
Abstract
Introduction
ADHD is a neurodevelopmental disorder that can persist into adulthood and has an estimated prevalence of 2.5% in adults (Simon et al., 2009). Patients with ADHD have a persistent pattern of inattention and/or hyperactivity/impulsivity, which can lead to impairments in their academic, professional, and social functioning (Karlsdotter et al., 2016). These impairments have a substantial personal (Garcia et al., 2012) and economic impact (Doshi et al., 2012). Although pharmacotherapy with stimulants is the first-line treatment for ADHD patients with moderate or severe levels of impairment, current guidelines do recommend a multimodal treatment for ADHD, also including psychological interventions (Kooij et al., 2019; National Institute for Health and Care Excellence, 2018).
Recent evidence demonstrates that psychosocial treatments can have additional effects to pharmacotherapy in alleviating residual symptoms in adults with ADHD (Cairncross & Miller, 2020; Hoxhaj et al., 2018; Vidal et al., 2013; Young et al., 2020). Mindfulness-based interventions (MBIs) are among the promising psychosocial treatments for ADHD. Mindfulness is defined as intentionally paying attention to present moment experiences in an accepting, nonjudgmental way (Kabat-Zinn, 1990). During the mindfulness exercises, such as body scan, sitting meditation, and mindful movement, participants learn to repeatedly bring their attention back to the experiences of the present moment. This experiential approach should allow participants to become more aware of their thoughts, feelings, bodily sensations, and, in time, it should enable them to recognize and gain insight into their behavioral patterns. By acknowledging their experiences and being able to regulate their attention, participants then can consciously choose how to respond to a stressor rather than automatically react to it (Segal et al., 2002). In addition, as participants learn mindfulness skills, they learn to give less authority to self-judgment and blame and to respond to these states with compassion (Feldman & Kuyken, 2011). Indeed, in systematic reviews, mindfulness training has been related, next to improvement in mindfulness skills, to improvement in self-compassion and specific domains of executive functioning (Alsubaie et al., 2017; Gu et al., 2015; Kuyken et al., 2010; Lao et al., 2016).
Currently, the evidence for MBIs for ADHD in adults is growing. A first quantitative review including three studies on adults with ADHD yielded preliminary evidence for their effectiveness in reducing ADHD symptoms with moderate to large effect sizes (Cairncross & Miller, 2020). However, these findings should be interpreted with caution, as the included studies either lacked randomization, were underpowered, and/or lacked a follow-up period (Edel et al., 2017; Mitchell et al., 2017; Schoenberg et al., 2013). More recently, based on findings of another randomized controlled trial (RCT) that showed improvements for ADHD patients after an MBI (Hepark et al., 2015) and an additional mixed-methods study (Janssen et al., 2020), we conducted a well-powered RCT, demonstrating that mindfulness-based cognitive therapy (MBCT) in addition to treatment as usual (TAU) was more effective than TAU alone in reducing core ADHD symptoms and improving positive mental health up till 6-month follow-up (Janssen et al., 2018).
In addition to examining the clinical effectiveness of MBCT, there is also a need to understand the mechanisms of change underlying the beneficial effects of MBCT (Dimidjian & Segal, 2015). Gaining a deeper understanding of the mechanisms through which interventions bring about change will enable us to refine and optimize the MBCT program, which might increase its potency (Kazdin, 2007). Regarding ADHD, the aims of MBIs might be twofold. First, by directly targeting the ADHD symptoms. Second, by helping patients manage their symptoms more effectively and relate to their suffering in a compassionate manner. Regarding the former, MBIs seem valuable because practicing mindfulness meditation can improve the underlying neuropsychological deficits related to attention regulation and other executive functions such as inhibition and working memory (Chiesa et al., 2011; Gallant, 2016; Lao et al., 2016, but see Vago et al., 2019). In line with this, neuroscientific studies showed that mindfulness meditation may be associated with structural and functional changes in brain areas responsible for the regulation of attention and emotion (Fox et al., 2014, 2016; Tang et al., 2015). We thus hypothesize that the beneficial effect of MBCT on core ADHD symptomatology might specifically result from treatment-related improvements in mindfulness skills and executive functioning.
Instead of directly alleviating the severity of core symptoms, participation in an MBI might also influence the way patients deal with symptoms, functional impairments and their related history of perceived failure and suffering. Indeed, an important element of cultivating mindfulness is learning to relate in a different way toward one’s experiences, irrespective of the quality or content of these experiences (Bishop et al., 2004). This change of attitude toward symptoms and suffering might account for the wide variety of psychiatric symptoms that show improvement after MBI (Goldberg et al., 2018). By practicing mindfulness, patients are taught to encounter their inner experiences, for example, their physical restlessness, with a curious, open, and accepting attitude instead of being harsh and judgmental toward oneself. This attitude might foster self-compassion, which involves acknowledging one’s pain and recognizing this is part of the human experience while meeting the pain with kindness and understanding (Neff, 2003). Based on these considerations, we hypothesize that the effect of MBCT on positive mental health in adults with ADHD might result from improvements in self-compassion and mindfulness skills.
