
Abstract
Objective:
This randomized controlled study explored the efficacy, feasibility, and acceptability of executive function training (EFT) for preschool children with ADHD.
Method:
The current study design was an 8 week randomized parallel groups, single-blinded trial, using EFT-P. A total of 96 children with an ADHD diagnosis at age 4 to 5 years old were randomized into the intervention group and waitlist group. In the intervention group, 46 out of 50 participants completed the 8-week program, compared with 39 out of 46 in the waiting group. The level of ADHD symptoms and the executive function (EF) were evaluated by both neuropsychological tests from NEPSY Second Edition (NEPSY-II) and Behavior Rating Inventory of Executive Function Preschool version (BRIEF-P).
Results:
The EFT is feasible to administer and is acceptable for preschool children, with a 93% retention rate. Results showed that following the intervention, the visual-motor precision (p = .024), ADHD diagnostic state (p = .01), and oppositional defiant symptoms (p = .023) improved significantly in preschool children. However, the symptoms of ADHD and other EF evaluations were found to be insignificant.
Conclusion:
The EFT is feasible, acceptable, and potentially effective to reduce symptoms and improve EF for preschool children with ADHD. The next step is to extend the program time and provide more frequent practice of activities between the children and the therapist and/or parent, to improve the effectiveness.
Introduction
ADHD is one of the common childhood neurodevelopmental disorders that occurs in preschool children, with the prevalence ranging from 2% to 6% (Angold et al., 2000). ADHD in preschoolers is a relatively stable condition characterized by chronic and severe impairment in terms of interpersonal relationships, behaviors in public, pre-academic skills, and executive function (EF) (Murray, 2010; Riddle et al., 2013). It is well-documented that ADHD is closely associated with EF deficits, and many researchers propose that ADHD is most appropriately characterized as an EF disorder (Sonuga-Barke et al., 2002).
EF is defined as self-directed actions that include creating, enacting, and sustaining actions in order to choose and achieve goals (Barkley, 2012). Deficits in EF co-occur with emotional dysregulation and cognitive impairments as part of ADHD (Ezpeleta & Granero, 2015). EF deficits can be observed in preschoolers using both direct performance-based measures and reports of children’s performance by parents (Zhang et al., 2018). Moreover, the preschool EF deficits associated with ADHD continues into school age (Shuai et al., 2011; Willcutt et al., 2005), adolescence (Martel et al., 2007), and adulthood (Biederman et al., 2006). Therefore, it is critical for interventions to target EF in early childhood in order to prevent developmental progression of EF deficits, which can later cause extensive and severe functional impairments (Tamm & Nakonezny, 2015).
These impairments associated with ADHD in the preschool years underscores the importance of early diagnosis and appropriate interventions to improve developmental trajectories (Posner et al., 2007). The use of psychostimulants remains a controversial option for preschool ADHD treatment studies (PATS) due to the lack of efficacy and commonly occurring side effects (Kollins et al., 2006). Therefore, early interventions mainly focus on nonpharmacological parent training programs (Sonuga-Barke et al., 2011), such as the Parent-Child Interaction Therapy (PCIT) (Bjørseth & Wichstrøm, 2016), the Incredible Years (IY) (Trillingsgaard et al., 2014), the Triple P—Positive Parenting Program (Bor et al., 2002), and the New Forest Parenting Programme (NFPP), which generally targets cognitive deficits (Sonuga-Barke et al., 2006). In fact, the earlier the intervention the more likely it is to reverse the pathogenic process with ADHD (Sonuga-Barke & Halperin, 2010). However, based on the EF deficits of ADHD, there is an emerging need for interventions that attempt to target these core deficits. There are different training programs for preschoolers with ADHD, such as the metacognitive executive function training (Tamm & Nakonezny, 2015), and the training, executive, attention, and motor skills (TEAMS) intervention (Halperin et al., 2013). To date, few interventions have been tested using a randomized controlled study (RCT) designs. These interventions are still in the early stages of development, are in need of further development such as using an intervention in combination with other treatments in order to provide more encouraging results (Halperin & Marks, 2019). EF can then be improved in early childhood through mental “exercise” similar to psychical exercise, which builds muscle (Diamond & Lee, 2011). Improving EF in early childhood may reduce the need for costly specialized education, may reduce social burden caused by antisocial behavior, and may reduce the risk of EF related problems like ADHD and Conduct Disorder (CD) (Diamond et al., 2007).
The current study was an RCT designed to evaluate the effects of Executive Function Training for Preschool (EFT-P) children with ADHD. The effects of EFT-P were evaluated measuring aspects of symptoms and functions. These effects were assessed using neuropsychological tests and behavioral ratings. We hypothesized that compared with the control group, the intervention group would show improvements in EF deficits and ADHD symptoms.
