
Abstract
Objective:
Shared genetic mechanisms have been hypothesized to explain the comorbidity between ADHD and asthma. To evaluate their genetic overlap, we relied on data from the 1982 Pelotas birth cohort to test the association between polygenic risk scores (PRSs) for ADHD (ADHD-PRSs) and asthma, and PRSs for asthma (asthma-PRSs) and ADHD.
Method:
We analyzed data collected at birth, 2, 22, and 30 years from 3,574 individuals.
Results:
Subjects with ADHD had increased risk of having asthma (OR 1.92, 95% CI 1.01–3.66). The association was stronger for females. Our results showed no evidence of association between ADHD-PRSs and asthma or asthma-PRSs and ADHD. However, an exploratory analysis suggested that adult ADHD might be genetically associated with asthma.
Conclusion:
Our results do not support a shared genetic background between both conditions. Findings should be viewed in light of important limitations, particularly the sample size and the self-reported asthma diagnosis. Studies in larger datasets are required to better explore the genetic overlap between adult ADHD and asthma.
Introduction
ADHD is a common neurodevelopmental disorder characterized by impairing and persistent symptoms of inattention, and/or hyperactivity/impulsivity (Faraone et al., 2015). The disorder has an estimated prevalence rate of 5.2% in school-aged children (Polanczyk et al., 2007) and 2.5% in adults (Vitola et al., 2017). The genetic architecture of ADHD is highly polygenic, where common variations contribute to a large proportion of its heritability (Demontis et al., 2019). ADHD is highly comorbid, and it has been shown that about 50% to 70% of both children and adults with ADHD have a psychiatric comorbidity (Biederman et al., 1991, 1993). Interestingly, over the last years there has been a growing body of literature indicating that ADHD is also associated with several immune-related disorders (Buske-Kirschbaum et al., 2013; Miyazaki et al., 2017; Nielsen et al., 2017; Schans et al., 2017). Among those, the comorbidity between ADHD and asthma has been repeatedly demonstrated and therefore is of particular interest (Cortese et al., 2018).
Asthma is a heterogeneous disease characterized by bronchial hyperresponsiveness associated with a chronic inflammatory process (Olin & Wechsler, 2014). Cortese et al. (2018) published a systematic review and meta-analysis reporting that patients with ADHD had an increase of 66% in the odds of having asthma. Most importantly, the association remained significant even after adjusting for known confounders (Cortese et al., 2018). A recent study has demonstrated a positive genetic correlation between adult-onset asthma and ADHD, and a Mendelian randomization analysis showed evidence of a causal effect of ADHD on asthma (Zhu et al., 2019). Therefore, it can be hypothesized that the high comorbidity between ADHD and asthma is the result of a common genetic background. The impact of genetic overlap between two conditions can be evaluated using polygenic risk scores (PRSs), which represents the additive effect of susceptibility loci for certain phenotype, in a cross-trait approach (Marees et al., 2018). Therefore, the objective of this study was to determine whether there is a genetic overlap between ADHD and asthma using PRSs. As far as we are concerned, this is the first study to investigate shared genetic mechanisms between ADHD and asthma using PRSs. Under the hypothesis of a common genetic background between both conditions, we constructed PRSs for ADHD and asthma using summary statistics from GWAS meta-analysis (GWAS-MAs) (Pividori et al., 2019; Rovira et al., 2020) and tested their association with ADHD and asthma in the 1982 Pelotas (Brazil) birth cohort.
Material and Methods
Sample and Phenotypic Assessment
Data from the 1982 Pelotas (Brazil) birth cohort was used. This cohort started with a perinatal health survey including all children born in maternity wards in the city of Pelotas in 1982. Those liveborns whose family lived in the urban area of the city (n = 5,914) were examined and their mothers interviewed soon after delivery, and these subjects have been followed for several times. Detailed description of assessments and attrition rates can be found elsewhere (Barros et al., 2008; Victora & Barros, 2006). For this study we have used data collected at birth (1982), 2 years (1984), 22 years (2004), and 30 years (2012).
In 2012, 3,574 subjects from the cohort were screened for ADHD in interviews applied by trained psychologists (Horta et al., 2015; Vitola et al., 2017). Screening was conducted using four inattention items and two hyperactivity items of the World Health Organization Adult ADHD Self-report Scale, as previously described (Vitola et al., 2017). Individuals that were positive in at least two items were subjected to a structured interview for the diagnosis of ADHD based on the DSM-5 criteria (Matte et al., 2015). In addition to data on ADHD diagnosis, the total number of inattention or hyperactivity/impulsivity symptoms reported by subjects with a full assessment was used as a continuous measurement of symptomatology.