Regarding the empirical evidence for mechanisms of change, only one preliminary RCT conducted an exploratory mediation analysis, which suggested that mindfulness skills indeed might mediate the effect of MBCT on clinician-rated ADHD symptoms (Hepark et al., 2015). Self-compassion has not been under investigation as a mediator in the ADHD population as of yet. Also, no assessment of mediation of positive mental health improvements has been conducted. Regarding this lack of solid evidence, we set out to further insights in the mechanisms of change of MBCT in adults with ADHD by conducting preregistered (Janssen et al., 2015) mediation analyses on data of a multicenter, parallel-group, randomized controlled superiority trial comparing the effect of MBCT in addition to TAU with TAU alone. Specifically, we assessed whether improvements of mindfulness skills and self-compassion over the course of MBCT indeed predicted improvement in ADHD core symptoms and positive mental health at 6-month follow-up. In addition, we took into account in our analyses that improvements in positive mental health might also be due to improvements in ADHD symptoms. Supplementary, in line with the hypothesis that improvements in ADHD core symptoms at 6-month follow-up might be due to MBCT-induced improvement of specific executive functions, we assessed, although not preregistered, whether specific domains of executive functioning indeed mediated ADHD core symptoms.
Method
Participants
This mediation study was embedded in a multicenter RCT investigating the impact of MBCT in addition to TAU (MBCT + TAU) on adults with ADHD (NCT02463396; Janssen et al., 2018). A total of 120 adults with ADHD were randomized to either MBCT + TAU or TAU only. Patients were assessed at baseline (0 months), posttreatment (3 months), 3-month follow-up (6 months), and 6-month follow-up (9 months). In the present study, we used for our primary analysis the baseline, posttreatment, and 9-month follow-up data. The trial protocol has been published previously (Janssen et al., 2015) and received approval by the medical ethics committee (CMO Arnhem-Nijmegen, 2014/206) for all participating centers. The eligibility criteria, study procedure, and CONSORT diagram are described fully in the main outcome paper (Janssen et al., 2018).
MBCT
The intervention was primarily based on the MBCT protocol (Segal et al., 2002). MBCT is an 8-week group-based intervention with sessions of 2.5 hr each plus a 6-hr silent day between Sessions 6 and 7. The program includes mindfulness practice (body scan, mindful movement, sitting meditation) combined with daily life practices, psychoeducation, cognitive behavioral therapy (CBT) techniques, group discussions, and inquiry into present moment experiences. Participants are invited to practice daily at home for approximately 30 min a day with audio-taped guided exercises. Some modifications to the classical MBCT format were made based on a mixed-method pilot study in adults with ADHD (Janssen et al., 2020). Sessions were led by well-trained mindfulness teachers whose level of competence ranged between beginner and advanced according to the Mindfulness-Based Interventions—Teaching Assessment Criteria (MBI:TAC; Crane et al., 2012).
TAU
TAU reflected the usual treatments of ADHD patients in various mental health centers across the Netherlands, consisting of pharmacotherapy and psychosocial treatment, such as psychoeducation and CBT.
Outcome Measures
Clinician-rated ADHD symptoms
A blinded clinician used the investigator-rated screening version of the 30-item Conners’ Adult ADHD Rating Scale–Investigator Rated: Screening Version (CAARS-INV: SV) to assess ADHD symptoms (Adler et al., 2008). The subscales Inattention and Hyperactivity/Impulsivity were summed to form a total score of Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) symptoms. Internal consistency in the present study was .84.
Positive mental health
The 14-item short form of the Mental Health Continuum (MHC-SF) contains three subscales (Emotional, Psychological, and Social), which were summed to form a total score of positive mental health (Lamers et al., 2011). Internal consistency in the present study was .91.
Potential Mediators
Mindfulness skills
The Dutch validated 24-item short form of the Five Facet Mindfulness Questionnaire (FFMQ-SF) is a reliable and valid alternative to the original FFMQ (Baer et al., 2008), which is based on an exploratory factor analysis of five mindfulness measures to provide an empirical integration of these independent attempts to operationalize mindfulness (Bohlmeijer et al., 2011). The FFMQ-SF consists of five subscales: Observing (α = .76), Describing (α = .81), Acting With Awareness (α = .73), Nonjudging of Inner Experience (α = .76), Nonreactivity to Inner Experience (α = .69). The subscales, as well as the total scale (α = .76), showed adequate to good internal consistency in the present study.
