
Abstract
Objective:
The current study assessed the utility of eye-movements measures, gathered while participants performed a commercially available Continuous Performance Test (CPT), to detect feigned ADHD-associated cognitive impairment.
Method:
Healthy simulators (n = 37), ADHD patients (n = 33), and healthy controls (n = 36) performed an eye-tracker integrated MOXO-dCPT and a stand-alone validity indicator.
Results:
Simulators gazed significantly longer at regions that were irrelevant for successful MOXO-dCPT performance compared to ADHD patients and healthy controls. This eye-movement measure, however, had lower sensitivity than traditional MOXO-dCPT indices.
Discussion:
Gaze direction measures, gathered while performing a CPT, show initial promise as validity indicators. Traditional CPT measures, however, are more sensitive and therefore offer a more promising path for the establishment of CPT-based validity indicators. The current study is an initial exploration of the issue and further evaluation of both theoretical and practical aspects is mandated.
Introduction
ADHD is common in adulthood, with estimated prevalence ranging between 2.2% and 2.8% (Faraone et al., 2021). It is associated with academic and vocational underachievement, lower quality of life, and other adverse outcomes (Arnold et al., 2020; Joseph et al., 2019). The backbone of its diagnosis is the clinical interview (Marshall et al., 2021; Sibley et al., 2017). Data from other sources, however, are routinely incorporated in the process, with Continuous Performance Tests (CPTs) ubiquitous in assessing relevant cognitive functions (Hall et al., 2016; Marshall et al., 2021; Shumaker & Hoyt, 2020). These tests assess the ability to respond to a target while inhibiting responses to non-targets (distractors), providing information regarding attentional lapses, impulsivity, and changes in performance over time (Hall et al., 2016). Their validity, however, is jeopardized by examinees who feign cognitive impairment.
The feigning of ADHD-associated cognitive impairment can stem from a myriad of external incentives, including procurement of academic accommodations and stimulants (Faraone et al., 2020; Harrison et al., 2021). It is a major clinical concern, with rates estimated to be as high as 50% in higher-education settings and, importantly, scant empirically validated techniques for its detection (Bordoff, 2017; Harrison et al., 2021; Sagar et al., 2017). Clinical judgment is inadequate for this purpose (Dandachi-FitzGerald et al., 2017; Guilmette, 2013) and most ADHD self-report scales do not include validity indicators (Marshall et al., 2021). Clinicians consequently mainly rely on standalone Performance Validity Tests (PVTs), tests constructed specifically for the detection of noncredible performance (Larrabee, 2012), and embedded validity indicators. The latter are derived from cognitive tests that are routinely used during assessment, with extremely poor performance indicative of feigning (Rickards et al., 2018). As CPTs are frequently used is the context of ADHD diagnosis, establishing embedded validity indicators for them is of clear importance. In addition, their use will not increase the evaluation’s duration, in contrast to the incorporation of standalone PVTs. A recent review (Harrison et al., 2021), however, concludes that although ADHD simulators perform worse than genuine patients on several CPTs, cutoffs of traditional measures were associated, at maximum, with moderate sensitivity levels (see, also, Nicholls et al., 2020; Scimeca et al., 2021).
Eye-movements highlight areas attracting the participant’s attention and thereby enhance our understanding of cognitive processes that are employed as the participant engages with a task (Duchowski, 2017; Klein & Ettinger, 2019). Commonly collected measures include those of fixations, periods during which the eyes come to rest and information is processed, and saccades (Holmqvist & Andersson, 2017, chs. 13–16; Klein & Ettinger, 2019, chs. 2–3). The latter are ballistic eye-movements that enable the eyes to move rapidly between fixations. Such eye-movement measures can be gathered in conjunction with specific areas of interest (AOIs), predefined regions of the participant’s field of view. This is of importance in the context of ADHD, as CPTs have a fixed AOI that displays targets/non-targets. Any gaze deviations from this central AOI can therefore only impair performance, making CPTs particularly amendable for integration with an eye-tracker. Intial studies indicated the utility of eye-movements, gathered while participants performed a CPT, to differentiate ADHD patients and healthy controls (Elbaum et al., 2020; Lev et al., 2020). Moreover, eye-movements are associated with deception (Gamer & Pertzov, 2018) and, importantly, the feigning of cognitive impairment. For example, simulators in Mahoney et al. (2018) had lower overall accuracy compared to controls in a forced-choice memory-recognition task, while gazing disproportionately at stimuli that they were presented with earlier (see also, Kanser et al., 2020; Patrick et al., 2021; Tomer et al., 2020). These studies, however, are numbered and we are aware of only one study that investigated the potential of a CPT integrated eye-tracker (Barry & Ettenhofer, 2016). In this study, healthy simulators had higher saccadic variability and made more saccadic commission errors than presumably honest healthy controls and mild traumatic brain injury (TBI) patients. Gaze direction, however, was not analyzed as part of the study and the CPT that was used is not commercially available. Barry and Ettenhofer (2016) also did not assess ADHD patients, the most relevant diagnosis for CPT use in clinical practice (Hall et al., 2016; Marshall et al., 2021; Shumaker & Hoyt, 2020), further decreasing the practical implications of the study.
