
Abstract
The transition from middle school to high school is considered a critical point in development wherein some adolescents experience declining grades, report lower self-worth and increasing loneliness, and experience elevated levels of anxiety (Benner, 2011; Mizelle & Irvin, 2000). This transition is also characterized by a marked increase in depression (Newman et al., 2007), with rates of major depressive disorder (MDD) increasing from 2% to 5% in childhood to 10% to 15% in adolescence (Avenevoli et al., 2015; Lewinsohn et al., 1994). The average age of onset for depression is squarely in adolescence (Hammen et al., 2014), and coincides with the transition to high school (Lewinsohn et al., 1994). Given the rise in depressive symptoms across high school and the significant morbidity and mortality associated with adolescent depression (Koplewicz & Klass, 2016), research is needed to specify which adolescents are most at risk for depressive symptoms across high school and to elucidate mechanisms (i.e., moderators) underlying the onset of depressive symptoms during this risk period.
Children and adolescents with symptoms of ADHD are significantly more likely to experience depression than their peers without elevated ADHD symptoms, and the significant difference in depressive symptoms between ADHD and non-ADHD groups likely emerges between ages 13 and 18 (Chronis-Tuscano et al., 2010; Meinzer et al., 2013, 2016). Adolescents with ADHD symptoms may be at particular risk for depressive symptoms during this period given the increasing social demands during this developmental stage and their corresponding impairments in this functional domain (Sibley et al., 2010). However, even beyond academics, these youth are more likely to experience social and emotional problems, more broadly, making the developmental transition through high school especially taxing for adolescents with ADHD and their parents (Litner, 2003).
Beyond the study of clinical samples, researchers have examined the link between ADHD and depression dimensionally and/or within subclinical ADHD samples. For instance, Roy and colleagues (2015) found that rates of depression were elevated in youth with subthreshold ADHD symptoms (24%), albeit somewhat less so than among youth with a diagnosis of ADHD (36%), compared to youth without ADHD symptoms (14%). Furthermore, teacher-rated levels of inattention have been shown to predict depressive symptoms, by way of levels of self-esteem, even among youth with subclinical ADHD. The risk of depression associated with ADHD symptoms and the reliability and validity associated with dimensional measurement approaches (Markon et al., 2011) further emphasizes the need to continue examining ADHD and other mental health constructs at varying degrees of severity in community samples rather than at diagnostic levels only.
With increasing academic, social, and emotional challenges emerging in high school for youth with elevated ADHD symptoms, the transition to and through high school can be thought of as a high-risk period for the development of depressive symptoms in adolescents with symptoms of ADHD. Therefore, research efforts to identify risk processes underlying the development of depression during this transition period among youth with varying degrees of ADHD symptoms are critical to inform prevention and intervention efforts.
Social Relationship Quality in the Context of Co-occurring ADHD-Depression
Consistent with research in unselected samples linking social impairments to adolescent depression risk, one possible mechanism underlying co-occurring ADHD and depressive symptoms may be the quality of significant social relationships. Longitudinal research highlights the role of both parents and peers in depression risk during adolescence. For instance, Newman and colleagues (2007) showed that declines in the quality of both parent and peer relationships from eighth to ninth grade predicted depressive symptoms in the ninth grade in a community sample of adolescents.
Indeed, ADHD is also associated with impairments in peer and family functioning (Sibley et al., 2010). For example, symptoms of inattention interfere with sustaining attention in conversations, following through on plans and discerning social cues (Mrug et al., 2001; Ray et al., 2017). Difficulties with inhibition and impulsivity may lead to rash verbal/emotional behavior and decision-making that can damage social relationships (Barkley et al., 2010). However, despite the social costs of ADHD symptoms and research linking social factors (e.g., loneliness, perceived rejection) to depression in unselected samples, most of this work is theory-based, with past empirical research providing equivocal support that social impairments underlie the relation between ADHD and depression symptoms. Only one study, to our knowledge, has investigated the quality of the relationships with their mother and close friends in the context of adolescent ADHD symptomology (i.e., Glass et al., 2012). Far less emphasis has been placed on the quality of relationships with close others, such as with a best friend (Mikami, 2010). In this study, we evaluated the independent contributions of negative relationship quality with an adolescent’s mother and best friend throughout middle school and high school on depressive symptoms using latent growth curve (LGC) modeling.
Negative Relationship Quality With Parents
Although peer relationships are especially important during the developmental stage of adolescence, adolescents’ relationships with their primary caregivers (e.g., typically mothers) remain key correlates of adolescent functioning, especially within the context of ADHD (see Johnston & Chronis-Tuscano, 2015). Despite adolescents with ADHD likely requiring increased support and scaffolding from their parents across adolescence and emerging adulthood relative to non-ADHD youth, the mother–child relationship is often riddled with conflict. Parents of adolescents with ADHD frequently report increased conflict and parenting stress relative to parents of youth without ADHD (Mazursky-Horowitz et al., 2015). Adolescents with ADHD also perceive more areas of conflict and more angry conflicts with their mothers than those without ADHD (Barkley et al., 1992).
Researchers have also shown, cross-sectionally, that youth with ADHD who rate their mothers as less warm and more power assertive experience greater depressive symptoms relative to youth with ADHD who do not endorse these perceptions (Gerdes et al., 2007). Parent–child problems and problematic relationships, more broadly, are also associated with depression in youth with ADHD (Ostrander & Herman, 2006). In addition, parent–adolescent difficulties have been shown to mediate the relation between youth ADHD and depressive symptoms both cross-sectionally and longitudinally (Humphreys et al., 2013). Recently, researchers have found that parent–child conflict partially mediates the association between social impairment (i.e., a construct comprised of communication, cooperation, assertion, responsibility, empathy, engagement, self-control) and depressive symptoms among young adolescents with ADHD (Eadeh et al., 2017). Taken together, negative parent–adolescent relationship quality may help to explain the relation between ADHD symptoms and depressive symptoms, particularly through key developmental transition periods. However, prior research has yet to examine these relations using trajectories of negative relationship quality. In addition, previous research has yet to examine these associations during the transition to and through high school while considering both parent and friend relations.
