
Abstract
ADHD is a neurodevelopmental disorder that affects about 5% of children (American Psychiatric Association [APA], 2013), making it one of the most prevalent childhood disorders. A more recent study even suggests a higher percentage. Result from the National Survey of Children’s Health states that 9.4% of children between 2 and 17 years old in the United States received an ADHD diagnostic (Danielson et al., 2018). Under the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013), the primary symptoms of ADHD are inattention, hyperactivity, and impulsivity behaviors that do not correspond to the child’s developmental level and that impair the child’s everyday functioning. Moreover, it is generally recognized that persons with ADHD have more attentional function deficits (e.g., Günther et al., 2011; Spronk et al., 2008) and more executive function deficits than persons without ADHD (e.g., Martinussen et al., 2005; Shallice et al., 2002; Willcutt et al., 2005). Attentional functions refer to the ability to supply a sustained mental effort (sustained attention), to focus one’s attention on relevant information (selective attention), and to divide one’s attention on multiple concurrent tasks (divided attention). Executive functions refer to the skills required to accomplish goal-directed tasks. The main functions are working memory, planning, cognitive flexibility, motor response inhibition, and interference control (Sergeant et al., 2002; Willcutt et al., 2005).
ADHD is more prevalent among boys, at a ratio of two to one (APA, 2013). A recent study has shown that 5.9% of boys and 3.04% of girls were diagnosed with ADHD before reaching 18 years old (Dalsgaard et al., 2019). The males to females ratio seems to be higher in clinical samples than in community samples (Gaub & Carlson, 1997; Nøvik et al., 2006; Ramtekkar et al., 2010). Although the percentage of girls with ADHD is nevertheless high (Staller & Faraone, 2006) and despite the consequences of the disorder for their psychosocial functioning (e.g., Rucklidge & Tannock, 2001), academic functioning (e.g., Hinshaw, 2002), and cognitive functioning (e.g., Biederman et al., 2008; Hinshaw et al., 2002), ADHD has been studied primarily in boys. It is reasonable to suppose that ADHD is experienced, diagnosed, and treated differently depending on the sex of the child affected. Two meta-analyses were published more than 15 years ago (Gaub & Carlson, 1997; Gershon, 2002a) to determine more clearly whether girls and boys with ADHD differed in terms of symptoms expression. Regarding sex differences on cognitive deficits associated with ADHD, the meta-analysis by Gershon (2002a) examined sustained attention, motor response inhibition, and interference control, and a more recent one by Hasson and Fine (2012) looked at sustained attention and motor response inhibition. Since the meta-analyses by Gaub and Carlson (1997) and Gershon (2002a) were published, efforts have been made to include girls in the samples of empirical studies. Results to date have been mixed. Whereas several studies support the existence of sex differences in the symptomatology of ADHD and in the cognitive deficits associated, others do not.
Sex Differences, Executive Functions, and Attentional Functions
According to research, girls with ADHD have more difficulty than girls without ADHD have on tasks that measure executive and attentional functions, whether in childhood (Hinshaw et al., 2002; Seidman et al., 2005), adolescence (Hinshaw et al., 2007; Seidman et al., 2005), or adulthood (Biederman et al., 2008; Miller et al., 2013). However, few studies have observed sex differences in the executive functioning of youths with ADHD (Hasson & Fine, 2012; O’Brien et al., 2010). Studies have suggested rather that girls have deficits comparable with those of boys, regarding inhibition (Houghton et al., 1999; Rucklidge & Tannock, 2002), cognitive flexibility (Houghton et al., 1999; Seidman et al., 2005), planification (Houghton et al., 1999), working memory (Rucklidge & Tannock, 2002), and attention (Seidman et al., 2005).
Two meta-analyses compared the executive and attentional functions of girls and boys with ADHD. Hasson and Fine (2012) and Gershon (2002a) focused on motor response inhibition and sustained attention, as measured via the CPT-II test (Conners, 1994). Only Gershon also considered interference control as measured by the Stroop test (Stroop, 1935) and the Matching Familiar Figures Test (Kagan, 1966). Gershon took into account all studies published from 1983 to 1999 that compared people of all ages with a valid ADHD diagnosis. Hasson and Fine, for their part, included all studies published from 1989 to 2006 but applied more restrictive selection criteria: only one instrument of measure (Continuous Performance Test–II [CPT-II]) was considered, age of participants was limited to 6 to 18 years, participants had to be unmedicated at the time of testing, and studies had to be published in a peer-reviewed journal. Whereas Gershon observed no significant difference between boys and girls, Hasson and Fine found that boys demonstrated a greater motor response inhibition deficit than girls did, although the effect size was small (d = 0.31). However, the differences mentioned above regarding the selection criteria used might explain the incongruence of the results.