The prevalence of asthma was estimated using data collected in 1984, 2004, and 2012. The following question was answered by the mothers in 1984 (children at 2 year of age): “Have your children ever had asthma or bronchitis?” In 2004 and 2012, when subjects were 22 and 30 years, they were required to answer the following question: “Have you ever had asthma or bronchitis in your life?” Based on that, subjects were classified as having asthma if a positive answer was giving on all evaluations. Only subjects that consistently reported an asthma diagnosis were classified as asthmatic for our analyses. This classification was intended to decrease the number of false positive diagnosis that could be present due to recall bias. In addition, since the current body of literature supports the presence of a higher genetic influence in early-onset when compared to late-onset asthma (Belsky et al., 2013), the inclusion of subjects with an early-onset disease could increase our power to detect genetic associations. Subjects with two positive answers and one missing data (n = 88) were included in the analysis as asthmatic subjects.
DNA Sample
Blood samples were collected during the 22-year follow-up (Lima-Costa et al., 2015). DNA was extracted from venous blood using the salting-out technique, based on the protocol established by Miller et al. (1988). DNA samples were genotyped for approximately 2.5 million genetic variants using the Illumina (CA, USA) HumanOmni2.5-8v1 array. In Pelotas, with few exceptions, cohort members were unrelated and have low consanguinity (Kehdy et al., 2015). Further details on genotyping techniques, results on genomic ancestry and quality control parameters can be found elsewhere (Kehdy et al., 2015; Lima-Costa et al., 2015). For the non-genotyped genetic variants, imputation was performed based on data from the overall population of the 1,000 Genomes Project Phase I integrated haplotypes (December 2013 release) as a reference panel (1000 Genomes Project Consortium et al., 2012). Imputation was performed using SHAPEIT (O’Connell et al., 2014) and IMPUTE2 (Delaneau et al., 2013).
Polygenic Risk Scores (PRS) Analysis
PRSs are created by combining the effect sizes estimated from GWAS for each single nucleotide polymorphism (SNP) surpassing a certain threshold of significance (Marees et al., 2018). Prior to creating the PRS, imputed and genotyped SNPs were filtered to include only those with (i) <2% missing genotypes, (ii) imputation quality score (INFO) ≥ 0.8, and (iii) minor allele frequency (MAF) ≥ 0.01, using PLINK 1.9 (Purcell et al., 2007). Variants out of Hardy Weinberg Equilibrium (HWE) (p < 1 × 10−06) were excluded before the score construction. The same procedure has been reported elsewhere (Ibanez et al., 2017). After the application of the quality control filters, 5,760,740 variants were retained for PRS analysis. Only autosomal variants were included. The major histocompatibility complex region (chr6: 26-33M) was removed.
PRSs for ADHD (ADHD-PRSs) were calculated using data from the International Multi-center persistent ADHD CollaboraTion (IMpACT) GWAS-MA (Rovira et al., 2020) as the discovery sample. The IMpACT dataset was used to compute PRSs based on summary statistics from adults and children with ADHD separately. The sample included 10,358 cases and 16,278 controls (only children), and 6,115 cases and 15,411 controls (only adults), all with European ancestry. In order to ensure independence between the discovery and target sample, all Brazilian subjects from the database by Rovira et al. (2020) were excluded and the summary statistics of a new meta-analysis including the remaining subjects was used.
PRSs for asthma (asthma-PRSs) were generated using data from the UK Biobank as the discovery sample (Pividori et al., 2019). We used data from subjects with self-report or doctor-diagnosed asthma divided in childhood (onset before 12 years of age) or adult-onset disease (onset between 26 and 65 years of age) (Pividori et al., 2019). The sample consisted of 9,433 adults with childhood-onset asthma, 21,564 adults with adult-onset asthma, and 318,237 controls.