Self-compassion
The Dutch validated, 12-item short form of the Self-Compassion Scale (SCS-SF: Raes et al., 2011) is a reliable and valid alternative to the original SCS (Neff, 2003). Recently, it has been pointed out that the Positive subscales of the SCS (Self-Kindness, Common Humanity, Mindfulness) directly refer to the three key components of self-compassion while the Negative subscales reflect the precise opposite of the key components (self-judgment, isolation, overidentification; Muris & Petrocchi, 2017). Following the authors’ recommendations, we used the Positive and Negative subscales of the SCS to discern the relative contributions of the positive and negative indicators of self-compassion. Both the Positive (α = .81) and Negative (α = .85) subscales, as well as the total scale (α = .87) of self-compassion, showed good internal consistency in the present study.
Executive functioning
The self-report version of the Behavior Rating Inventory of Executive Function–Adult Version (BRIEF-A; Roth et al., 2005) measures executive functioning in daily life. This questionnaire consists of 75 items on a 3-point Likert-type scale and has nine subscales: Inhibit, Shift, Emotional Control, Self-Monitor, Initiate, Working Memory, Plan/Organize, Task Monitor, and Organization of Materials. MBCT did not improve executive functioning significantly from pre- to posttreatment but did improve executive functioning significantly from pre- to 3-month follow-up as reported by Janssen et al. (2018): Specifically, the subdomains Inhibition, Initiate, and Working Memory changed significantly. Therefore, we used the 3-month follow-up data for our supplementary mediation analysis. The Inhibition (α = .66), Shift (α = .72), Emotional Control (α = .87), Self-Monitor (α = .71), Initiate (α = .75), Working Memory (α = .62), Plan/Organize (α = .80), Task Monitor (α = .74), Organization of Materials (α = .85) subscales, and total BRIEF-A scale (α = .92) showed questionable to good internal consistency in the present study.
Statistical Analysis
Analyses were based on the sample of patients who received an adequate treatment dose (treatment-adherent sample), that is, at least four sessions.
Using a bootstrapping method (Hayes & Preacher, 2013), we conducted multiple mediation analyses to examine whether the effect of treatment (MBCT + TAU vs. TAU) on the outcome at 6-month follow-up was mediated by changes, over the treatment, of the mediators. According to our hypotheses, we ran five analyses: First, we assessed two models with clinician-rated ADHD symptoms as outcome and the total and subscale scores of the FFMQ-SF and the SCS-SF at posttreatment respectively as mediators. Supplementary to these analyses, we ran a model with the nine subscales of the BRIEF-A at 3-month follow-up as mediators. Second, we assessed two models with positive mental health as outcome and clinician-rated ADHD symptoms and the total and subscale scores of the FFMQ-SF and the SCS-SF at posttreatment respectively as mediators. To run these models, we employed Hayes and Preacher’s (2013) SPSS PROCESS macro that uses ordinary least squares regression to estimate the direct effect (impact of treatment on outcome) and indirect effects (impact of treatment on outcome through mediators). More specifically, the bootstrapping produces an approximation of the sampling distribution of the indirect effects. This is achieved through empirically generating a sample (with 5,000 replacements) from the full data set and calculating the indirect effects in the resamples. Following recommendations by Hayes and Rockwood (2017), we used baseline measures of the outcome and mediators as covariates to model difference scores. As we hypothesize that MBCT for ADHD might work through more than one mechanism, we will test the different mediators in one model. This has several advantages, including the reduction in parameter bias, and the determination of the relative magnitude of the indirect effects associated with each of the proposed mediators. Statistical significance of the mediator was determined at p = .05 if the 95% bias-corrected percentile bootstrapped confidence interval of the indirect effect point estimate did not contain 0 (Hayes & Preacher, 2013). Effect size for the mediation effect is the ratio of the indirect effect to the total effect (i.e., direct plus indirect effect; Preacher & Kelley, 2011).
Results
Participants
Of the 60 patients allocated to MBCT + TAU, two did not start MBCT and seven dropped out. Reasons for not completing MBCT included work interference (n = 4), moving away (n = 1), physical condition (n = 1), divorce (n = 1), trouble planning (n = 1), and death of a relative (n = 1). Fifty-two of the participants in the MBCT + TAU group completed posttreatment and 50 completed 6-month follow-up assessment. Of the 60 patients who were allocated to TAU, all 60 refrained from participating in an MBI and 55 completed posttreatment and 52 completed 6-month follow-up assessments. See Table 1 for demographic and clinical characteristics of the treatment-adherent sample. There were no significant differences in sociodemographic or clinical characteristics between completers and noncompleters of the intervention, except that those patients who dropped out (n = 9; 15%) were less likely to use ADHD medication, χ2(1) = 6.30, p = .023, at baseline (Janssen et al., 2018).
Demographic and Clinical Characteristics of Treatment-Adherent Sample (n = 111).
