
Abstract
Objective:
To test whether parental factors including internalizing symptoms, parenting style, and confidence in assisting with remote learning conferred risk/resilience for children with/without ADHD’s learning and emotional outcomes during the COVID-19 pandemic.
Method:
291 parents of children (ages 6–13; n = 180 males) with (n = 148) and without ADHD completed questionnaires online (April–July 2020).
Results:
Structural equation modeling identified parental risk/resilience factors. Across groups, risk predicted greater difficulties with learning, internalizing and externalizing symptoms, while parent confidence in educating their child predicted better outcomes. A positive association was observed between parental involvement and child difficulties, which was stronger in families of children with ADHD. Children with/without ADHD did not differ in remote learning difficulties.
Conclusion:
Parent factors impacted child emotional and learning outcomes during the pandemic. With increases in remote learning practices, there is a need for improved understanding of how parent factors impact outcomes of children with/without ADHD.
Introduction
In 2020, government-imposed social distancing and quarantine measures associated with the SARS CoV-2 virus (COVID-19) pandemic, including shifts from in-person schools to remote learning, had a significant impact on daily life across the globe (Mækelæ et al., 2020). Families were particularly impacted by remote learning mandates as parents who needed to juggle their new role as teacher with work and other responsibilities reported an increase in their stress levels (Kowal et al., 2020). These effects were exacerbated for parents of youth with neurodevelopmental disorders, such as ADHD (Leitch et al., 2019) who exhibited worsening symptoms following COVID-19-related changes (Bobo et al., 2020; Breaux et al., 2021; Melegari et al., 2021; Sciberras et al., 2022; Swansburg et al., 2021; Wendel et al., 2020; Zhang, Shuai et al., 2020), and had more difficulty adapting to remote learning than youth without ADHD (Becker, Breaux et al., 2020). Several parent characteristics have been associated with behavioral and academic difficulties of ADHD children during the pandemic. These include balancing work and school responsibilities (Roy et al., 2021), parental mood (Zhang, Shuai et al., 2020), psychopathology (McFayden et al., 2021), and parents’ confidence in their ability to teach their children at home (Becker, Breaux et al., 2020). As parents played a pivotal role in their children’s education during the pandemic, a reality that is quite possible to occur again in the future, it is particularly important to consider what parental factors may confer risk or protection for psychological and academic outcomes among elementary-aged children with and without ADHD during remote learning. The present study aims to address this important issue.
Several previous studies have highlighted the challenges faced by children and adolescents with ADHD when they shifted to remote learning during the COVID-19 pandemic. For example, during remote learning, school-based services which students with ADHD often rely on (DuPaul et al., 2019) such as therapy/counseling, modified assignments, speech or physical therapy, and individualized tutoring, were frequently reduced, or not offered at all (Bobo et al., 2020; McFayden et al., 2021). As a result, parents of adolescents with ADHD who had mandated accommodations through an Individualized Education Plan (IEP) or Section 504 plan were more likely to indicate that the shift to remote learning was very challenging, as compared to parents of adolescents with ADHD without formal school accommodations (Becker, Breaux et al., 2020). In addition to decreased efficacy of school accommodations, recent work in adolescents and young adults (ages 13–22) with ADHD found that difficulty engaging in remote learning was one of the most prominent difficulties during the pandemic, a problem reported by both parents and youth, alike (Sibley et al., 2021). This may have been exacerbated by the fact that during remote learning, children were receiving significantly less teacher-led instructional time (Becker, Breaux et al., 2020; Bobo et al., 2020; McFayden et al., 2021; Roy et al., 2021).
In addition to school difficulties, children with ADHD also often exhibit comorbid social challenges (Hoza, 2007; Mikami, 2010; Normand et al., 2013), emotion dysregulation (Faraone et al., 2019; Lugo-Candelas et al., 2017), and anxiety (Armstrong et al., 2015; Sciberras et al., 2014). Given the myriad of co-occurring difficulties associated with ADHD, it is not a surprise that these in addition to academic challenges, children with ADHD exhibited exacerbated symptoms of sadness, loneliness and anxiety (Sciberras et al., 2022), as well as conduct symptoms (Nonweiler et al., 2020) in the context of the pandemic. Recent longitudinal research found that, among adolescents with ADHD, those who demonstrated the most difficulty with emotion regulation prior to COVID-19 were at the highest risk for experiencing anxiety, depression, and increased symptoms of hyperactivity and impulsivity during the pandemic (Breaux et al., 2021). Moreover, a longitudinal study of 992 children and adolescents with ADHD found that while internalizing and externalizing symptoms occurring less than two times per week prior to the pandemic decreased in frequency during lockdown, symptoms occurring at moderate (three to four times per week) or severe (five to seven times per week) frequencies significantly increased (Melegari et al., 2021). Alternatively, one study of children with ADHD living in France found that one-third of children in their sample experienced decreased well-being, while an additional third exhibited no change and the last third reported symptom improvement (Bobo et al., 2020). Thus, while the majority of studies demonstrate increased difficulties for youth with ADHD during remote learning, this finding is not consistent, suggesting that there may be factors, including parent characteristics, that impacted such outcomes.
