
Abstract
Introduction
ADHD is a highly prevalent neurodevelopmental disorder with developmentally inappropriate symptoms of inattention and hyperactivity/impulsivity (American Psychiatric Association [APA], 2003).Since the publication of DSM-IV in 1994, diagnosis of ADHD requires that ADHD symptoms and impairments be present in multiple settings (usually at home and school) (APA, 1994); thus, reports of ADHD symptoms from both parents and teachers are required to assist in making a diagnosis of ADHD. However, the concordance between parent and teacher reports of ADHD symptoms is weak in clinical practice and research (Mitsis et al., 2000; Murray et al., 2007). Some clinically referred children show atypical heightened ADHD symptoms in just one specific situation (Cohen & Minde, 1983; Rapoport et al., 1986; Rommelse et al., 2015). For example, children with “school-specific ADHD” have ADHD symptoms reported exclusively by the teacher, with only minimal or sub-clinical ADHD symptoms reported by the parents; “home-specific ADHD” refers to the opposite pattern (Ho et al., 1996; Weber et al., 2007).
Several studies have proposed that such situational ADHD may represent the variation in the child’s regulation of attention and impulsivity according to the different social and cognitive demands at home or school (Dirks et al., 2012; Rommelse et al., 2015). However, the different roles of the informants (i.e., parents vs. teachers) and their different experiences with the child lend each a unique perspective, which may also contribute to the variability in ADHD symptoms reported in different settings (Dirks et al., 2012; Rommelse et al., 2015). It has been proposed that teacher-reported ADHD symptoms may be related to the structured learning environment in schools, which requires greater cognitive capacity than the home environment (Ho et al., 1996; Szatmari et al., 1990). Studies have also shown that ADHD symptoms reported by parents are related to parental stress and weak family function (Dirks et al., 2012; Ho et al., 1996). However, few studies have used group comparisons of situational ADHD to assess whether these children have different cognitive capacities or parent-child relationships (Rommelse et al., 2015).
ADHD symptoms vary with context (APA, 1994). Symptoms are suppressed in specific contexts, such as when there is a contingent reward (Douglas & Parry, 1983), when there is adult supervision (Douglas & Parry, 1983), or while engaged in a novel and enjoyable activity (Morsink et al., 2017). In contrast, symptoms are prominent when the environment is structured and lacks flexibility, as in schools (Offord et al., 1996). Several studies have demonstrated that teacher-reported ADHD symptoms are associated with children’s performance on standardized cognitive tasks (Cho et al., 2011) but that parent-reported symptoms are not. The greater cognitive demands of the school setting may provide teachers with more opportunities to observe impaired attentional and inhibitory functioning in children with ADHD symptoms. Jacobson et al. (2018) found that performance on an inhibitory control task was sensitive to reports of the children’s inhibitory control in the classroom. Hence, deficits in neurocognitive performance may be a contextual risk factor for teacher-reported ADHD symptoms (Cho et al., 2011; Rommelse et al., 2015).
In clinical practice, parental reports have generally been treated as the most accurate information for clinical evaluation of ADHD, owing to the familiarity of the parents with their children’s daily life and behavioral history (Murray et al., 2007). However, several studies have found that parental reports of ADHD symptoms are linked to impaired family relationships (Ho et al., 1996; Rommelse et al., 2015) and parental stress (Mofokeng & van der Wath, 2017). Parents with higher levels of stress tend to over-evaluate the severity of ADHD symptoms compared with teacher reports (Chen et al., 2017; Yeguez & Sibley, 2016). The associations between parents’ perception of the severity of ADHD symptoms and the parent-child relationship are, therefore, bidirectional (Lifford et al., 2008). Hence, parenting style and parental stress may be family-context risk factors for parent-reported ADHD symptoms.
It is evident that situational inattention/hyperactivity does not meet the DSM-5 requirements for ADHD diagnosis (APA, 2013), but it provides an opportunity to explore which context-dependent risk factors are related to the ADHD symptoms reported by different informants (Dirks et al., 2012; Rommelse et al., 2015). Despite this, situational ADHD has not been well studied. In particular, prior studies of situational ADHD have tended to combine children with school-specific ADHD and children with home-specific ADHD into a single situational ADHD group (Beck et al., 1990; Tripp & Luk, 1997). However, such an experimental design precludes the discrimination of differential risk factors for children with school-specific ADHD and those with home-specific ADHD. To our knowledge, Ho et al. (1996) were the first to conduct research among four groups of children: those with pervasive hyperactivity (home and school), those with school-specific hyperactivity, those with home-specific hyperactivity, and a control group. Ho et al. (1996) found that the school-hyperactivity group was associated with low intelligence, poor academic performance, and motor clumsiness. They also found that the home-hyperactivity group was associated only with a tense family relationship without impaired cognitive capacity or lower academic performance in school. The pervasive-hyperactivity group had higher motor activity and a higher percentage of children with delayed language development than the other groups. These findings support the hypothesis that situational hyperactivity is sensitive to different contextual factors, according to whether teachers or parents report the hyperactivity. However, more studies are needed to replicate these findings, especially in preschool-age children.
ADHD symptoms often begin during the preschool years (Campbell et al., 2000; Halperin et al., 2012; Halperin & Healey, 2011). At this age, ADHD symptoms are mainly reported by parents and teachers (Chen et al., 2017; Jacobson et al., 2018). Hence, investigating situational ADHD symptoms as reported by different informants may offer vital information about the contextual risk factors in preschool-aged children, enabling better assessment and intervention at this age. In the current study, we used the Conners Kiddie Continuous Performance Test (K-CPT) (Barnard et al., 2015) and the Color Flanker Task (Lindqvist & Thorell, 2009) as objective measures of attention and inhibitory control. To measure the severity of ADHD symptoms as well as internalizing and externalizing behavioral problems, we used several subjective rating scales with parent and teacher versions. We also included measures of parental stress and of parents’ perceptions of their parenting. Preschoolers were assigned to one of the four groups according to the severity of their ADHD symptoms as reported by their teachers and parents. The four groups were as follows: Pervasive high-ADHD-symptoms (PHA), school-situational high-ADHD-symptoms (SHA), home-situational high-ADHD-symptoms (HHA), and pervasive low-ADHD-symptoms (PLA). Based on the findings of past studies, we formulated three hypotheses: (a) preschoolers with SHA have significant impairments in attention and inhibitory control; their parents perceive their parenting to be less harsh and have lower parental stress, (b) preschoolers with HHA have a worse relationship with their parents; their parents perceive their parenting to be harsh and feel severe parental stress, and (c) Preschoolers with PHA have impairments in attention and inhibitory control; their parents also perceive their parenting to be harsh and have high levels of parental stress.