Method
Participants
The study included 96 native Chinese speaking preschool children with DSM-V diagnosed ADHD, ranging from 4 years 0 months to 5 years 11 months. Children with major sensory-motor disorders, history of brain damage, epilepsy, diagnosis of autism spectrum disorder, intelligence quotient (IQ) score <80 (as assessed by the Wechsler Primary and Preschool Scale of Intelligence [WPPSI]), and under pharmacological or nonpharmacological treatment (e.g., neurofeedback, balance training, other behavioral therapy, etc.) were excluded. The study protocol was approved by the ethics committee of the Xinhua Hospital. Informed consent was obtained from all the children using informal assent to take part and their parents signed a consent form. Separate participant information sheets were provided to the parent and child, with the children receiving the information by reading them the form in a way that they could understand what would happen and using language that was age appropriate. A psychiatrist was available at all testing points in case the child became upset by any aspect of the study. Parent and child were both informed of any risks and that they could withdraw from the research at any point without any impact on continued or future treatment with the hospital. The study was registered on clinicaltrials.gov (register number: NCT03515135).
Procedure
The eligible participants were recruited from a medical psychological outpatient clinic of a general hospital in Shanghai, China, from June, 2017 to December, 2018. All the children were newly diagnosed using structured interviews, with their parents, following the criteria of the DSM-5 by Diagnostic Infant Preschool Assessment (DIPA) (Scheeringa & Haslett, 2010). DIPA was developed and updated according to the DSM-5 in 2014. It is intended as an interview for caregivers of 6 years and younger, with the minimum age ranging below 1 year of age. The instrument is semi-structured but also contains some structured categories, including ADHD and the other psychiatric disorders. The ADHD category includes all 18 symptoms of the DSM-5 criteria for ADHD. Parents described the emergence, frequency, and severity of ADHD symptoms in two or more settings for the previous 6 months. The interviewer then rates these descriptions. The DIPA has been demonstrated to be a reliable and valid measure in research and clinical work with young children. To ensure diagnostic accuracy, the parents of the children were interviewed by two independent psychiatrists, with at least one of the psychiatrists being a senior psychiatrist.
The parents were provided the information on EFT-P and trained in the delivery of the intervention. There were 96 parents who agreed to participate in the study. Participants were randomized to either the intervention group (n = 50) or waitlist group (n = 46) that received treatment as usual (TAU) by using a random envelope method. The random envelopes were managed and revealed by researchers who were not directly involved in this study. TAU is mainly the psychoeducation of ADHD and general behavioral guidance provided by doctors in outpatient clinic appointments that lasted about 10 to 15 min per visit.