The MOXO-dCPT is a widely used and researched computerized CPT (for recent publications, see; Ben-Sheetrit et al., 2021; Dobrakowski & Łebecka, 2020; Peled et al., 2020; Slobodin & Davidovitch, 2019; Slobodin et al., 2020). Importantly, it contains dynamic visual and auditory distractors (e.g., a barking dog) which better simulate real life environments (i.e., promise to enhance ecological validity). This, as well the MOXO-dCPT’s use of an online platform that does not require special equipment, are strengths which make it of particular interest. The goal of the current study was to investigate, for the first time, the utility of integrating a commercially available CPT (i.e., MOXO-dCPT) with an eye tracker for the purpose of detecting feigned cognitive impairment. To achieve this aim, we analyzed the eye-movements of simulators (i.e., healthy participants simulating impairment) and ADHD patients. Healthy controls were also assessed, providing an additional comparison of interest. We hypothesized that simulators would gaze significantly less time at the center of the screen (i.e., location of target/non-targets) than ADHD patients. This corresponds to a strategy of feigned inattentiveness which was noted in earlier studies (e.g., Goebel, 1983; Jones, 2017; Kanser et al., 2017) and the tendency of TBI simulators to gaze at irrelevant stimuli when performing forced-choice recognition memory-based PVTs (Kanser et al., 2020; Tomer et al., 2020).
Method
Participants
Inclusion criteria were: (a) 18 to 65 years of age. (b) ADHD patients: Current diagnosis of ADHD (314.0x according to the Diagnostic and Statistical Manual of Mental Disorders-5, DSM-5; American Psychiatric Association, 2013), established using the Structured Clinical Interview for DSM-5 (SCID-5-RV; First et al., 2015) and conducted by a trained clinician upon study entry. Participants also had to provide documentation of a previous (i.e., ≤5 years and ≥18 years) ADHD diagnosis made by a licensed clinician. Exclusion criteria were: (a) Significant past or present neuro-psychiatric disorders (evident, e.g., in psychiatric inpatient hospitalization and past suicide attempts) or developmental disorders (e.g., dyslexia). Participants with personality disorders were not excluded from the study and a diagnosis of ADHD was not an exclusion criterion for participants in the ADHD patient group. (b) Eye impairment (e.g., limited visual field, nystagmus, astigmatism [cylinder], strabismus), past strabismus, and refractive surgery. ADHD patients were requested to refrain from taking stimulants >12 hours before the start of the experiment.
Of the study’s initial sample (N = 111), two participants disclosed information at the end of the experiment that raised suspicion of a learning disability and three participants reported insufficient motivation to adhere to the experimental instructions in the debriefing survey (<4 on a Likert scale that ranged from 0 to 7). The data of these participants were excluded from analyses (final N = 106). The study was approved by the institutional review board (IRB) committee. All participants signed a written informed consent form and received course credit for participating in the study.
Materials
MOXO-dCPT: An online computerized CPT with eight stages (duration = 18.7 minutes). Each stage consists of 60 trials in which stimuli (target or non-target) are presented, followed by an inter-stimulus interval (ISI) of the same duration. Participants are requested to press the spacebar once as quickly as possible in response to targets and to refrain from pressing it when presented with non-targets. Two of the MOXO-dCPT stages are without distractors, while the others include visual distractors, auditory distractors, or a combination of both visual and auditory distractors. Four indices serve as outcome measures: (a) Attentiveness: Responses made during target presentations or the ISI following them. (b) Timeliness: Responses made during target presentations. (c) Impulsivity: Responses made during non-target presentations (i.e., commission errors). (d) Hyperactivity: Commission responses that were not coded as impulsive.
Self-report questionnaires: (a) Adult ADHD Self-Repot Scale (ASRS; Kessler et al., 2007): The ASRS assesses adult ADHD symptoms. It includes 18 items, representing ADHD symptoms listed in the DSM-5 (American Psychiatric Association, 2013). Items are rated on a 5-point Likert scale from 0 (never) to 4 (very often). (b) Wender Utah Rating Scale (WURS; Ward et al., 1993): The WURS retrospectively assesses the presence and severity of childhood ADHD symptoms. It includes 25 items, each rated on a 5-point Likert scale from 0 (not at all) to 4 (a lot).
Word Memory Test (WMT; Green & Astner, 1994; Green et al., 1996): A well-established computerized standalone PVT (Armistead-Jehle et al., 2021; Schroeder & Martin, 2021; Stevens & Licha, 2019). As part of the current study, participants were requested to memorize a list of noun pairs. After presenting the list twice, a forced-choice test was performed in which they identified the previously presented nouns out of target-foil pairs. Thirty-minutes after performing the first subtest (Immediate Recognition, IR), participants performed the Delayed Recognition (DR) subtest which includes only a forced-choice test. Feedback regarding the accuracy of responses was provided in both the IR and DR subtests. IR-score and DR-score (% correct responses in each subtest), as well as a consistency score (CNS; measure of consistency in performing the subtests), were used to classify participants in accordance with the WMT’s manual (Green, 2005).
