
Abstract
With the introduction of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013), attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) can now be simultaneously diagnosed. Although the neurobiology of these disorders is still not fully understood, imaging and genetic findings suggest there may be shared neurobiological features that underlie both disorders (Dougherty, Evans, Myers, Moore, & Michael, 2016; Rommelse, Franke, Geurts, Hartman, & Buitelaar, 2010). Although about one in eight children with ADHD meet criteria for ASD (Zablotsky, Bramlett, & Blumberg, 2017), a greater number (up to half) display symptoms of ASD that do not reach diagnostic threshold (Mulligan et al., 2009).
Children with ADHD and symptoms of ASD have been shown to have substantially impaired functioning compared with those with ADHD alone (Cooper, Martin, Langley, Hamshere, & Thapar, 2014; Green, Sciberras, Anderson, Efron, & Rinehart, 2016; Kotte et al., 2013). For example, ASD symptoms in children with ADHD have been associated with more peer relationship difficulties (Green et al., 2016; Kotte et al., 2013), increased oppositional behavior, depression, and anxiety symptoms (Cooper et al., 2014; Green et al., 2016; Grzadzinski et al., 2011; Kotte et al., 2013), and a greater likelihood of comorbid conditions such as oppositional defiant disorder and conduct disorder (Mulligan et al., 2009).
There are three symptom domains that are important when considering an ASD diagnosis (communication, reciprocal social interaction, and repetitive and stereotyped behaviors). To the best of our knowledge, only one study has examined the association between individual symptom domains of ASD and functioning in children with ADHD (Cooper et al., 2014). The study used the Social Communication Questionnaire to examine whether ASD symptom severity was associated with a more severe ADHD presentation in a sample of 711 children with ADHD aged 5 to 18 years. Analyses examining individual ASD symptom domains showed repetitive stereotyped behaviors were independently associated with both anxiety and hyperactive/impulsive symptoms, whereas social interaction deficits were more associated with oppositional defiant disorder symptoms (Cooper et al., 2014). However, this study did not examine the association between ASD symptoms and the broader emotional and peer functioning of children with ADHD. Such knowledge is important to tailoring the management of ADHD when accompanied by symptoms of ASD.
This study aimed to examine whether specific ASD symptom domains (communication, reciprocal social interaction, and repetitive and stereotyped behaviors) were associated with the following outcomes: peer problems, mental health, and quality-of-life functioning in children with ADHD.
Method
Participants
The sample consisted of 164 children with ADHD aged between 6 and 10 years of age, 7.9 (SD = 1.08) years, 50 females and 114 males, who were participating in the Children’s Attention Project (Green et al., 2016; Sciberras et al., 2013). Twenty-seven participants were taking medication for ADHD management.
Children were recruited from 43 Melbourne primary schools during their second year of schooling in 2011 (Cohort 1) and 2012 (Cohort 2) (Wave 1). In the first stage of recruitment, the Connors 3 ADHD indices (Conners, Erhardt, & Sparrow, 1999) were distributed across all schools when children were in Grade 1 (second year of primary school) and completed by both the child’s parent and teacher. A child was deemed a positive screen if they met ADHD symptom thresholds on both the parent and teacher indices. Children with a parent-reported ADHD diagnosis were also considered to have screened positive. In the second stage of recruitment, the Diagnostic Interview Schedule for Children version 4 (DISC-IV) (Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000) was completed with parents to determine the presence or absence of ADHD. If children had a positive diagnosis at the interview, the child was allocated to the ADHD group. For each child recruited into the ADHD group, a control child, matched on age and sex was also recruited. The families were followed up again at 18 months postrecruitment (Wave 2). Written consent from the parent was obtained for all participants. Children with an intellectual disability or serious medical condition were excluded, as well as parents who lacked sufficient English to complete questionnaires.
Measures
ADHD status was confirmed using the DISC-IV (Shaffer et al., 2000). The interview was conducted with the parent and was also used to identify the presence of other externalizing and internalizing disorders. Modules for depression, generalized anxiety disorder, social phobia, post-traumatic stress disorder, and mood disorders were used to assess internalizing disorders. Modules for oppositional defiant disorder and conduct disorder were administered to assess for externalizing disorders. The DISC-IV has been shown to have good diagnostic reliability in community samples (Shaffer et al., 2000).
The severity of ASD symptoms was measured dimensionally using the Social Communication Questionnaire (SCQ) (Berument, Rutter, Lord, Pickles, & Bailey, 1999). The SCQ is a 40-item parent-reported measure, consisting of three subscales assessing the ASD domains; communication, reciprocal social interaction, and repetitive and stereotyped behaviors. It corresponds well with gold standard ASD diagnostic measures and has high discriminant validity (Berument et al., 1999).