Figure 1 presents the flow diagram of the RCT. All outcomes were measured before and after the intervention for both groups. The waitlist group received the same intervention after the second assessment. The assessments were administered and scored by examiners blind to the diagnostic and treatment status of the participants. Four participants in the intervention group (two claimed having no time and another two had missed more than three sessions) and seven participants in the waitlist group (three claimed having no time, two were not willing to attend this study, and another two were unreachable) dropped out of the study.
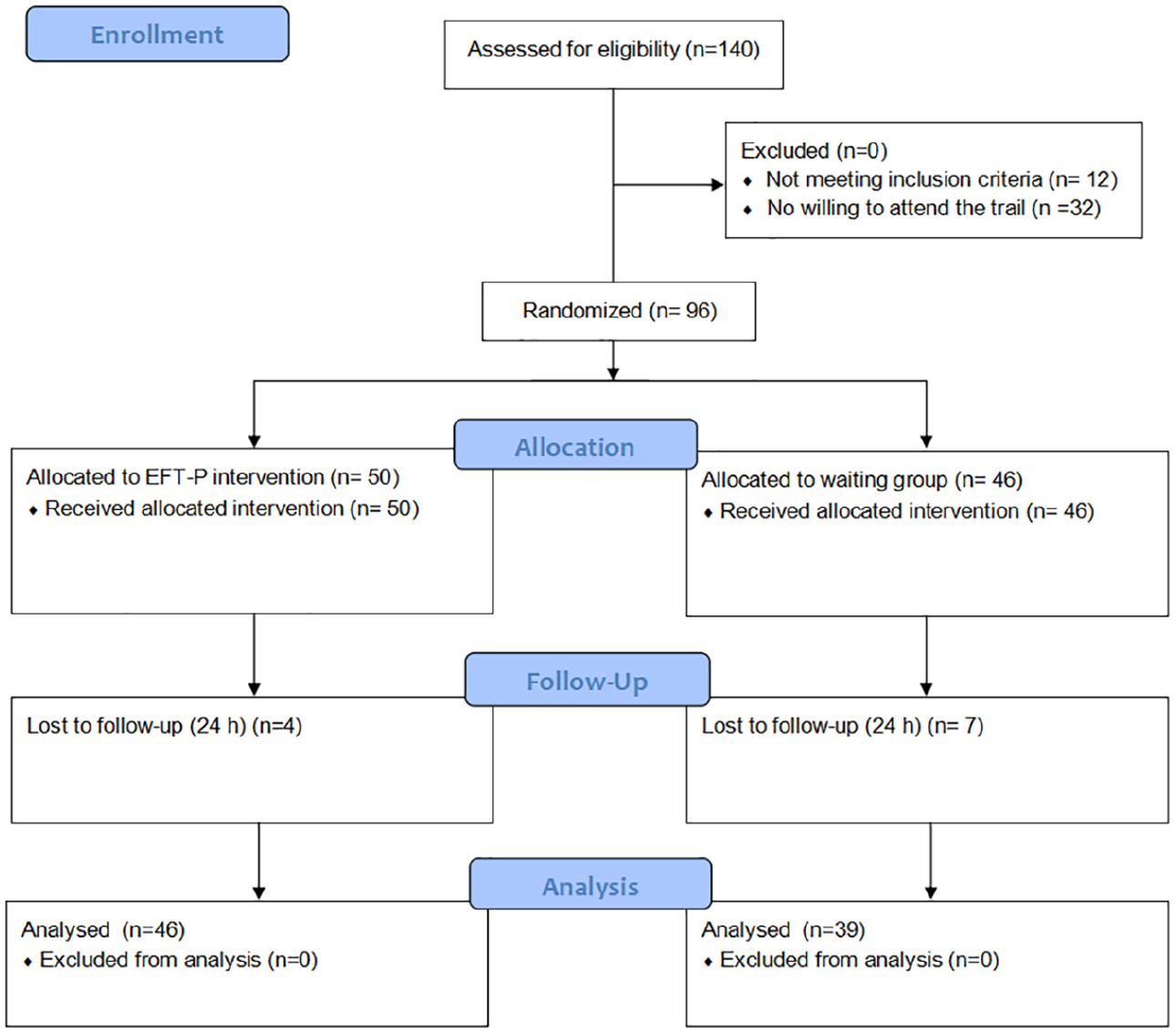
Trial flow diagram.
Measures
Swanson, Nolan, and Pelham Rating Scale (SNAP): Parents rated each ADHD and Oppositional Defiant Disorder (ODD) symptom on a 4-point Likert scale (0 = not at all, 1 = just a little, 2 = quite a bit, 3 = very much). A rating of a 2 or 3 was recorded as positive meaning the child met criteria for the symptom. The reliability and validity of the 26 item Chinese version of SNAP-IV form is satisfactory to use among preschooler in China (Zhang et al., 2016). Both the number of positive entries and raw scores of the ADHD and ODD symptom were calculated.
Strengths and difficulties questionnaire (SDQ) is a brief measure of the prosocial behavior and psychopathology of 3- to 16-year olds, which can be completed by parents (Goodman, 2001). The Chinese version of SDQ has 25 items and shows satisfactory reliability and validity (Kou et al., 2005). The score used to sum the child’s level of difficulties contained areas such as emotional symptoms, conduct problems, hyperactivity/inattention, and peer relationship problems. A higher raw score indicated greater levels of difficulties.
Behavior Rating Inventory of Executive Function Preschool version (BRIEF-P) is a rating scale for parents to assesses behaviors in daily life reflecting the EF in preschool children aged 2 to 5 years (Gioia et al., 2003). The instrument consists of 63 items on a 3-point ordered scale that measure 5 clinical dimensions of EF. There is a composite score called global executive composite (GEC), which indicates general executive performance. The higher the raw score, the higher the difficulty of the construct. The BRIEF-P has shown high concurrent and discriminant validity and adequate reliability in Chinese children (Lu et al., 2017).
Neuropsychological Measures: NEPSY-II is a comprehensive instrument designed to assess neuropsychological development (Korkman et al., 2007). It consists of a series of neuropsychological subtests from six domains of performance: attention and EF, memory and learning, social perception, language, sensorimotor skills, and visuospatial processing. In this study, nine age-appropriate subtests related to EF were used and raw scores were recorded, including Memory for Designs (MD), Narrative Memory (NM), Statue, Affect Recognition (AR), Theory of Mind (TM), Word Generation (WG), Comprehension of Instructions (CI), Block Construction (BC), and Visuomotor Precision (VP). These subtests have been found to be suitable for Chinese preschool children and effectively discriminate between ADHD and a health control (Zhang et al., 2018).