Eye Tracking System and Selected Eye-Movement Measure
Eye-movements were recorded at a sampling rate of 250 Hz (resolution: noise limited at <0.01°) by means of the EyeLink 1000 system (http://www.sr-research.com). The eye-tracking system uses two separate computers: (a) A host PC which performs real-time eye-tracking and computes the participant’s true gaze position. (b) A display PC that displays targets during the calibration process and experimental stimuli. The stimuli were presented on an Alienware OptX 23″ display screen with 1920 × 1080 resolution with eye-to-screen viewing distance of approximately 60 cm. Black curtains were placed behind the computer screen to minimize distractions and the room was noise isolated.
As detailed in Elbaum et al. (2020), the participants’ field of view was divided into two AOIs; areas in which the MOXO-dCPT stimuli (targets and non-targets) are presented and areas outside of the task AOI (target AOI and distractibility AOI, respectively). An eye-movement distractibility scale (%) operationalized the extent to which the participant’s visual attention was directed toward AOIs that are irrelevant for successful MOXO-dCPT performance (i.e., proportion of time spent gazing at the distractibility AOI). See Figure 1.
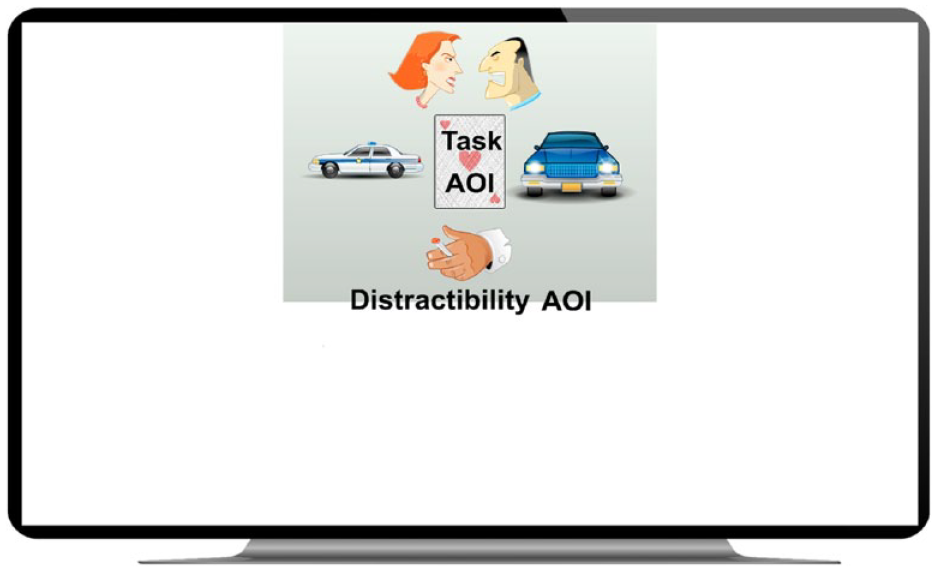
Participants’ FOV while performing the MOXO-dCPT.
Procedure
Participants were requested to remove eye mascara before the start of the experiment to ensure the reliability of the eye-tracking and filled questionnaires (demographic-medical, ASRS, and WURS). ADHD patients also underwent the SCID-5-RV. Healthy participants were randomized to one of two conditions: (A) Simulators: Participants read a script in which they were requested to play the part of an undergraduate student who attempts to procure academic accommodations by feigning ADHD. (b) Honest controls: Participants were requested to perform the tasks to the best of their ability. Comprehension of the experimental instructions was assessed by the research team using open-ended questions and a questionnaire that included three forced-choice items. Any misunderstandings were clarified, and participants were notified that they are eligible for an additional course credit which would be voided if they were found to have exerted insufficient effort (healthy controls and ADHD patients) or their performance was deemed overly exaggerated (simulators). In actuality, all participants received the course credit at the end of the study. They then performed the WMT’s IR-subtest and underwent a calibration procedure to ensure the eye-tracker’s measurement precision (between 7 and 20 minutes). Finally, they performed the MOXO-dCPT, the WMT’s DR-subtest, and filled a debriefing survey inquiring about their motivation to follow the experimental instructions. ADHD patients also filled a brief questionnaire inquiring whether they feigned impairment when originally diagnosed (for additional information, see Berger et al., 2021).
Data Analysis
Group comparisons and general remarks
The groups were compared in demographic, clinical (ASRS and WURS), performance validity (WMT), and the eye-movement distractibility scale using analyses of variance (ANOVAs) and chi-square analyses (for parametric and nonparametric variables, respectively). A multivariate ANOVA (MANOVA) was used to compare the groups in the MOXO-dCPT indices (attentiveness, timeliness, impulsivity, hyperactivity). Density heat-maps, based on groups’ aggregated durations of fixations, were then created using the Data-Viewer software (SR Research Ltd) with parameter settings like those used in Elbaum et al. (2020). Analyses were conducted using IBM SPSS version 26, with two-tailed p < .05 considered statistically significant.
