
Abstract
Objective:
To examine the relationship between nation-level prevalence of ADHD and COVID-19 prevalence and mortality indices.
Method:
Associations between nation-wise estimated prevalence, crude mortality rates and case-fatality ratios for COVID-19 and estimated prevalence rates for ADHD were examined, controlling for medical conditions known to be associated with COVID-19 outcome, as well as demographic, climate-related, and economic variables.
Results:
Prevalence of ADHD was positively correlated with COVID-19 prevalence and crude mortality rates on bivariate analyses, though the strength of this association was low. On multivariate regression, prevalence of ADHD was negatively associated with COVID-19 prevalence and crude mortality rates, though only the former finding was statistically significant.
Conclusion:
The association between ADHD and COVID-19 prevalence and mortality at a national level is inconsistent, modest, and may be largely due to confounding factors such as age, lifestyle factors, and medical comorbidities.
Introduction
ADHD is one of the most frequently diagnosed behavioral disorders in childhood, characterized by a triad of inattentiveness, impulsivity, and over-activity (Faraone et al., 2021). The estimated global prevalence of ADHD in children is 6.7% to 7.8% (Thomas et al., 2015), and a substantial number of individuals have symptoms persisting into adulthood (Caye et al., 2016). The current scientific consensus is that ADHD is a neurodevelopmental disorder arising from the interaction of genetic and environmental factors (Gallo & Posner, 2016). From the perspective of evolutionary advantage theory, some of the traits associated with ADHD are postulated to offer a survival advantage in specific environments, in which rapid responses and high levels of exploratory behavior are required (Arildskov et al., 2021). From this point of view, the disorder clinically diagnosed as ADHD may represent the extreme end of a continuum of temperamental traits such as high novelty seeking, high harm avoidance, and low persistence (McLennan, 2016; Pinzone et al., 2019), and may be accentuated by exposure to specific environmental factors either pre- or post-natally (Azeredo et al., 2018). Such a model would account for the persistence of this disorder across cultures and populations (Williams & Taylor, 2006), as well as the difficulties faced by individuals with these traits in environments that require alternate response patterns characterized by greater persistence and more sustained patterns of behavioral change (Kirova et al., 2019).
These hypotheses have been brought into focus by the current global pandemic of novel coronavirus disease (COVID-19), which is a situation characterized by a high level of threat, resource scarcity (potential or actual), and the need to adapt rapidly to changes in one’s social environment (Coelho et al., 2020; Dickins & Schalz, 2020). The lockdowns and other restrictions necessitated by this pandemic may be poorly tolerated by individuals suffering from syndromal ADHD (Bruni et al., 2021). It has been observed that the presence of ADHD is associated with poorer adaptation to the COVID-19 pandemic (Pollak et al., 2021a) as well as increased psychological distress (Pollak et al., 2021a; Swansburg et al., 2021), decline in financial status (Pollak et al., 2021a), and an increased risk of adopting unhealthy dietary practices (Swansburg et al., 2021). These effects could potentially increase the risk of infection with SARS-CoV-2, as well as lead to poorer outcomes in infected patients with ADHD (Rajkumar, 2021). The effective control of COVID-19 also requires sustained adherence to safety measures, such as masking, social distancing, and hand hygiene, which might pose problems for individuals with low persistence and high impulsivity (Merzon et al., 2021a). This was confirmed in two recent reports which found that the presence of ADHD symptoms was associated with an increased likelihood of non-adherence to safety measures (Pollak et al., 2021a, 2021b). ADHD has also been associated with alterations in immune and inflammatory activity, such as elevated or decreased levels of particular inflammatory mediators (Anand et al., 2017; Chang et al., 2020, 2021; Krahel et al., 2021). It is not clear if these changes have a beneficial or harmful effect in individuals with SARS-CoV-2 infection (Yonas et al., 2020).