For PRS calculation we used the genetic additive model, using the sum of the weighted effect alleles for independent markers across the genome. Genomic 250 kb window and 0.1 r2 linkage disequilibrium were used as criteria to define independent SNPs. PRSs were calculated using PRSice-2.21 (https://choishingwan.github.io/PRSice/) (Choi & O’Reilly, 2019; Euesden et al., 2015). Subsequently, ADHD-PRSs or asthma-PRSs were tested for association with ADHD and asthma in the 1982 Pelotas birth cohort. We included a range of PRS at increasingly liberal significance thresholds (PT) defined a priori (5 × 10−6; .05; .1; .3; .5). The score outputs (from PRSice 2.2.1) were exported to Stata 14 (Stata Corporation, 245 CollegeStation, USA), where they were standardized to z-scores.
Statistical Analysis
The association between self-reported asthma diagnosis and ADHD diagnosis was evaluated using multivariate logistic regression models. The following covariates were added to the model: sex, birthweight, maternal age at birth, maternal smoking during pregnancy, maternal years of study, and family income. Covariates were chosen a priori based on previous knowledge regarding their association with both ADHD and asthma (Cortese et al., 2018). In the first analysis, ADHD diagnosis according to DSM-5 was used as the categorical independent variable. In a secondary analysis, a linear regression was performed using the total sum of inattention or hyperactivity/impulsivity symptoms (ranging from 0 to 9) observed in each patient according to the DSM-5 as a continuous independent variable. This data was available only for individuals who performed the full assessment after a positive screening (n = 666).
Multivariate logistic regression models were also used to test the association between ADHD-PRSs and asthma diagnosis, and between asthma-PRSs and ADHD diagnosis. Ten principal components from the principal component analysis calculated based on whole genomic dataset using PLINK1.9 (Purcell et al., 2007) and sex were included in the controlled analysis. In order to show the prediction ability of each tested PRS, pseudo-R2 statistics was estimated and the amount of variance explained was calculated as the difference in pseudo-R2 between the full model and the null model. Considering that the PRSs were calculated at different p-value threshold, we applied the Benjamini-Hochberg false discovery rate (FDR) method (Benjamini & Hochberg, 1995) in order to correct for multiple comparisons. A false discovery rate of 5% was applied, and results were considered to be statistically significant if the correct p-value was <.05.
Ethics Committee