Intervention Method
EFT-P is a structured psychotherapy developed using the theory of EF and the results of our research review. The aim was to improve ADHD children’s EF through designed tasks and games, meanwhile providing support from parents. The participants attended a 90-min session (60-min for children, 30-min for parents) once a week for 8 weeks. The EFT-P was applied with four to five families in a clinical setting. The outline for each session is presented in Table 1. The intervention was designed using the following features:
Every session contained four parts for both children and parents: tasks and games aiming to practice EF (40 min), paper-pencil tasks (15 min), relaxation (5 min) for children, and parents also received a session on guiding their child (30 min).
Activities in EFT-P were fun for 4 to 5 year old children to ensure the young children’s cooperation. Some tasks required movements therefore the young children did not need to sit still for a long period of time. The activities were designed with increasing difficulty. Therefore the EF was continually challenged to gain improvement (Diamond & Lee, 2011). Each session focused on EF elements including inhibition, instruction comprehension, working memory, spatial perception, theory of mind, and visual fine motion, which were shown to be impaired in preschool children with ADHD (Zhang et al., 2018).
Paper-pencil tasks had two purposes, first to train visual fine motion found to be impaired significantly in a previous study. The other was to help a young child gain familiarity with writing skills. This is important in preparation for primary school because there are large amounts of written homework for Chinese students.
Relaxation was designed to calm down the young children at the end of session. It lasted 3 to 5 min. The strategies of deep breathing and muscle relaxation were taught in a simple and easy way suitable for preschoolers.
Guidance for parents addressed psychoeducation about ADHD and behavioral management skills mainly from NFPP (Thompson et al., 2017).
Therapists included psychiatrists and clinical psychologists, who possessed the skills of behavior therapy for children and had working experience with ADHD children. All the therapists had to comply with the EF training manual developed by the researchers. Weekly meetings were held to provide feedback and allow for group supervision.
Outline of Executive Function Training for Preschool Children With ADHD (EFT-P).

Note. EF = executive function.
Data Analysis
Statistical analyses of the data were performed using SPSS Version 19.0. The demographic differences between the two groups were assessed using paired sample t-test for continuous data and Chi-square test for categorical data. To compare intervention effects, a general linear model with repeated measures was performed, with time as the within-subject factor (before and after intervention), and group as the between-subject factor (intervention and TAU). Differences were compared using the SNAP, SDQ, BRIEF-P, and the children’s performances in the NEPSY subtests. The significance level was set at p < .05. Intention-to-treat (ITT) analyses with Last Observation Carried Forward (LOCF) was used to impute the dropped data. The sample size was estimated to be 90 (45 per group) and providing 80% power (Cohen’s d = 0.6) to detect moderate effect between two groups.
Results
The demographic and clinical characteristics of the intervention group and waitlist group are presented in Table 2. There was no significant difference of age (F = 0.07, p = .79) and IQ (F = 0.27, p = .60) between the two groups. At baseline, the ADHD subtypes, co-occurrence of ODD, scale results, and EF tests performances showed no significant differences between the intervention and waitlist groups (p > .05).
Demographic and Clinical Characteristics of the Study Sample.
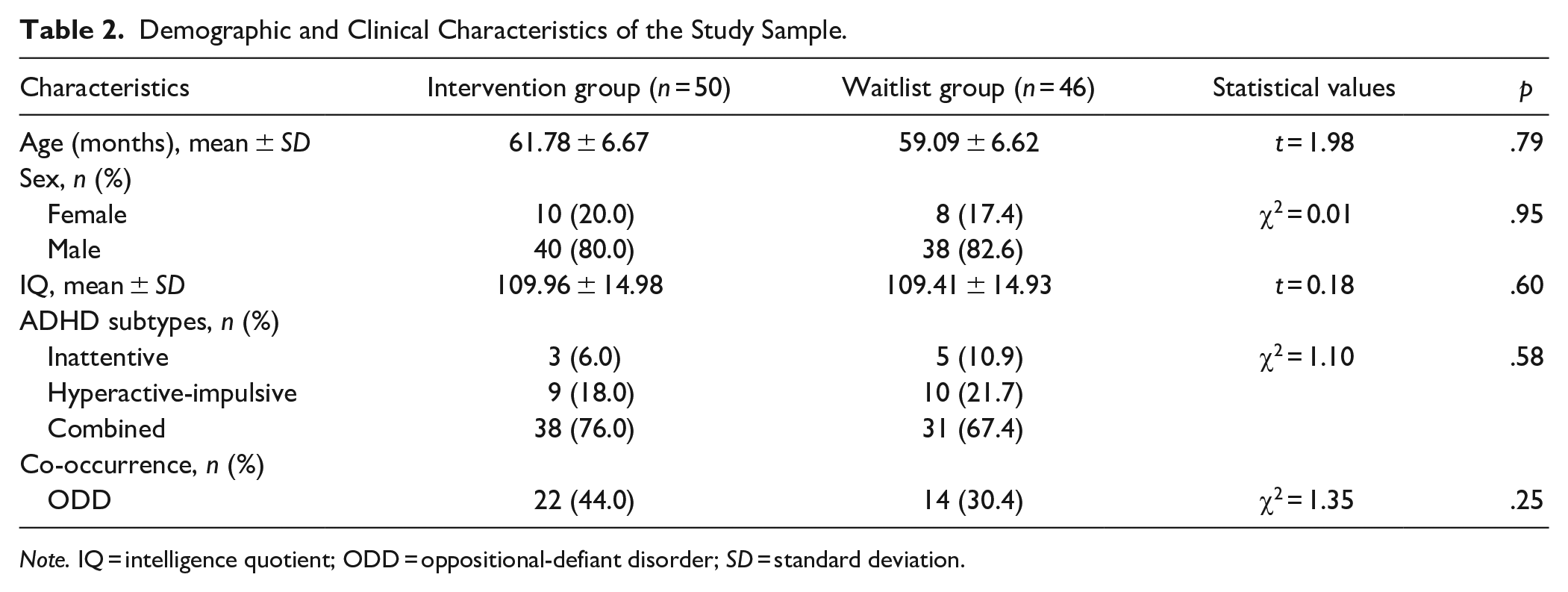
Note. IQ = intelligence quotient; ODD = oppositional-defiant disorder; SD = standard deviation.