Sex Differences and Primary Symptoms of ADHD
The meta-analyses by Gaub and Carlson (1997) and Gershon (2002a) assessed sex differences regarding the primary symptoms of ADHD as measured via behavioral questionnaires. Gaub and Carlson included studies with participants aged 13 and below with a minimum IQ of 80, and at least 10 participants per group. The two meta-analyses showed that boys with ADHD were more inattentive and hyperactive than girls with ADHD were. Where impulsive behaviors are concerned, there is no consensus on sex differences. Only the meta-analysis by Gershon has shown boys to have more impulsive behaviors than girls have.
Results from more recent studies are inconsistent. Some studies have suggested sex differences in ADHD symptoms. For example, Elkins et al. (2011) found that boys with ADHD were more hyperactive–impulsive than girls, but no difference in inattention symptoms was found. Results from a large study with participants from eight different countries rather suggest more inattention symptoms for boys and no difference for hyperactivity–impulsivity symptoms (Muller et al., 2011a). However, not all studies found differences between boys and girls with ADHD (M. Chen et al., 2008; Mayfield et al., 2016; Skogli et al., 2013).
Moreover, it is interesting to note that significant differences have emerged depending on whether behaviors were observed by teachers or parents. Parents have tended to report the same primary symptoms of ADHD in boys and girls (Graetz et al., 2005; Mayfield et al., 2016; Nøvik et al., 2006). Teachers, instead, have tended to report boys as more inattentive, hyperactive, and impulsive than they do girls (DuPaul et al., 2006; Hartung et al., 2002; Isaksson et al., 2016; Wang et al., 2015).
Knowledge Gap
A major limitation of the studies reviewed is that most recruited their participants in clinical settings rather than in the community. In fact, it has been demonstrated that girls with ADHD are not referred and diagnosed as well as boys are (Gershon, 2002b; Hinshaw & Blachman, 2005; Madsen et al., 2018; Quinn & Nadeau, 2002). Indeed, girls tend to be diagnosed much later than boys (Dalsgaard et al., 2019). Also, girls who are referred clinically tend to have more severe deficits and are thus not representative of girls with ADHD as a whole (Hinshaw, 2002; Hinshaw & Blachman, 2005; Rucklidge, 2010).
Furthermore, in the two meta-analyses that examined sex differences on primary symptoms of ADHD, most of the studies considered used the Diagnostic and Statistical Manual of Mental Disorders (2nd ed., DSM-II; APA, 1968) or Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-III-R; APA, 1987) diagnostic criteria for ADHD. However, these criteria changed considerably from the third to the fourth edition of the DSM. A new meta-analysis of studies that used the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) diagnostic criteria was clearly warranted.
The two meta-analyses to date that have looked at sex differences in the cognitive deficits associated with ADHD examined only motor response inhibition, sustained attention (Gershon, 2002a; Hasson & Fine, 2012), and interference control (Gershon, 2002a). As it happens, it is recognized that people with ADHD have other deficits that merit consideration in a meta-analysis, such as those relating to working memory, planning, and cognitive flexibility (Martinussen et al., 2005; Shallice et al., 2002; Willcutt et al., 2005). This would serve to arrive at a more comprehensive picture of the differences between girls and boys with ADHD regarding executive functioning.
Another critical aspect is to find out whether the sex differences observed in the youth population with ADHD vary by age group (childhood vs. adolescence) and ADHD type (predominantly inattentive, predominantly hyperactive–impulsive, combined). So far, the moderating effect of age has been considered by Gershon (2002a) alone, but the conclusions to be drawn are limited by the fact that children were compared against adolescents and adults together.
Study Objectives
Against this background, we undertook a meta-analysis to verify whether sex differences existed among children and adolescents with ADHD in terms of (a) primary symptoms of ADHD (inattention, hyperactivity, and impulsivity) and (b) executive and attentional functioning (attention, inhibition, working memory, cognitive flexibility, planification). To do so, we first compared boys and girls with ADHD on each variable. The moderating effects of age group, recruitment setting (clinical or community), informant (parent or teacher), ADHD type, and DSM version used for diagnosis were taken into account.
As a secondary goal, for the studies that included a typically developing control group (children and/or adolescents without ADHD), we compared girls with and without ADHD, as well as boys with and without ADHD, and then the difference between those two groups. This analysis of relative differences seems appropriate to us because the meta-analysis of Hasson and Fine (2012) suggests a greater difference in the level of inhibition between boys with and without ADHD, compared with girls with and without ADHD.