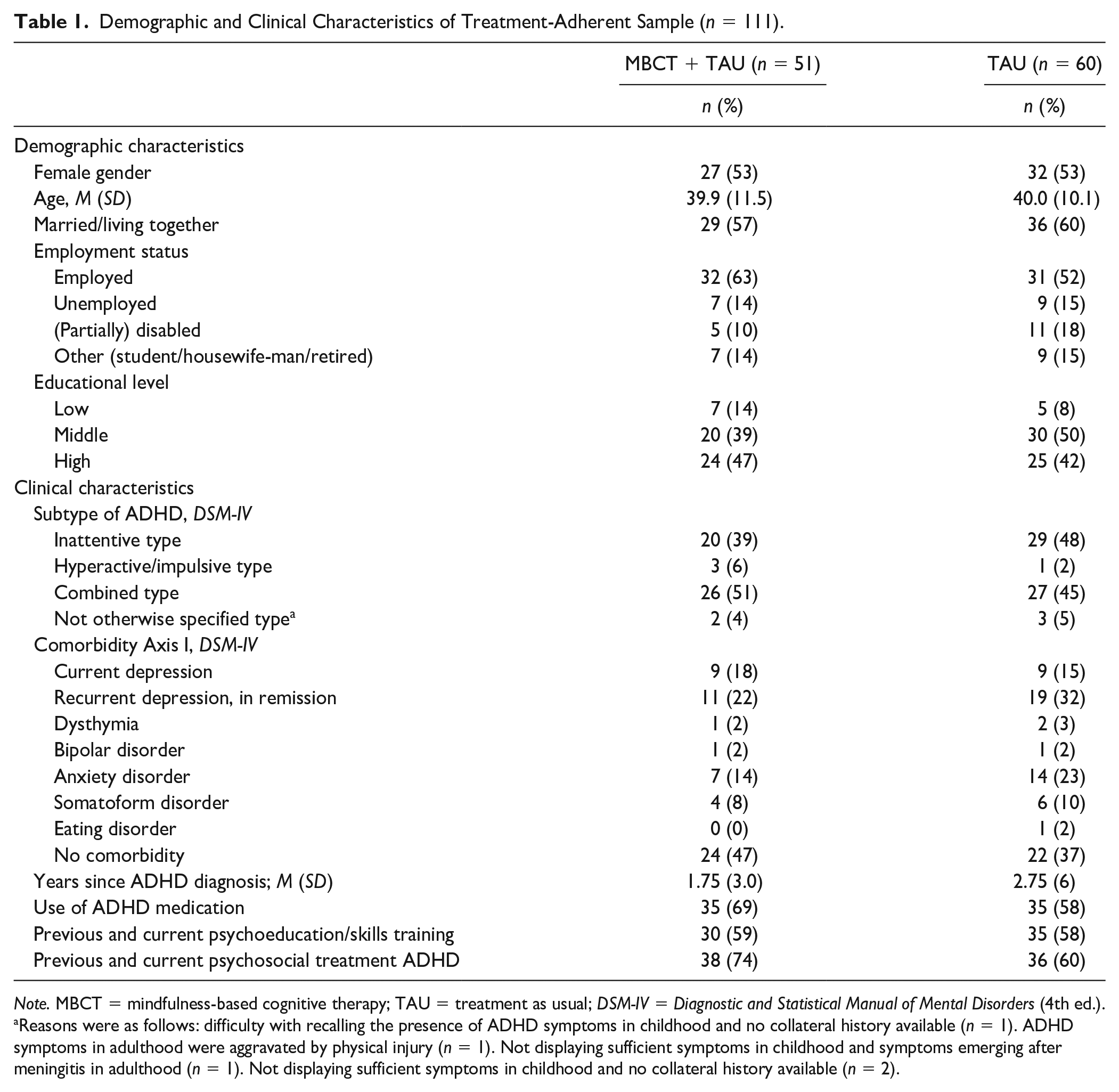
Note. MBCT = mindfulness-based cognitive therapy; TAU = treatment as usual; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.).
Reasons were as follows: difficulty with recalling the presence of ADHD symptoms in childhood and no collateral history available (n = 1). ADHD symptoms in adulthood were aggravated by physical injury (n = 1). Not displaying sufficient symptoms in childhood and symptoms emerging after meningitis in adulthood (n = 1). Not displaying sufficient symptoms in childhood and no collateral history available (n = 2).
Mediation Analyses
Baseline and 6-month follow-up data of the outcomes (ADHD symptoms, positive mental health), and baseline and posttreatment data on the mediator variables mindfulness skills and self-compassion and 3-month follow-up data on executive functioning for the treatment-adherent sample are presented in Table 2.
Mean Data for the Outcome and Potential Mediator Variables for the Treatment-Adherent Sample.

Note. MBCT = mindfulness-based cognitive therapy; TAU = treatment as usual; CAARS-INV = Conners’ Adult ADHD Rating Scale–Investigator Rated; MHC-SF = Mental Health Continuum–Short Form; FFMQ-SF = Five Facet Mindfulness Questionnaire–Short Form; SCS-SF = Self-Compassion Scale–Short Form; BRIEF-A = Behavior Rating Inventory of Executive Function–Adult Version.