Negative Relationship Quality With Best Friends
Most youth have a best friend; however, the quality of best friendships varies and the putative benefits of friendship are determined by the extent to which the relationships are viewed as positive and supportive (Rubin et al., 2015). For example, it has been shown that friendships characterized by conflict and negativity predict anxiety and depressive symptoms in adolescence (e.g., Burk & Laursen, 2005). Moreover, friendship quality is often viewed as a moderator of the association between youths’ behavioral characteristics and both positive and negative outcomes (Bagwell & Bukowski, 2018; Hiatt et al., 2015). In this regard, it may be that symptoms of ADHD are socially aversive in the context of close relationships (e.g., interrupting or intruding on others; Nijmeijer et al., 2008), contributing to lower quality friendships characterized by more negative interactions. In turn, these conflicted relationships may predict depressive symptoms in youth. This hypothesis would be consistent with the oft-noted finding that qualitatively poor friendships predict negative outcomes, especially for youth who present with particular psychological and interpersonal characteristics (e.g., social withdrawal; peer rejection; rejection sensitivity; victimization) to begin with (Bagwell & Bukowski, 2018; Rubin et al., 2015).
Relative to youth without ADHD, youth with ADHD experience more difficulty maintaining friendships (Mikami, 2010). This may be in part due to youth with ADHD being less cooperative relative to their friends without ADHD (Normand et al., 2007, 2011). In the extant literature on friendship quality and ADHD, children and adolescents with ADHD have been described as making more insensitive and self-centered proposals during negotiations and displaying more dominant behavior compared with their non-ADHD peers (Normand et al., 2011). In another study, ADHD predicted conflict with a best friend (Zucchetti et al., 2015). However, in a study of friend dyads, symptoms of ADHD were surprisingly positively associated with both self-reported and friend-reported friendship quality (Glass et al., 2012). Although several studies report that ADHD is predictive of poorer quality friendship, findings are mixed and the trajectory of friendship quality over the course of middle school and high school in the context of ADHD has yet to be examined. Moreover, only one study to date has examined the moderating role of sex in the relation between ADHD symptoms and friendship quality; though females rated their friendships more positively, gender did not significantly moderate the relation between ADHD symptoms and friendship quality (Glass et al., 2012), though all analyses were cross-sectional in nature. In addition to limited research on potential sex differences in ADHD and friendship quality, it is unknown whether negative quality within the best friend relationship is predictive of adverse outcomes (e.g., depression) among youth with ADHD symptoms.
Given that adolescents are thought to place more stock in social norms and the expectations and opinions of their peers, repeated negative social interactions with peers and close friends across adolescence confer substantial depression risk (e.g., Mrug et al., 2012). Indeed, social acceptance within a peer system indexes adolescent adjustment, and youth with good social skills are considered better adjusted than those with poor social skills (see Rubin et al., 2015, for a review). Youth with ADHD may be especially prone to negative peer interactions within friendship dyads and subsequent depression risk during the transition to high school given their symptoms and associated social impairments. Although researchers have examined different facets of peer difficulties as mediators between ADHD and depressive symptoms (e.g., Humphreys et al., 2013), adolescents’ relationships with close friends has seldom been examined and only one study (i.e., Zucchetti et al., 2015) has examined conflicts in best friendships and ADHD. Furthermore, researchers, to our knowledge, have not examined the quality of best friendships as a mechanism linking symptoms of ADHD to depressive symptomatology across a high-risk developmental period for depression. Therefore, one important research direction that remains to be addressed is to examine longitudinal relations of ADHD symptoms, relationship quality with a best friend, and depressive symptoms during a high-risk developmental period, and elucidating the ways by which sex impacts this risk pathway.
Sex Differences in Parent and Peer Risk Mechanisms for Depression in ADHD
Although research suggests that ADHD is a risk factor for the development of depressive symptoms, less is known about the ways by which sex moderates the psychosocial risk mechanisms of depression in the context of adolescent ADHD symptoms. Therefore, an important direction is to evaluate whether and how this study’s hypothesized risk mechanisms for depression—negative interactions with mothers and best friends—may operate differentially for males versus females with ADHD symptoms. Indeed, research suggests that boys and girls evidence different patterns of ADHD symptoms and impairments (Bauermeister et al., 2007), which may also lead to sex-specific patterns of relational functioning with friends and mothers. There is some literature to suggest that boys rely on relationships with their mothers throughout adolescence as they continue to hone their interpersonal skills (Rubin et al., 2004). Some research supports a “gender appropriateness hypothesis” such that peers tolerate higher levels of ADHD symptoms, particularly hyperactivity, among boys versus girls with ADHD (Diamantopoulou et al., 2005). However, beyond the ADHD literature, boys demonstrate a steeper decline in peer social support than girls following the transition to high school (DeWitt et al., 2011). Similarly, for girls, intimate disclosure in friendships increases into adolescence whereas this trend is not observed in boys (Buhrmester & Furman, 1987). Other researchers have found that interpersonal difficulties in ADHD are consistent across sexes (Greene et al., 2001), and a recent review elucidated difficulties in various domains of peer relationships across both males and females with ADHD (Gardner & Gerdes, 2015).