The study was approved by the Ethics Committee of the School of Medicine of the Universidade Federal de Pelotas, and all participants signed an informed consent form. All procedures contributing to this work comply with the Helsinki Declaration of 1975, as revised in 2008.
Results
From the 5,914 live born infants from 1982, 3,574 (60.4%) were screened for ADHD at 30 years, and 2,798 (47.3%) had genetic data. From those, 666 (23.8%) screened positive and 74 (2.6%) were diagnosed with ADHD according to DSM-5. Table 1 presents the demographic characteristics of individuals with and without ADHD. The prevalence of self-reported asthma (considering subjects with a positive answer in all evaluations) was 9.7% in the whole population and 16.2% in the ADHD population. Perinatal demographic differences between subjects screened at 30 years and the whole population can be found at Supplemental Table 1, and between subjects with and without genetic data can be found at Supplemental Table 2.
Demographic Characteristics of Individuals with and without ADHD.
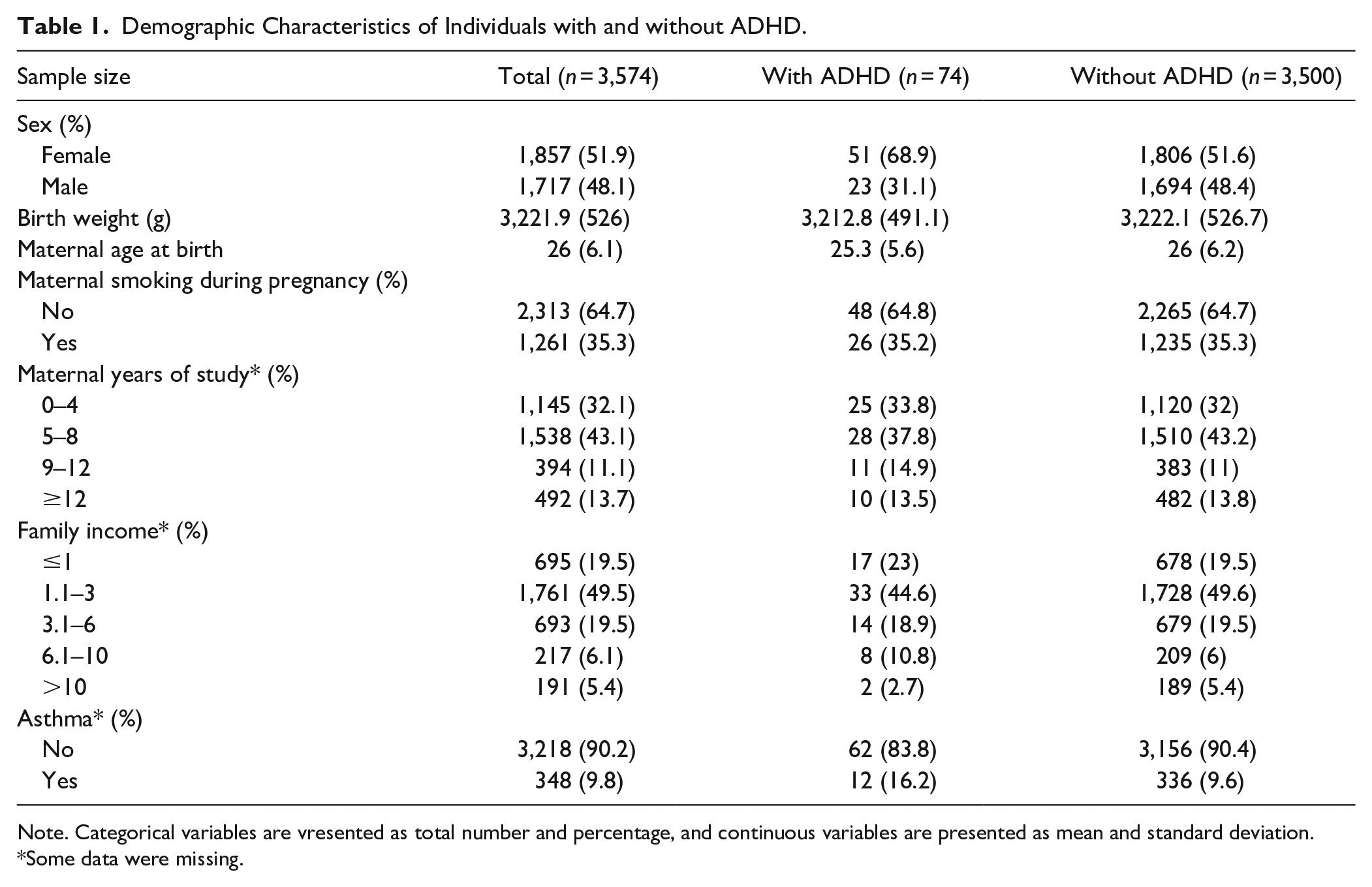
Note. Categorical variables are vresented as total number and percentage, and continuous variables are presented as mean and standard deviation. *Some data were missing.
Association between ADHD Diagnosis and Self-Reported Asthma Diagnosis
Table 2 shows the results from the association between ADHD and asthma. After adjusting for potential confounders, there was a statistically significant association between ADHD (diagnosis at 30 years of age) and self-reported asthma (OR 1.92, 95% CI 1.01–3.66). Additionally, asthma was also associated with the total number of ADHD symptoms (OR 1.08, 95% CI 1.01–1.16), and with the total number of hyperactivity/impulsivity symptoms (OR 1.19, 95% CI 1.06–1.33), but not with inattention symptoms (OR 1.03, 95% CI 0.93–1.15). The association between ADHD diagnosis and asthma was observed only in the female population (OR 2.29, 95% 1.07–4.89 for females; OR 1.25, 95% CI 0.36–4.39 for males), the same was true for asthma and the total number of ADHD symptoms (OR 1.12, 95% CI 1.02–1.23 for females; OR 1.03, 95% CI 0.92–1.16 for males) and number of hyperactivity/impulsivity symptoms (OR 1.23, 95% CI 1.05–1.44 for females; OR 1.12, 95% CI 0.94–1.35 for males).
Association between Asthma and ADHD: Adjusted Regression Analyses.

Note. Association between asthma and ADHD was evaluated using logistic regression. Asthma status was used as the categorical dependent variable. The following covariates were added to the model: sex, birthweight, maternal age at birth, maternal smoking during pregnancy, maternal years of study and family income. OR = odds ratio.
Some data were missing.