Method
Article Search and Selection
The methods were defined prior to the beginning of the search. Articles were searched by two separate investigators on October 4, 2017, in the following databases: PsycInfo/PsycArticles, PudMed, ERIC (with ProQuest and EBSCO), Scopus, Cochrane, and Education Source (with EBSCO). The following keywords were used: ADHD OR attention deficit disorder AND Gender OR sex AND (cognitive OR neuropsychological OR executive function OR shifting OR working memory OR inhibition OR planning) OR (symptom OR severity). The search terms were selected to cover all the variables included and were inspired by the keywords used in relevant articles. The search was limited to articles published from 1997 to 2017. A manual search of the references of the articles found was also carried out by the two investigators separately to uncover other articles. Eligible articles were those with boys and girls between 3 and 17 years with a valid diagnosis of ADHD according to the criteria of DSM-IV, Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000), or DSM-5 (APA, 1994, 2000, 2013), or CIM-10 (Classification statistique internationale des maladies et problèmes de santé connexes, Dixième révision; Organisation mondiale de la santé [OMS], 2008). Boys and girls had to be compared on at least one of the variables of interest measured by a valid instrument. The variables in question were the primary symptoms of ADHD, that is, inattention, hyperactivity, and impulsivity, as well as executive and attentional functions, namely, working memory, motor response inhibition, interference control, planning, cognitive flexibility, and attention. Validated instruments for ADHD symptoms were behavioral measures such as the Conners’ rating scales (Conners, 1997) or the ADHD-Rating Scale-IV-Parent (DuPaul et al., 1998). Instruments for cognitive functions included validated cognitive tasks such as the CPT (Conners, 1994), the Trail Making Test, or the Color-Word Interference Test (Delis–Kaplan Executive Functioning; Delis et al., 2001). Results for the measure had to be presented in a way that allowed us to calculate the effect size (e.g., means, standard deviations, sample size, p value). Articles written in languages other than English were eligible.
The articles were selected by two separate investigators as well. The articles were first screened on the basis of their title and abstract. An article was retained if any of the variables of interest was measured and the participants met the selection criteria. To avoid eliminating articles of relevance, we kept articles at this stage of the process even if a comparison of the sexes was not mentioned in the abstract. Next, a second wave of screening based on the full text of each of the articles retained was conducted by each investigator separately. At this point, articles had to meet all of the inclusion criteria. Interrater reliability was 88% (i.e., 272/310 articles). Disagreements were settled by consensus.
An assessment of the quality of the studies was also carried out by the two investigators separately. Any disagreement was again resolved by consensus. The assessment was informed by the Cochrane Collaboration’s tool for assessing risk of bias (Higgins & Green, 2011). The investigators had to rate the risk of bias (low, high, or unclear) in the following domains: selection bias, performance bias, evaluation process bias, results analysis bias, and reporting bias.
Statistical Analyses
The statistical analyses were run on Comprehensive Meta-Analysis–Version 3 (CMA; Borenstein et al., 2013). Sex differences in terms of ADHD symptoms and executive and attentional functioning were calculated using Hedges’ g as estimator, with a 95% confidence interval. For each variable, effect size was calculated for each individual study using the reported data (mean, standard deviations, and sample size; or p value and sample size; or means, sample size, and p value). If there were different measures of a variable in a study (e.g., number of inattention symptoms reported by parent and by teacher), each measure was first entered individually, and then the measures were grouped into a single effect size. A combined effect size was calculated for all the variables, using the random-effect model. The direction of the effect size was considered negative when boys showed more ADHD symptoms or executive and attentional deficits. To determine the existence of sex differences among children with or without ADHD, the same procedure was applied to calculate effect size for each sex and then the difference between the two effect sizes for each variable.
Effect size heterogeneity was assessed through the Q statistic and the I2 statistic, which is reported to indicate the percentage of the total variance in effects due to actual differences between the samples. For variables where heterogeneity proved significant, subgroup analyses were conducted to determine the potential moderating effects of age group (3–5, 6–11, 12–17 years old), ADHD type (combined, inattentive, or hyperactive–impulsive), recruitment setting (community, clinics), informant (parent, teacher), and DSM version used (DSM-IV, DSM-IV-TR, DSM-V).
Publication biases were assessed using Begg’s rank correlation test (Begg & Mazumdar, 1994) and Egger’s test (Egger et al., 1997). These tests serve to assess the symmetry of the funnel plot, where asymmetry indicates a potential publication bias.
Results
Study Selection
The article selection process is summarized in Figure 1. The database search yielded 3,624 articles, of which 1,144 duplicates were eliminated, leaving 2,480. Screening based on title and abstract resulted in 2,178 articles being eliminated. The remaining 302 articles were screened based on the full text. From these, 252 were eliminated for the following reasons: no valid ADHD diagnosis, no relevant variable measured, no boy–girl comparison, age range not respected (n = 247), and full text could not be found (n = 5). The remaining 50 articles were included in the meta-analysis. A manual search of the references of these articles yielded four other relevant articles, for a total of 54 articles involving 47 different samples. The characteristics of these studies are presented in Table 1.

Flowchart of the search and selection procedure.