Only two studies (within one manuscript; Humphreys et al., 2013), to our knowledge, have specifically examined sex differences in the relations between ADHD and interpersonal problems. Findings were equivocal in that no sex differences were found in either study examining ADHD and adolescent interpersonal problems (i.e., with parents or peers). Mixed findings regarding sex differences in parent and peer interactions in ADHD may be due to the lack of research using a dynamic approach to examining both baseline and course characteristics of relationship impairments during a key developmental risk period, as we do in this study. It may be the case that sex is an important yet overlooked and insufficiently studied component of key risk mechanisms responsible for the co-occurrence of ADHD and depression symptoms during adolescence. Therefore, beyond the importance of identifying trajectories of negative interactions with both mothers and close friends as possible mechanisms placing adolescents with elevated ADHD at risk for depressive symptoms, there is also a clear need to elucidate potential sex differences in the relation between ADHD symptoms and these mechanisms of depression risk.
The Current Study
Both relationships with parents and friends, especially close friends, exert an important influence on adolescent development. It is also the case that adolescents with elevated ADHD symptoms are more likely than those without symptoms of ADHD to experience impairments in these domains, which may explain the high risk for depressive symptoms in this population. However, researchers have yet to examine whether adolescents with more ADHD symptoms transitioning to high school are especially vulnerable to poor relationship quality with their mother and their best friend and whether the negative quality of these key relationships is stable over high school or increasingly negative for adolescents with ADHD symptoms. Furthermore, we sought to determine whether course characteristics of best friend and mother interactions (e.g., static or increasingly negative over time) mediate the relation between ADHD and depressive symptoms. Despite the fact that sex is a well-established risk factor for depression during this time and the possibility that the relation between ADHD and interpersonal relationships may operate differentially for males and females, researchers have not attempted to specify the ways by which sex moderates the relation between ADHD symptoms and relationship quality mechanisms for depressive symptoms.
This study, therefore, fills several important gaps in the literature by examining the relative contribution of the changes in mother and best friend negative relationship quality across adolescence as a mediator of the association between ADHD symptoms and depressive symptoms. This study is poised to address risk factors in a critical developmental period associated with elevated depressive symptoms—the transition from middle school to high school. Moreover, this study explores whether the relation between ADHD symptoms at Grade 8 (the last year of middle school) and negative relationship quality varies by sex and, in turn, whether changes in negative relationship quality mediate the relation between ADHD symptoms and depressive symptoms in the 12th grade. Furthermore, these trajectories will be examined in the context of ADHD symptoms, a construct associated with increased likelihood of both parent–child relationship (Barkley et al, 1992; Mazursky-Horowitz et al., 2015) and best friend relationship (Zucchetti et al., 2015) difficulties. To our knowledge, this is the first study to examine the trajectory of mother and best friend relationships in adolescence in the context of sex, depressive symptoms, and ADHD symptoms, simultaneously, across the transition from middle school to high school, a time period that has rarely been studied in relation to ADHD. In sum, this study extends the literature by proposing a moderated mediation model in which we evaluate whether the intercept or slope of mother negative relationship quality and negative relationship quality with a best friend mediates the relation between ADHD symptoms in the eighth grade and depression symptoms in the 12th grade differentially for boys and girls.
Method
Participants and Procedures
Youth were recruited from one of three public middle schools in the Washington, DC, metropolitan area for participation in a longitudinal study of peer and parent–child relationships. After obtaining classroom data pertaining to mutual friendship nominations (see McDonald et al., 2013), a subset of youth and their parents or guardians were recruited to complete additional measures in the lab. Inclusionary criteria for the study required participants to have a mutually identified best friend within the sixth grade. More specifically, children were asked in the sixth grade to identify their “very best friend” and their “second best friend” (of the same sex) at their school. Children were considered best friends if they were each other’s very first or second best friend choice (i.e., a mutually identified best friend). At subsequent time points, adolescents reported on the quality of their best friendship at that grade level.
Data presented below are from a sample of N = 368 youth who completed key study variables at the eighth grade (Mage = 13.64, SDage = 0.56; 48.5% male). Data were also collected at ninth (N = 351) and 12th (N = 245) grades. The sample was racially diverse and reflective of the area from which it was drawn, including 53.9% of youth identifying as White, 15.9% of youth as Black, 13.3% as Asian, 11.4% as LatinX, and 5.5% as multiracial or other race.
Measures
Adolescent ADHD symptoms
The Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001) is a parent-report measure that assesses children’s mood and behavior. Participants’ parents/guardians completed the CBCL in Grade 8. This study utilized the attention problems subscale, which includes 11 items such as “can’t sit still” and “can’t concentrate.” Items are ranked on a 3-point rating scale ranging from (0) not true to (2) very true or often true. Items are then summed, with higher scores reflecting greater attention problems. The CBCL is widely used and has been found to be both reliable and valid (Achenbach & Rescorla, 2001; Chen et al., 1994). It has also been used as the measure of ADHD symptoms in past research (e.g., Chen et al., 1994; Lifford et al., 2008). The coefficient alpha for the CBCL attention problems scale in this study was .79.
Mother and best friend relationship quality
The Network of Relationships Inventory (NRI; Furman & Buhrmester, 2009) assesses participants’ relationship quality with their best friends and parents. Participants completed this measure at Grades 8, 9, and 12. In this study, we used the best friend and mother negative relationship quality subscales, which consist of six items each, tapping conflict and punishment within the relational dyad. Items include “How often do you and this person disagree and quarrel with each other?” ranked on a 5-point rating scale ranging from (1) little or none to (5) the most. Higher total scores reflect more negative relationship quality. It is important to note that in this study, the best friend that adolescents reported on in the eighth grade was not necessarily the same best friend reported on in ninth and 12th grades.
The scale has demonstrated good internal consistency in other community-based adolescent samples (Furman & Buhrmester, 1985). The coefficient alphas for this study ranged from .87 to .91 for mother–adolescent negative relationship quality and .83 to .84 for best friend negative relationship quality across eighth-grade, ninth-grade, and 12th-grade time points.