The primary outcome was EF performance as presented in Table 3. The intervention group showed significantly less errors on the visuomotor precision test (F(1, 94) = 5.33, p = .02, η2 p = 0.05, 95% confidence intervals: −27.74, 10.33). The total score in MD, the free-cued recall in NM, the completion time in VP, and the performances on the ST, AR, TM, WG, CI, and BC did not show significant treatment effects.
Results of SNAP and NEPSY-II at Baseline and Post-Treatment.
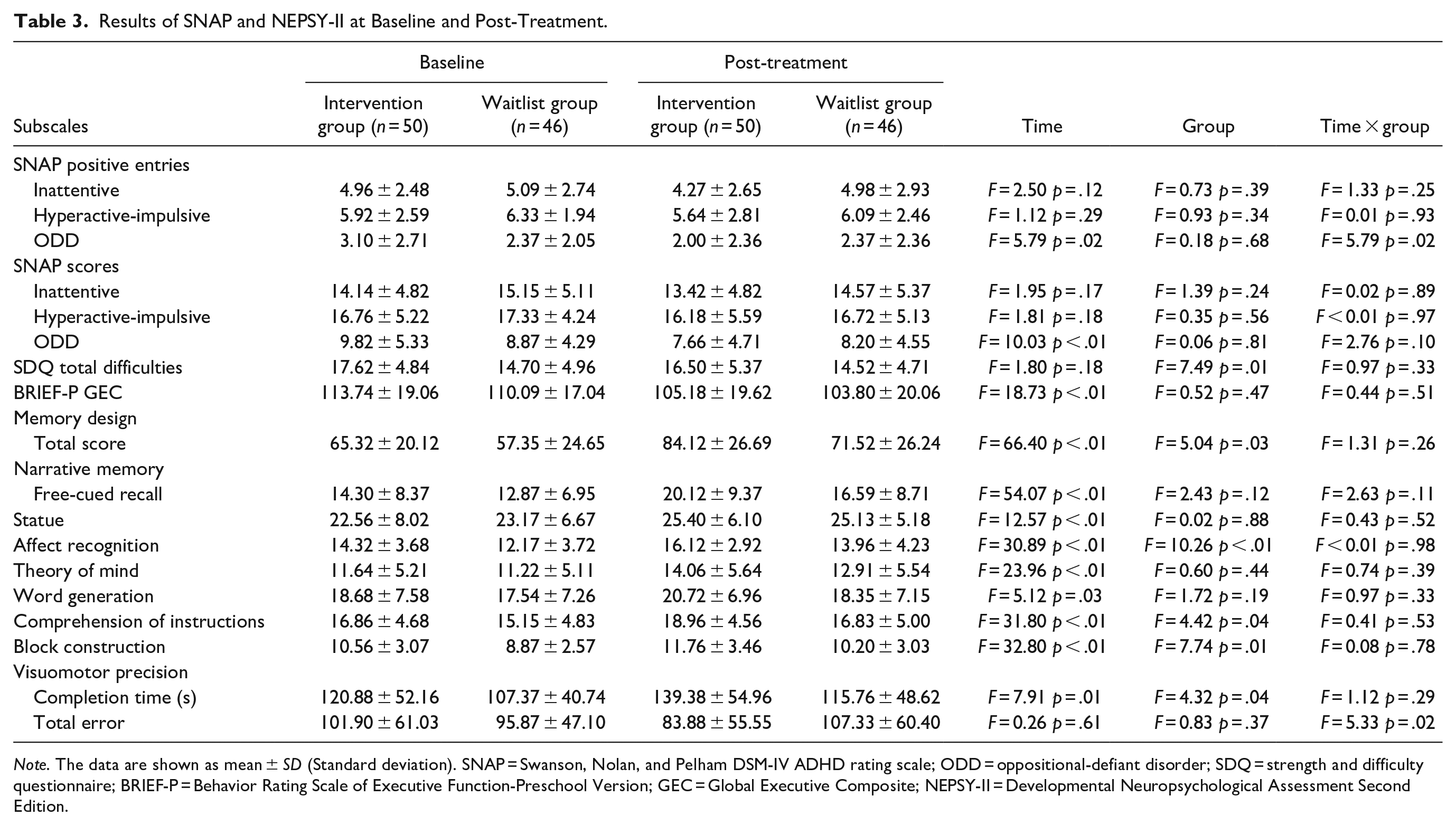
Note. The data are shown as mean ± SD (Standard deviation). SNAP = Swanson, Nolan, and Pelham DSM-IV ADHD rating scale; ODD = oppositional-defiant disorder; SDQ = strength and difficulty questionnaire; BRIEF-P = Behavior Rating Scale of Executive Function-Preschool Version; GEC = Global Executive Composite; NEPSY-II = Developmental Neuropsychological Assessment Second Edition.
The secondary outcome was the ADHD symptoms. Table 3 shows the results of the repeated measures ANOVA (2 × 2) of the parents’ rating of SNAP between baseline and posttreatment, comparing intervention and waitlist groups. Parents of the intervention group reported a significant reduction of ODD symptom than the waitlist group (F(1, 94) = 5.79, p = .02, η2 p = 0.06, 95% confidence intervals: −0.67, 1.04). The inattentive symptom did no show significant differences.