Characteristics of the Studies Included in the Meta-Analysis.
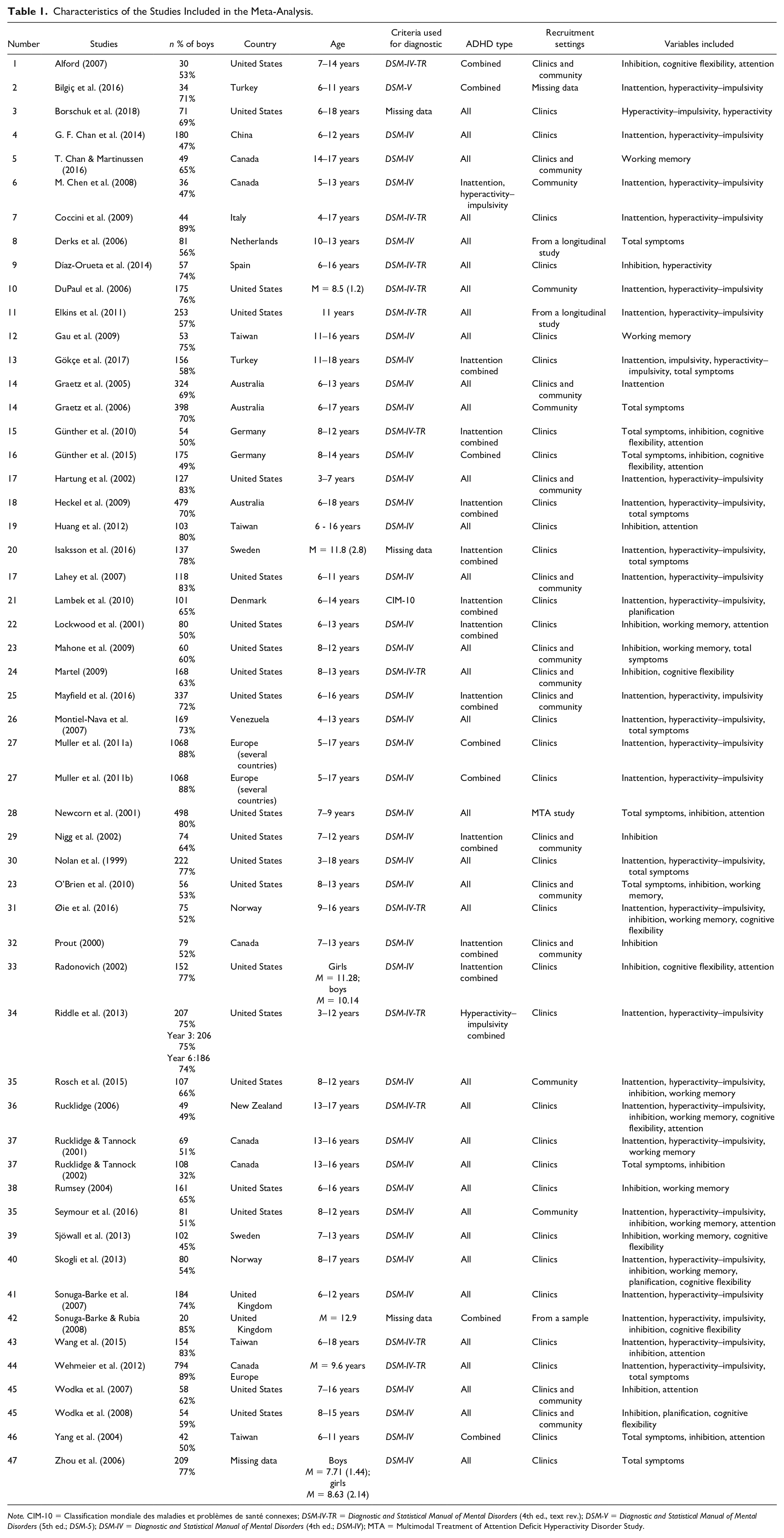
Note. CIM-10 = Classification mondiale des maladies et problèmes de santé connexes; DSM-IV-TR = Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.); DSM-V = Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5); DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV); MTA = Multimodal Treatment of Attention Deficit Hyperactivity Disorder Study.
Assessment of Quality of Studies
Generally speaking, the principal risks of bias concerned participant selection and performance. Regarding selection biases, numerous studies used samples drawn from clinical settings, which limited their representativeness. A fair number of studies reported no information regarding participant attrition. Moreover, risks of performance biases were also present. The description of the methodological procedures did not always allow assessing risk of bias, or the method used did not allow doing blind evaluations regarding presence or absence of ADHD in participants or regarding research questions and objectives. The risks of bias were generally low regarding the relevance of the evaluation tools, the data analysis techniques, and the reporting of results. A summary of the quality of included studies is provided in Supplemental Table S1.