Classification accuracy: ROC curve analyses (simulators vs
ADHD patients) and criteria for choosing suitable cutoffs.
Discrimination capacities of the eye-movement distractibility scale were analyzed using receiver operating characteristic (ROC) curves. Areas under the curve (AUC) were qualitatively interpreted based on Hosmer et al. (2013, p. 177); poor (0.5 < AUC < 0.7), acceptable (0.7 ≤ AUC < 0.8), excellent (0.8 ≤ AUC < 0.9), and outstanding (≥0.9). Next, we focused on the comparison of interest (i.e., simulators and ADHD patients) and selected cutoffs that maintain ≥ 90% specificity (in accordance with established conventions; Sherman et al., 2020, p. 12; Sweet et al., 2021).
Utility of conjunctive and disjunctive rules to detect feigned ADHD-associated cognitive impairment
Berger et al. (2021) created a scale, termed feigned ADHD scale which integrates the contributions of traditional MOXO-dCPT indices to detect feigning. As part of the current study, we assessed the utility of a scale to differentiate the simulators and genuine ADHD patients. This was done using the first cutoff with >90% specificity (0.610, see Table 3 “Classification Accuracy of MOXO-d-CPT Indices and the Combined Feigned Cognitive Impairment Scale, Based on Prospective Analyses of Simulators and ADHD Patients (Study 1).” in Berger et al. 2021). This cutoff was then used to assess the utility of decision rules for the detection of feigned ADHD-associated cognitive impairment. More specifically, we assessed conjunctive (i.e., determination of feigning requiring failure in both validity indicators) and disjunctive (i.e., failure in one measure is sufficient for determining feigning) decision rules based on the eye-movement distractibility scale and feigned ADHD scale. As the current study’s sample and that of Berger et al. (2021) overlap, utility estimates for the feigned ADHD scale and decision rules were calculated on data of non-overlapping participants (n = 21 simulators, n = 18 ADHD patients, n = 18 healthy controls).