Given the necessary roles that parents played in remote learning during the pandemic, it is important to consider parent factors, such as psychopathology, stress, parenting style, and parent confidence in their ability to support remote learning, that might have contributed to child outcomes. An emergent literature indicates that parents generally experienced heightened symptoms of psychopathology and stress during the COVID-19 pandemic and that these difficulties impacted child psychological well-being (Chafouleas & Iovino, 2021; Cusinato et al., 2020; Lee et al., 2021). For example, Lee et al. (2021) found that among 654 parents, 40% met criteria for a major depressive episode and that these parents reported feeling less well prepared to help with their children’s education at home than those who were not depressed (Lee et al., 2021). Moreover, greater parenting stress and general stress during the pandemic predicted greater inattention/hyperactivity, conduct problems, and emotional difficulties among youth ages 2 to 14 years old (Spinelli et al., 2020). Prior to the COVID-19 pandemic, there was strong evidence to suggest that parents of children with ADHD exhibit greater psychopathology (for meta-analysis see Cheung & Theule, 2016) and parenting stress (for meta-analysis see Theule et al., 2013) than parents of typically-developing children. Thus, already heightened symptoms of psychopathology and stress among parents of children with ADHD may have been additionally exacerbated by the circumstances of the pandemic. Consistent with this, in a study across several European countries, approximately 40% of parents endorsed stress related to their children’s education, and stress levels were higher among parents of children with a mental health condition than those without (Thorell et al., 2021). Further, evidence suggests that greater parental psychopathology was associated with more remote learning difficulties during the pandemic among youth with neurodevelopmental disabilities including ADHD (McFayden et al., 2021).
Closely tied to parent stress and psychopathology, parenting style (for review see: Deault, 2010) has also been found to impact outcomes among youth with ADHD prior to the pandemic. Specifically, low parental warmth and negative disciplinary style have been associated with externalizing problems among youth with ADHD (Johnston et al., 2002; Kashdan et al., 2004). One study explored parenting style and child well-being during the pandemic in a community sample via a 3-week daily diary study (Neubauer et al., 2021). A parenting style that supported children’s autonomy (e.g., offering choices, avoiding controlling language, etc.) was associated with greater same-day positive affect and lesser average negative affect among children. Further, greater child positive affect across the 3-week study period was associated with increased prosocial behavior and decreased hyperactivity and emotional problems. The impact of parenting style specifically on children with ADHD during COVID-19 remote learning has yet to be examined.
In a study conducted prior to the pandemic, parents of children with ADHD endorsed lower self-efficacy in relation to helping their children with school and reported having less time and energy to be involved in their children’s education compared to parents of children without ADHD (Rogers et al., 2009). These findings highlight the need to understand how these parents, who may have already felt less effective in regards to their child’s schooling, managed remote learning responsibilities during the pandemic. Interestingly, Becker, Breaux et al. (2020) found that compared to parents of healthy adolescents, parents of adolescents with ADHD endorsed less confidence in managing remote learning and more difficulties supporting remote learning. Greater parent confidence was predictive of fewer remote learning difficulties in both groups, although the association was stronger for the adolescents with ADHD. Thus, while remote learning was difficult for many parents, preliminary evidence suggests that greater parent confidence may have helped minimize remote learning difficulties particularly for adolescents with ADHD.
Overall, remote learning during the COVID-19 pandemic had a clear impact on families, and those with a child with ADHD experienced, poorer outcomes (Becker, Breaux et al., 2020; Bobo et al., 2020; Breaux et al., 2021; McFayden et al., 2021; Melegari et al., 2021; Roy et al., 2021; Sciberras et al., 2022; Wendel et al., 2020; Zhang, Shuai et al., 2020). Prior to the pandemic, parental psychopathology, parental stress, and parenting style, were all shown to impact outcomes among children with ADHD (Cheung & Theule, 2016; Chronis et al., 2007; Johnston et al., 2002; Rogers et al., 2009; Theule et al., 2013). During the COVID-19 pandemic, parents’ symptoms of psychopathology and stress increased (Cusinato et al., 2020; Lee, Ward et al., 2021), particularly for parents of children with mental health conditions (Thorell et al., 2021), parenting style impacted children’s emotional outcomes, and parents of youth with ADHD reported feeling less confident about helping with their child’s schooling (Becker, Breaux et al., 2020). The current study brings these variables together into one model to explore how these facets of parenting may have conferred risk or resilience to emotional and school-related difficulties of children with and without ADHD. Specifically, we hypothesized that parental stress, psychopathology, negative parenting styles, and negative effects of COVID-19 on the family would constitute a risk factor predictive of more child difficulties with remote learning and increased emotional and behavioral problems. We further hypothesized that positive parenting and involvement, parenting efficacy and confidence regarding remote learning, and positive family changes as a result of COVID-19 would represent a resilience factor, predicting fewer child difficulties with remote learning and fewer emotional and behavioral concerns. We then explored how these factors differentially impacted children with and without ADHD, and within the ADHD group, how these factors impacted those with and without school accommodations.