Change in ADHD diagnosis are presented in Table 4. All the participants in this study met ADHD criterion at baseline. After 8 weeks, two children in the intervention group no longer meet ADHD diagnostic criteria, while all children in the waitlist group did still meet ADHD diagnostic criteria. Ten children in the intervention group and only one child in the waitlist group changed to ADHD-NOS, meaning that ADHD symptoms (four or five items) failed to completely met the minimum number of criteria (six items). However, they still had significant functional impairment. The difference between the two groups was significant (χ2 = 9.80, p = .01). As for the comorbidity of ODD diagnostic status, there was no significant difference between two groups (χ2 = 0.32, p = .85).
Results of DIPA at Post-Treatment.
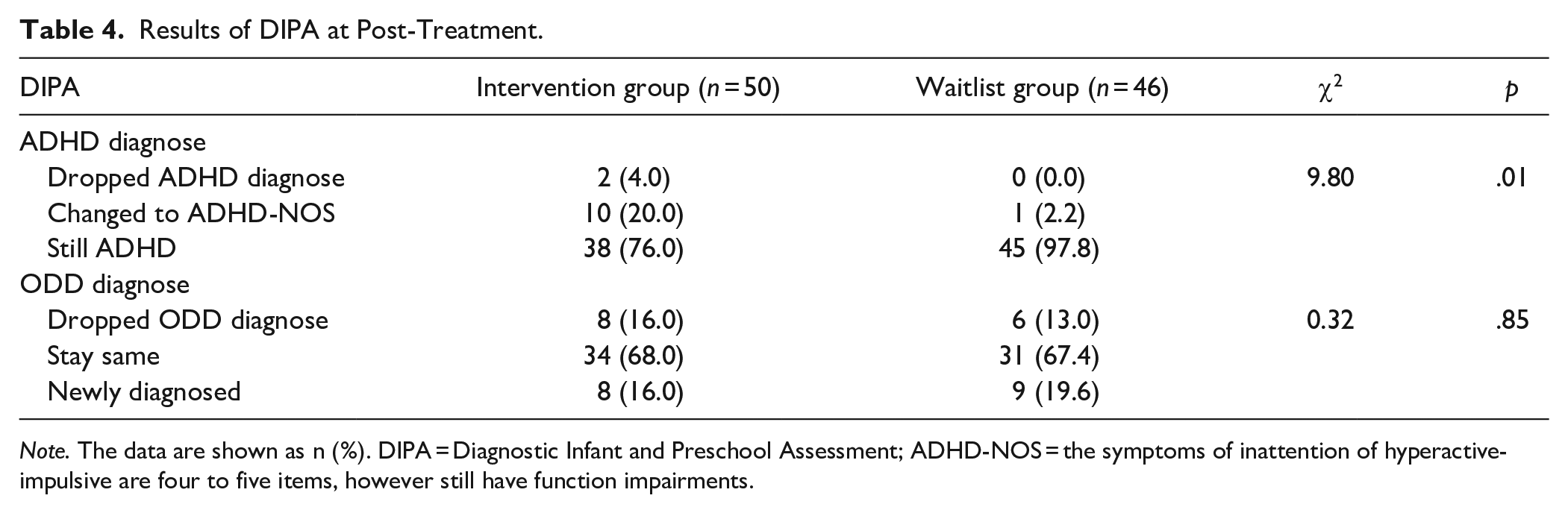
Note. The data are shown as n (%). DIPA = Diagnostic Infant and Preschool Assessment; ADHD-NOS = the symptoms of inattention of hyperactive-impulsive are four to five items, however still have function impairments.