Method
Participants
Two hundred and sixty children aged 4 or 5 were recruited from the community (n = 153) or hospitals (n = 107). The 153 preschoolers recruited from the community were referred to the study by teachers at the New Taipei City and Taoyuan City kindergartens based on parental interest in the study. We recruited 107 preschoolers from the hospitals by the senior child psychiatrists at the National Taiwan University Hospital (NTUH), Taipei, Taiwan, or the Chang Gung Memorial Hospital (CGMH), Linkou, Taiwan. Teachers or parents had expressed prior concern about ADHD symptoms in these participants. Thirty preschoolers were excluded, including 27 preschoolers who did not complete the assessments (25 lacked teacher reports, two did not receive the computerized lab task). Three preschoolers who met one of the following exclusion criteria: (a) estimated Full-Scale IQ scores (estimated FSIQ) less than 80, (b) developmental delays, autism spectrum disorders, major psychiatric disorders, seizures, or brain injuries, based on the clinical evaluation by board-certificated child psychiatrists or as reported by the parents.
We used the parent (Gau et al., 2008) and teacher (Gau et al., 2009) versions of the Swanson, Nolan, and Pelham (SNAP-IV) rating scale to assess ADHD symptoms and to assign participants to four groups. The four groups were: (a) the PHA group (n = 42): preschoolers with six or more symptom items in the SNAP inattention (IA) category or six or more symptom items in the SNAP hyperactivity/impulsivity (HI) category, in both the parent report and the teacher report, (b) the SHA group (n = 30): preschoolers with six or more symptom items in either the IA category or the HI category in the teacher report and four or fewer symptom items in each of the IA and HI categories in the parent report, (c) the HHA group (n = 27): preschoolers with six or more symptom items in either the IA category or the HI category in the parent report and four or fewer symptom items in each of the IA and HI categories in the teacher report, and (d) the PLA group (n = 111): preschoolers with four or fewer symptom items in each of the IA and HI categories in both the parent report and the teacher report. Twenty participants did not meet the criteria for any of the four groups.
Measurements
Swanson, Nolan, and Pelham Scale, Version IV (SNAP-IV)—Chinese Version
The Chinese version of SNAP-IV contains 26 items, each rated on a 4-point Likert scale, including the core DSM-IV-derived ADHD subscales of inattention (items 1–9), hyperactivity/impulsivity (items 10–18), and symptoms of oppositional defiant disorder (items 19–26). Each item is rated from 0 (not at all) to 3 (very much). A score of 2 (quite a bit) or 3 was coded as indicating the presence of the behavioral symptom; scores 0 or 1 were coded as the absence of the behavioral symptom (Swanson et al. 2001). Gau et al. (2008, 2009) developed the Chinese version and published the normative data as well as the psychometric properties for the parent (Gau et al. 2008; Yeh et al., 2008) and teacher (Gau et al., 2009) reports, with good psychometric reliability and validity. The Chinese SNAP-IV has been widely used in clinical screening and research in Taiwan (Chen et al., 2017; Hwang-Gu et al., 2019; Shang et al., 2015; Tsai et al., 2017). We used SNAP-IV as reported by parents and teachers as the basis for classifying preschoolers into the four groups described above (PHA, SHA, HHA, and PLA).
Child Behavior Checklist (CBCL/1.5–5) and Caregiver–Teacher Report Form—Chinese Versions
The child behavior checklist (CBCL) is a widely used screening measure to assess children’s behavioral and emotional problems (Achenbach & Ruffle, 2000). Parents completed the CBCL/1.5–5 and kindergarten teachers completed the Caregiver–Teacher Report Form (C-TRF; teacher version). The Chinese versions of the CBCL/1.5–5 and C-TRF were translated by Chen et al. (2009). Eight narrow bands (anxious/depressed mood, somatic complaints, aggressive behaviors, conduct behaviors, sleep problems, attentional problems, social problems, and other) and two broad dimensions (internalizing and externalizing syndromes) are derived from the emotional and behavioral items on the CBCL/1.5–5 and C-TRF. Each item is rated on a 3-point Likert scale, scored 0 (not true), 1 (somewhat or sometimes true), or 2 (very true or often true). The Chinese versions of the CBCL and TRF have been used to screen children for behavioral and emotional problems. Cronbach’s alpha coefficients for the internalizing syndromes and externalizing syndromes from the CBCL/1.5–5 and C-TRF ranged from .90 to .96 in this study, indicating good internal consistency for both the parents’ and teachers’ reports.
Parenting Stress Index-Short Form—Chinese version
The Parenting Stress Index-Short Form (PSI-SF), developed by Abidin (1995), is one of the most widely used tools for measuring stress in parents of children with ADHD (Gerdes et al., 2012; Vitiello et al., 2007). The Chinese version of the PSI-SF was translated by Wong (2003). It contains 34 items rated on a 5-point Likert scale ranging from 1 (strongly agree) to 5 (strongly disagree), including 11 parental distress items, ten parent-child dysfunction items, and 13 difficult-child items. In this study, the Cronbach’s alpha value for the total scores was .93, and those for each of the three subscales ranged from .88 to .93.
Parenting Perceptions Scale
We used the 17-item revised parenting perceptions scale of Wei and Yang (2010). This scale has four components: accepting (e.g., “I will ensure my child feels that he/she has the right to have his/her own opinion and the opportunity to express it.”), punishing (e.g., “I will punish my child for talking back or resisting.”), indulgent (e.g., “If I refuse to buy something my child wants and he/she cries about it, then I will buy it for him/her.”), and ignoring (e.g., “I don’t know who my child’s good friends are.”). Each item is rated on a 5-point Likert scale from 1 (not at all) to 5 (very much). In this study, Cronbach’s alpha for each of the four subscales ranged from .72 to .86, indicating the acceptable internal consistency of this scale.
Conners K-CPT
The K-CPT is a commercially available computerized lab task that measures attentional performance in 4- to 6-year-old preschoolers with excellent reliability and validity (Conners, 2006). The stimuli used in the K-CPT are familiar to young children and include a football, a horse, a house, scissors, and a sailboat. The child participant was asked to press the spacebar each time a picture appears unless the picture is of a football. The pictures are presented in five blocks, and there were 200 trials that were presented in 7.5 min. Attentional performance on the task is scored as follows: (a) omission errors: the number of trials on which the child did not respond to a non-football stimulus, (b) commission errors: the number of trials on which the child incorrectly responded to the football stimulus, (c) Hit RT: the overall mean hit reaction time recorded in milliseconds (ms) for correct responses, and (d) Hit RTSD, the within-child variability of hit RT.