Method
Participants
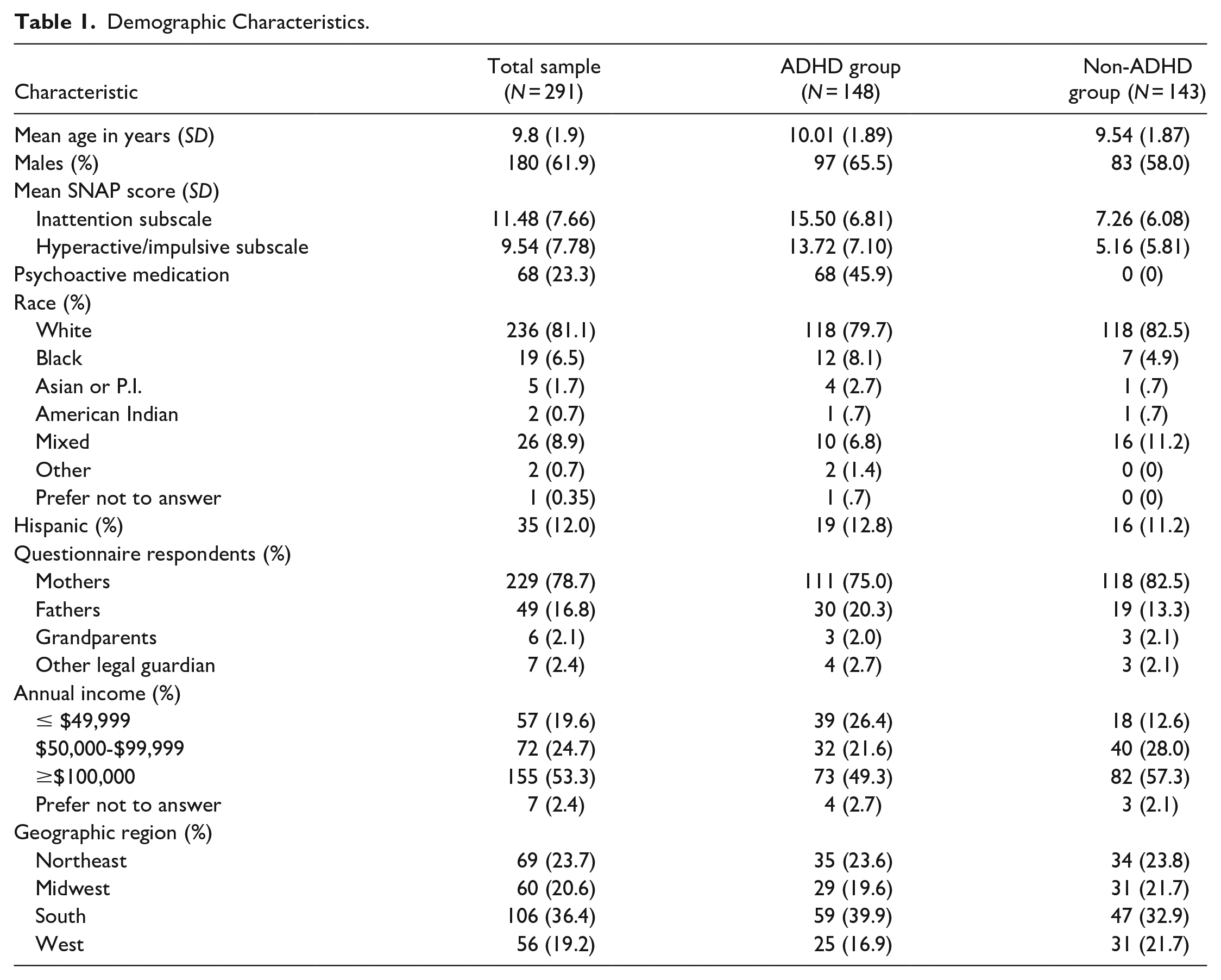
A total of 452 parents signed consent for an online study of parenting school-aged children with or without ADHD during the COVID-19 pandemic. Inclusion criteria included being a fluent, English-speaking parent of a child with ADHD or a child without any diagnosed psychological disorders who was enrolled in first through sixth grade. Forty-four respondents were excluded for failing to meet these criteria, including seven who did not have a child in first through sixth grade, 12 who reported the child’s age as outside the expected age-range for reported grade (i.e., below age 6 or over age 14), and 25 because the child did not have ADHD but were reported to have other psychopathology (e.g., anxiety/mood disorders) excluding them from being in the non-ADHD group. An additional 107 were excluded for having incomplete data precluding us from determining the child’s diagnostic status and/or key demographic information (e.g., sex), 8 people failed at least one of two attention checks, and 2 participants were excluded for duplicate entries (responses from the same IP address). The final remaining sample consisted of 291 parents of children (n = 180 males; 61.9%) in first through sixth grade (ages 6–13 years; M = 9.8; SD = 1.9). The sample was nearly evenly split on ADHD diagnosis status, with 148 parents (51%) reporting that their child had been diagnosed with ADHD by a medical or mental health professional. Among the children with ADHD, 68 (45.9%) reported taking psychoactive medication at the time of the study, 57 (38.5%) reported they were taking psychoactive medication, and these data were missing for 23 children (15.5%). Children were primarily non-Hispanic (n = 256; 88%) and Caucasian (n = 236; 81.1%). Questionnaires were mostly completed by mothers (n = 229; 78.7%) and 53% of families had an annual reported income over $100,000. See Table 1 for detailed demographic information.
Demographic Characteristics.
Procedures
Participants from across the United States were recruited via the internet, including postings on social media (e.g., Facebook), Craigslist, ResearchMatch, and Qualtrics Survey Services between May 20th and July 4th, 2020, during which time social distancing measures and remote learning were in place in most states.
Interested parents completed a brief online screening form to ensure that they met the above inclusion criteria. If eligible, parents proceeded to complete an online consent form. This was followed by a battery of questionnaires that included measures of (1) family variables: demographic information and the impact of COVID-19 on the family, (2) parent variables: their own mental health, parenting style, involvement in their child’s remote schooling, and (3) child variables: ADHD status and school services prior to remote learning and child’s mental health and academic difficulties during the pandemic. If parents had more than one child in the target age range, they were instructed to consider one child while completing the measures. Measures relevant to the current study are described in detail below. Participants who completed the questionnaires were able to opt into a drawing for a $100 Amazon gift card, and for each participant who completed the questionnaires, $1 was donated to a charity that supported children who were impacted by the pandemic. All materials were presented via Qualtrics. The study was approved by the Fordham University Institutional Review Board.
Measures
Parent measures
Family background form
Parents completed study-specific questionnaire that asked for basic demographic information about both the child and the household (e.g., child age, grade level, annual household income, etc.). This measure also asked about the child’s diagnostic status and whether the child received school-based services.