The EF in the day-to-day life of preschool children was assessed by BRIEF-P. There were no significant differences on all the factors and the GEC of BRIEF-P. We also compared the SDQ results which showed no significant differences of the total level of difficulties.
We investigated the children’s acceptance for all participants. None of them found the program unacceptable, nine children (10%) had some minor difficulty understanding the program, 32 children (38%) felt good about the program, and 44 children (52%) liked the program very much. Considering parent’s satisfaction with EFT-P, all of them felt satisfied with EFT-P and would like to recommend it to other parents of young children with ADHD. We also carried an open evaluation of parent’s opinions of the program after EFT-P. The sample extracts are as follows: “Her attention and self-control is improving. When we go out to play, she could follow my order, not running away as before.” And “The teacher of his pre-school praised him for his concentration lately.” The treatment and evaluation were conducted on the weekend to avoid conflicting with pre-school, however, some parents still had time conflicts with their work. The dropout rate of this study is 11%, mostly due to time conflicts.
Discussion
The current study found that EFT-P improved the visual-motor precision, the ADHD diagnostic state and ODD symptoms, and resulting in high attendance and acceptance for preschool children with ADHD. The result indicated that EFT-P could be a strong candidate of nonpharmacological early intervention for ADHD.
EFT-P was developed as a novel nonpharmacological early intervention for kindergarten children with ADHD as considerable studies suggest that ADHD is related to severe and comprehensive EF impairments (Shuai et al., 2011) even at young age (Zhang et al., 2018), which leads to education failure or later adulthood career failure (Gathercole et al., 2004). Considering children’s performances in the neuropsychological evaluation of EF, most of the results showed insignificant differences between EFT-P and the waiting group after 8 weeks, except visuomotor precision. Other similar intervention studies rarely include neuropsychological evaluations. In a study using metacognitive EF training for young children with ADHD, including neurocognitive measures such as concept, matrix reasoning and visual attention, improvements failed to show significance as well (Tamm & Nakonezny, 2015).
In this study, the significant function improvement was visuomotor precision. The reason might be due to the exercises, which the parents practiced at home with pencil-paper tasks. These tasks were used to train the visuomotor precision. Poor motor coordination and fine motor skills is a common coexisting problem in children with ADHD, which makes the tasks requiring fine visuomotor skills difficult, such as writing improvement (Mokobane et al., 2019). Previous studies have showed that the visuomotor function is associated with ADHD symptoms in early childhood (Peyre et al., 2019), therefore, any intervention for ADHD should include the training of fine motor skills (Fenollar-Cortés et al., 2017). The improvement observed in the visuomotor precision is meaningful for treating ADHD. Future interventions should focus on improving other EF components as well as visuomotor precision using a variety of interactive tasks. This finding is similar to previous research, for example a 12 week interactive yoga exercise for preschool children with ADHD found that both the visuomotor precision and ADHD symptoms showed improvement (Jarraya et al., 2019). Furthermore, a recent meta-analysis of cognitive training indicated that non-computerized training activities, such as playing cards, doing body exercises, and pencil activities might be effective for improving EF in preschoolers (Scionti et al., 2020). This study adopted non-computerized tasks and delivered the program in group format which likely led to the improvement of functioning.
The same meta-analysis also demonstrated that the duration of training sessions, rather than number of sessions, was an important factor for significant improvement in function, which suggests a need for longer exercises (Scionti et al., 2020). The results of this study suggest as long as the tasks and games are suitable for young children with ADHD that improvements in functioning would occur quicker, particularly if training were implemented not only in clinical setting, but also in the family setting to guarantee the training duration and intensity. Another preschool intervention study which focused on 356 case of young children with EF deficits delivered for one academic year, and followed for 5 years, further found improvements in function over a longer period of exercises (Sasser et al., 2017). Therefore, we speculate the contents and delivery format of EFT-P was suitable for preschoolers with ADHD, however, the lack of significant improvements of EF in this study might due to the short training time. The results suggest that there should be solid efficacy on the children’s functioning if the training “dose” is strong enough overtime. Future studies with extended program time and frequent practices between children and therapist and/or parent are required to confirm this.