Social and emotional functioning was measured using the Strength and Difficulties Questionnaire (SDQ) (Hawes & Dadds, 2004). This was completed by both the child’s parent and teacher. In this study the five-item emotional problems, peer problems, prosocial behavior, and conduct problems subscales were used. Moderate-to-strong internal reliability has been found for all subscales of the SDQ, with the external validity being strong (Hawes & Dadds, 2004).
The child’s quality of life was assessed using the Pediatric Quality of Life Inventory 4.0 (PedsQL4.0) (Varni, Burwinkle, & Seid, 2006), which was completed by the parent. The PedsQL4.0 consists of 23 items across four subscales (physical functioning, emotional functioning, social functioning, and school functioning). Strong reliability and validity have been found across all subscales as well as the total scale score (Varni et al., 2006).
Procedure
Ethics approval was obtained from the Human Research and Ethics Committee at both The Royal Children’s Hospital (#31056) and Deakin University (#2016-396) in Melbourne, Australia. Informed written consent was obtained from the primary caregiver.
For Cohort 1, the SCQ was completed over the telephone with parents at Wave 2. For Cohort 2, the SCQ was completed via questionnaire as part of the Wave 1 face-to-face assessment. A research assistant with a minimum 4-year study sequence in psychology administered the DISC-IV and the SCQ for children in both cohorts, and there was no difference of the collection of the data besides the mode of assessment (telephone vs. face-to-face). Other measures (SDQ and PedsQL) were collected as part of the parent and teacher completed surveys at Wave 1.
Statistical analysis
Total SCQ score was converted into standard deviation units to assist interpretation. Adjusted linear regression was used to examine the association between SCQ symptom domains and child functioning outcomes (peer problems, mental health, and quality of life). The three SCQ subscales were first examined separately to determine whether the ASD symptom domains were associated with child functioning. Variables adjusted for in these models comprised of child factors (age, sex, internalizing disorder, externalizing disorder, recruitment cohort, and ADHD symptom severity), school factors (school clustering), and family factors (parent high school completion and Socio-Economic Indexes for Areas Disadvantage Index; Australian Bureau of Statistics, 2011).
Scores on the communication, reciprocal social interaction, and restricted and stereotyped behaviors subscales were then entered simultaneously as independent variables and examined in relation to each functional outcome in separate linear regression models, which also adjusted for the variables described above. All analyses were conducted using Stata 13. An alpha level of .05 was used to determine statistical significance.
Results
ASD Subdomains Analyzed in Separate Regressions