The depression, anxiety, and stress scale (DASS)
The DASS is a 21-item self-report questionnaire that asks about mood, anxiety, and stress symptoms over the past month, with each construct assessed via seven items (Lovibond & Lovibond, 1995). Questions are rated on a 4-point Likert scale from 0 (“does not apply to me at all”) to 3 (“applies to me very much or most of the time”), with higher scores indicating higher levels of distress. The current study utilized the depression, anxiety and stress subscales independently, which had Cronbach’s alphas of .92, .92, and .91, respectively.
Alabama parenting questionnaire (APQ)
Parenting style was measured using the APQ, a 42-item survey that asks questions about the frequency of common parenting practices (Shelton et al., 1996). Items are rated on a 5-point Likert scale from 1 (“never”) to 5 (“always”) and sum into five subscales: involvement, positive parenting, poor monitoring/supervision, inconsistent discipline, corporal punishment. In this study, each subscale was entered into analyses independently; Cronbach’s alphas for the current study ranged from .79 to .95.
Home adjustment to COVID-19 scale—learning at home parent confidence (HACS-Parent Confidence)
Parents’ confidence in their ability to help their children’s schooling at home was assessed via the Learning at Home Parent Confidence subscale of the HACS, a large parent-report inventory of families’ adjustment to the pandemic (Becker, Quach et al., 2020). This subscale is composed of six-items rated on a 4-point Likert scale from 0 (“not at all confident”) to 3 (“very confident”). This subscale had a Cronbach’s alpha of .93 in the current sample.
Parent’s perceptions of self-efficacy for helping the child succeed in school from the parental involvement project (PIP)
Parental efficacy and confidence for teaching children at home was measured using the PIP, an 11-item scale that asks parents to rate how much they agree or disagree with statements regarding their ability to educate their child (e.g., “I know how to help my child do well in school”) (Walker et al., 2005). Questions are rated on a 6-point Likert scale from “disagree very strongly” to “agree very strongly.” All scale items are summed to form a total score, with higher scores indicating higher levels of confidence. Cronbach’s alpha in the current sample was .83.
Parental stress scale (PSS)—adapted for the COVID-19 Pandemic
Parenting stress during the COVID-19 pandemic was assessed via the PSS, which was adapted to instruct parents to report specifically on their experiences during the pandemic (Berry & Jones, 1995). The measure is composed of 18-items rated on a 5-point Likert scale from 1 (“strongly disagree”) to 5 (“strongly agree”). The items are summed to produce a single total score, which had a Cronbach’s alpha of .89 in the current sample.
Epidemic-pandemic impacts inventory (EPII)
Impacts of the COVID-19 pandemic on personal and social life were assessed via the EPII (Grasso et al., 2020). Parents responded to 92 items, indicating whether impacts (e.g., laid off from job) had happened to: “me,” a “person in my home,” or that “no, it did not happen.” For the current study, a score of 2 was assigned if the impact affected both the reporter and a person in their home, a 1 was assigned if the impact affected either the reporter or a person in their home, and a 0 was assigned if no one in the home was affected. Scores on the first 73 items which assessed negative impacts were summed to produce an index of the negative impacts of COVID-19 on the family. Scores on items 74 through 92 were summed as a measure of positive impacts of COVID-19 on the family.
Child measures
Swanson, Nolan, and Pelham-IV 26 item scale (SNAP-IV 26-Item)
Children’s symptoms of ADHD were assessed via the SNAP. Parents responded to 26-items regarding symptoms of inattention, hyperactivity/impulsivity, and oppositionality/defiance on a 4-point Likert scale from 0 (“not at all”) to 3 (“very much”) (Swanson, 1992; Swanson et al., 1983, 2001). The current study utilized the inattention and hyperactivity/impulsivity subscales, which had Cronbach’s alphas of .94 and .93, respectively.
Behavior and feelings survey—parent version (BFSP)
Children’s internalizing and externalizing symptoms over the past month were assessed via the BFSP (Weisz et al., 2020). Parents responded to 12-items regarding child symptoms (e.g. “feeling down or depressed,” “being rude and disrespectful to people) on a 5-point Likert scale from 0 (“not a big problem”) to 4 (“a very big problem”). The measure produces a total score and two subscales, internalizing symptoms and externalizing symptoms. The current study utilized the internalizing and externalizing subscales, which had Cronbach’s alphas of .91 and .95, respectively.
Home adjustment to COVID-19 scale—learning at home child difficulties (HACS-child difficulty)
Children’s difficulties with learning from home were assessed via the Child Difficulties subscale of the HACS (Becker, Quach et al., 2020). This subscale is composed of 6-items rated on a 5-point Likert scale assessing the frequencies of difficulties from 0 (“never”) to 4 (“always”). This subscale had a Cronbach’s alpha of .92 in the current sample.
Data Analysis
Data were analyzed using a structural equation approach with the lavaan package in R (Rosseel, 2012). First, measurement invariance analyses were conducted for each scale or subscale to determine whether these measures functioned in the same way for both the ADHD non-ADHD groups. To do this, we fit the strong invariance model (Meredith, 1993), which constrains the factor loadings and the intercepts to be equal across groups while allowing the latent means, latent variances, and residual variances to differ across groups. If the strong invariance model fits, then group scores are on a comparable scale. Model fit judgments were guided by Hu and Bentler’s (1998) recommendations of the Comparative Fit Index (CFI) > 0.95, Tucker Lewis Index (TLI) > 0.95, Root Mean Square Error of Approximation (RMSEA) < 0.06, and Standardized Root Mean Square Residual (SRMR) < 0.08. The model fit measures for all scales and subscales are displayed in Supplemental Table 1. Although not all scales met all of these criteria, the PSS, the PIP, and both EPII scales all exhibited severe misfit, which indicates that we have evidence that these scales do not function the same way for children with and without ADHD in this sample. For these reasons, these scales were omitted from further analyses with the exception of EPII negative impact. Although the EPII negative impact subscale exhibited less-than-ideal fit, we thought it better to include an imperfect measure of general COVID-19 impact rather than ignore the differential impact of the pandemic on families in the study. Of note, when the EPII was removed from the model, results did not significantly differ.