Association between ADHD-PRSs and ADHD
Odds ratio, p-values and FDR corrected p-values from the regression analysis for the association between ADHD-PRSs and ADHD can be found in Supplemental Table 3. Before FDR correction, increased childhood ADHD-PRSs were associated with ADHD diagnosis (OR 1.32, 95% CI 1.01–1.73, PT = 5e−6), with higher total number of ADHD symptoms (β 0.40, 95% CI 0.03–0.77, PT = .3; β 0.39, 95% CI 0.02–0.75, PT = .5), and with higher number of inattention symptoms (β 0.24, 95% CI 0.03–0.45, PT = 5e−6). However, there was no statistically significant association after correction for multiple comparisons (Supplemental Tables 4 and 5). Childhood ADHD-PRSs were associated with higher number of hyperactivity/impulsivity symptoms in one p-value threshold after FDR correction (β 0.27, 95% CI 0.04–0.50, PT = .5) (Supplemental Table 6).
Association between ADHD-PRSs and Asthma
In the association between ADHD-PRSs and asthma (Table 3), we found no statistically significant result after FDR correction. Prior to FDR correction, increased adult ADHD-PRSs were associated with increased odds of having asthma in one out of five p-value cutoffs (OR 1.14, 95% CI 1.00–1.30, PT = .5), with a trend in other three (OR 1.12, 95% CI 0.99–1.28, PT = .05; OR 1.12, 95% CI 0.98–1.27, PT = .1; OR 1.13, 95% CI 0.99–1.29, PT = .3).
Adjusted Logistic Regression Results for the Association Between ADHD-PRSs and Asthma.
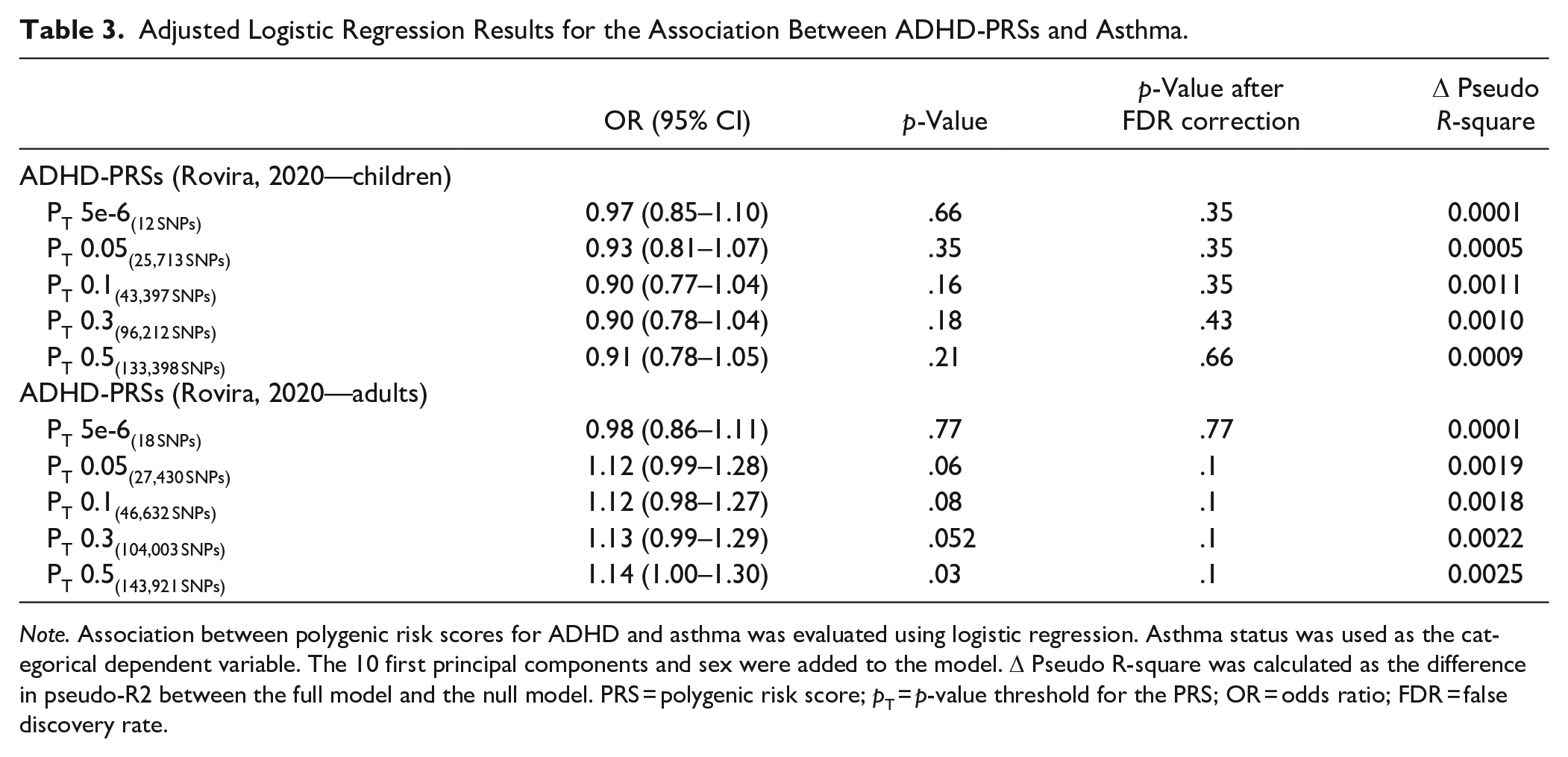
Note. Association between polygenic risk scores for ADHD and asthma was evaluated using logistic regression. Asthma status was used as the categorical dependent variable. The 10 first principal components and sex were added to the model. Δ Pseudo R-square was calculated as the difference in pseudo-R2 between the full model and the null model. PRS = polygenic risk score; pT = p-value threshold for the PRS; OR = odds ratio; FDR = false discovery rate.
Association between Asthma-PRSs and Asthma and Asthma-PRSs and ADHD
Supplemental Table 7 shows the logistic regression analysis results for the association between asthma-PRSs and asthma in the Pelotas cohort. In the non-corrected analysis, there was a positive association between childhood asthma-PRSs and asthma in most of the p-value cutoffs tested (OR 1.18, 95% CI 1.03–1.34, PT = .05; OR 1.14, 95% CI 1.00–1.30, PT = .1; OR 1.16, 95% CI 1.02–1.33 PT = .3), with a trend in the PT = .5 (OR 1.14, 95% CI 0.99–1.30). The association with childhood asthma-PRSs remained significant after FDR correction in the 0.05 and 0.3 cutoffs. There was no significant association between adult asthma-PRSs and asthma diagnosis. Association between asthma-PRSs and ADHD diagnosis can be found in Table 4. There was no significant association even before FDR correction.
Adjusted Logistic Regression Results for the Association between Asthma-PRSs and ADHD.