Comparing Boys and Girls With ADHD
Sex differences in ADHD symptoms
The results of the meta-analysis are presented in Table 2. A positive effect size indicated more severe symptoms in girls, whereas a negative effect size indicated more severe symptoms in boys. Regarding the primary symptoms of ADHD, only one significant difference emerged between boys and girls with ADHD. Boys expressed more hyperactivity symptoms than girls did (g = −0.154, p = .010, 95% CI = [−0.339, 0.030]). No sex difference was observed on any of the other variables.
Differences Between Boys and Girls With ADHD.
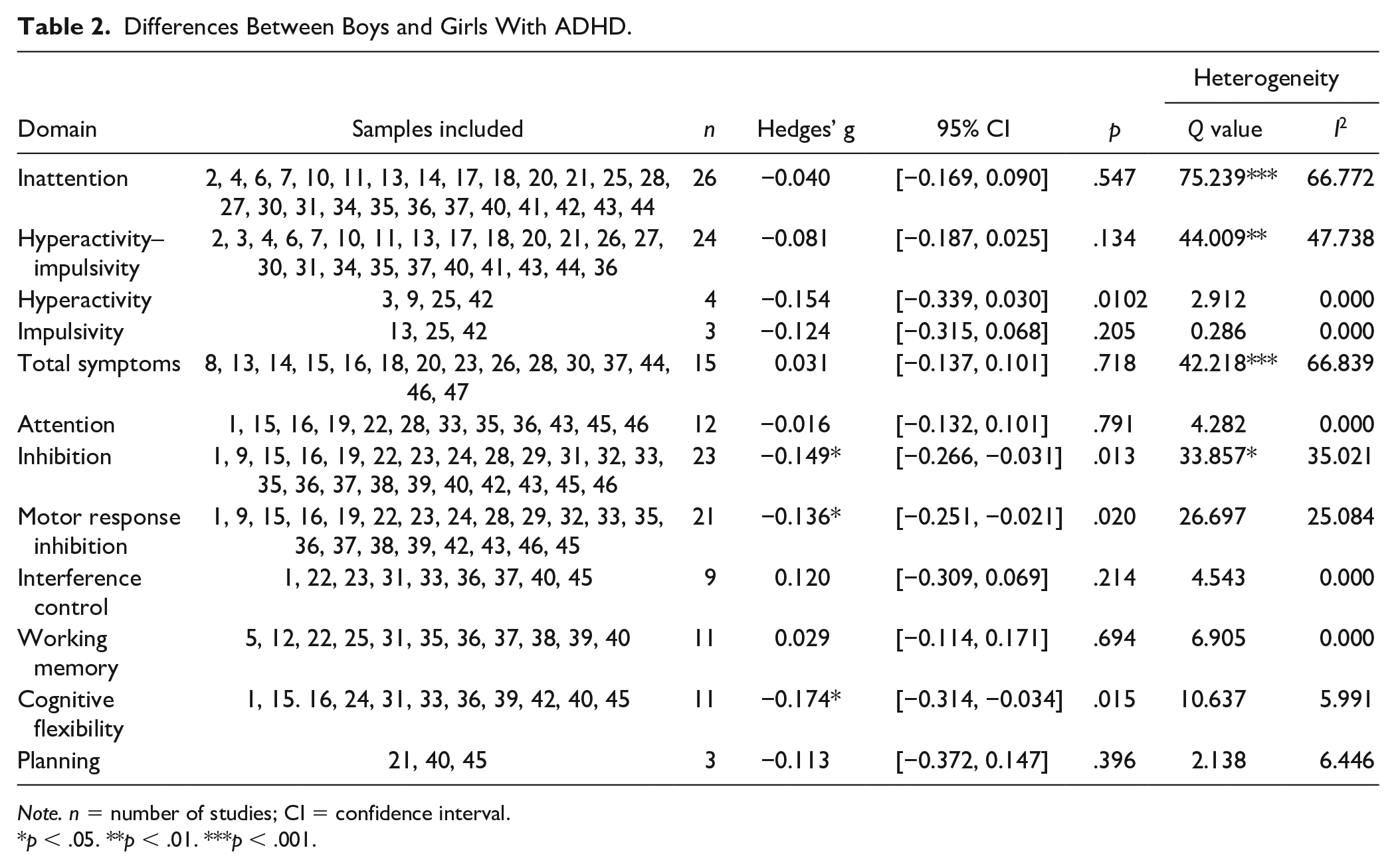
Note. n = number of studies; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
When results were analyzed separately for parents and teachers, other sex differences emerged. Teachers reported boys had more inattention (g = −0.304, p = .006, 95% CI = [−0.521, −0,087]) and hyperactive–impulsive (g = −0.204, p = .022, 95% CI = [−0.377, −0.030]) behaviors than girls did.