After establishing measurement invariance for the measures described above, we proceeded by using the sum scores of each of these measures in linear regression models. Sum scores of the six subscales that measure risk (DASS Anxiety, Depression, and Stress subscales, and the APQ Core Monitoring, Inconsistent Discipline, and Corporal Punishment subscales) correlated moderately with each other (0.43–0.85). Therefore, a general risk variable was defined by summing the standardized sum scores of these subscales. However, HACS-Parent Confidence correlated negligibly APQ Positive Parenting and APQ Involvement (0.15 and 0.29 respectively), suggesting that these scales may reflect distinct aspects of resilience. Therefore, we decided not to create an aggregated resilience variable and instead used these variables as separate predictors. Three models were fit using three different criteria: HACS-Child Difficulties, BFSP Internalizing, and BFSP Externalizing. For each model, the predictors were the composite risk variable, the APQ Positive Parenting subscale, the APQ Involvement subscale, the HACS-Parent Confidence subscale, ADHD diagnosis, EPII negative impact scale, age, sex (males = 1, females = 0), pre-COVID-19 SES (income categories treated as a linear predictor), and the interaction of ADHD status with four primary variables: risk, APQ Positive Parenting, APQ Parent Involvement, and HACS-Parent Confidence. All predictors were standardized (including the composite risk variable) except for ADHD diagnosis, sex, age, and pre-COVID-19 SES. For these analyses, we used the mice package in R (van Buuren & Groothuis-Oudshoorn, 2011) to fit the regression models with multiple imputation. Then, in light of prior research demonstrating an impact of formalized school services (i.e., IEP/504 plan) on difficulties with remote learning (Becker, Breaux et al., 2020), we then refit these three regression models using only the subset of children with ADHD and including the reception of school services as a predictor (students with missing responses to the school services question were excluded in this set of regressions; n = 11). In