown by other empirical studies. Further research exploring temporality and sleep trajectories in the sleep–ADHD association as well as studies exploring the specificity of this relationship are still necessary to narrow this gap in the literature.
Supplemental Material
supplementary_material – Supplemental material for The Role of Sleep Duration and Sleep Problems During Childhood in the Development of ADHD in Adolescence: Findings From a Population-Based Birth Cohort
Supplemental material, supplementary_material for The Role of Sleep Duration and Sleep Problems During Childhood in the Development of ADHD in Adolescence: Findings From a Population-Based Birth Cohort by Marina Xavier Carpena, Tiago N. Munhoz, Mariana Otero Xavier, Luis Augusto Rohde, Iná S. Santos, Bianca Del-Ponte, Fernando C. Barros, Alicia Matijasevich and Luciana Tovo-Rodrigues in Journal of Attention Disorders
Footnotes
Authors’ Note
This article is based on data from the study “Pelotas Birth Cohort, 2004” conducted by Postgraduate Program in Epidemiology at Universidade Federal de Pelotas, with the collaboration of the Brazilian Public Health Association (ABRASCO).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Luis Augusto Rohde has been a member of the speakers’ bureau/advisory board and/or acted as a consultant for Eli-Lilly, Janssen-Cilag, Medice, Novartis and Shire in the last three years. He receives authorship royalties from Oxford Press and ArtMed. He has also received travel awards from Shire for his participation in the 2017 WFADHD meetings and from Novartis to take part of the 2016 AACAP meeting. The ADHD and Juvenile Bipolar Disorder Outpatient Programs chaired by him received unrestricted educational and research support from the following pharmaceutical companies in the last three years: Janssen-Cilag, Novartis, and Shire.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The World Health Organization, National Support Program for Centers of Excellence (PRONEX), Brazilian National Research Council (CNPq), Brazilian Ministry of Health, and Children’s Pastorate supported previous phases of the study until 2009. The 11-year follow-up was supported by the Science and Technology Department/Brazilian Ministry of Health, with resources transferred through the Brazilian National Council for Scientific and Technological Development (CNPq), Grant Number 2400943/2013-1. This follow-up was also funded by the São Paulo Research Foundation (FAPESP; Grant Number 2014/13864-6). This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001. M.X.C., A.M., I.S.S., and L.T.-R. are supported by the CNPq (National Council for Scientific and Technological Development).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.