Exploratory analyses
Group comparisons were performed on gaze-shifts, the number of times the participant crossed the target AOI’s border, using an ANOVA. This exploratory analysis examined the behavioral profile of simulators (i.e., whether they simply disengaged from the task by gazing at the surrounding environment). We then calculated the ROC curve of the eye-movement distractibility scale based on data of simulators and healthy controls. Finally, we performed Pearson correlations between MOXO-dCPT outcome measures (eye-movement measures and indices).
Results
Group Comparisons
There were significant group differences in the eye-movement distractibility scale (p < .001). Post hoc Scheffe tests revealed that simulators gazed significantly more time outside the target AOI (i.e., location of target and non-targets) than ADHD patients and healthy controls (p = .001, p = .002; respectively). Differences between ADHD patients and controls were not significant. See Tables 1 and 2. Density heat maps are presented in Figure 2.
Descriptive Statistics and Statistical Analyses of Demographic Measures According to Experimental Group: Simulators (n = 37), ADHD Patients (n = 33), and Healthy Controls (n = 36).
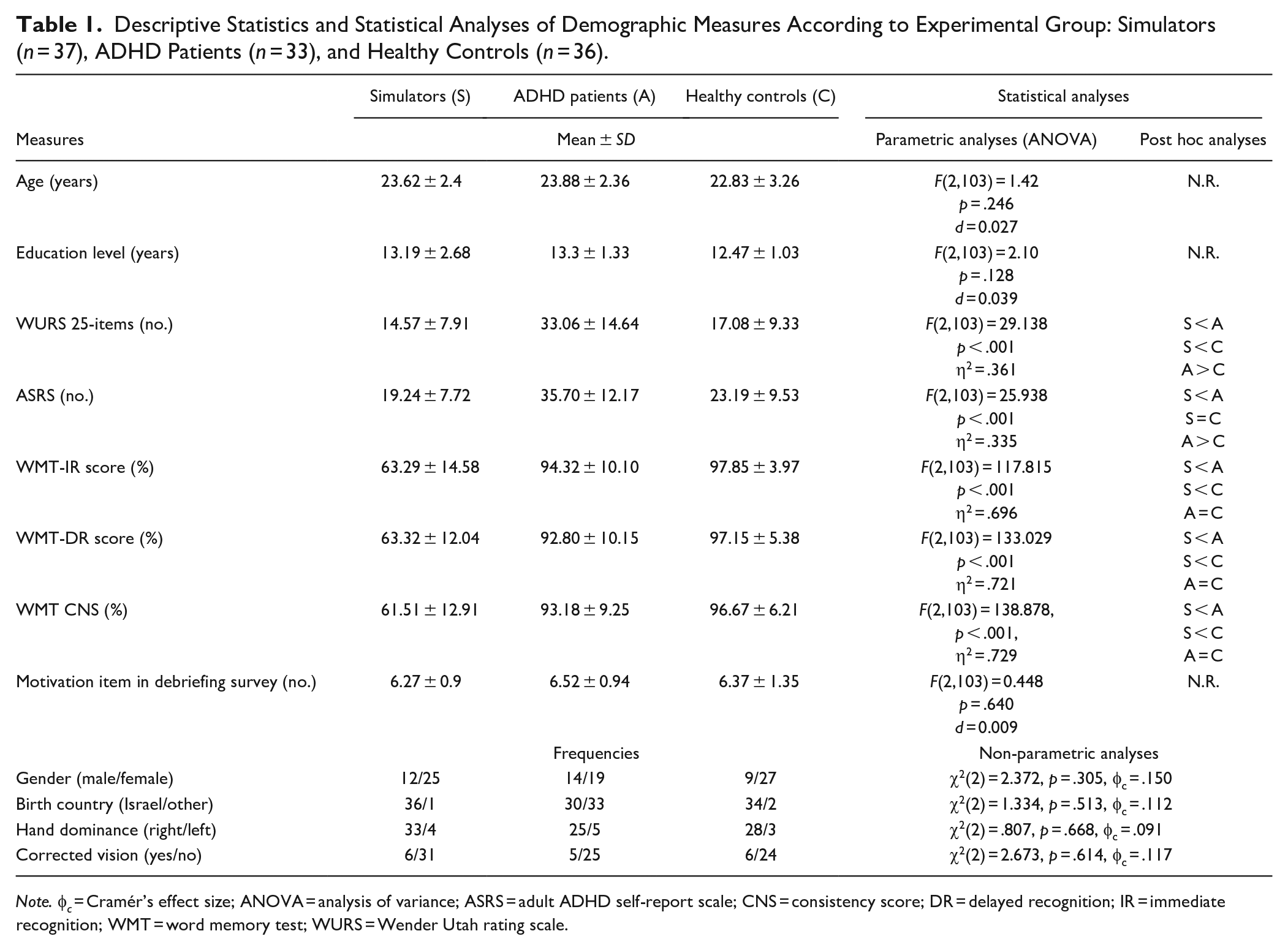
Note. φ c = Cramér’s effect size; ANOVA = analysis of variance; ASRS = adult ADHD self-report scale; CNS = consistency score; DR = delayed recognition; IR = immediate recognition; WMT = word memory test; WURS = Wender Utah rating scale.
Descriptive Statistics and Statistical Analyses of MOXO-dCPT Outcome Measures (i.e., Indices and Eye Movement Measures) According to Experimental Group: Simulators (n = 37), ADHD patients (n = 33), and healthy controls (n = 36).
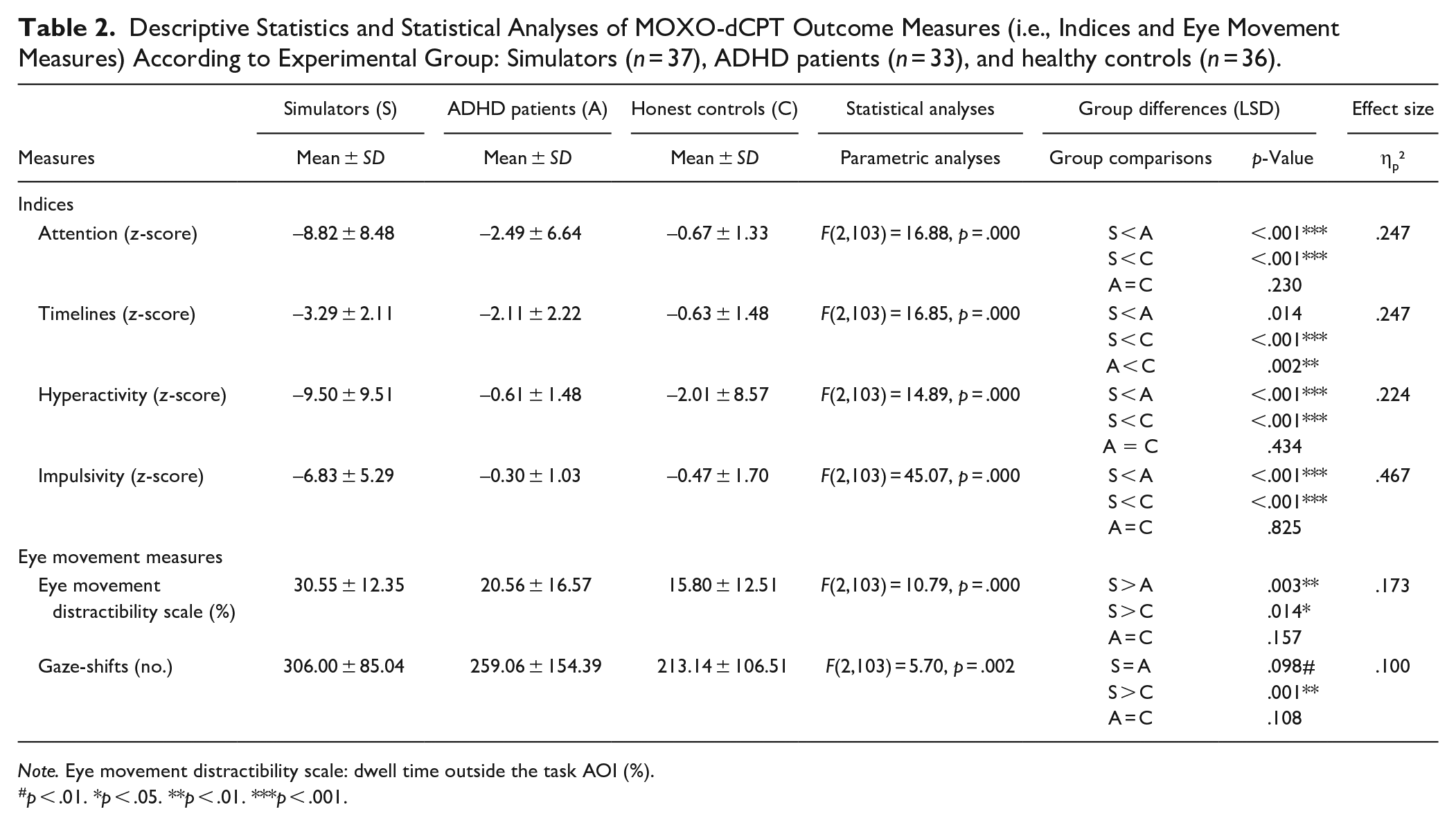
Note. Eye movement distractibility scale: dwell time outside the task AOI (%).