This study had additional noticeable strengths. The examiners of the outcome evaluations were blinded to treatment allocations. The measures were relatively comprehensive including behavior symptoms reported by parents, the diagnostic interviews by clinicians, the neuropsychological performances of the children, and the attendance of the participants in the intervention group was as high as 93%. The high attendance also indicated that young children with ADHD not only could cooperate by completing the activities in this study, but also for the most part enjoyed the program. Moreover, the consumer satisfaction survey revealed that 89.4% preschool children accepted the EFT-P program. Surprisingly 100% of parents felt satisfied with the treatment. We assume the reason might not be due to the efficacy, but due to there being no alternative intervention for preschool children with ADHD in China. In addition, relationship between parents and children were enhanced in this intervention. Parents were coached on how to make play fun and interact warmly with their children. As the parents felt very satisfied about this program this could have provided a tolerant environment in which they could accept the children’s ADHD symptoms and provide appropriate activities for them.
Without interventions for comparison in China, the results were compared to the interventions previously mentioned in the introduction. Parent ratings of ODD symptoms showed a significant decline following treatment. In the meanwhile, compared with the TAU, more children in EFT-P group become ADHD-NOS from the ADHD diagnose (as interviewed by DIPA). These results indicated that EFT-P showed effective impacts on young children’s problematic symptoms of ADHD and ODD. This supports the previous parent-focused interventions implemented in preschool children with ADHD, such as The Incredible Years (Trillingsgaard et al., 2014), Triple P (Bor et al., 2002), and New Forest Parenting Programme (Thompson et al., 2017), which have been conducted outside of China. Given empirical evidence showing that parental management training has a positive effect on challenging behaviors in children, the clinical improvements may be attributed to parental engagement and involvement in the intervention rather than the EF enhancement per se. Significant reductions in ADHD symptoms could be found following parent training, especially when the program focused on underlying impairments in self-regulation as well as the quality of mother-child interactions (Sonuga-Barke et al., 2011).
The most similar findings to this intervention are the training, executive, attention, and motor skills (TEAMS) intervention, which focuses on preschool children with ADHD. The open trial of TEAMS shows a significant decline of ADHD symptoms and impairment (Halperin et al., 2013). However, the improvements of TEAMS dropped to non-significant in a RCT when compared with the standard treatment (Vibholm et al., 2018). Vibholm et al. suggests that the high dropout in the standard treatment might be the reason the RCT was insignificant, and that those parents had wanted their children to initiate medication rather than participate in the TEAMS (Vibholm et al., 2018). In our study, both parents in EFT-P and the waiting group were strongly resistant to medication, therefore, the dropout was lower and the improvements were significant in the RCT.
EFT-P is a program delivered in a clinical setting by highly trained personnel and requiring a time commitment and need for travel from the families, which might have also acted as barriers for participation in the intervention when compared with telepsychiatry or online therapy. However, the intervention under the hospital scenario is suitable for the national conditions in China and similar countries. Interventions are usually carried out by professionals in clinical settings, therefore, efforts should be made to improve the effectiveness of EFT-P.
Limitation
A few limitations of this study should be noted. First, the parental involvement in this study was not strong enough. Although we encouraged parents to continue using strategies and activities at home, we did not provide strong support and supervision to promote home practices like we did when providing EF training for school age children with ADHD (Shuai et al., 2017). When the therapist introduced the strategies to the parents, the child stayed in the same room with lots of noise and movements, which might have interfered with the parent’s learning. Despite 30 min of guidance for parents, there is still a lack of systematic training for parenting based interventions. Second, the training “dose” might be low in this study. The treatment only lasted for 8 weeks with 1 hr for children per week. We plan to revise the EFT-P to solve these limitations. Third, in China, many children’s caregivers not only consist of their parents, but also grandparents. Therefore, that the parent who participated in the interview and who filled in the questionnaires might not the same caregiver. This may be one of the explanations why SNAP and DIPA results were inconsistent. We will try to keep the questionnaire and interview evaluation that are provided by the same caregiver in further research.
Conclusion
Overall, the results of this RCT suggest that EFT-P is a feasible intervention to administer in a population of preschool children with ADHD in a clinical setting. The data also indicates considerable palatability for the program as measured by attendance and satisfaction surveys. EFT-P is effective in reducing young children’s ADHD and ODD symptoms, and improving visuomotor precision. Further RCTs using a revised EFT-P is needed to determine the true clinical utility of this program.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by Grants from the Scientific research project of Shanghai Science and Technology Commission (14411968600), Shanghai Top-Priority Clinical Key Discipline (2017ZZ02026), and Xinhua Hospital Research Fund (XH2417).