Color Flanker Task
The Color Flanker Task is a modified computerized version of the Flanker task (Lindqvist & Thorell, 2009). Children are presented with two conditions (congruent/incongruent) in this task. On congruent trials, the target red/blue circle is flanked by four red/blue balls (two on either side) of the same color as the target circle. On incongruent trials, the target red/blue circle is flanked by four blue/red balls (two on either side) of a different color to the target circle. In all conditions, children are asked to press the colored button (red/blue) that corresponds to the color of the central target circle. On each trial, a fixation cross appears in the center of the screen for 500 ms and is then replaced by the stimulus (congruent or incongruent). The participant must then press the response button to register the color of the middle circle. A happy face (500 ms) is displayed after a correct response and a sad face (500 ms) after an incorrect response. If no response is registered after 3,000 ms, the trial automatically terminates, a sad face is shown, and then the next trial starts. The task contains three blocks, with 24 trials in each block: six trials for each condition (blue/red balls and congruent/incongruent conditions), presented randomly. We used the number of errors, the reaction time (RT) for correct responses, and the standard deviation of the reaction time (RTSD) for correct response in the congruent/ incongruent conditions as dependent measures.
Procedure
The Chang Gung Medical Foundation Institutional Review Board of CGMH (ID: 102-4775B) and the Research Ethics Committee of NTUH (IRB ID: 201405086RINB) approved this study before implementation. The study was registered at ClinicalTrials.gov (NCT02433145). Written informed consent and child assent were obtained from the parents after a detailed explanation of the purpose and procedure of the study and reassurance concerning confidentiality and the voluntary nature of participation. All participants underwent the assessment, which included the Chinese WPPSI-IV short version (which estimates IQ through three subtests: information, matrix reasoning, and picture memory), followed by the K-CPT and the Color Flanker Task.
Statistical Analysis
Statistical analyses were conducted in SAS 9.4 (SAS Institute Inc., Cary, NC, USA). The four comparison groups were the PHA, SHA, HHA, and PLA groups. Detailed demographic results from the four groups are expressed as the frequency, percentage, and chi-square statistics for categorical variables, and as the mean, SD, and one-way analyses of variance for continuous variables. We compared the main effects of group (PHA, SHA, HHA, and PLA) with multiple analyses of variance (MANOVA) using the GLM procedure in SAS. The nuisance covariates included gender. The LSD procedure was used in post hoc analyses among the four groups. We also computed effect sizes (Cohen’s d) for the group comparisons for task performance (K-CPT and the Color Flanker Task), internalizing/externalizing behavioral problems (CBCL/1.5–5 and C-TRF), parental stress (PSI-SF), and parenting perceptions (Cohen, 1988).
Results
Sample Description
The four main groups (PHA, SHA, HHA, and PLA ) differed significantly with respect to gender but did not differ with respect to age, estimated FSIQ, parental age, parental education, teachers’ age, or teachers’ education level (Table 1).
Participant Characteristics.

Note. FSIQ = Full-Scale IQ; SD = standard deviation.
p < .01.
Internal/External Scores on the CBCL/1.5-5 and C-TRF
MANOVA analyses across the internal/external behavioral problems in CBCL/1.5 and C-TRF yielded statistically significant difference among the four groups (F[6, 408] = 15.48, Wilks’ Lambda = .66, p < .001; F[6, 408] = 29.40, Wilks’ Lambda = .48, p < .001). Table 2 shows the subsequent univariate ANOVA analyses, revealing significant group effects for internalizing behavioral problems assessed by the CBCL/1.5-5 and C-TRF (F[3, 205] = 9.49, p < .001; F[3, 205] = 33.16, p < .001), and externalizing behav-ioral problems assessed by the CBCL/1.5-5 and C-TRF (F[3, 205] = 29.56, p < .001; F[3, 205] = 67.23, p < .001).
The Comparisons Between ADHD Symptoms and Internalizing/Externalizing Behavioral Symptoms Among Four Groups.
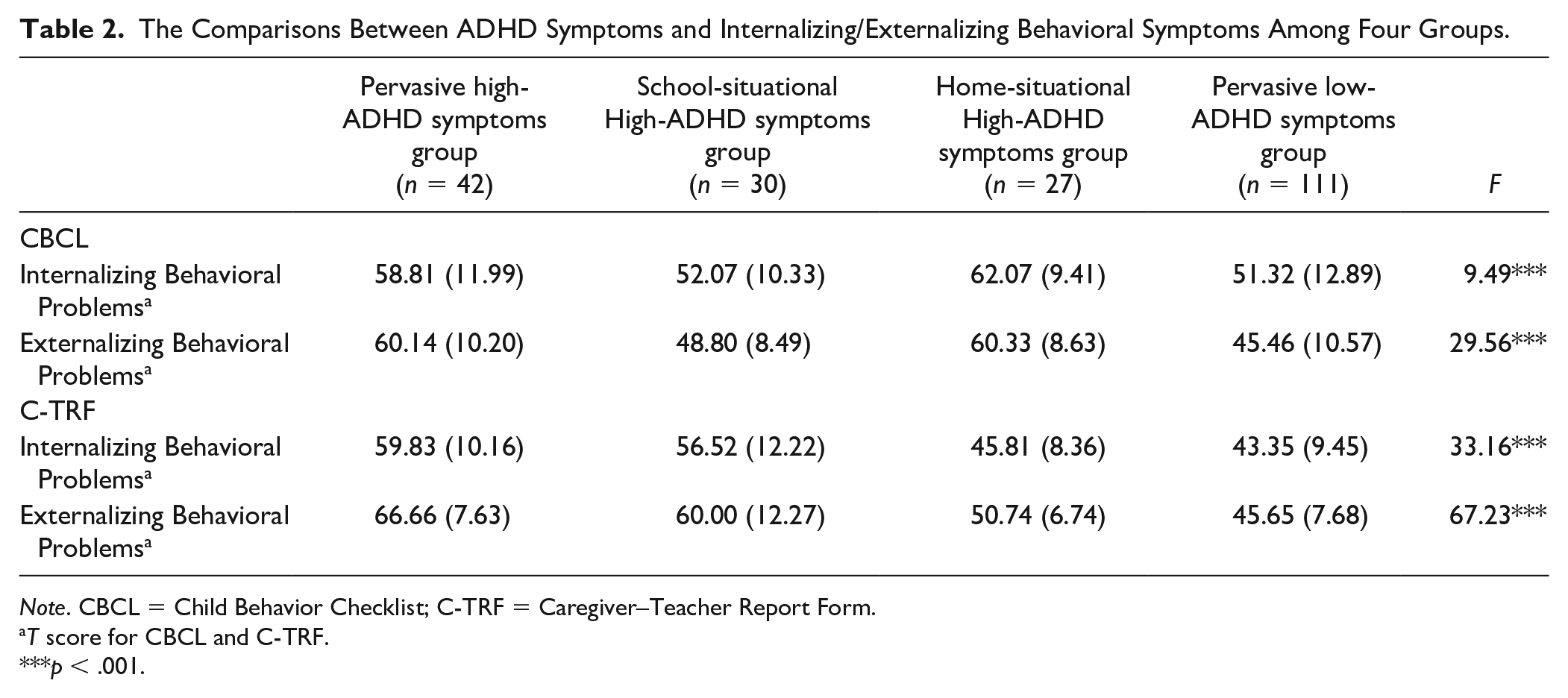
Note. CBCL = Child Behavior Checklist; C-TRF = Caregiver–Teacher Report Form.