In line with these findings, some researchers have found an association between ADHD and a greater clinical severity of COVID-19 (Merzon et al., 2021b). However, another group of researchers has observed found a spatial correlation between the regional prevalence of ADHD and COVID-19 recovery rates (Arbel et al., 2020), suggesting a possible protective effect. While neither of these findings can be taken as definitive, they suggest that further analysis of the relationship between ADHD and the risk of infection with, or mortality from, COVID-19 is warranted. Such an analysis would lack validity unless corrected for several potential confounders. These include demographic factors such as age, gender, and socioeconomic status (Shi et al., 2021), lifestyle factors such as obesity and nicotine use (Hou et al., 2021; Rajkumar, 2021), the presence of comorbid medical conditions (Dorjee et al., 2020; Shi et al., 2021; Thakur et al., 2021), the extent and duration of protective measures, such as screening and lockdown, imposed by local and federal governments (Johanna et al., 2020), and even climatic factors such as temperature and humidity (Chen et al., 2021; Sajadi et al., 2020). Without correction for these factors, any observed association between ADHD and COVID-19-related indices may represent an incidental or chance finding. Therefore, the current study was undertaken to examine: (a) the relationship between the population-level burden of ADHD and the estimated prevalence of COVID-19, and (b) the relationship between the burden of ADHD and measures of COVID-19 mortality, after correcting for the influence of the numerous, independent factors that could influence these variables.
Methodology
Data Sources
Assuming that ADHD lies on a continuum with ADHD-like traits that are more widely distributed in a given population (McLennan, 2016; Williams & Taylor, 2006), it can be further assumed that the regional prevalence of ADHD would be positively correlated with the presence of such traits in a given region.
The most recent estimates of the prevalence of ADHD for each country (ADHD-Prev), derived from the 2019 Global Burden of Disease Study, were used for the purpose of this analysis. This data is available in the public domain for non-commercial research purposes, and was obtained from a database query from the Global Burden of Disease Collaborative Network’s website (Global Burden of Disease Collaborative Network, 2020). Complete data on this variable could be obtained for 156 countries, and these countries were included in subsequent analyses.
COVID-19 related data was obtained from the Johns Hopkins University’s Coronavirus Resource Centre, which provides real-time updates of global and national numbers of COVID-19 cases based on official data, as well as mortality analyses (Dong et al., 2020; Johns Hopkins University of Medicine, 2021). Three nation-level indices related to COVID-19 were obtained from this source:
(a) estimated prevalence (C19-Prev), defined as the number of COVID-19 cases per 100,000 population,
(b) crude mortality rates (C19-CMR), defined as the number of deaths attributed to COVID-19 per 100,000 population, and
(c) case-fatality ratio (C19-CFR), defined as the ratio between the number of deaths due to COVID-19 and the total number of cases, expressed as a percentage. COVID-CFR is calculated using the formula (C19-CMR ÷ C19-Prev) × 100.
To address the potential confounding effect of specific demographic and lifestyle factors associated with COVID-19, information on average life expectancy (in years), gross national income (expressed as current United States dollars, using the Atlas method), and prevalence of nicotine use (expressed as a percentage) was obtained from the World Bank’s database (The World Bank, 2021).
To address the potential effects of climate, the mean distance of the capital city of the equator, measured as the absolute value of the latitude, was obtained for each country from an online atlas (World Atlas, 2020). This variable was chosen because it is a reliable correlate of climatic factors such as humidity and rainfall, and has been used in prior research related to COVID-19 (Chen et al., 2021; Sajadi et al., 2020).
In order to assess the confounding effect of comorbid medical conditions, information on the prevalence of six medical conditions—obesity, diabetes mellitus (DM), systemic hypertension (SHT), chronic renal disease (CKD), chronic obstructive pulmonary disease (COPD), and ischemic heart disease (IHD)—was collected. These five conditions were selected because they were all significantly associated with COVID-19 severity and mortality in the most recent meta-analytic review (Dorjee et al., 2020). Information on the prevalence of DM, IHD, CKD, and COPD was obtained from the Global Burden of Disease Collaborative Network database (Global Burden of Disease Collaborative Network, 2020), while information on the prevalence of hypertension and obesity for each country was obtained from the World Health Organization’s Global Health Observatory (World Health Organization, 2021).
Data Analysis
As none of the study variables were normally distributed on applying the Shapiro-Wilk test (p < .01 for all variables), a natural logarithmic transformation was used for each variable prior to further data analysis. Pearson’s correlation coefficient (r) was used to test for linear relationships between ADHD-DALY and these variables (C19-Prev, C19-CMR, and C19-CFR). Additional bivariate correlations were carried out to examine the relationships between these variables and measures of all confounding variables—demographic (life expectancy, gross national income), lifestyle (nicotine use, obesity), climate-related (distance from the equator), and specific medical comorbidities (DM, SHT, IHD, COPD, and CKD). All tests were two-tailed, and a significance level of p < .05 was considered significant for bivariate analyses. The assessment of the strength of correlations was made using the guideline values for medical research summarized in Akoglu (2018), in which r < .1 denotes no significant correlation, .1 < r < .3 indicates a poor correlation, .3 < r < .6 indicates a fair correlation, and r > .6 indicates a strong correlation.