The heterogeneity tests (Table 2) showed significant heterogeneity between effect sizes for inattention behaviors, Q(26) = 75.239, p < .001, I2 = 66.8%, hyperactivity–impulsivity behaviors, Q(24) = 44.009, p = .005, I2 = 47.74%, and total symptoms, Q(15) = 42.218, p < .001, I2 = 66.8%. Consequently, we ran analyses on a subgroup to determine the potential sources of this heterogeneity. These revealed no difference by age group, recruitment setting, or DSM version used with respect to level of inattention, level of hyperactivity–impulsivity, and total symptoms (see Table 3). The principal source of heterogeneity was the informant (parents or teachers), where inattention symptoms were concerned, Q(31) = 7.831, p = .005, as a sex difference emerged only when children were assessed by teachers. No moderating effect of informant was observed with respect to hyperactive–impulsive behaviors, Q(29) = 0.816, p = .366, and total symptoms, Q(18) = 2.285, p = .131.
Moderator Analyses.

Note. DSM = Diagnostic and Statistical Manual of Mental Disorders; n = number of studies.
Test of the difference between effect size in each subgroup.
p < .05. **p < .01.
Sex differences in cognitive functions
Regarding executive and attentional functions, significant differences between boys and girls with ADHD emerged on inhibition (motor response inhibition and interference control together; g = −0.149, p = .013, 95% CI = [−0.266, −0.031]) and cognitive flexibility (g = −0.174, p = .015, 95% CI = [−0.314, −0.034]). Accordingly, boys scored higher than girls did in this respect, though the effect sizes proved small. No significant difference was noted on working memory (g = 0.029, p = .694, 95% CI = [−0.114, 0.171]), planning (g = −0.113, p = .396, 95% CI = [−0.372, 0.147]), and attention (g = −0.016, p = .791, 95% CI = [−0.132, 0.101]).
A significant heterogeneity across effect sizes was present for inhibition, Q(23) = 33.857, p = .051, I2 = 35.0%. Subgroup analyses revealed a moderating effect of ADHD type, Q(22) = 6.945, p = .008. In this regard, only studies that included youths with ADHD inattentive type noted a larger deficit in boys (g = −0.179, p = .002, 95% CI = [−0.290, −0.068]). Age group, Q(17) = 3.343, p = .188, recruitment setting, Q(21) = 1.863, p = .394, and DSM version, Q(23) = 0.169, p = .681, used did not appear to have an influence.
A separate analysis of effect sizes by inhibition type, that is, motor response inhibition or interference control, revealed a sex difference only for the former, with boys presenting more difficulties (g = −0.136, p = .020, 95% CI = [−0.251, −0.021]).
Comparing Youths With and Without ADHD
When youths with ADHD were compared against those without, significant differences emerged between the two groups on all the variables, in both girls and boys (see Table 4). However, when we compared the effect sizes for girls against those for boys, no significant difference was observed for any of the variables measured. In other words, boys and girls with ADHD presented significantly more primary symptoms and executive and attentional deficits than did their peers without ADHD, and effect sizes were not significantly different between the sexes.
Differences Between Youths With and Without ADHD, by Sex.

Note. n = number of studies; CI = confidence interval.
Test of the difference between effect size for girls and effect size for boys.
p < .05. **p < .01. ***p < .001.
Publication Bias
Egger’s test raised the possibility of a publication bias in the studies that measured hyperactivity–impulsivity (t = 2.296, p = .032) and cognitive flexibility (t = 3.194, p = .011), whereas the rank correlation test raised the possibility of a publication bias only for studies that measured hyperactivity–impulsivity (τ = 0.366, p = .012). However, for all the other variables, the analyses revealed no potential publication bias. This suggested that the results of the present meta-analysis did not seem to be affected by a publication bias.
Discussion
The aim of this meta-analysis was to verify the presence of differences between boys and girls in terms of ADHD primary symptoms and of executive and attentional functioning. The main results show that boys with ADHD manifest more hyperactive behaviors and bigger inhibition and cognitive flexibility problems than girls with ADHD do. This meta-analysis confirms also that youths with ADHD present more primary symptoms of ADHD and more problems in terms of executive and attentional functions than do youths without ADHD, regardless of sex.
As for ADHD symptoms, boys with ADHD are more hyperactive than girls with ADHD are, which is consistent with results obtained in earlier meta-analyses (Gaub & Carlson, 1997; Gershon, 2002a). However, other sex differences emerge when effect sizes are compared by informant type (parent or teacher). Indeed, only according to teacher reports are boys more inattentive and hyperactive–impulsive than girls are. Various hypotheses might explain these results.