T score for CBCL and C-TRF.
p < .001.
The PHA and HHA groups had higher parent-reported (CBCL/1.5–5) scores for internalizing/externalizing behavioral problems than the SHA (internal: p = .015, Cohen’s d = .60; p = .002, Cohen’s d = 1.01; external: p = .001, Cohen’s d = 1.21; p < .001, Cohen’s d = 1.35) and the PLA (internalizing: p = .001, Cohen’s d = .60; p < .001, Cohen’s d =.95; externalizing: p < .001, Cohen’s d = 1.41; p < .001, Cohen’s d = 1.54) groups. Meanwhile, the PLA and SHA groups had higher teacher-reported (C-TRF) scores for internalizing behavioral problems than the HHA (p = .001, Cohen’s d = 1.51; p = .001, Cohen’s d =1.02) and PLA (internalizing: p = .001, Cohen’s d = 1.68; p = .001, Cohen’s d = 1.21) groups. For the teacher-reported externalizing behavioral problems, the PHA group had higher scores than the SHA (p = .002, Cohen’s d = .65), HHA (p = .001, Cohen’s d = 2.21) and PLA (p = .001, Cohen’s d = 2.95) groups; the SHA group had higher externalizing scores than the HHA (p = .001, Cohen’s d = 0.95) and PLA (p = .001, Cohen’s d = 1.53) groups; and the HHA group had higher externalizing scores than the PLA group (p = .005, Cohen’s d = .70; Figure 1).

(a) T scores for internalizing behavioral problems in CBCL for the four groups (PHA, SHA, HHA, and PLA), (b) T scores for externalizing behavioral problems in CBCL for the four groups (PHA, SHA, HHA, and PLA), (c) T scores for internalizing behavioral problems in C-TRF for the four groups (PHA, SHA, HHA, and PLA), and (d) T scores for externalizing behavioral problems in C-TRF for the four groups (PHA, SHA, HHA, and PLA).
Group Comparisons for the K-CPT and Color Flanker Task
K-CPT
A MANOVA across the performance index (commission errors, omission errors, RT, and RTSD) in the K-CPT yielded a statistically significant difference among the four groups (F[12, 534] = 3.38, Wilks’ Lambda = .82, p < .001). Table 3 shows the subsequent univariate ANOVA, showing significant group effects for the number of commission errors (F[3, 205] = 2.93, p = .035), the number of omission errors (F[3, 205] = 5.62, p = .001), and the RTSD (F[3, 205] = 9.35, p < .001). Post hoc comparisons showed that the PHA and SHA groups had more commission errors (p = .024, Cohen’s d = .63; p = .015, Cohen’s d = .60; Figure 2a) and omission errors (p = .005, Cohen’s d = .64; p = .004, Cohen’s d = .65; Figure 2b) than the PLA group; the HHA group had more omission errors than the PLA group (p = .031, Cohen’s d = .52). The PHA and SHA groups also had heightened RTSD compared with the HHA (p = .001, Cohen’s d = .83; p = .010, Cohen’s d = .70) and PLA (p < .001, Cohen’s d = 0.77; p = .001, Cohen’s d = 0.79) groups (Figure 2c).
The Comparisons of the Performance at K-CPT and Color Flanker Task Among Four Groups.