p < .01. *p < .05. **p < .01. ***p < .001.

Fixation duration heat maps according to experimental group: (A) Simulators. (B) ADHD patients. (C) Healthy controls.
Classification Accuracy: Discriminating Between Simulators and ADHD Patients
The ability of the eye-movement distractibility scale to discriminate simulators and ADHD patients was acceptable (AUC = 0.708, p = .003, CI: 0.580–0.836). Cutoffs ≥43.10% were associated with adequate specificities (i.e., ≥90%). Their sensitivities, however, were low. For example, a 43.10% cutoff was associated with 90.9% specificity and 18.9% sensitivity (PPP range: 34.2%–67.5%, NPP range: 21.9%–52.9%). The highest specificity that could be reached was 97.0% (cutoff = 57.35%). However, it was associated with negligible sensitivity (2.7%). Utility estimates for a range of cutoffs are presented in Appendix 2.
Utility of Conjunctive and Disjunctive Rules to Detect Feigned ADHD-Associated Cognitive Impairment
The use of the feigned ADHD scale’s 0.610 cutoff was associated with 94.4% specificity among both ADHD patients and controls, while sensitivity was excellent (81.0%). A conjunctive (“and”) decision rule based on the eye-movement distractibility scale and feigned ADHD scale was associated with 94.4% specificity among ADHD patients and 100% specificity among healthy controls. Sensitivity, however, was low (i.e., 14.3%). In contrast, a disjunctive (“or”) decision rule was associated with 83.3% specificity among ADHD patients and 88.9% specificity among healthy controls. Sensitivity was excellent (i.e., 90.5%).
Exploratory Analyses
Simulators and ADHD patients did not differ significantly in gaze-shifts (p = .098). Simulators, however, did cross the division between the center of the screen and areas outside of it significantly more time than healthy controls (p = .001). Differences between ADHD patients and controls were not significant. ROC curves derived from data of simulators and healthy controls indicated excellent discrimination capacity of the eye-movement distractibility scale (AUC = 0.832, p < 0.001, CI: 0.736–0.928). Finally, the correlation between the eye-movement distractibility scale and gaze-shifts was strong (r = .77), while those with the conventional MOXO-dCPT indices ranged between −.29 and −.54 (with timelines index). In other words, participants that spent more time gazing outside of the screen’s center tended to cross its border more times and to perform more poorly in traditional indices of the MOXO-dCPT. Correlations of the eye-movement distractibility scale and WMT’s validity indicators were all significant, mostly in the medium to strong effects size range (Cohen, 1992). The strongest correlation with traditional MOXO-dCPT indices was with impulsivity (r = .71). See Appendix 2 for the coefficient matrix.
Discussion
Simulators gazed significantly more time than ADHD patients outside of the computer screen’s center (i.e., had higher scores in the eye-movement distractibility scale). In other words, they spent a larger proportion of time gazing at screen regions in which distractors were presented, blank screen regions, and regions that were altogether outside of the border of the screen (see Figure 2 for a graphical presentation). This finding is of importance as the center of the screen is the only region in the participants’ field of view which contains information that is relevant for success in the MOXO-dCPT, as in most CPTs. The scale was also significantly correlated with the outcome measures of the WMT, a well-established PVT (Armistead-Jehle et al., 2021; Schroeder & Martin, 2021; Stevens & Licha, 2019), an additional indication of its potential as an embedded validity indicator. Establishing clinical utility, however, necessitates more than significant group differences and initial evidence of convergent validity. Rather, it mandates more thorough analyses of discrimination capacity and these lead to more qualified conclusions in this case. The eye-movement distractibility scale had acceptable capacity in differentiating simulators and ADHD patients (AUC in ROC curve analysis = 0.708), manifested in cutoffs that were associated with low sensitivity levels. For example, a 43.1% eye-movement distractibility scale cutoff (i.e., >43.1% of time spent gazing at irrelevant AOIs) was associated with 90.9% specificity and 18.9% sensitivity. Though we can be fairly confident that cognitive impairment is being feigned when examinees fail such a cutoff, concluding that their performance is credible when they pass it is problematic (for qualitative interpretation guidelines of sensitivity levels, see Boone, 2013, p. 32). This is not particularly surprising as ADHD patients in the current study exhibited an eye-movement profile that is intermediate between that of simulators and healthy controls. Such a feigning profile (i.e., exaggerating deviations of neuropsychiatric patients) enables easy discrimination between simulators and controls (note the excellent discrimination capacity of the eye-movement distractibility scale between simulators and healthy controls; AUC = 0.832). However, this comparison is less clinically important, and we are left with a stand-alone validity indicator that is limited in its ability to “rule in” feigned cognitive impairment.