these regressions, ADHD status was not included as a predictor (because all included children had ADHD), and the moderation effect of school services with the risk factor, general COVID-19 impact, positive parenting, parent confidence, and parent involvement were included. In addition, given the known impact of medication status on the functioning of children with ADHD, we refit these three regression models using only the subset of children with ADHD and including medication status as a predictor (students with missing responses to the medication question were excluded in this set of regressions; n = 23). In these regressions, ADHD status was not included as a predictor (because all included children had ADHD), and the moderation effect of school services with the risk factor, general COVID-19 impact, positive parenting, parent confidence, and parent involvement were included.
Results
Descriptive Analyses
Children with ADHD (ADHD group) and without ADHD (non-ADHD group) did not differ significantly on grade, sex, or race, but did differ, as expected, on SNAP scores: inattention, t(254) = −10.19, p < .001; hyperactivity/impulsivity, t(254) = −10.53, p < .001. No group differences were observed for SES.
Predicting Parent Reports of Child Difficulties With Remote Learning
Results of the regression on HACS-Child Difficulty scores are presented in Table 2. ADHD status did not predict HACS-Child Difficulty, indicating no differences between the ADHD and non-ADHD groups. Child sex was a significant predictor, with boys having higher scores than girls (
Model Predicting Child Difficulties With Remote Learning.
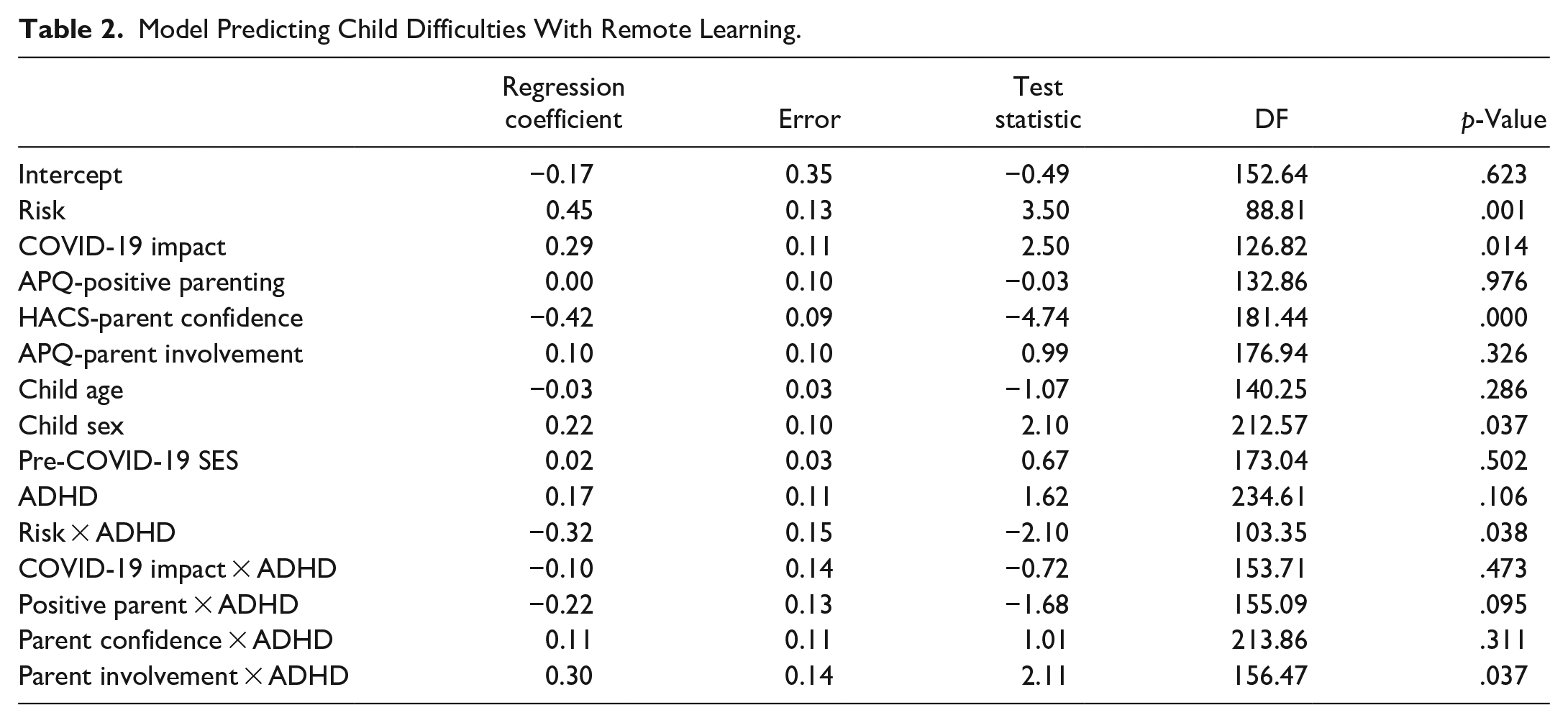

Moderation effect of ADHD on risk and HACS-child difficulty.

Moderation effect of ADHD on parent involvement and child difficulty.
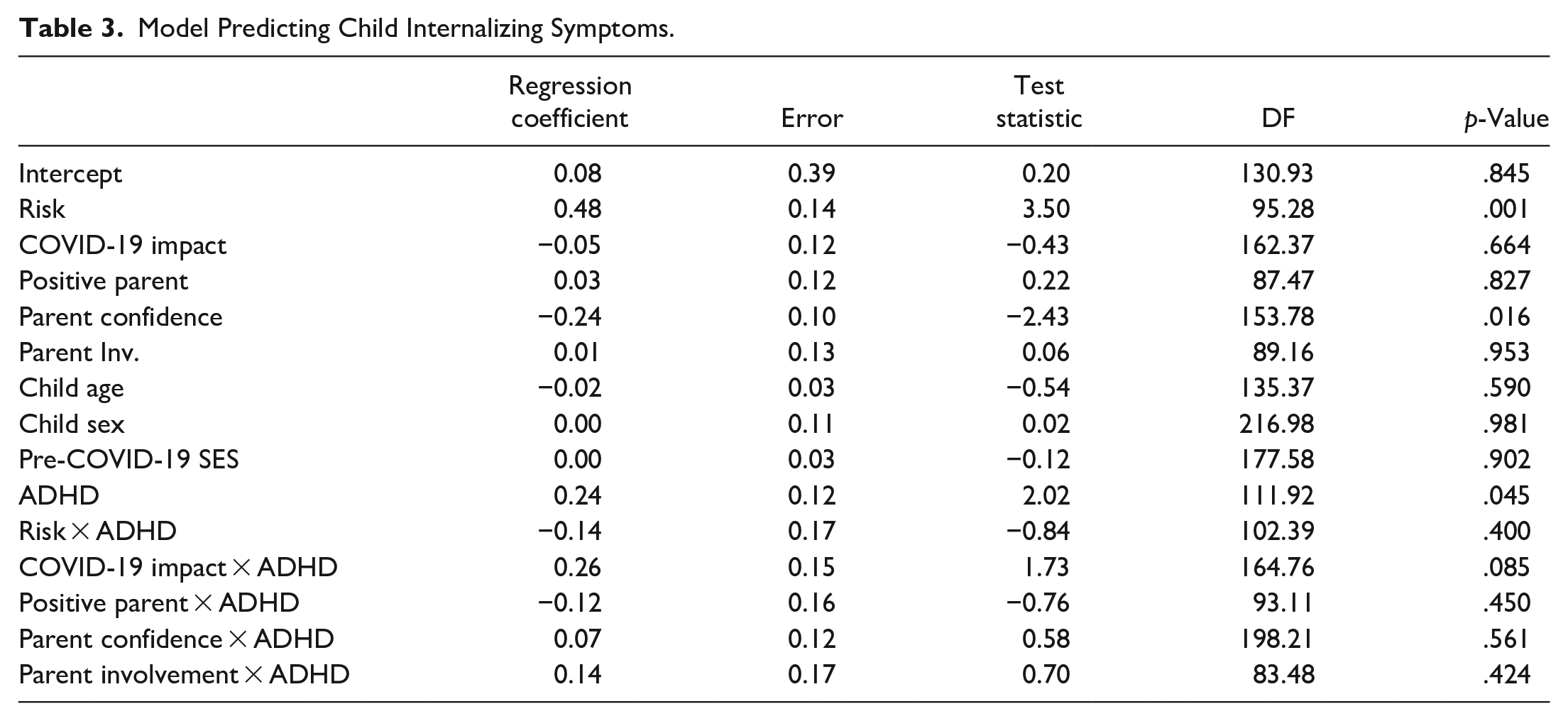
Predicting Parent Report of Internalizing Symptoms
Results of the regression on BFSP-Child Internalizing scores are presented in Table 3. ADHD was a significant predictor with BSFS Internalizing scores higher for children with ADHD than those without (
Model Predicting Child Internalizing Symptoms.