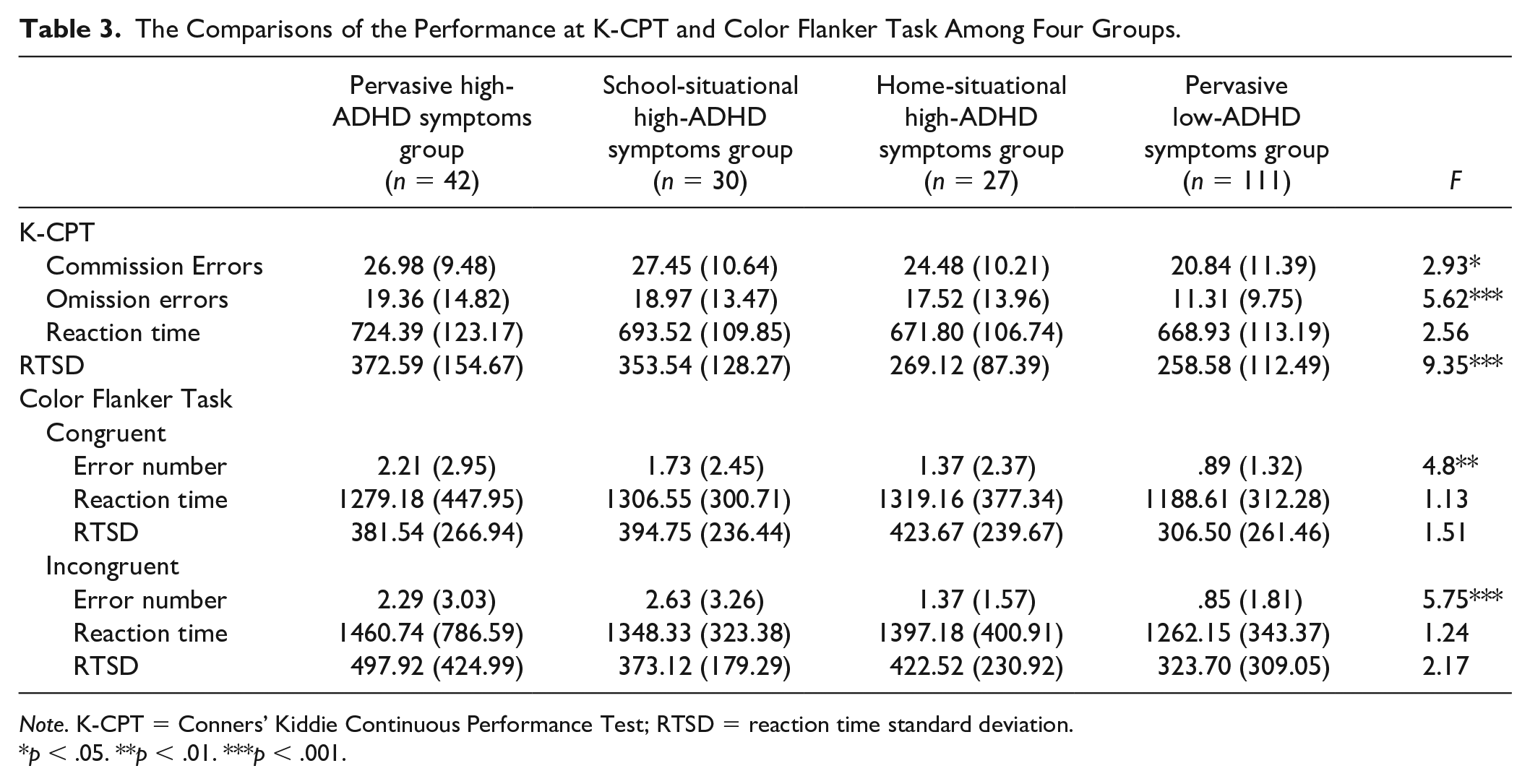
Note. K-CPT = Conners’ Kiddie Continuous Performance Test; RTSD = reaction time standard deviation.
p < .05. **p < .01. ***p < .001.
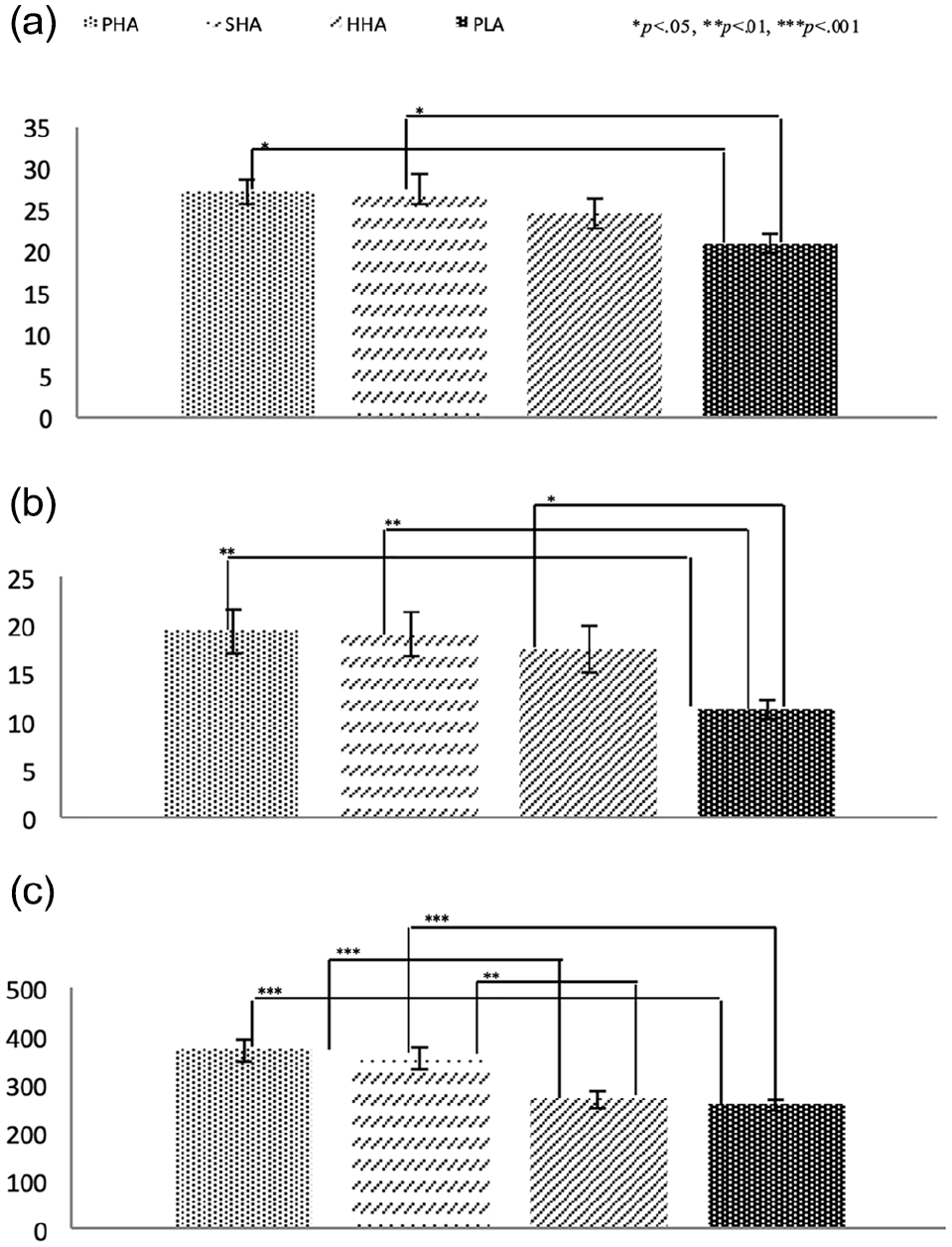
(a) The number of commission errors for the four groups (PHA, SHA, HHA, and PLA), (b) the numbers of omission errors for the four groups (PHA, SHA, HHA, and PLA), and (c) reaction time standard deviation (RTSD) for the four groups (PHA, SHA, HHA, and PLA).