Grade 12 depressive symptoms
The Beck Depression Inventory–II (BDI-II; Beck et al., 1996) is a 21-item self-report assessment of depressive symptoms administered at Grade 12 only. Participants were asked to rank how often they experienced specific affective and behavioral symptoms of depression in the last 2 weeks, including (0) I do not feel sad; (1) I feel sad; (2) I am sad all the time and I can’t snap out of it; and (3) I am so sad and unhappy that I can’t stand it. Total scores were created by summing items, with higher scores indicating greater depressive symptoms. The measure is both reliable and valid (Beck et al., 1996) and has been used extensively with adolescents (e.g., Krefetz et al., 2002; Rohde et al., 2001). The coefficient alpha was .92 in this study.
Data Analytic Plan
This study utilized structural equation modeling and an LGC approach to examine trajectories of best friend and mother negative relationship quality over time and the pathway from Grade 8 ADHD symptoms to Grade 12 depressive symptoms for boys and girls. We derived latent intercepts and slopes for both best friend and mother relationship quality in separate models. Means and variables for the intercept (or baseline) and the slope (trajectory) factors associated with best friend and mother relationship quality were estimated using all available data points from Grade 8 through Grade 12. Statistically significant mean estimates for the intercept indicate that youth start at nonzero levels of negative relationship quality, while statistically significant slope means suggest that negative relationship quality increases (in the case of a positive slope) or decreases (in the case of a negative slope) over time. Significant variances associated with each factor indicate important individual differences around these estimates. All analyses were completed using Mplus 6.0 (Muthén & Muthén, 2010) and full information maximum likelihood (ML) estimation methods to handle missing data. ML approaches provide less biased estimates than procedures such as listwise or pairwise deletion under the missing at random assumption (Little & Rubin, 1989). All LGC models thus utilized the full sample to estimate parameters.
First, unconditional LGCs were estimated for both mother and best friend negative relationship quality. To estimate these models, regression weights from the latent intercept factor to each of the manifest measures were constrained to be 1.0. Regression weights from the latent slope factor to each manifest measure dictate the shape of the trajectory and reflect the timing of assessments. In this case, we examined a linear trajectory from Grades 8 to 12 with a 2-year gap at Grades 10 and 11; thus, regression weights were constrained to 0.0, 1.0., and 4.0, respectively. Latent intercept and slope factors were also allowed to covary. Residuals associated with each manifest measure were constrained to be equal across repeated measurements (i.e., homoscedasticity) to create a more parsimonious model. Model fit was determined by examining four fit indices, including the χ2 statistic, the comparative fit index (CFI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR).
Next, conditional LGCs for mother and best friend negative relationship quality were examined in separate models. We regressed the latent intercept and slope of negative relationship quality onto our predictors (ADHD symptoms and sex) and examined model fit again. To evaluate whether the pathway from ADHD symptoms to the latent intercept and slopes of negative relationship quality varied by sex, we added an ADHD Symptoms × Sex interaction term as a predictor to the model. A significant effect of the interaction term on either factor would indicate that the impact of ADHD symptoms on the baseline values, and trajectory of negative relationship quality is moderated by sex. To more closely examine effects by sex, in the case of a significant interaction term, multigroup LGCs were then run examining the effect of the focal predictor on the latent intercept and slope in separate groups of boys and girls.
To examine our mediation hypotheses, we added Grade 12 depressive symptoms and regressed these symptoms onto the latent intercept and slope factors as well as our predictors. We then examined the indirect effect of the interaction between ADHD symptoms and sex on Grade 12 depressive symptoms via changes in negative relationship quality in both best friend and mother models (i.e., Grade 8 ADHD Symptoms × Sex → latent slope of negative relationship quality from Grades 8 to 12 → Grade 12 depressive symptoms). A 95% confidence interval (CI) band was estimated around the indirect effect using bootstrapping procedures (Preacher & Hayes, 2008), which do not assume normality of the distribution of the indirect effect. An indirect effect with a CI that does not contain zero indicates a statistically significant indirect effect (i.e., mediation).
Results
Preliminary Analyses
We examined the data for patterns of missingness utilizing two complementary approaches. Little’s (1988) missing completely at random (MCAR) test was conducted using all key study variables; results supported the assumption that data were MCAR: χ2(85) = 79.45, p = .650. We examined correlations between missingness and key study variables at Wave 1 (all correlations were p > .050) and each of our dependent variables (best friend negative relationship quality at all grades, mother negative relationship quality at all grades, and depressive symptoms at Grade 12) for univariate normality. Skew and kurtosis statistics appeared to be in the acceptable range (≤3.0). Descriptive statistics and correlations between key study variables are reported in Table 1. Sex was correlated with ADHD symptoms, such that boys were more likely to evidence greater ADHD symptomology than girls. Sex was also associated with mother negative relationship quality at eighth and ninth grades, indicating that girls reported greater negative relationship quality with their mothers, but not with their best friends. Significantly, ADHD symptoms at the eighth grade were positively correlated with adolescent–mother negative relationship quality at every grade.
Means, Standard Deviations, and Correlations Between Key Study Variables.