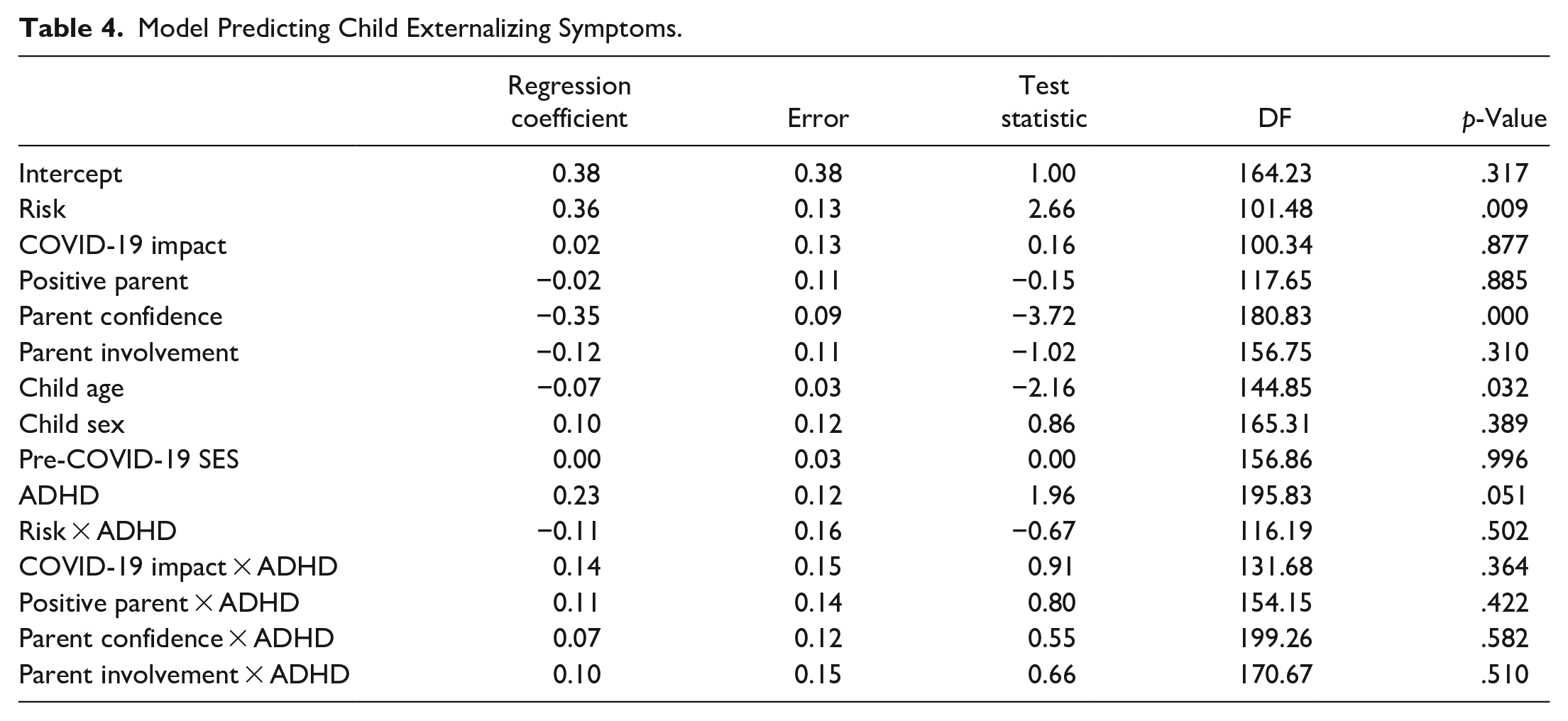
Predicting Parent Report of Externalizing Symptoms
Results of the regression on BFSP-Child Externalizing scores are presented in Table 4. ADHD status was not found to be a significant predictor. Higher risk scores (
Model Predicting Child Externalizing Symptoms.
Analyses Examining Risk and Resilience Depending on School Accommodations
Within the ADHD group, 48 children were not receiving any school accommodations while 89 had an IEP or 504 plan prior to the pandemic, based on parent report. Results of the regressions on HACS-Child Difficulty scores, BFSP-Child Internalizing scores, and BFSP-Child Externalizing scores are presented in Supplemental Tables 2 to 4. For each outcome variable, no statistically significant differences were found for ADHD children who did and did not receive school services prior to the COVID-19 pandemic, nor were any of the moderation effects statistically significant.
Analyses Examining Risk and Resilience Depending on Medication Status
Within the ADHD group, 57 children were not taking psychoactive medications while 68 were taking psychoactive medications at the time of the study. Results of the regressions on HACS-Child Difficulty scores, BFSP-Child Internalizing scores, and BFSP-Child Externalizing scores are presented in Supplemental Tables 5 to 7. For each outcome variable, no statistically significant differences were found for ADHD children who were or were not taking psychoactive medication, nor were any of the moderation effects statistically significant.
Discussion
The present study examined how parental factors impacted difficulties with remote learning and internalizing and externalizing symptomatology during the COVID-19 pandemic for children with and without ADHD. Building upon prior findings (Becker, Breaux et al., 2020; Bobo et al., 2020; Breaux et al., 2021; McFayden et al., 2021; Melegari et al., 2021; Roy et al., 2021; Sciberras et al., 2022; Wendel et al., 2020; Zhang, Shuai et al., 2020), the current study was the first to bring multiple parental risk and resilience factors together into a comprehensive model to assess their impact on outcomes for children with and without ADHD. Our study identified a risk factor for child outcomes that included parents’ symptoms of anxiety, depression, and stress and maladaptive parenting styles, including poor supervision, inconsistent discipline, and corporal punishment. Moreover, three separate resilience factors were identified: parents’ confidence in helping their children with remote learning, positive parenting, and an involved parenting style. The relationship between these parental risk and resilience factors and child difficulties with remote learning and symptoms of psychopathology were examined while considering ADHD diagnostic status, COVID-19 impact, and demographic variables.