Flanker task
A MANOVA across the performance index (error number, RT, and RTSD) yielded a statistically significant difference among the four groups for the congruent (F[9, 494] = 2.07, Wilks’ Lambda = .91, p = .031) and incongruent (F[9, 494] = 2.67, Wilks’ Lambda = .89, p = .005) trials. Table 3 shows that there were significant group effects for the number of response errors in both the congruent condition (F[3, 205] = 4.80, p = .003) and the incongruent condition (F[3, 205] = 5.75, p = .001). Post hoc comparisons showed that the PHA and SHA groups had more response errors than the PLA group in both the congruent condition (p = .001, Cohen’s d = .58; p = .040, Cohen’s d = .43; Figure 3a) and the incongruent condition (p = .003, Cohen’s d = .58; p = .001, Cohen’s d = .68; Figure 3b).
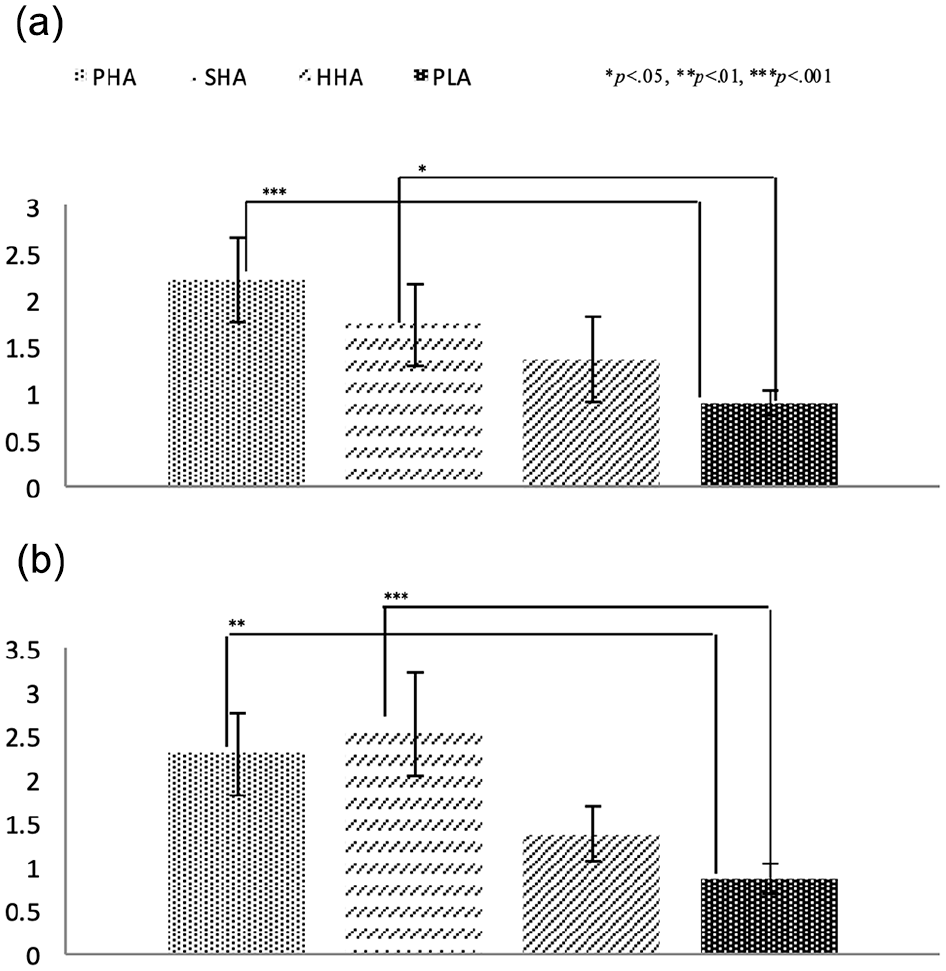
(a) The error number in congruent for the four groups (PHA, SHA, HHA, and PLA) and (b) the error number in incongruent for the four groups (PHA, SHA, HHA, and PLA).
Group Comparisons for the PSI/SF and Parenting Perceptions
A MANOVA across the PSI/SF and parenting perceptions subscale yielded a statistically significant difference among the four groups (F[15, 555] = 4.07, Wilks’ Lambda = .75, p < .001). Table 4 shows the results of the subsequent univariate ANOVA, revealing that there were significant group effects for the total parental distress score (F[3, 205] = 12.83, p < .001) as well as for the accepting (F[3, 205] = 3.75, p = .012) and punishing (F[3, 205] = 9.94, p < .001) parenting perceptions. Post hoc comparisons showed that the parents of preschoolers in the PHA and HHA groups reported more parental stress than parents of preschoolers in the SHA (p = .003, Cohen’s d = .68; p < .001, Cohen’s d = .97) and PLA (p < .001, Cohen’s d = .91; p < .001, Cohen’s d = 1.25) groups (Figure 4a). Meanwhile, the parents of preschoolers in the SHA and PLA groups reported higher scores on the accepting component of parenting perceptions subscale than the parents of preschoolers in the PHA (p = .048, Cohen’s d = .45; p = .019, Cohen’s d = .63) and HHA (p = .024, Cohen’s d = .68; p = .010, Cohen’s d = .63) groups (Figure 4b). Consistent with this, the parents of preschoolers in the PHA and HHA groups reported higher scores on the punishing component of the parenting perceptions subscale than the parents of preschoolers in the SHA (p < .001, Cohen’s d = 1.01; p < .001, Cohen’s d = 1.06) and PLA (p = .001, Cohen’s d = .65; p < .001, Cohen’s d = .70) groups (Figure 4c).
The Comparisons Between the Parental Stress and Parenting Perceptions Among Four Groups.