It was observed that the estimated prevalence of ADHD was significantly lower than the global average in 57 of the 156 countries included in this study. To address this issue, a sub-group bivariate analysis was undertaken including only those 99 countries where the prevalence of COVID-19 was greater than or equal to 1%.
Variables identified as significant in these analyses were entered into stepwise multivariate linear regression analyses with C19-Prev, C19-CMR, and C19-CFR as the dependent variables. To minimize the possibility of multicollinearity affecting the results of multivariate analyses, variance inflation factors (VIF) were computed during linear regression. A VIF > 4 was taken to indicate possible multicollinearity, and a VIF ≥ 10 as indicating significant multicollinearity likely to compromise the study’s results.
Results
Data was available for a total of 156 countries. The estimated prevalence of ADHD in these countries ranged from a minimum of 0.4% in the United Arab Emirates to a maximum of 3.6% in Belize, with a mean value of 1.2% ± 0.6% across countries.
On direct bivariate analyses, ADHD-Prev was found to be positively correlated with C19-Prev (r = .17, p = .035) and C19-CMR (r = .19, p = .019), but not with C19-CFR (r = .08, p = .306). However, the strength of these correlations, rated using the guidelines cited above, was poor (r < .3). It was observed that C19-Prev and C19-CMR were strongly positively correlated (r > .6), while C19-CFR showed a poor positive correlation with C19-CMR and a poor negative correlation with C19-Prev. The latter finding reflects the nature of the formula used to compute C19-CFR, in which C19-CMR is the numerator and C19-Prev is the denominator. A complete correlation matrix including all three COVID indices, ADHD-Prev, and all 10 confounding variables of interest is presented in Table 1. It was observed that besides ADHD-Prev, all the confounding variables identified based on prior published research were also positively correlated with C19-Prev and C19-CMR. The strength of these correlations for both these outcome variables was weak for systemic hypertension (r < .3), fair for distance from the equator and nicotine use (r < .6), and strong for gross national income, obesity, and the prevalence of all five medical conditions (r > .6).
Correlation Matrix of Associations Between COVID Indices, Estimated Prevalence of ADHD, and Other Confounding Variables.
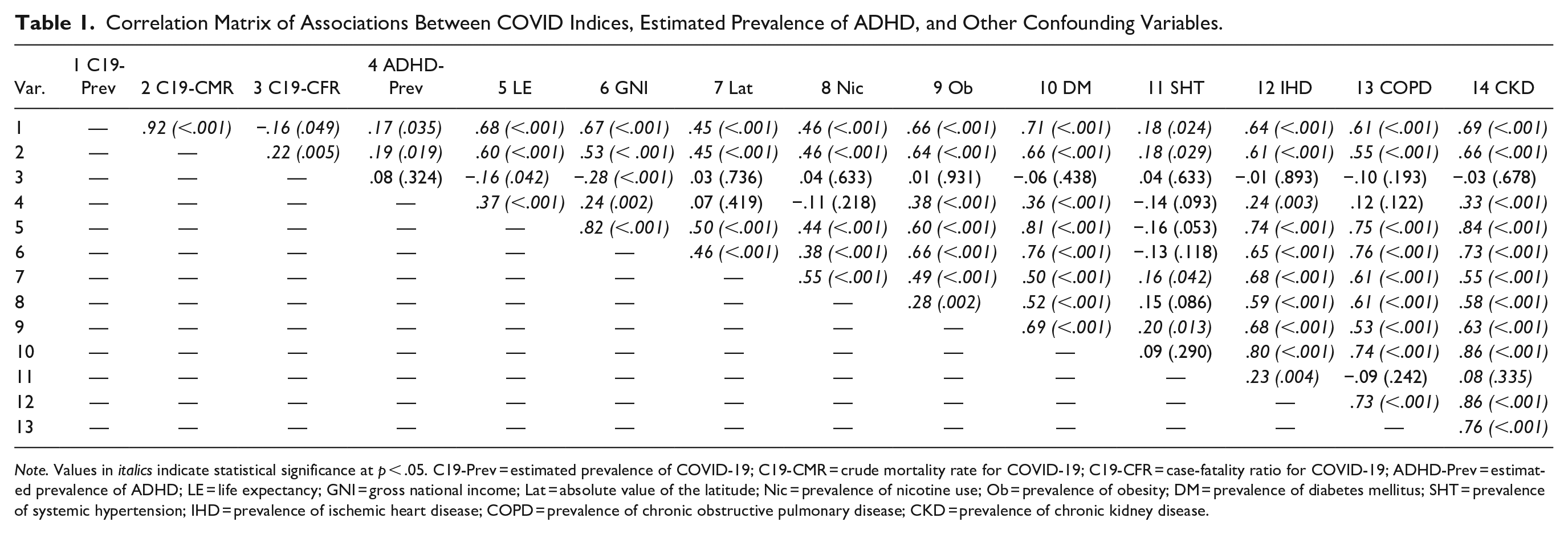
Note. Values in italics indicate statistical significance at p < .05. C19-Prev = estimated prevalence of COVID-19; C19-CMR = crude mortality rate for COVID-19; C19-CFR = case-fatality ratio for COVID-19; ADHD-Prev = estimated prevalence of ADHD; LE = life expectancy; GNI = gross national income; Lat = absolute value of the latitude; Nic = prevalence of nicotine use; Ob = prevalence of obesity; DM = prevalence of diabetes mellitus; SHT = prevalence of systemic hypertension; IHD = prevalence of ischemic heart disease; COPD = prevalence of chronic obstructive pulmonary disease; CKD = prevalence of chronic kidney disease.