Note. Association between polygenic risk scores for asthma and ADHD diagnosis was evaluated using logistic regression. ADHD status was used as the categorical dependent variable. The 10 first principal components and sex were added to the model. Δ Pseudo R-square was calculated as the difference in pseudo-R2 between the full model and the null model. PRS = polygenic risk score; pT = p-value threshold for the PRS; OR = odds ratio; FDR = false discovery rate.
Discussion
The present study was designed to determine the possible genetic association between ADHD and asthma using PRSs derived from ADHD and asthma discovery samples, together with epidemiological data from a birth cohort. Briefly, our results provided additional evidence on the comorbidity between ADHD and asthma, suggesting that the association might be driven by hyperactivity/impulsivity symptoms. ADHD-PRSs were able to predict hyperactivity/impulsivity symptoms but only predicted ADHD diagnosis in one p-value cutoff, with no significant results after correction for multiple comparisons. On the other hand, childhood asthma-PRSs were able to predict asthma in the Pelotas cohort, but no evidences supporting the hypothesis that both conditions have a shared genetic background were found. However, an exploratory analysis indicated a possible genetic association between adult ADHD and asthma.
Our study confirms previous findings showing comorbidity between ADHD and asthma. We showed that having ADHD diagnosis according to DSM-5 increases in 1.9 times the odds of having asthma even after controlling for known confounders. This association has been already described by several authors in both children (Calam, Gregg, & Goodman, 2005; Calam, Gregg, Simpson, et al., 2005; Hammer-Helmich et al., 2016; Jameson et al., 2016; Kline-Simon et al., 2016; Kwon et al., 2014; Leibson et al., 2001; Meyers et al., 2010; Romanos et al., 2010; Schmitt et al., 2009; Silva et al., 2014; Yang et al., 2018) and adults (Fasmer, Halmøy, et al., 2011; Fasmer, Riise, et al., 2011; Secnik et al., 2005; Stickley et al., 2017) with ADHD. The evidence we have examined suggests that the comorbidity between ADHD and asthma is significantly higher for women when compared to men. Those findings corroborate previous studies showing higher rates of ADHD and asthma comorbidity in women (Fasmer, Halmøy, et al., 2011; Holmberget al., 2015), and higher chances of being prescribed asthma and ADHD medication simultaneously in women when compared to men with ADHD (Fasmer, Riise, et al., 2011). In our sample, 69% and 46% of subjects with ADHD diagnosis and self-report asthma were female, respectively. A higher prevalence of ADHD in females during adulthood has been previously reported in clinical (Karam et al., 2015) and population-based samples (Kooij et al., 2005; Matte et al., 2015), and this gender disparity has been approached elsewhere (Kooij et al., 2010). The impact of gender on the comorbidity between ADHD and asthma deserves further empirical studies.