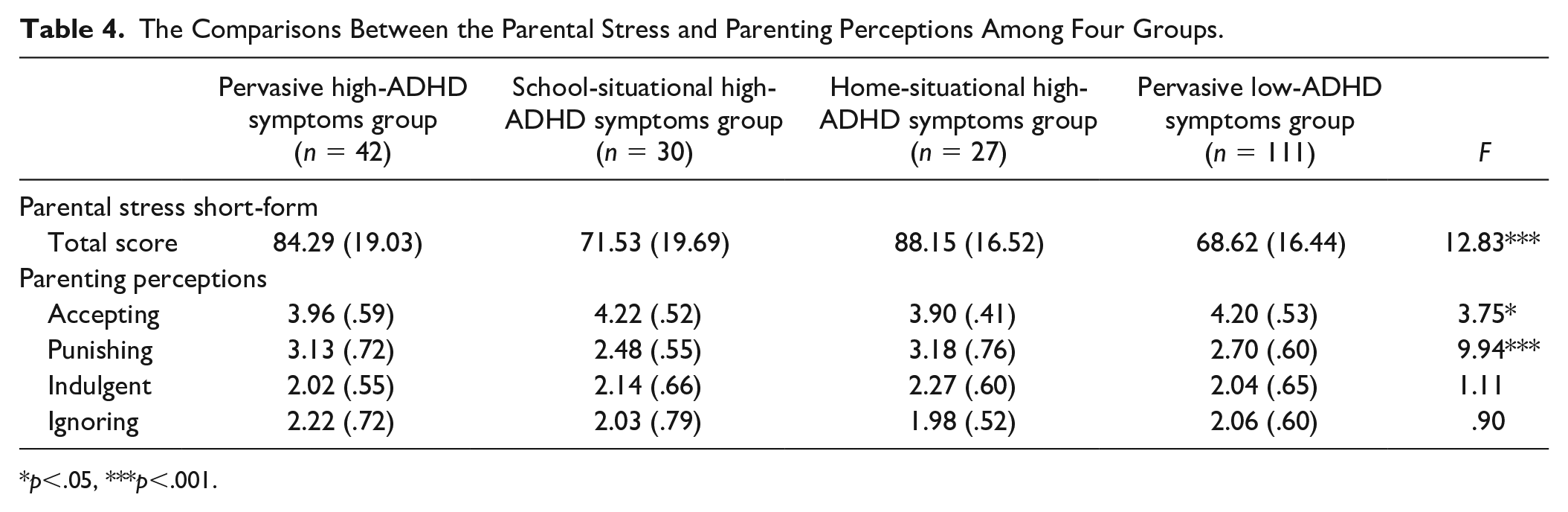
p<.05, ***p<.001.
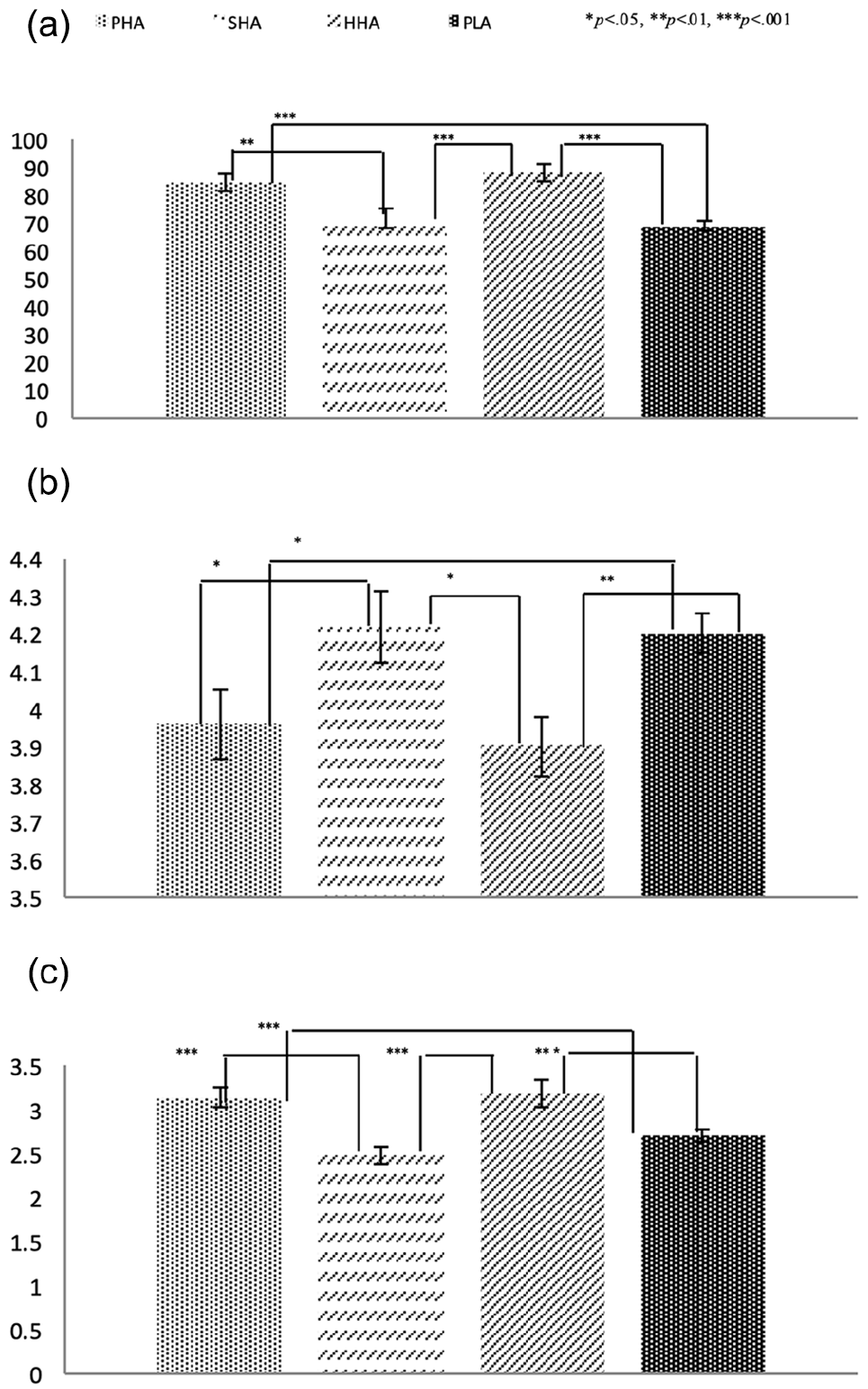
(a) Scores on the parental stress–short form for the four groups (PHA, SHA, HHA, and PLA), (b) accepting in parenting perceptions for the four groups (PHA, SHA, HHA, and PLA), (c) punishing in parenting perceptions for the four groups (PHA, SHA, HHA, and PLA).
Discussion
The current study is the first to investigate the contextual risk factors related to cross-situational variability in ADHD symptoms in preschoolers, as reported by parents and teachers. In line with previous studies (Cho et al., 2011; Jacobson et al., 2018), the results lend evidence to support our first hypothesis that preschoolers with SHA have heightened internalizing and externalizing behavior problems reported by teachers, as well as poor performance on laboratory attentional and inhibitory control tasks. Conversely, preschoolers with HHA have heightened internalizing and externalizing behavior problems reported by parents, as well as poor parent–child relationships, a higher level of parental stress, and greater exposure to perceived negative parenting. Our second hypothesis is supported by the above-mentioned results. Lastly, as predicted, preschoolers with PHA had heightened parent-reported and teacher-reported internalizing and externalizing behavior problems, as well as impairments in attentional and inhibitory control; parents of these children also reported higher levels of parental stress and perceived their parenting to be harsher than parents of TD children. These results are useful for identifying the essential contextual risk factors associated with the different ADHD informants at home and school.