Only two variables (life expectancy and gross national income) were significantly associated with C19-CFR, and the strength of both these correlations was poor (r < .3).
It was also observed that ADHD-Prev was significantly correlated with many of these confounding variables. Poor positive correlations were observed with gross national income and the prevalence of ischemic heart disease, and fair positive correlations were noted with life expectancy and with the prevalence of obesity, diabetes mellitus and chronic kidney disease.
In the subgroup analysis of 99 countries with an estimated COVID-19 prevalence of >1%, ADHD-Prev was non-significantly and negatively correlated with C19-Prev (r = −.12, p = .224) and non-significantly positively correlated with C19-CMR (r = .02, p = .817) and C19-CFR (r = .15, p = .136). In these analyses, C19-Prev was positively correlated with all the confounding variables except nicotine use and prevalence of systemic hypertension; C19-CMR was positively correlated with only six of the ten confounding variables (distance from the equator and prevalence of obesity, diabetes mellitus, ischemic heart disease, chronic obstructive pulmonary disease, and chronic kidney disease); and C19-CFR was negatively correlated with only one variable, gross national income. As ADHD was not significantly associated with any COVID-19 index, multivariate analyses were not attempted for this subgroup.
Based on these analyses, stepwise multivariate linear regression was carried out for C19-Prev and C19-CMR. Multivariate analysis for C19-CFR was not conducted, as this variable did not correlate significantly with ADHD-Prev or with the majority of confounding factors. Both these dependent variables were significantly correlated with all 11 independent variables on bivariate analysis.
The results of these analyses are presented below. The final multivariate regression model for COVID-19 prevalence (Table 2) was arrived at after six steps, included five variables, and explained approximately 62% of the variation in this variable (adjusted R2 = .619). In this model, the prevalence of ADHD showed a modest but significant negative association with C19-Prev (β = −.15, p = .02), while all the other four variables life expectancy and prevalence of obesity, diabetes mellitus, and systematic hypertension—were all positively associated with C19-Prev. Variance inflation factors were below 4 for all variables except the prevalence of diabetes mellitus (VIF = 4.11). Variables not included in the model were gross national income, distance from the equator, and prevalence of nicotine use, ischemic heart disease, chronic obstructive pulmonary disease, and chronic kidney disease.
Stepwise Linear Regression Analysis of Variables Associated With the Log-Transformed COVID-19 Estimated Prevalence.