Full data available for n = 98, MBCT + TAU = 46, TAU = 52. bFull data available for n = 93, MBCT + TAU = 44, TAU = 49. cFull data available for n = 101, MBCT + TAU = 46, TAU = 55. d Full data available for n = 96, MBCT + TAU = 45, TAU = 51.
Clinician-rated ADHD symptoms
As shown in Table 3, the model using the total scales demonstrated that improvement in mindfulness skills and self-compassion did not mediate the effect of MBCT + TAU versus TAU on clinician-rated ADHD symptoms at 6-month follow-up. Moreover, the model with the subscales did not demonstrate mediation by the separate facets of mindfulness skills or indicators of self-compassion. Supplementary, the model with the nine executive functioning subscales did demonstrate that improvements of inhibition mediated improvements of ADHD symptoms at 6-month follow-up (Table 4).
Mediators of the Effect of MBCT on Clinician-Rated ADHD Symptoms at 6-Month Follow-Up.

Note. Full data available for n = 94, MBCT + TAU = 43, TAU = 51. Effect size = ratio of the indirect effect to the total effect. MBCT = mindfulness-based cognitive therapy; CI = confidence interval; TAU = treatment as usual.
Different Domains of Executive Functioning as Mediators of the Effect of MBCT on Clinician-Rated ADHD Symptoms at 6-Month Follow-Up.
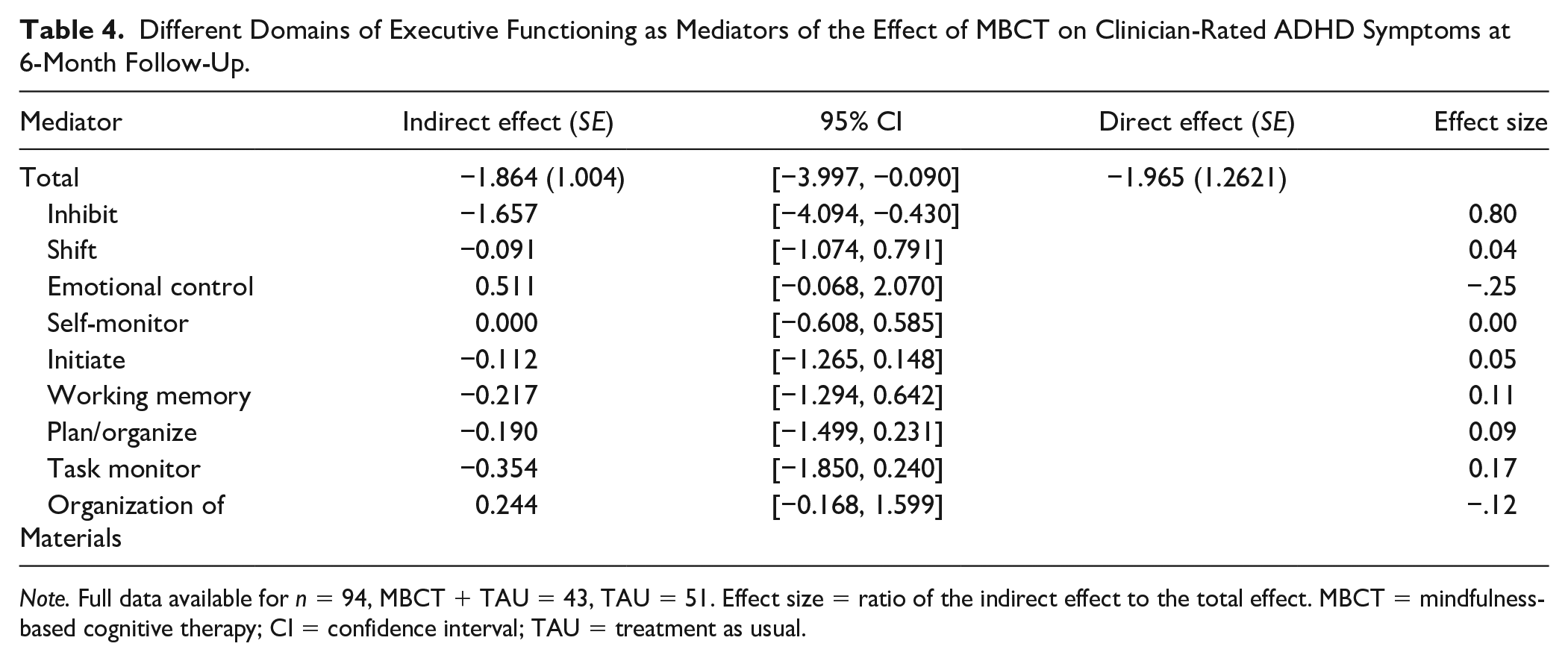
Note. Full data available for n = 94, MBCT + TAU = 43, TAU = 51. Effect size = ratio of the indirect effect to the total effect. MBCT = mindfulness-based cognitive therapy; CI = confidence interval; TAU = treatment as usual.