Several studies have shown that situational ADHD may, in fact, be subthreshold ADHD (Kobor et al., 2012; Rommelse et al., 2015). However, the current study shows that preschoolers with SHA and HHA appear to differ in the risk factors associated with their ADHD symptoms. In line with a previous study (Cho et al., 2011; Jacobson et al., 2018), we found that preschoolers with SHA, like those with PHA group, had significant impairments in attention and inhibitory control, as measured by the K-CPT and Color Flanker Task. The impairments in these neurocognitive functions may be associated with poor adaptation to school life, learning, and peer interactions, such that their teachers report severe ADHD symptoms and internalizing/ externalizing behavioral problems. Notably, the parents of preschoolers with SHA reported less parental distress than the parents of preschoolers with HHA or PHA, as well as perceiving their parenting to be more accepting and less harsh. These results indicate that preschoolers with SHA have a good relationship with their parents.
On the other hand, and in line with the results from a previous study (Ho et al., 1996), we found that preschoolers with HHA experienced more stressful family conditions, with their parents reporting higher levels of parental stress and harsher perceived parenting than parents of preschoolers in the SHA, and PLA groups. Preschoolers with HHA also had poor attentional control, with more omission errors than preschoolers in the PLA group; however, they appeared adapted to school life, with no heightened teacher-reported externalizing or internalizing behavioral problems (Ho et al., 1996). These results suggest that preschoolers with HHA may share the poor neurocognitive function seen in preschoolers with SHA. The results we observed for the HHA group may also be due to a bidirectional, transactional, and tense parent–child relationship (Lifford et al., 2008), whereby parents feel that their child has behavioral problems (i.e., heightened ADHD symptoms and externalizing/internalizing behavioral problems) and respond with harsher and less accepting parenting, and experience more parental stress.
As predicted, the preschoolers with PHA had impairments in neurocognitive functioning and heightened internalizing/externalizing behavioral problems in school and at home, as reported by both teachers and parents. These results are consistent with those from previous studies showing that preschoolers with ADHD symptoms have deficits in attentional and inhibitory control (Hwang-Gu et al., 2019; Merkt et al., 2016; Schoemaker et al., 2014) and have more behavioral problems at home and school (Dirks et al., 2012). These findings validate the DSM-5 cross-situational criteria for ADHD diagnosis. Several studies have shown that preschoolers with ADHD symptoms perform worse in elementary school, and even during adolescence (Lee et al., 2008; O’Neill et al., 2017). Thus, it is important to assess this population and provide appropriate interventions in early childhood.
The current study shows that there may be different contextual risks (but not necessarily unique factors) associated with clinical ADHD symptoms in preschoolers with SHA and HHA. Consistent with previous studies, teacher-reported ADHD symptoms were related to objective measurements, such as tests of inhibitory control (Jacobson et al., 2018), language ability (Gooch et al., 2017), and academic performance (Ho et al., 1996). Mannuzza et al. (2002) showed in a 12-year follow-up study that children with pervasive ADHD and school-specific ADHD have a higher prevalence of antisocial disorder and greater difficulties with educational attainment and academic performance than children with home-specific ADHD. This suggests that children with school-specific ADHD may be at a higher risk of future problems than those with home-specific ADHD (Mannuzza et al., 2002). Parental reports of ADHD have also been found to be distorted by the level of parental distress (Chen et al., 2017), the presence of parental psychopathological problems, like depression (Dirks et al., 2012), and the level of family functioning (Rommelse et al., 2015). Hence, clinicians should be concerned with the severity of ADHD symptoms in different contexts: referred children may have different vulnerabilities, especially at preschool age.
Limitations
Although the present study has several strengths, interpretation of the results should remain conservative because of the following limitations. First, because we lacked a measure of the teachers’ stress, it is difficult to rule out a bidirectional relationship regarding teacher-reported evaluations (Lifford et al., 2008). Second, the current study did not measure parents’ psychopathology, so we do not know whether the characteristics of the parents affect their evaluation of ADHD symptoms. Previous studies have shown that parental depression is associated with psychopathology in children, especially ADHD (Dirks et al., 2012). Thus, this measure will be needed in future studies. Third, the study lacked a strict diagnosis interview by a psychiatrist and independent behavioral observations; hence, the clinical implications should be interpreted with caution.
Clinical Implications
The lack of parent-teacher agreement about ADHD symptoms may be a major contributor to situational ADHD (Rommelse et al., 2015). Even with structured diagnosis interviews, parental reports of ADHD symptoms in school were only moderately correlated (r = 0.3–0.39) with teacher reports for the same behavioral problems (Mitsis et al., 2000). Hartman et al. (2007) suggested that the lack of agreement between parent-reported and teacher-reported ADHD ratings is related to the raters observing different ADHD behaviors in different contexts (i.e., home vs school). Each informant reported based on his/her evaluation criteria of specific experience (Dirks et al., 2012). Hence, clinicians should not rely on information from a single informant to make a diagnosis of ADHD (Dirks et al., 2012). Clinician observations in multiple situations are needed to clarify issues surrounding situational ADHD (Rommelse et al., 2015). It is further suggested that ADHD referrals should include a comprehensive clinical assessment not just of the child, but also of their family function, including the parenting style, parental stress, and even the psychopathology of the parents. With such comprehensive information, the risk factors for ADHD symptoms could be identified.
Footnotes
Acknowledgements
The authors would like to express our thanks to all the participants and their parents and our research assistants for their contribution to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Ministry of Science and Technology (MOST 103-2410-H-182-003-MY3), and Chang Gung University (NMRPD1D0131, NMRPD1D0132, NMRPD1D0133), Taiwan. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Compliance with Ethical Standards
This study was approved by the Research Ethics Committee of the National Taiwan University Hospital and by the Chang Gung Medical Foundation Institutional Review Board. Parents’ written informed consent and child assent were obtained before study implementation. All procedures involving human participants were in accordance with the ethical standards of the institutional and national research committees, the 1964 Helsinki Declaration and its later amendments, or comparable ethical standards.