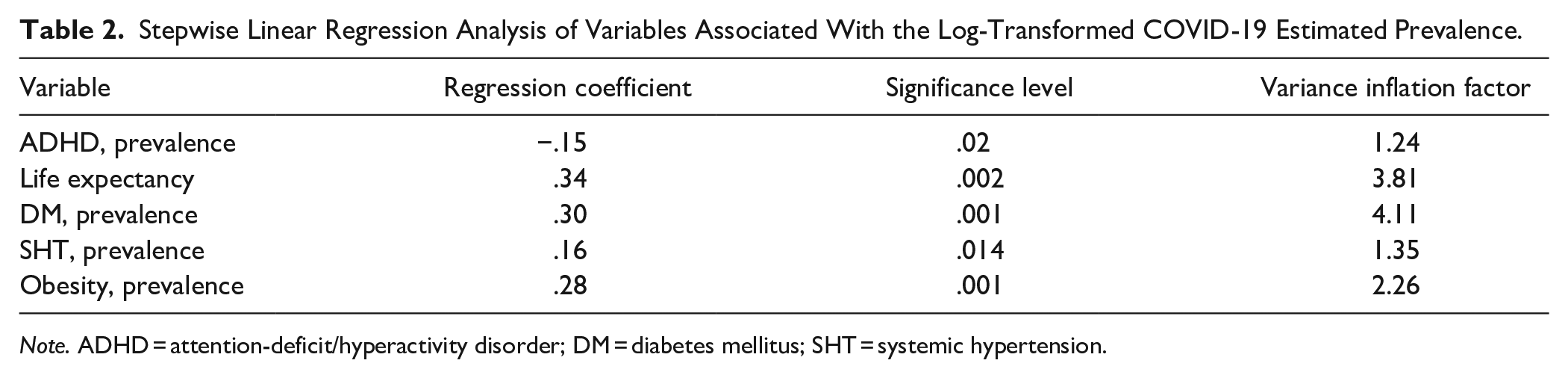
Note. ADHD = attention-deficit/hyperactivity disorder; DM = diabetes mellitus; SHT = systemic hypertension.
For the COVID-19 crude mortality rate (C19-CMR), the final multivariate model (Table 3) was arrived at after four steps, included three variables, and explained approximately 54% of the variance in this variable (adjusted R2 = .539). The three variables significantly associated with C19-CMR were the prevalence rates for obesity, nicotine use, and diabetes mellitus. All other study variables, including ADHD-Prev, were excluded from this model, and variance inflation factors for all variables were less than 4.
Stepwise Linear Regression Analysis of Variables Associated With the Log-Transformed COVID-19 Crude Mortality Rate.

Discussion and Conclusions
In this study, direct bivariate analyses suggested a weak (r < .3) positive association between the estimated national prevalence of ADHD and COVID-19 prevalence and crude mortality rates. However, on correcting for established confounding factors associated with mortality at the individual and national levels, a somewhat different result was obtained: the prevalence of ADHD was negatively associated with COVID-19 prevalence, and showed no significant association with COVID-19 crude mortality rate. These findings remained consistent regardless of the type of linear regression method adopted, suggesting that they are unlikely to be due to chance.
The finding of an apparent negative association between ADHD-Prev and COVID-19 prevalence, though unexpected, should be interpreted with caution. Available evidence suggests that ADHD, even in older adolescents and adults, is associated with a lower likelihood of adherence to public health measures (Pollak et al., 2021a, 2021b). This would be expected to lead to a relative increase in prevalence. Thus, it is likely that this association—if valid—is not related to the behaviors characteristic of ADHD but to an indirect factor of some sort. One possibility is that the immune and inflammatory changes associated with ADHD may be associated with a reduced likelihood of infection. These changes include lower levels of cortisol, elevated levels of interleukin-6 (IL-6) and C-reactive protein (CRP), and reduced levels of tumor necrosis factor alpha (TNF-α) in children and adolescents (Chang et al., 2020, 2021; Elsadek et al., 2020; Krahel et al., 2021), though these findings have not been consistent in adult patients (de Jong et al., 2016). The association with IL-6 is of particular interest, because genetic variants affecting the expression of IL-6 have been associated with variations in cross-national prevalence of COVID-19 (Karcioglu Batur & Hekim, 2021). Though it is not known if variants in the IL-6 gene and related immune genes are associated with ADHD (van Dongen et al., 2019), this hypothesis merits further investigation, as it may explain the finding of a possible “protective” effect (Arbel et al., 2020) despite the higher likelihood of “risky” behaviors in persons with ADHD.