First, in replicating the results obtained by Abikoff et al. (1993), Jackson and King (2004) claimed that a halo effect was at play where teacher reports of ADHD symptoms were concerned. The authors demonstrated that the presence of oppositional behaviors increased the ADHD symptoms reported by teachers, but only for boys (Jackson & King, 2004). Thus, this tendency might potentially contribute to the sex difference observed, as boys with ADHD are more likely to manifest externalizing behaviors than girls with ADHD are (Nussbaum, 2012). Teachers might also underestimate symptoms in girls, given that, compared with boys, their symptoms are less disruptive. Indeed, the demands of the school setting might underscore the more disruptive behaviors of boys, such as agitation or opposition, which are known to interfere with classroom management and student learning. Furthermore, contrary to parents, teachers are in contact with numerous children and are trained in child development. Thus, it may be easier for them to identify ADHD symptoms and, in turn, potential sex differences, given that they can more easily make comparisons against what is normally expected for children of the same age.
Regarding executive functions, results show a sex difference in inhibition, with boys demonstrating greater deficits than girls do. This is not consistent with previous meta-analysis by Gershon (2002a), who found no sex differences in tasks measuring inhibition. In our meta-analysis, the ADHD type of the participants included in the studies moderates this result. Indeed, studies that included youths with ADHD inattentive type were the ones to report a significant sex difference, rather than studies that included only youths with ADHD combined type. It has been argued that ADHD types are different disorders with different cognitive deficits (Barkley, 2005). Consequently, future studies would do well to specify ADHD type more clearly.
Comparing effect sizes by inhibition type examined shed some fresh light on the difference observed between boys and girls and could also explain, in part, the different results obtained. A significant difference emerges only on tasks measuring motor response inhibition, with boys exhibiting a larger deficit than girls do. This result is consistent with Hasson and Fine (2012), who found that boys made more errors of commission on the CPT than girls did. However, there is no difference where interference control is concerned.
In sum, our results suggest on the whole that the behavioral expression of ADHD symptoms differs by sex: Girls are less hyperactive and manifest less motor response inhibition difficulties. However, like boys, they are inattentive and have interference control problems. These results are important in that, on one hand, they underscore the fact that girls have symptoms that are more subtle and, consequently, less disruptive, which may undermine their chances of being referred clinically. These results thus support the idea to the effect that current diagnostic criteria are ill-adapted to properly screen girls with ADHD (Hinshaw & Blachman, 2005; Nadeau et al., 1999; Nussbaum, 2012; Ohan & Johnston, 2005; Quinn & Nadeau, 2002; Roberts et al., 2014). Indeed, the group of hyperactivity–impulsivity criteria comprises six items describing hyperactive behaviors and three items describing behaviors involving motor response inhibition. In light of these results, it seems that most of these criteria refer to behaviors more commonly manifested by and more easily noted in boys. This points to a serious limitation of the DSM-5, namely, that symptoms are not modulated according to sex. This constitutes a major obstacle when it comes to recognizing and diagnosing girls with ADHD, as it might be harder for girls to meet the hyperactivity–impulsivity diagnostic criteria. This could lead to a wrong diagnosis or to late diagnosis and, over time, to a worsening of symptoms (Dalsgaard et al., 2019; Ohan & Johnston, 2005; Quinn & Madhoo, 2014) and to associated problems, such as academic, social, and psychological difficulties (Bussing et al., 2010, 2012; Harpin et al., 2013). Moreover, the costs of the disorder over the long run cannot be neglected, as difficulties can persist into adulthood (Quinn & Madhoo, 2014). The long-term effects of untreated ADHD include problems regarding self-esteem (Harpin et al., 2013; Shaw et al., 2012), suicidal behaviors (Fitzgerald et al., 2019), psychotropic drug addiction (Shaw et al., 2012), social functioning (Harpin et al., 2013; Shaw et al., 2012), job performance (de Graaf et al., 2008; Shaw et al., 2012), and antisocial behaviors (Shaw et al., 2012). Also, it has been suggested that girls with ADHD may have higher relative premature deaths than boys with ADHD (Dalsgaard et al., 2014) and higher risk of developing schizophrenia (Díaz-Orueta et al., 2014). According to one study, women with untreated ADHD are at higher risk than men are of developing an affective, eating, or somatic disorder (Rasmussen & Levander, 2009).
Our study also shows that boys with ADHD have more cognitive flexibility problems than girls do. This could be explained by a later brain development in boys than in girls (Lenroot et al., 2007; Thompson et al., 2005), especially for later developing skills such as cognitive flexibility (O’Brien et al., 2010). However, working memory, planning, and attention deficits are just as common in boys as in girls. In other words, our results show that girls with ADHD have difficulties regarding executive and attentional functioning. In sum, girls with ADHD do not differ from boys with ADHD in many domains of cognitive functioning and they have significantly more severe difficulties across the executive and attentional functions measured relative to girls without ADHD. This meta-analysis is the first to examine sex differences on cognitive flexibility, working memory, and planning.