Curiously, a separate analysis of hyperactivity/impulsivity and inattention symptoms demonstrated that only hyperactivity/impulsivity symptoms were associated with increased odds of having asthma. The findings of the current study are consistent with Jameson et al. (2016), where the prevalence of asthma was significantly higher in patients with the hyperactive/impulsive subtype when compared to inattention subtype. Similar findings were also reported by Mogensen et al. (2011), who showed that children with asthma at the age of 8 to 9 years had increased symptoms of hyperactivity/impulsivity at 13 to 14 years, with no difference in inattention symptoms. Those findings might point to a distinct pattern of comorbidities according to different ADHD dimensions, and should be further explored.
ADHD-PRSs calculated using the IMpACT database were not able to predict asthma diagnosis in the 1982 Pelotas Birth Cohort, arguing against a shared genetic background between both conditions. However, we observed a trend for increased odds of an asthma diagnosis in subjects with a higher adult ADHD-PRSs in four out of the five p-value thresholds selected, although we did not find statistically significant results after correcting for multiple comparisons. Moreover, the odds ratio was found to be at the same direction for all p-value thresholds, pointing to a similar predisposition of being diagnosed with asthma with increasing PRSs for adult ADHD. These results could be useful to design new hypothesis-driven studies investigating the role of adult ADHD in the genetic association between ADHD and asthma.
Higher odds of having asthma with increased adult ADHD-PRSs could be the result of stable genetic influences from childhood, newly arising dynamic genetic influences in adulthood, or a combination of both. Several longitudinal studies evaluating subjects from childhood to adolescence have shown that a persistent trajectory of ADHD is associated with a higher genetic influence (Kuntsi et al., 2005; Larsson et al., 2006; Rietveld et al., 2004). Hence, a possible interpretation is that the use of PRSs derived from an adult sample could be selecting subjects lying at the extreme end of a continuous genetic predisposition for the disorder. On the other hand, this association might also be driven by the genetic influence of a subsample of adult ADHD patients with a distinct pattern of comorbidities and possibly a distinct pathophysiology. There has been recent debate regarding the possibility of an adult-onset ADHD based on data from different cohorts (Agnew-Blais et al., 2016; Caye et al., 2016; Moffitt et al., 2015). The hypothesis of an adult ADHD with similar phenotype but distinct pathophysiological mechanisms should be kept in mind, even though it would certainly require a complete new set of evidences.
It is important to highlight that the association of ADHD-PRSs and ADHD diagnosis was only significant in the 5e−6 p-value cutoff, arguing against the validity of the PRSs in this population. These results might indicate heterogeneity in the genetic background between the discovery and target samples, diagnosis inaccuracy in the Pelotas cohort sample, or even a lack of statistical power since there were only 74 subjects with an ADHD diagnosis in the target sample. However, we have observed a positive association between the ADHD-PRSs and hyperactivity/impulsivity symptoms in the subsample subjected to a full assessment. Those results suggest a higher genetic influence in subjects with hyperactivity/impulsivity phenotypes, even though higher inattention symptoms in childhood have been associated with ADHD persistence into adulthood (Lara et al., 2009).
Our results should be viewed in light of several limitations. Our main limitation is the sample size, since only 74 subjects had a diagnosis of ADHD in the cohort. In this sense, the study could be underpowered to detect significant differences. In addition, even though we have used data from a birth cohort, an ADHD diagnosis was only performed at the age of 30 years, dampening our ability to explore causality. Furthermore, we decided to use data only for those subjects which reported an asthma diagnosis consistently in all evaluations—at 2, 22, and 30 years. Therefore, patients with symptoms starting after 2 years were not included in the current analysis as asthmatic subjects. Another limitation is the fact that asthma diagnosis was self-reported, which might be a source of bias since subjects with mild disease are less prone to report their asthma (Torén et al., 2006). It is important to stress that a dimensional assessment of ADHD symptoms was only performed in a subsample of subjects that screened positive for the disorder. Moreover, while the PRSs were calculated based on European discovery samples, our target sample was composed by a mixed population in which the median European individual ancestry was shown to be 85.3% (Lima-Costa et al., 2015), a fact that might have also reduced our statistical power.