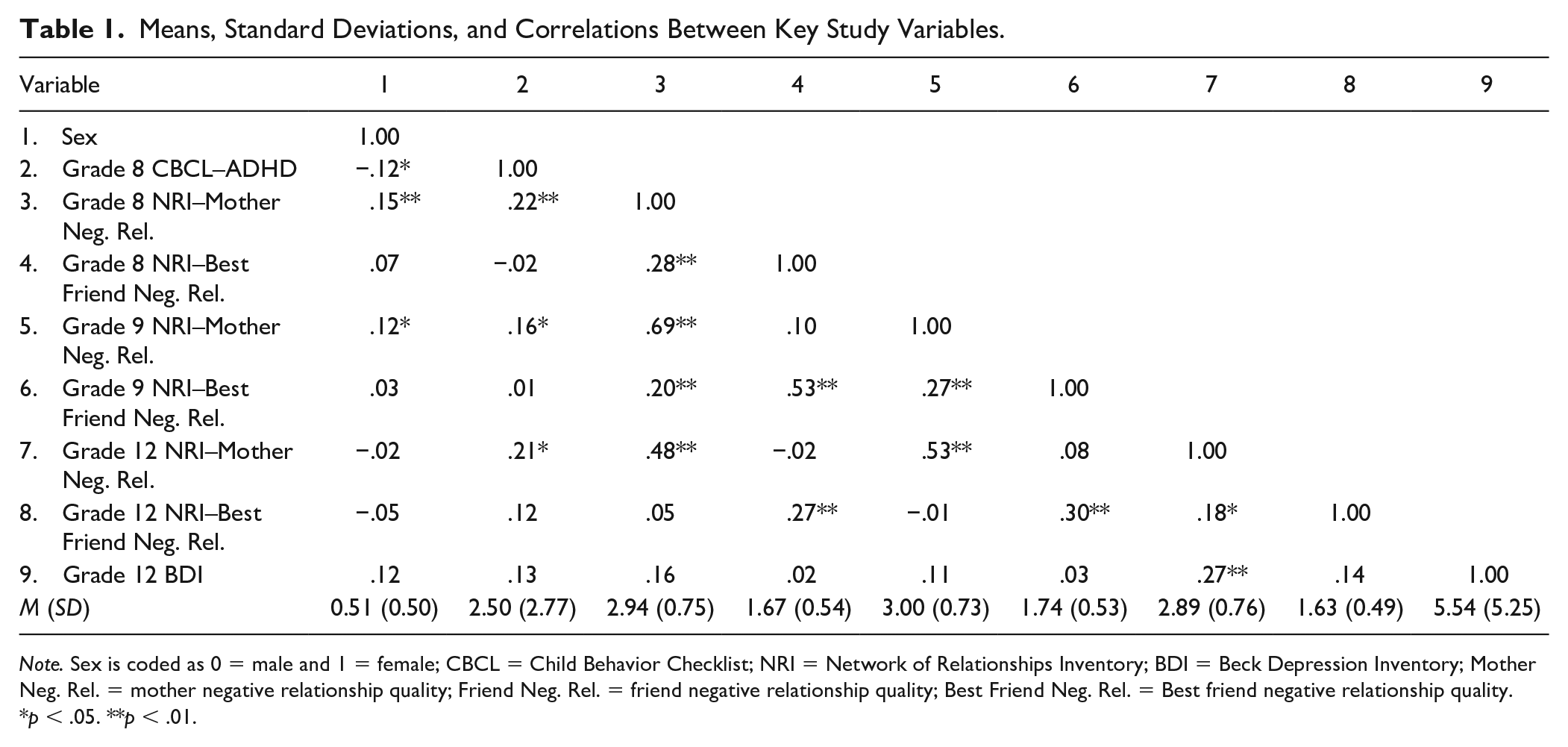
Note. Sex is coded as 0 = male and 1 = female; CBCL = Child Behavior Checklist; NRI = Network of Relationships Inventory; BDI = Beck Depression Inventory; Mother Neg. Rel. = mother negative relationship quality; Friend Neg. Rel. = friend negative relationship quality; Best Friend Neg. Rel. = Best friend negative relationship quality.
p < .05. **p < .01.
Adolescent–Mother Negative Relationship Quality
We first examined an unconditional LGC of adolescent–mother negative relationship quality. The model fits the data well: χ2(df=3) = 4.47, p = .215, CFI = 0.99, RMSEA = 0.03 (90% CI = [0.00, 0.09]), and SRMR = .03. The mean of the intercept (M = 3.00, SE = 0.04, p < .001) but not the slope (M = −0.02, SE = 0.01, p = .085) was significant, indicating that baseline adolescent–mother negative relationship quality was significantly greater than zero but did not, on average, change over time. The variance of both the mean (variance = .42, SE = .04, p < .001) and the slope (varia-nce = .02, SE = 0.00, p < .001) were significant, suggesting individual differences around these estimates. In other words, on average, adolescent–mother negative relationship quality was stable, but there were statistically significant differences in the trajectories of relationship quality across individuals in the sample. The slope and intercept were also negatively associated (r = −.42, p = .002), suggesting that youth reporting higher baseline adolescent–mother negative relationship quality demonstrated steeper decreases in negative relationship quality over the course of adolescence.
Next, we added ADHD symptoms at the eighth grade and sex as exogenous predictors of the latent intercept and slope factors. This model also provided a good fit to the data: χ2(df=5) = 5.72, p = .334, CFI = 1.00, RMSEA = 0.02 (90% CI = [0.00, 0.08]), and SRMR = .04. Both ADHD symptoms (β = .27, p < .001) and sex (β = .197, p = .002) were significant predictors of the intercept, indicating that girls and youth with higher ADHD symptoms at the eighth grade evidenced higher levels of adolescent–mother negative relationship quality at baseline. We then added a Sex × ADHD interaction term to the model. This model also fits the data well: χ2(df=6) = 7.00, p = .321, CFI = 1.00, RMSEA = 0.02 (90% CI = [0.00, 0.08]), and SRMR = .04. The interaction term was a significant predictor of both the intercept and slope factor. Post hoc multigroup analyses were then conducted to look at this model in separate groups of boys and girls. The multigroup model also fits the data well: χ2(df=9) = 8.01, p = .533, CFI = 1.00, RMSEA = 0.00 (90% CI = [0.00, 0.08]), and SRMR = .08. Boys demonstrated a significant and positive relation between Grade 8 (baseline) ADHD symptoms and the slope of adolescent–mother negative relationship quality (β = .34), whereas the relation between Grade 8 ADHD symptoms and the slope of adolescent–mother negative relationship quality was negative for girls (β = −.37). In other words, boys with higher levels of ADHD symptoms at the eighth grade reported steeper increases in adolescent–mother negative relationship quality relative to girls from eighth to 12th grades (see Table 2, Model 1). Alternatively, higher baseline ADHD symptoms were also associated with higher rates of adolescent–mother negative relationship quality for girls at baseline, but girls with high levels of ADHD symptoms also experienced a slower increase in negative relationship quality over time compared to girls with low ADHD symptoms.