Limitations and Future Research
Some of the methodological limitations of studies of sex differences in ADHD also apply to the results of our meta-analysis. For example, a large proportion of the samples considered were drawn from clinical settings (29 of 47 samples with participants exclusively from a clinical setting and nine of 47 samples with participants from both a clinical setting and the community). This poses a problem, in that, these samples are not representative of girls with ADHD, given that girls from clinical settings are those more severely affected by the disorder (Hinshaw, 2002; Rucklidge, 2010). In addition, using the DSM criteria (IV, IV-TR, or 5) makes it harder to identify girls with ADHD, as these criteria were developed based on samples composed essentially of boys. As a result, girls recruited for research may be those who present a profile most like that of boys. This could limit the sex differences that might otherwise be observed in general-population samples. This notwithstanding, sex differences did emerge, and the results did not seem to be moderated by recruitment setting. However, this result must be interpreted with caution given the small number of studies that have recruited in the community. Consequently, to arrive at a more representative profile of youths with ADHD, it is essential that future studies draw more of their participants from the community.
Another limitation of this meta-analysis concerns the small number of studies found, as this restricts the interpretation of results for some variables or subgroups. Moreover, we managed to find only a few sources of heterogeneity in the results obtained. Other potential sources remain to be investigated, such as presence of concurrent disorders (e.g., anxiety), a potential moderator that could not be examined in our meta-analysis for lack of suitable data in the studies considered. The prevalence of disorders concurrent with ADHD was given at times, but no study presented specific results for groups of children with concurrent diagnoses. This did not allow us to examine differences between groups with and without concurrent disorders. It would have been worthwhile to assess the moderating effect of this variable given that concurrent disorders are common in youths with ADHD (APA, 2013), and some sex differences seem to exist in the prevalence of certain disorders. For example, it has been reported that boys are more likely to present externalizing problems and that girls are more likely to present internalizing problems (Biederman et al., 1999; Hartung et al., 2002; Hinshaw, 2002; Quinn & Madhoo, 2014; Staller & Faraone, 2006; Zalecki & Hinshaw, 2004), a factor that could play a role in the manifestation, symptom severity, and treatment of ADHD. Indeed, a similar same sex difference is found in individuals without ADHD and it has been suggested that ADHD increases the relative risk of a comorbid anxiety more so in males than in females, both in children and adolescents (Ottosen et al., 2019) and in adults (Chen et al., 2018).
Cultural differences are another potential moderator that could have been explored. The majority of the samples in our meta-analysis came from North America (United States n = 17, Canada n = 4) or Europe (n = 13), with a minority from Asia (n = 5), Oceania (n = 3), South America (n = 1), or several countries (n = 4). It has been suggested that recognition of ADHD symptoms and referral of boys and girls with ADHD varied a lot between countries (Nøvik et al., 2006).
Yet another limitation of our meta-analysis lies in the fact that most of the studies considered included participants from different age groups (0–5, 6–11, 12–17). This made it difficult to compare subgroups. As it happens, several characteristics specific to the development in girls (e.g., earlier onset of puberty, hormones) might influence their behavioral and cognitive profile. The role of these characteristics needs to be examined in future research (Nussbaum, 2012; Quinn & Madhoo, 2014).
Future studies will need to focus special attention on how they report data with respect to age groups and concurrent disorders. Furthermore, it would be useful to verify the impact of characteristics specific to each sex, and to do so as a function of development. Other sources of heterogeneity might then come to the fore. It would also be worthwhile to verify whether other factors such as emotional regulation, social relations, self-esteem, and the development of coping strategies characterize the profile of girls with ADHD. These variables were identified by Quinn and Madhoo (2014) as potentially characteristic of girls with ADHD. With these data, we will be able to refine the behavioral, affective, and cognitive profile of girls with ADHD and thus facilitate their identification.
In summary, a different behavioral profile between boys and girls with ADHD is highlighted by our results. Boys exhibit more hyperactivity behaviors and greater difficulty in inhibiting a motor response. These results highlight that the current diagnostic criteria do not correspond to the behavioral expression of ADHD symptoms in girls. There is, therefore, still work to be done, in particular, to set up an evaluation process taking into account the specific characteristics of the girls’ profile. Addressing the issue will then be a priority, so that health and school professionals can have good screening tools and can develop accurate knowledge to recognize and refer girls to ADHD, as well as help them to develop their full potential.
Supplemental Material
Supplementary_material_ – Supplemental material for Meta-Analysis of Sex Differences in ADHD Symptoms and Associated Cognitive Deficits
Supplemental material, Supplementary_material_ for Meta-Analysis of Sex Differences in ADHD Symptoms and Associated Cognitive Deficits by Maryanne Loyer Carbonneau, Martin Demers, Marc Bigras and Marie-Claude Guay in Journal of Attention Disorders
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.