Positive mental health
As shown in Table 5, the model with total scales showed that increases in self-compassion mediated the effect of MBCT + TAU versus TAU on positive mental health at 6-month follow-up. The increase in mindfulness skills did not mediate the effect on positive mental health. When looking at the subscales, only the negative indicators of self-compassion mediated the effect of MBCT + TAU versus TAU on positive mental health. More specifically, a decrease in the negative indicators of self-compassion mediated the increase in positive mental health.
Mediators of the Effect of MBCT on Positive Mental Health at 6-Month Follow-Up.
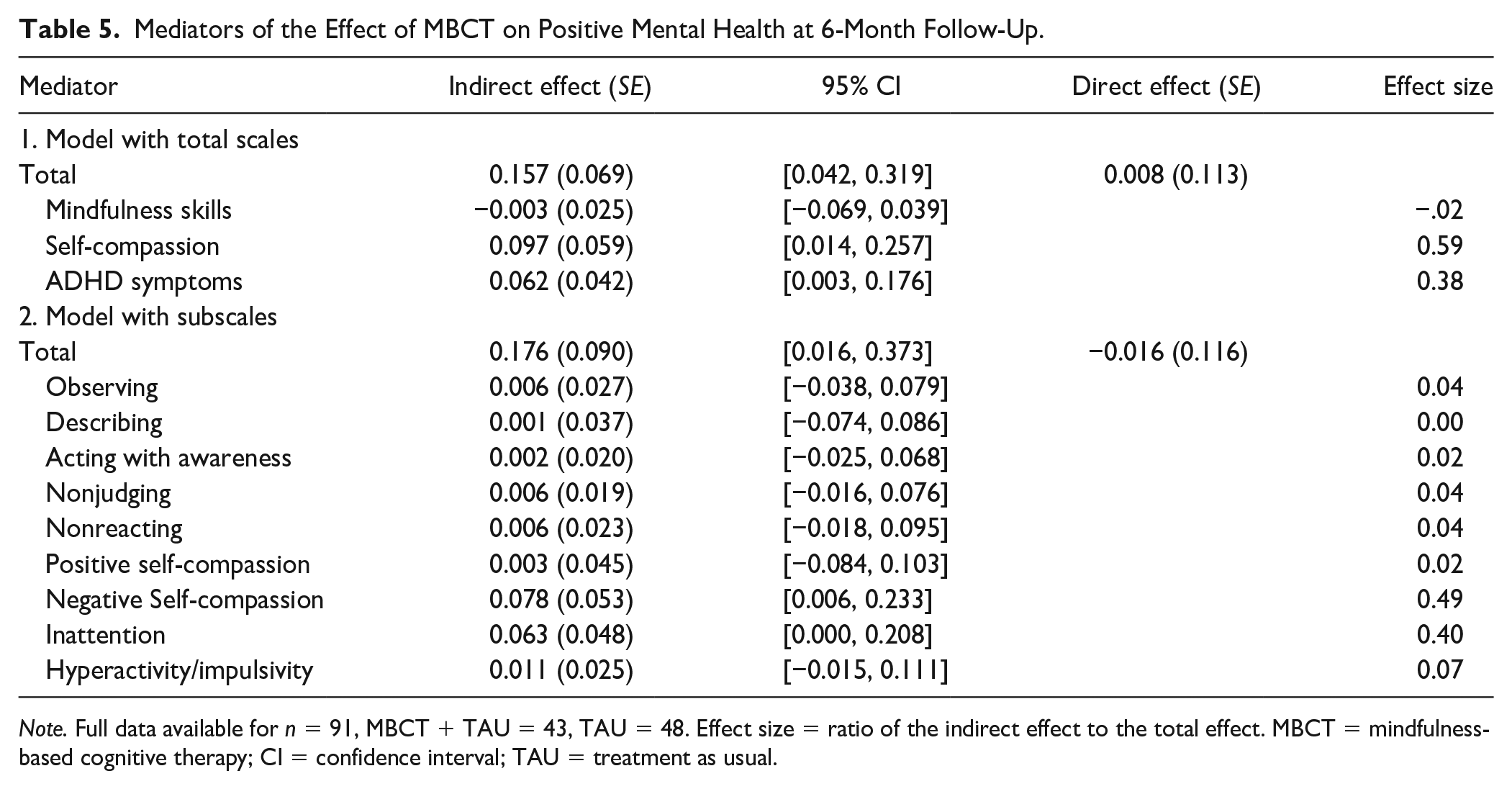
Note. Full data available for n = 91, MBCT + TAU = 43, TAU = 48. Effect size = ratio of the indirect effect to the total effect. MBCT = mindfulness-based cognitive therapy; CI = confidence interval; TAU = treatment as usual.