Unstandardized (and Standardized) Parameter Estimates for Models Examining Sex × ADHD Symptoms Predicting a Latent Growth Curves of Negative Relationship Quality.

Note. CBCL = Child Behavior Checklist.
p < .05. **p < .01.
Finally, we examined a moderated mediation model in which we evaluated whether the intercept or slope of adolescent–mother negative relationship quality mediated the relation between eighth-grade ADHD symptoms and depression symptoms at Grade 12 differentially for boys and girls. The model continued to fit the data well: χ2(df=7) = 7.51, p = .378, CFI = 0.99, RMSEA = 0.02 (90% CI = [0.00, 0.07]), and SRMR = .03. We found that both the latent intercept and slope were significant and positive predictors of depressive symptoms, suggesting higher initial levels, and steeper increases in, adolescent–mother negative relationship quality were associated with increases in depressive symptoms. Moreover, the slope factor mediated the relation between the Sex × ADHD Symptom interaction term and 12th-grade depressive symptoms (indirect effect = −.27, SE = 0.12, 95% CI = [−0.50, −0.043]). Post hoc multigroup analyses were conducted to examine these differences in boys and girls; this model also fits the data well: χ2(df=11) = 8.75, p = .645, CFI = 1.00, RMSEA = 0.00 (90% CI = [0.00, 0.07]), and SRMR = .07. Boys continued to demonstrate a more positive relation between Grade 8 ADHD symptoms and the slope of adolescent–mother negative relationship quality, such that greater levels of ADHD symptoms in boys were associated with steeper increases in maternal negative relationship quality compared with girls. Greater increases in adolescent–mother negative relationship quality were positively associated with Grade 12 depressive symptoms in both sexes, controlling for ADHD symptoms. In other words, eighth-grade ADHD symptoms were associated with faster increases in adolescent–mother negative relationship quality for boys over time, which, in turn, were associated with greater 12th-grade depressive symptoms (see Figure 1).
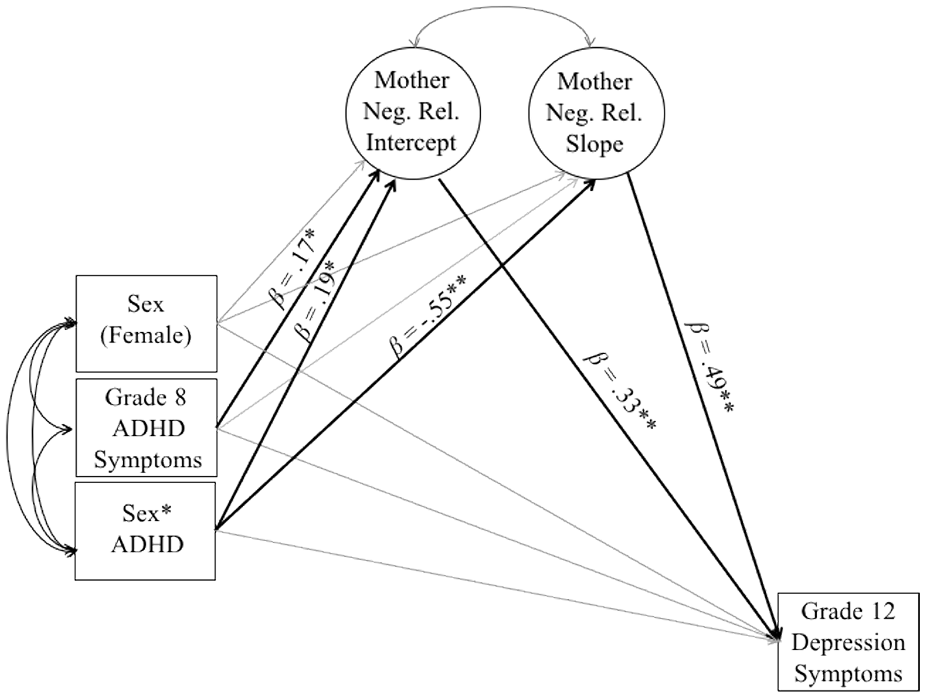
Latent growth curve mediation model with standardized path estimates.
Best Friend Negative Relationship Quality
Next, we examined an unconditional linear growth model of best friend negative relationship quality over time. Fit indices suggest an adequate fit to the data: χ2(df=3) = 10.15, p = .017, CFI = 0.90, RMSEA = 0.07 (90% CI = [0.03, 0.12]), and SRMR = .04. The mean of the intercept (M = 1.72, SE = 0.03, p < .001), but not the slope (M = −0.02, SE = 0.01, p = .135), was significant, suggesting that baseline best friend negative relationship quality is significantly greater than zero but that it does not, on average, change over time. Furthermore, the variance of the mean (variance = .18, SE = 0.03, p < .001) was significant while the variance of the slope (vari-ance = .01, SE = 0.00, p = .059) was marginally significant, indicating individual differences around these estimates. The slope and intercept were also correlated with each other (r = −.65, p = .006), suggesting that participants who reported greater levels of negative friendship quality at baseline evidenced decreases in negative relationship quality over the course of high school.