A related hypothesis has to do with the observation that ADHD is associated with a higher risk of contracting viral respiratory infections in childhood (Li et al., 2021), which is likely related to their hyperactive and impulsive behaviors (Hak et al., 2013; Li et al., 2021). Due to this, patients with ADHD may have higher baseline rates of exposure to endemic (non-COVID) coronaviruses, which produce an asymptomatic or mild upper respiratory infection. It has been noted that patients with endemic coronavirus infections have less severe manifestations of COVID-19 due to cross-reactive antibodies (Sagar et al., 2021); if this is the case, patients with ADHD may be partially or fully protected from COVID-19, leading to either an actual decrease in prevalence, or an attenuated form of the disease that escapes detection and hence is not reflected in prevalence statistics. This hypothesis is consistent with what is known about the links between behavior and infection risk in ADHD, but requires testing through the comparison of antibody levels to endemic coronaviruses in ADHD and non-ADHD subjects.
In contrast, no significant association was observed between the estimated prevalence of ADHD and COVID-19 crude mortality rates, after correction for confounders. This suggests that there is no direct protective or harmful effect of this diagnosis on mortality at a population level; the associations observed in bivariate analyses may have been due to confounding factors, such as lower income (Gjervan et al., 2012) or comorbid substance abuse (Huntley & Young, 2014), which are both common complications of ADHD (van den Burg et al., 2019) and were significantly associated with mortality rates in this study and in others (Benzano et al., 2021). However, there was a trend toward lower mortality rates, which is consistent to a limited degree with an earlier study (Arbel et al., 2020) reporting an ecological association between prevalence of ADHD and COVID-19 recovery. It is possible that the immune changes indirectly linked to ADHD, discussed above, may have a mild attenuating effect on the severity of COVID-19. Still, it is not possible to draw a firm conclusion on this based on these results, and they must be weighed against findings of worse disease outcome in an independent study involving a clinical sample (Merzon et al., 2021b).
These results are subject to certain limitations. First, the local prevalence and outcome of COVID-19 are influenced by a multiplicity of factors, and it was not possible to account for all of these. For example, federal and local governmental measures to minimize the spread of COVID-19 can significantly affect prevalence (Johanna et al., 2020), but as these measures are difficult to operationalize and quantify, they could not be analyzed in this study. Second, a study of this kind can only identify potential correlations; it is not possible to make accurate inferences regarding causal mechanisms, and one must be cautious to avoid the ecological fallacy, in which findings at a population level are mistakenly applied to individuals. Third, the estimates of COVID-19 prevalence and mortality used in this study have a significant margin of error, as prevalence rates can be significantly influenced by a variety of other factors. These include the under-estimation of mild or asymptomatic cases (Koh & Cunningham, 2020), the availability and extent of COVID-19 testing for mildly symptomatic and asymptomatic cases or contacts (Corrao et al., 2021; Rajgor et al., 2020) and the inaccuracy of officially reported numbers of cases and deaths, particularly in lower-income countries (Corrao et al., 2021). This could lead to mistaken estimates of any link between ADHD and COVID-19 indices; this was supported by the subgroup analysis in this study, in which the prevalence of ADHD was not significantly associated with any COVID-19 variable in those countries with a COVID-19 prevalence of ≥1%. Finally, the analysis presented in this paper can only identify correlations and associations; it is not possible to conclude that ADHD has any sort of “protective” effect, even if indirect, on certain COVID-19 indices.
Nevertheless, it is hoped that these findings will add to the growing body of literature in two ways: first, by examining the potential links between mental and behavioral disorders and the regional impact of COVID-19, and second, by providing leads that would help to explain the discrepant findings in existing research on ADHD and COVID-19. It is unlikely that an ADHD diagnosis alone has a significant impact on the risk of contracting COVID-19, or on the outcome of this disease. However, a further investigation of immune and inflammatory activity in patients with ADHD and COVID-19, and of the socioeconomic and medical confounding factors present in these patients, may lead to the emergence of a more accurate estimate of potential “risk” or “protective” mechanisms. Above all, these results suggest that an observed univariate or bivariate association between any single proposed risk or protective factor and COVID-19-related variables should be viewed critically, as it may be influenced by multiple confounding factors.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.