All SCQ subscales were associated with poorer peer problems irrespective of measure or reporter (Table 1). The only exception was that none of the symptoms domains were associated with teacher-reported SDQ prosocial behavior.
Adjusted Associations Between ASD Symptom Domains and Child Functioning Outcomes for Children With ADHD Using Separate Regressions for Each Domain.
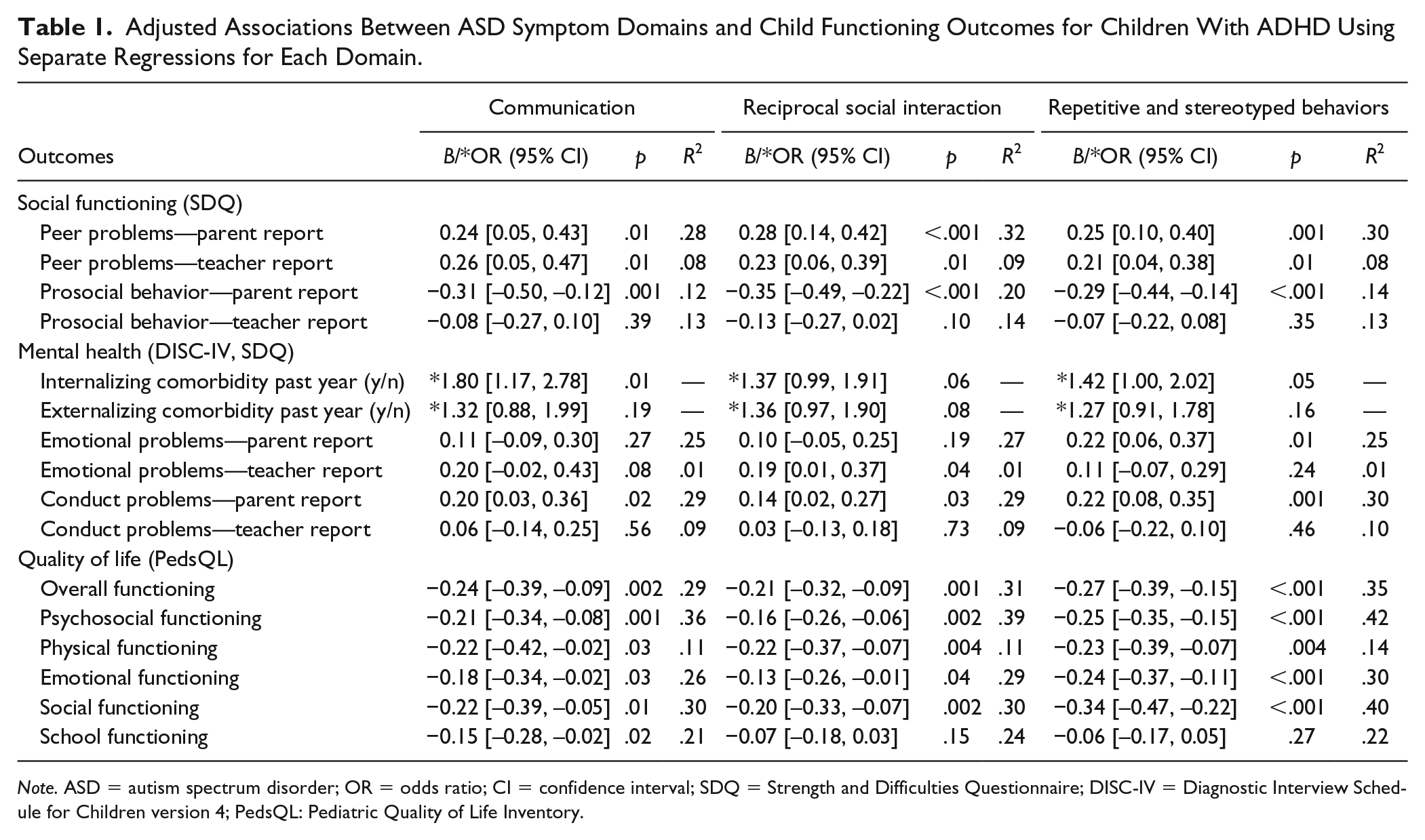
Note. ASD = autism spectrum disorder; OR = odds ratio; CI = confidence interval; SDQ = Strength and Difficulties Questionnaire; DISC-IV = Diagnostic Interview Schedule for Children version 4; PedsQL: Pediatric Quality of Life Inventory.
SCQ communication symptoms (p = .01) and repetitive and stereotyped behaviors (p = .05) were both associated with greater odds of a DISC-IV internalizing comorbidity in the past year. In contrast, odds of a DISC-IV externalizing comorbidity were unrelated to communication and repetitive and stereotyped behaviors symptom domains; however, there was some evidence of a relationship for reciprocal social interaction (p = .08). Parents reported greater SDQ conduct problems in children with greater symptoms for all SCQ domains; communication (p = .02), reciprocal social interaction (p = .03), and repetitive and stereotyped behaviors (p = .001); however, teacher-reported SDQ conduct problems were unrelated to ASD symptom domains.
Greater SDQ emotional problems were related to greater SCQ repetitive and stereotyped behaviors when reported by parents (p = .01), yet were related to reciprocal social interaction symptoms when reported by teachers (p = .04).
ASD Symptom Domains Analyzed Together
When all three SCQ subscales were analyzed simultaneously (Table 2), there were no independent associations between SCQ communication symptoms and measures of child functioning.
Adjusted Associations Between ASD Symptom Domains and Child Functioning for Children With ADHD With All Domains Considered Together.

Note. ASD = autism spectrum disorder; OR = odds ratio; CI = confidence interval; SDQ = Strength and Difficulties Questionnaire; DISC-IV = Diagnostic Interview Schedule for Children version 4; PedsQL: Pediatric Quality of Life Inventory.
SCQ reciprocal social interaction symptoms were independently associated with higher parent-reported peer problems (p = .03) and lower prosocial behaviors (p = .004). No other independent associations were evident.
SCQ restricted and stereotyped behavior symptoms were independently associated with greater parent-reported conduct (p = .03) and emotional problems (p = .02), and poorer quality of life on the PedsQL including overall (p = .004), psychosocial (p < .001), emotional (p = .004), and social (p < .001) subscales.
The odds of a DISC-IV internalizing or externalizing comorbidity in the past year were unrelated to all SCQ symptoms domains. No significant associations between SCQ symptom domains and measures of child functioning were found for teacher-reported measures.