Next, we regressed the latent slope and intercept onto our baseline predictors, including eighth-grade ADHD symptoms and sex. The model continued to provide an adequate fit to the data: χ2(df=5) = 8.20, p = .146, CFI = 0.96, RMSEA = 0.04 (90% CI = [0.00, 0.10]), and SRMR = .03. Neither ADHD symptoms nor sex were significant predictors of the intercept or slope. We then added an interaction term (ADHD × Sex) as a predictor. Again, the model provided an adequate fit: χ2(df=6) = 11.84, p = .066, CFI = 0.93, RMSEA = 0.06 (90% CI = [0.00, 0.10]), and SRMR = .04. Results suggest that the interaction of sex and ADHD symptoms significantly predicted the latent slope of best friend negative relationship quality (β = −.57, p = .016). A post hoc multigroup model fits the data well: χ2(df=9) = 14.55, p = .104, CFI = 0.93, RMSEA = 0.06 (90% CI = [0.00, 0.12]), and SRMR = .08. Findings indicated that ADHD symptoms in the eighth grade were significantly associated with steeper increases in negative relationship quality with their best friend over time (across high school) for boys (β = .56) but not girls (β = −.21) (see Table 2, Model 2).
Finally, in a moderated mediation model, we examined whether changes in negative friendship quality mediated the relation between ADHD symptoms at the eighth grade and depressive symptoms at the 12th grade differentially for boys and girls. We regressed 12th-grade depressive symptoms onto the latent intercept and slope which were then regressed onto eighth-grade ADHD symptoms, sex, and a Sex × ADHD symptoms interaction term. The model provided an adequate fit to the data: χ2(df=7) = 12.34, p = .466, CFI = 0.93, RMSEA = 0.05 (90% CI = [0.00, 0.09]), and SRMR = .04. The Sex × ADHD interaction term continued to significantly predict the slope of negative relationship quality with the best friend through high school in the same direction as the previous model, but neither the slope nor intercept significantly predicted Grade 12 depressive symptoms.
Discussion
Youth with ADHD are at twice the risk for developing depression by the end of adolescence, yet less is known about the relative contributions of negative relationships with mothers and peers (and specifically, best friends) in predicting depression risk. Furthermore, no known research has examined the extent to which trajectories of negative relationships with best friends and mothers explain the association between ADHD and depressive symptoms across a high-risk developmental period (i.e., the transition from middle school to high school) and whether sex moderates these relations over time. Using a prospective longitudinal design and a community sample, this study sought to elucidate predictors of adolescent depressive symptoms in the 12th grade; namely, changes in adolescents’ negative relationships with their mothers and best friends across high school as a function of ADHD symptoms and sex. We examined a moderated mediation model in which we evaluated whether the relation between ADHD symptoms and the intercept and slope of mother and best friend negative relationship quality differed for boys and girls, and, in turn, whether this mediated the relation between ADHD symptoms and 12th-grade depression symptoms.
Negative Mother–Adolescent Relationship Quality
The quality of the adolescent–mother relationship in the eighth grade as well as the trajectory of adolescent–mother relationship quality from eighth to 12th grades predicted depressive symptoms in the 12th grade. Females were also at greater risk for negative mother–adolescent relationship quality than boys in the eighth grade. Furthermore, adolescents with elevated ADHD reported more negative relationships with their mothers in the eighth grade; this was especially true of females. In other words, independently, both ADHD and sex each cross-sectionally predicted poorer adolescent–mother relationship quality, with a significant interaction term indicating that higher levels of ADHD symptoms predicted increases in negative mother–adolescent relationship quality from eighth through 12th grades more so for boys than for girls. That is, boys with more ADHD symptoms experienced steeper increases in negative relationship quality with their mothers over the transition from eighth through 12th grades relative to girls. One rationale for males driving this relation between ADHD symptoms and increases in negative relationship quality with mothers may be that increases in negative relationship quality between females and mothers may occur earlier in development (e.g., early adolescence). In the general population, conflicts between mothers and adolescents peak in early adolescence with girls reporting more conflicts than boys (Laursen, 1995). Thus, it may be that this incline in girls’ negative maternal relationship was not captured in this study. Future research should examine this possibility.
In regard to predicting depressive symptoms, regardless of ADHD symptoms, higher baseline levels of mother–adolescent negative relationship quality as well as steeper increases in mother–adolescent negative relationship quality across high school predicted higher levels of depressive symptoms in the 12th grade. When examining the full mediation model, the association between ADHD symptoms in the eighth grade and growth in adolescents’ negative relationship quality with their mother was stronger for boys, and these changes, in turn, predicted depressive symptoms in the 12th grade. These findings correspond with the larger literature suggesting that family support, parent–child difficulties, and conflict mediate the association between ADHD and depressive symptoms (Barkley et al., 1992; Eadeh et al., 2017; Humphreys et al., 2013; Meinzer et al., 2015; Ostrander & Herman, 2006). The literature has neither identified sex as a moderator in the relation between ADHD symptoms and mother–adolescent negative relationship quality in adolescence nor examined the trajectories of mother and best friend relationships during the transition from middle school and high school in the context of ADHD and depressive symptoms. In children with ADHD, maternal rejection has not been shown to differ between boys and girls (Lifford et al., 2008). However, in one longitudinal study, ADHD symptoms predicted the degree of mother–son but not mother–daughter hostility (Lifford et al., 2009). Therefore, this study provided some clarity on the role played by child gender in the relation between ADHD and negative mother–adolescent relationship quality during the transition from middle school to high school and through the 12th grade. Specifically, changes in mother–adolescent relationship quality was a significant mediator of the association between ADHD symptoms in the eighth grade and depression symptoms in the 12th grade.