Combining several validity indicators may enhance overall classification accuracy (Davis, 2021). We therefore investigated the utility of integrating the eye-movement distractibility scale and traditional MOXO-dCPT indices (i.e., a scale which integrates the indices, termed “feigned ADHD scale”; Berger et al., 2021). This was done using disjunctive (i.e., requiring failure in at least one of the scales) and conjunctive (i.e., requiring failure in both scales) decision rules. The first was associated with excellent sensitivity (i.e., 90.5%) and specificities of 83.3% and 88.9% (ADHD patients and healthy controls, respectively), while the latter achieved adequate specificities (i.e., > 90%) though its sensitivity was low (i.e., 14.3%). In other words, these decision rules were associated with either inadequate specificity (<90%; Sherman et al., 2020, p. 12; Sweet et al., 2021) or low sensitivity. As the use of the feigned ADHD scale (i.e., a feigning scale based on traditional MOXO-dCPT indices) was associated with excellent utility estimates (i.e., 94.4% specificity among ADHD patients and 81.0% sensitivity), there does not seem to be an incentive to use any of the beforementioned decision rules. Though not the focus of the current study, this latter finding also provides initial validation of the feigned ADHD scale. This is encouraging, as traditional CPT indices with adequate specificities tend to be associated with only moderate sensitivities, up to 63% (see review; Harrison et al., 2021, p. 547).
Comparison with earlier studies is challenging as they are numbered and differ from the current one in key aspects, including selected outcome measures and research designs (e.g., simulation studies vs. studies in which real-life examinees are divided according to assumed credibility). Only one study integrated an eye tracker with a CPT (Barry & Ettenhofer, 2016). However, the CPT that was utilized is not available commercially, ADHD patients were not assessed, and spatial eye-movement measures (i.e., gaze location) were not analyzed as part of the study (Barry & Ettenhofer, 2016). Measures of spatial attention were assessed in two studies, though comparisons with the current study’s findings are still challenging. In the first study, healthy simulators spent more time looking at correct and incorrect response options when performing the Warrington Recognition Memory Test of Words (RMT-Words) than presumably honest TBI patients and healthy controls (Kanser et al., 2020). Notably, eye-movement measures exceeded accuracy in differentiating the groups, adding incremental predictive value to the accuracy-based validity indicator (Kanser et al., 2020). In the second study, healthy participants simulating TBI spent more time than controls gazing at irrelevant stimuli when performing the WMT (Tomer et al., 2020). These studies provide some support for the tendency of simulators to gaze at irrelevant stimuli. Forced-choice recognition memory-based PVTs (Schroeder & Martin, 2021), however, were used in both studies, rather than CPTs. Reaching overarching conclusions at present is therefore difficult to reach, emphasizing the need for further research focusing on CPT performance.
Theory-wise, we lack understanding regarding the sources of the observed eye-movement profile of simulators. On the one hand, it may indicate an intentional feigning strategy of inattentiveness (i.e., gazing at areas that are irrelevant for success in the task). Ignoring stimuli was mentioned in post-test interviews as a feigning strategy in Goebel (1983) and more recent studies note feigning strategies such as “showing attention and concentration difficulties” (Jones, 2017) and “acting inattentive/distractible” (endorsed by 24.1% of the simulators in Kanser et al., 2017). These studies therefore suggest that simulators may adopt a strategy of inattentiveness that, though speculative at present, may lead them to avert gaze from the center of the screen when performing the MOXO-dCPT. Group differences, however, may be driven by unintentional cognitive processes. At least certain aspects of ocular behavior are relatively free of conscious control (e.g., early trajectory of eye movements; Theeuwes et al., 1998) and we can also speculate that the cognitively demanding nature of deception (Giolla & Luke, 2021; Vrij et al., 2017; Walczyk et al., 2018, pp. 6–8) may impact eye-movements (for links between increased cognitive load and eye behavior, see Eckstein et al., 2017; Skaramagkas et al., 2021; van Gog et al., 2009, pp. 327–328). Regrettably, exploring these options (intentional vs. unintentional sources of eye-movement behavioral patterns) is hindered by the fact that simulators were not required to note strategy use in the debriefing survey of the current study. Finally, simulators may have simply disengaged from the task. It should, however, be noted that the simulators also crossed the border between the target AOI and areas outside of it significantly more times than honest controls (see “gaze-shifts” measure in Table 2). It is therefore less likely that they simply disengaged from the task. Also note the lack of differences in stated motivations to follow the experimental instructions (see Table 1) which supports this conclusion.