Discussion
ASD symptoms in children with ADHD can have a substantial impact on child functioning. There are three key findings from this study. The first is that reciprocal social interaction deficits independently contribute to peer problems in children with ADHD. The second is that restricted and stereotyped behaviors are independently associated with emotional, conduct, and quality-of-life functioning in children with ADHD. Finally, communication deficits were not independently associated with functioning in this population. Although the effect size of the associations between ASD domains and aspects of functioning were small, they are important as the associations found were above and beyond ADHD symptomology alone.
ASD symptoms in children with ADHD have been previously linked to social difficulties such as problems with peers (Green et al., 2016; Kotte et al., 2013); however, previous research has not examined which specific ASD symptoms contribute to these difficulties. This study shows that reciprocal social interaction deficits independently contribute to peer problems in children with ADHD after accounting for other ASD symptoms, mental health comorbidities, and even ADHD symptom severity. As children with ADHD have been found to struggle with forming and maintaining friendships (Heiman, 2005; McQuade & Hoza, 2008), it could be that reciprocal social interaction deficits have a compounding effect, thereby exacerbating the existing difficulties seen in this group. There is limited evidence that existing social skills interventions vastly improve social functioning in children with ADHD (Mikami, Miller, & Lerner, 2019). Considering the social difficulties experienced by children with ADHD through an ASD lens may be a productive avenue for future intervention research (Mikami et al., 2019).
The current findings demonstrate that in children with ADHD, restricted and stereotyped behaviors are independently associated with emotional functioning. This finding is consistent with the one previous study in the area, which found that restricted and stereotyped behaviors were independently associated with anxiety symptoms in children with ADHD (Cooper et al., 2014). The association between restricted and stereotyped behaviors and anxiety has been researched in ASD populations; however, the direction of the link is still unclear. In children with ADHD, it could be possible that the higher levels of restricted and stereotyped behaviors, such as repetitive thoughts or worries, may be resulting in the higher levels of emotional problems reported (such as “worries a lot” and “many fears or easily scared”). Alternatively, it may be that children with ADHD and ASD symptoms experience higher levels of emotional problems and use restricted and stereotyped behaviors as a way to reduce this.
Previous research has reported an association between higher ASD symptoms and comorbid conduct disorders in children with ADHD (Cooper et al., 2014; Mulligan et al., 2009). Our study extends this finding by demonstrating that restricted and stereotyped behaviors symptoms were independently associated with parent-reported conduct problems. It is possible that repetitive and stereotyped behaviors (such as SCQ item: complicated movements of the body) may worsen during temper tantrums or when fighting with other children, leading to parents rating them more highly on measures of conduct problems.
This study is also the first to investigate how ASD symptom domains affect quality of life in children with ADHD. It is evident that repetitive and stereotyped behavior symptoms have a significant impact on quality of life, affecting multiple aspects including psychosocial, emotional, and social quality of life. These findings may have implications for future interventions as directly targeting this ASD symptom domain may result in an improvement in functioning across these domains thereby improving the quality of life for this group.
A strength of this study is that it included a large, community-based sample of children with ADHD. The study included a rigorous two-stage ADHD assessment process and included a relatively large sample of girls when compared with previous ADHD research. One limitation of the study is that the SCQ is not a diagnostic measure of ASD symptoms, and it was collected at a separate time point to the ADHD screening process for Cohort 1. Although adjusted for in the analyses, it is possible that ADHD symptoms or severity could have changed in the 18 months between the ADHD screening and administration of the SCQ in this cohort.
Conclusion
This study demonstrates that individual ASD symptom subdomains are associated with poorer functioning in children with ADHD, with reciprocal social interaction deficits affecting peer relationships, and repetitive and stereotyped behaviors affecting multiple domains of functioning including quality of life. Given the unique impact that repetitive and stereotyped behaviors can have on aspects of functioning, further research is needed to consider whether interventions specifically targeting this domain can improve functioning in this group of children.
Footnotes
Author’s Note
Timothy J. Silk and Emma Sciberras are also affiliated with University of Melbourne, Victoria, Australia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Project Grants from the Australian National Health and Medical Research Council (NHRMC) (1065895 and 1008522), the Murdoch Children’s Research Institute (MCRI), and the Collier Foundation. Associate Professor Emma Sciberras was funded by an NHMRC Career Development Fellowship (1110688: 2016-21) and a veski Inspiring Women Fellowship. Dr. Efron was funded by a Clinician Scientist Fellowship from the MCRI. Professor Jan M. Nicholson was funded by the Australian Communities Foundation (Coronella sub-fund) at La Trobe University. Professor Vicki Anderson was supported by an NHMRC Senior Practitioner fellowship. MCRI was supported by the Victorian Government’s Operational Infrastructure Support Program.