As hypothesized, improvements in ADHD symptoms over the course of MBCT mediated improvements in positive mental health at 6-month follow-up. Thus, the beneficial effect of MBCT on positive mental health was mediated by both self-compassion and improvements in ADHD symptoms. Note that we tested both significant mediations in one model, indicating that self-compassion mediates the effect of MBCT on positive mental health over and above the mediating effect of MBCT-induced ADHD symptom reduction.
Discussion
In the present study, we examined whether the significant effect of MBCT on clinician-rated ADHD symptoms and positive mental health at 6-month follow-up, measured in a relatively large RCT, was mediated by changes in mindfulness skills, self-compassion, executive functions, or their subscales over the course of MBCT. No evidence was found for mediation of improvement in ADHD symptoms at 6-month follow-up by either change in mindfulness skills or self-compassion over the course of MBCT. Additional analyses did suggest that improvement in ADHD symptoms at 6-month follow-up was mediated by MBCT-induced changes in inhibition at 3-month follow-up. Improvements in positive mental health at 6-month follow-up were mediated by improvements in self-compassion over the course of MBCT, even when controlled for improvements in ADHD symptoms.
Which Mechanisms Drive MBCT-Induced Improvements on Clinician-Rated ADHD Symptoms?
The RCT, in which the current mediation study was embedded, showed that MBCT led to substantial improvements in ADHD symptoms (Janssen et al., 2018). The lack of evidence for a mediational role of mindfulness skills in the current study is noteworthy. Ample studies reveal that MBCT substantially increases mindfulness skills and that increasing mindfulness skills is involved in MBCT-induced improvements (Alsubaie et al., 2017; Kuyken et al., 2010; van der Velden et al., 2015). There is one report on preliminary data (from our group) that showed that reductions in ADHD symptoms were partially mediated by the mindfulness skill “Act With Awareness” (Hepark et al., 2015). The key differences between this latter study and our current study are the duration of the MBCT program and differences in mediation analyses. Notably, Hepark et al. used a 12-week instead of an 8-week program. It might be a possibility that the 8-week MBCT might have been too short for a significant mediating role of mindfulness skills to emerge in this particular population. Moreover, Hepark et al. did not assess temporal mediation, that is, the measurement of the mediator did not precede the measurement of the outcome. That we do assess temporal mediation (6 or 3 months difference between mediator and outcome assessment), is a stronghold of our study, as this is regarded to be a major criterion for indicating mediators in mechanisms of change (Kazdin, 2007).
If mindfulness skills indeed are not involved in the positive effects MBCT brings about in patients with ADHD, the question remains how MBCT impacts these symptoms? First, we note that the vast majority of evidence on a mediating role for mindfulness skills in MBCT is derived from more internalizing patient groups, such as depressed patients (Kuyken et al., 2016). The effect of mindfulness on depressogenic cognitions such as repetitive negative thoughts and cognitive reactivity is thought to be part of the main mechanism of improvement in these groups (van der Velden et al., 2015). Although depressogenic cognitions might be found in a proportion of ADHD patients, this might not relate to their core symptoms. There might be quite different mechanisms underlying MBI-induced changes for more externalizing patient groups such as ADHD patients. MBCT might improve cognitive control resulting in a decrease in symptoms of attentional deficit, hyperactivity, and impulsivity. Indeed, MBIs have been shown to affect several cognitive control functions (Chiesa et al., 2014; Lao et al., 2016), such as working memory, cognitive flexibility (Lao et al., 2016) and inhibition (Gallant, 2016; but see for critical review Vago et al., 2019). In line with this latter finding, we show the first evidence for a mediating role of self-reported improvements in appropriate inhibition of thoughts and actions (measured with the BRIEF-A Inhibit subscale) in the improvement of ADHD symptoms. It is noteworthy that in the RCT, on which our mediation analyses are based, improvements in executive functions became only apparent at 3-month follow-up instead of directly posttreatment (Janssen et al., 2018). We consider that the BRIEF-A might not have been sensitive enough to capture subtle differences that might already have been there at posttreatment. Specific executive functions, such as inhibition and working memory, might also be better captured by behavioral tasks in combination with neuroimaging and computational modeling of underlying latent cognitive processing than by self-report questionnaires (Maia et al., 2017). Future research should assess whether these tasks can indeed contribute to understanding the mechanisms of change underlying MBCT in general and for ADHD in particular (Schoenberg et al., 2013; cf. van der Velden et al., 2015).