Negative Relationship Quality With Best Friend
Results suggest that neither ADHD symptoms nor sex predicted baseline or increases in negative relationship quality with best friends. While this result was surprising given the importance of peers in adolescence, these results are consistent with a study by Glass and colleagues (2012) that showed that ADHD symptoms were actually positively correlated with friendship quality. That is, ADHD symptoms may impact close friendships differently than peer relations. However, and in contrast with Glass and colleagues’ (2012) cross-sectional findings, the interaction between ADHD symptoms and sex was significant, suggesting that for boys, but not girls, ADHD symptoms predicted steeper increases in negative relationship quality with best friends from eighth to 12th grades. It is also important to note that the best friend that adolescents reported on in the eighth grade was not necessarily the same best friend that adolescents reported on in ninth and 12th grades. Therefore, results suggest that adolescent boys with elevated ADHD symptoms had increases in negative close relationship quality across the transition from middle school to high school despite the strong possibility that the best friend dyad in Grades 9 and 12 comprised different adolescents.
Strengths and Limitations
This study extends previous findings by indicating that ADHD not only predicts rejection (Hoza et al., 2005) from peers in general but also, in males, increases negative relationship quality with their current best friend across adolescence. Our results are also similar to those in reported in Humphreys et al. (2013) in that (a) adolescents with elevated ADHD symptoms had more negative interactions with their best friend at baseline and (b) the increase in negative relationship quality across high school did not mediate the relationship between eighth-grade ADHD symptoms and 12th-grade depressive symptoms. However, Humphreys and colleagues only examined the mediational role of peer support at one time-point where negative relationship quality was measured over time in this study.
The present findings elucidate the links between the quality of adolescent males’ relationships with their mothers and best friends across adolescence and how the quality of these relationships relate to their later depressive symptoms. Results from this study suggest that mother–adolescent relationships may be especially important in the context of elevated levels of ADHD symptoms among males. More specifically, increasingly negative mother–adolescent relationships from Grades 8 to 12 accounted for the association between eighth-grade ADHD symptoms and 12th-grade depressive symptoms. These findings support the importance of including parents in prevention and intervention programs for adolescents with elevated ADHD symptoms. Indeed, even within this unselected sample, negative relationship quality with mothers across high school was a key risk mechanism associated with the development of depressive symptoms in the 12th grade.
The strengths of this study need to be considered in light of the study’s limitations. First, although the study employed the use of parent-reported ADHD symptoms in a community sample, the gold-standard for ADHD assessment consists of using a combination of rating scales and diagnostic interviews as well as a multi-informant (i.e., parent and teacher report) approach (Pelham et al., 2005). A second limitation comes from using only adolescent report of relationship quality with their best friend and mother. Adolescents with ADHD tend to underreport impairment (Wasserstein, 2005), and thus negative relationship quality may have been underreported in this study. However, there is value in understanding how adolescents’ own perceptions of their relationships impact their symptoms. Future projects should incorporate the use of both parent-report and best friend report in addition to adolescents’ report of relationship quality. Positive aspects of relationships with mothers and best friends (e.g., warmth, support) might also mitigate risk between ADHD and depressive symptoms and should be considered in future research. In addition, relationship quality between adolescents and fathers was not examined here. Future research should investigate fathers’ role in the emergence of depression among youth with symptoms of ADHD. Another limitation is that a measure of baseline depressive symptoms (i.e., BDI) was not obtained. Future work should examine levels of depression in Grade 8 as well as changes throughout high school.
A final limitation is that all children were required to endorse having a best friend at the start of the study. Children with ADHD often have strained relationships with peers including being less liked and more rejected than those without ADHD (Hoza et al., 2005). Thus, during recruitment for the larger longitudinal study, some children with elevated ADHD symptoms may have been excluded due to not having a best friend. This possibility could have contributed to the lack of findings regarding best friend negative relationship quality and ADHD and depressive symptoms. However, despite this, the lack of mediation findings for peer negative relationship quality in this study findings is consistent with Humphreys and colleagues’ (2013) longitudinal study. Despite the limitations of our measure of peer relationship quality, only one other study has examined these relationships in relation to ADHD in adolescence.
Conclusion and Future Directions
Findings from this study and findings from extant literature (e.g., Humphreys et al., 2013) indicate that focusing intervention efforts on negative parent–child relationships rather than adolescent–best friend dynamics may prevent more adverse outcomes, including depressive symptoms. Early intervention for parent–adolescent conflict during this high-risk developmental period could serve to reduce greater mother–child dysfunction throughout adolescence and subsequent depressive symptoms. Interventions that aim to improve interactions between mothers and adolescents, particularly males with elevated ADHD symptoms, may be especially important for preventing depression at the transition from middle school through high school when relationships can contribute to the “storm and stress” that can characterize adolescence (Arnett, 1999). For instance, Meinzer and colleagues (2018) developed and piloted the Behaviorally Enhancing Adolescents’ Mood program (BEAM) to prevent depressive outcomes among adolescents with ADHD. BEAM targeted mediators of the relationship between ADHD and depression, one of which was family support. In addition, given that adolescents with ADHD report difficulties in self-regulation, treatments (e.g., Supporting Teens’ Academic Needs Daily; Challenging Horizons) have been developed to provide support (e.g., academic, social) for adolescents with ADHD (Evans et al., 2011; Sibley et al., 2013). This study suggests that negative relationship quality between adolescent males and their mothers represents one important mechanism by which youth with elevated ADHD symptoms can come to experience depression, indicating that parent involvement in treatment for this population is crucial. Future research should examine whether psychosocial interventions can alter the course of negative interactions with adolescents and their parents and whether, in turn, those improvements lead to reductions in depressive symptoms over the course of adolescence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was principally supported by a grant from the National Institute of Mental Health (MH58116), awarded to Dr. Kenneth H. Rubin.