One of the strengths of our analysis is the use of a birth cohort, thereby decreasing the chance of selection bias due to the use of a clinically referred sample. Furthermore, the 1982 Pelotas birth cohort retained 68.1% of the original population, a follow-up rate similar to that observed in birth cohort from high-income countries, and higher than the ones found in cohort from low- or middle-income countries (Lima-Costa et al., 2015). The cohort also included more than 99% of all births that took place in 1982, and, as a result, it can be considered a representative sample of the city’s population (Lima-Costa et al., 2015). Although the follow-up rates at 30 years were slightly higher among females and among subjects in intermediate socioeconomic categories, it is unlikely that this difference would be enough to bias the final results. Psychiatric diagnoses were carried out by trained psychologists in face-to-face interviews, increasing the accuracy of diagnosis. As far as we are concerned, we are the first to investigate genetic associations between ADHD and other conditions using PRSs derived from children and adult patients separately. In this sense, our findings might stimulate research focusing on the shared and distinct patterns of genetic correlation between children and adults with ADHD.
To sum up, the main findings of this research do not support a shared genetic background between ADHD and asthma, but an exploratory analysis suggests that adult ADHD might be genetically associated with asthma. Studies with larger sample sizes should be conducted in order to test if our negative findings are related to a lack of power. The presence of a shared genetic architecture between adult ADHD and asthma might point to a subsample of ADHD patients with a distinct pattern of comorbidities. The role of gender and ADHD subtypes in the comorbidity between ADHD and asthma should be further explored.
Supplemental Material
sj-pdf-1-jad-10.1177_10870547211020111 – Supplemental material for Association between Polygenic Risk Scores for ADHD and Asthma: A Birth Cohort Investigation
Supplemental material, sj-pdf-1-jad-10.1177_10870547211020111 for Association between Polygenic Risk Scores for ADHD and Asthma: A Birth Cohort Investigation by Douglas Teixeira Leffa, Bernardo Horta, Fernando C. Barros, Ana M. B. Menezes, Thais Martins-Silva, Mara Helena Hutz, Claiton Henrique Dotto Bau, Eugenio Horacio Grevet, Luis Augusto Rohde and Luciana Tovo-Rodrigues in Journal of Attention Disorders
Footnotes
Acknowledgements
We thank all the subjects who took part in this research. We thank Paula Rovira, Maria Soler, Antoni Ramos-Quiroga, and Marta Ribasés for providing summary statistics from their genome-wide association study and Marta Ribasés for also critically reviewing the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Grevet served as a consultant to Shire/Takeda do Brasil, and served on the speakers’ bureau of Novartis/Sandoz and Shire/Takeda in the last three years. Dr. Rohde has received grant or research support from, served as a consultant to, and served on the speakers’ bureau of Bial, Medice, Novartis/Sandoz, Pfizer and Shire/Takeda in the last three years. The ADHD and Juvenile Bipolar Disorder Outpatient Programs chaired by Dr. Rohde have received unrestricted educational and research support from the following pharmaceutical companies in the last three years: Novartis/Sandoz and Shire/Takeda. Dr. Rohde has received authorship royalties from Oxford Press and ArtMed and travel grants from Shire to take part in the 2018 APA annual meeting. All other authors have nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is based on data from the study “Pelotas Birth Cohort, 1982” conducted by Postgraduate Program in Epidemiology at Universidade Federal de Pelotas with the collaboration of the Brazilian Public Health Association (ABRASCO). The International Development Research Center, World Health Organization, Overseas Development Administration, European Union, National Support Program for Centers of Excellence (PRONEX), the Brazilian National Research Council (CNPq), and the Brazilian Ministry of Health supported previous phases of the study. DTL was supported by a CNPq postdoctoral fellowship (grant number 154116/2018-1), and supported by a NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation (gran number 29486). This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001. LTR is also supported by the CNPq.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.