Self-Compassion Mediates MBCT-Induced Improvements in Positive Mental Health
Next to mindfulness skills, the importance of self-compassion for the workings of MBIs has been established in a wide variety of mediation studies, including different patient groups and different outcome measures (e.g., Gu et al., 2018; Kingston et al., 2015; Kuyken et al., 2010). We now add to this body of research by showing that the effect of MBCT on positive mental health is mediated by self-compassion in ADHD patients. Increases in self-compassion over the course of MBCT induced increases in positive mental health at 6-month follow-up, over and above the positive effect of improvements in ADHD symptoms. Self-compassion, however, did not mediate the positive effect of MBCT on ADHD symptoms at 6-month follow-up. Together, these results suggest that the positive impact of self-compassion on positive mental health is independent of the change in ADHD symptoms. It is of note that in our subscale analyses, changes in specifically negative self-compassion contributed to the above-described mediation. This suggests that for ADHD patients MBCT increases psychological well-being through reducing negative aspects of self-compassion. This is in line with the finding that especially the negative subscale has been related to changes in psychopathology (Muris & Petrocchi, 2017). The negative aspects measured by this subscale (Self-Judgment, Overidentification, and Isolation) are thought to amplify suffering of patients. Patients can be harsh on oneself in judgment and being self-centered with an overfocus on the relation between oneself and the suffering (Neff, 2003). This negative way of dealing with symptoms, functional impairments and their related history of perceived failure and suffering is not uncommon in our clinical experience with ADHD patients. Our finding is also in line with the qualitative findings of the mixed-method trial of Janssen et al. (2020) where several participants reported that instead of hurting themselves with self-criticism they developed more self-acceptance and self-kindness when facing general suffering or personal short-comings.
Together, these observations indicate that there are different pathways through which MBCT might lead to improvements in mental health in ADHD patients: At least one through enhancing self-compassion and another through reduction of core ADHD symptomatology. This dovetails with the idea that MBIs might improve health by symptom reduction on the one hand and by the development of adaptive, positive psychological perspectives on one’s day-to-day experiences (including but not limited to the aforementioned symptoms) on the other.
Clinical Implications
One clinical implication based on the above considerations would be to incorporate more self-compassion elements in the MBCT training. ADHD patients might benefit from this in terms of their positive mental health. In addition, prolonging the training might also have beneficial effects on core ADHD symptoms. More practice might lead to better mastery of, for example, executive inhibition (Sahdra et al., 2011), which (at 3-month follow-up) was indicated by our current study as a significant mediator of change in ADHD symptoms (at 6-month follow-up). In addition, two other observations might add to this suggestion: First, the study by Hepark et al. (2015) employing a 12-week MBI sorted large effect sizes in terms of improvement in ADHD symptoms and mindfulness skills. Second, increasing practice was also among the suggestions of participants in a previous mixed-method study on MBCT for ADHD: The 8-week duration of the training was considered a barrier to a substantial part of the patients and some of them suggested to extend the length of the training to create more room for practice (Janssen et al., 2020). Obviously, whether longer treatment and inclusion of more self-compassion elements indeed would sort better outcomes is something that should be trialed.
Strengths, Limitations, and Research Implications
To date, this study is the largest RCT on MBCT in an ADHD population that assesses mediation processes in detail. A major strength of this study is the measurement of mediators at points in time preceding the outcomes contributing to the soundness of the mediation analyses (Kazdin, 2007). Notwithstanding this strength, future studies might further improve this by assessing mediators during instead of after treatment. The RCT design, with a follow-up of half a year without MBCT for the TAU condition, allowed us to assess mediation in a properly controlled cohort. Furthermore, the current study had a relatively high number of participants for the mediation analyses, although we should acknowledge that for mediation studies typically larger samples are needed to reduce false-negative findings (Fritz & MacKinnon, 2007; Schoemann et al., 2017). Moreover, the RCT in which the data were acquired made sure that the integrity of treatment was high, with qualified teachers whose competence was assessed with a standardized observational measure. This is especially important for mediation studies that search for mechanisms via which therapy works. If not carried out well, one might not expect therapy-related working mechanisms to arise.
Although there were no differences in comorbidity between treatment groups (Janssen et al., 2018), we did not gather data on depressive symptoms or rumination. The Negative subscale of self-compassion involves items relating to rumination, such as “When I’m feeling down I tend to obsess and fixate on everything that’s wrong.” Indeed, a relation between especially the negative aspects of self-compassion and depression, and anxiety and negative affect has been reported (Muris & Petrocchi, 2017). We did record diagnoses of current depression, but the low number of participants (nine in each group) prevents subgroup analyses. Thus, we cannot exclude that (subclinical) depressive symptoms and/or rumination might explain the mediational role of self-compassion in the improvement of positive mental health.
In sum, this study uncovers different mechanisms of change underlying the beneficial effect of MBCT on ADHD core symptoms and positive mental health in adults with ADHD. We hope that these findings might be stepping stones for future research on mechanisms of change and for improving MBIs for ADHD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ZonMW, The Netherlands, Organization for Health Research and Development (grant number 837001501).