Limitations and Venues for Future Research
The current study’s strengths include its novelty, as well as the inclusion of ADHD patients who anonymously disclosed whether they feigned the disorder in the past. The study’s primary limitation concerns its research design. Simulation studies allow researchers to manipulate key variables and consequently have high internal validity. They can also be easily implemented. However, differences in both positive and negative incentives between simulators and examinees who feign ADHD in clinical practice may lead to differences in task performance (Rogers, 2018; Schroeder et al., 2021). In addition, ADHD patients in the current study were university undergraduate students. Though a relevant population in the context of feigned ADHD, these are highly functioning patients. Both factors likely limit the generalization of findings to real-life clinical settings. Inclusion of examinees undergoing assessments in clinical practice is therefore advised in future studies (researchers are advised to consult the relevant literature; Rogers, 2018; Schroeder et al., 2021). Several additional lines of research can be suggested. First, researchers are encouraged to further explore the integration of traditional CPT measures and eye-movement-based validity indicators (as long as the validity indicators do not overlap excessively, this may enhance their sensitivity; Sherman et al., 2020, p. 748). Second, additional eye-movement measures can be explored, including pupillometry (i.e., pupil size analyses) which showed potential when assessed during the performance of the test of memory malingering, TOMM, an established forced-choice memory-based PVT (Patrick et al., 2021). Third, sources of eye-movement patterns (i.e., intentional vs. unintentional effects) can be further explored through post-experimental debriefing surveys and other psychophysiological measures (e.g., use of pupil dilation as a marker of cognitive load; Patrick et al., 2021). Finally, there is room to investigate the utility of the MOXO-dCPT in detecting feigned cognitive impairment in other neuropsychiatric disorders.
Summary
The current study provides initial support for the feasibility of integrating an eye tracker with a commercially available CPT for the detection of feigned cognitive impairment. As hypothesized, simulators spent significantly more time gazing at irrelevant areas for success in the MOXO-dCPT compared to both ADHD patients and healthy controls. This provides initial support for the use of spatial eye-movement in the context of feigned CPT performance, in lieu of recent studies attesting to their usefulness in other neuropsychiatric disorders (Smyrnis et al., 2019; Tao et al., 2020). From a clinical vantage point, the sensitivity of the eye-movement distractibility scale was low. Passing such a validity indictor is therefore insufficient evidence that the examinee performed the MOXO-dCPT to the best of their ability. Stronger support in this regard was found for a scale that integrates the contribution of traditional MOXO-dCPT indices, validating earlier findings (Berger et al., 2021). Further research, however, is needed and may shed light on theoretical issues (e.g., intentional vs. unintentional factors impacting simulators’ eye-movements), as well as the utility of additional eye-movement measures. Technological advances are expected to lower the cost and enhance the usability of eye trackers in the near future (e.g., Ivanchenko et al., 2021), an additional incentive to conduct such research.
Supplemental Material
sj-docx-1-jad-10.1177_10870547211063643 – Supplemental material for Feigned ADHD Associated Cognitive Impairment: Utility of Integrating an Eye-trAcker and the MOXO-dCPT
Supplemental material, sj-docx-1-jad-10.1177_10870547211063643 for Feigned ADHD Associated Cognitive Impairment: Utility of Integrating an Eye-trAcker and the MOXO-dCPT by Astar Lev, Tomer Elbaum, Corinne Berger and Yoram Braw in Journal of Attention Disorders
Supplemental Material
sj-docx-2-jad-10.1177_10870547211063643 – Supplemental material for Feigned ADHD Associated Cognitive Impairment: Utility of Integrating an Eye-trAcker and the MOXO-dCPT
Supplemental material, sj-docx-2-jad-10.1177_10870547211063643 for Feigned ADHD Associated Cognitive Impairment: Utility of Integrating an Eye-trAcker and the MOXO-dCPT by Astar Lev, Tomer Elbaum, Corinne Berger and Yoram Braw in Journal of Attention Disorders
Footnotes
Acknowledgements
The research reported in this paper was completed as part of the first author’s (A.L.) MA dissertation (Bar-Ilan University, Ramat Gan, Israel), the second and third authors’ (T.E. and C.B.) PhD dissertation (Ariel University, Ariel, Israel), and the undergraduate program requirements of Adi Narov, Adi Zafris, Amit Yarkoni, Eden Katzav, Ela Drookman, Michal Shisha, Sean Shachar, and Tzoor Cohen. We thank them for their invaluable contribution to the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Neurotech Solutions, the publishers of the MOXO-d-CPT, permitted the researchers to use the MOXO-d-CPT free of charge for the duration of the study and for the purpose of the described study.
Supplemental material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.