Contrary to prior work in adolescents (Becker, Breaux et al., 2020), children with and without ADHD did not differ in degree of difficulty with remote learning in our sample. Age and sex differences between the present sample and the sample studied by Becker, Breaux et al. (2020) may contribute to these inconsistent findings. School-aged children without ADHD may have had a similar level of difficulty adapting to remote learning as youth with ADHD, while among adolescents, this transition was more difficult for those with ADHD. In addition, Becker, Breaux et al. (2020) had an ADHD sample with a higher proportion of males in the ADHD group than in the group without ADHD, while our diagnostic groups did not differ in sex (~60% male in each group). Across the whole sample in the current study, males were found to have more difficulties with remote learning than females; thus, sex differences may contribute to the greater difficulties among adolescents with ADHD found in prior work. Regarding psychopathology, children with ADHD had more internalizing symptoms than children without ADHD. Surprisingly, however, the two groups did not significantly differ in externalizing symptoms, although this effect approached significance (p = .051), suggesting an expected trend toward more externalizing symptoms among children with ADHD. Since pre-COVID functioning was not assessed, it cannot be determined if the non-ADHD group may have experienced a worsening of behaviors or the children with ADHD exhibited improvements, which, if the latter were true, would be similar to the findings of Bobo et al. (2020). Overall, findings from the current study indicate that, while remote learning difficulties did not differ between groups, children with ADHD experienced more internalizing symptoms and a trend toward more externalizing symptoms during the pandemic than children without ADHD.
Across youth with and without ADHD, the parental risk factor which included parents’ internalizing symptoms, stress, and implementation of maladaptive parenting styles, significantly predicted poorer outcomes across all three domains: difficulties with remote learning, internalizing symptoms, and externalizing symptoms. This suggests that parents who experienced higher levels of internalizing symptoms and stress, and relied more heavily on disengaged approaches to parenting (i.e., poor supervision, inconsistent discipline, and corporal punishment), were less well able or had less capacity to support their children with the transition to remote learning, which may have contributed to greater school-related difficulties. This relationship between parental risk and child difficulties with remote learning was stronger among children without ADHD than those with the diagnosis. Parents of children with ADHD may have already been providing their child with additional academic support at home, and thus, were better able to do so in the stressful and evolving context of the COVID-19 pandemic. Specifically, parents of youth with ADHD may have learned how to effectively assist their child with their academic work (e.g., providing organizational structure, frequent breaks, rewards for sustained attention) prior to the pandemic, and thus were better prepared to do so during remote learning, which helped mitigate the association between parental risk factors and child difficulties.
With regard to psychological outcomes in relation to the latent risk factor, children of parents with more internalizing symptoms and negative approaches to parenting demonstrated more internalizing symptoms themselves as well as more externalizing behaviors. This observed relationship between parent and child internalizing symptoms is consistent with prior work demonstrating the social learning of anxiety and depression between parents and their children (Beardslee et al., 1996; Fisak & Grills-Taquechel, 2007; Lieb et al., 2002; Woodruff-Borden et al., 2002). Further, parental responses to trauma and prolonged parental difficulty has been associated with increasing internalizing symptoms among youth (Chen et al., 2020), while disengaged approaches to parenting have been associated with increased externalizing symptoms in children with ADHD (McRae et al., 2020). These associations were not moderated by ADHD diagnosis, suggesting that child internalizing and externalizing symptoms were exacerbated by parent psychopathology, stress, and negative parenting approaches, regardless of ADHD status.
Proposed resilience factors were not as consistently predictive of child outcomes as the risk factor described above. Parents’ confidence in their ability to help their children with remote learning was the only resilience factor negatively associated with all three child outcomes across diagnostic groups. This indicates that parents who felt they were able to help their children complete assignments and stay academically motivated during the pandemic had children with fewer difficulties with remote learning and fewer psychological concerns. This suggests that parents’ confidence related to one of the core changes for families during the pandemic—the shift to remote learning—helped children succeed academically and emotionally during this uncertain time. In addition, ADHD status moderated the effect of an involved parenting style on difficulties with remote learning. Contrary to study hypotheses, greater parental involvement was predictive of greater child difficulties with remote learning, a relationship that was stronger in the children with ADHD than without. This suggests that parents may have become more involved once their child exhibited difficulties, and that parents of children with ADHD may have done so to a greater degree, in light of possible school challenges prior to the pandemic. Indeed, recent findings indicate that parents of youth with ADHD used active involvement as a strategy to help their children with remote learning during the pandemic more frequently than parents of youth without ADHD (Roy et al., 2021). Additionally, parents with a more involved style may have been more attuned to their child’s difficulties with remote learning and thus reported higher levels of difficulty.
There are several limitations to the current study. First, while the sample was geographically diverse with representation from many regions of the U.S., it was predominately white and middle- to upper-class, which may have impacted results. To address this, we included a COVID-19 impact score as well as annual household income as a proxy for SES in our models to try to account for these differential effects of COVID-19. However, the demographic characteristics of our sample limit the generalizability of the findings, particularly in a time when resources available at home likely impacted family and academic experiences. Given the greater impact of COVID-19 on marginalized populations (see https://www.ama-assn.org/delivering-care/health-equity/impact-covid-19-minoritized-and-marginalized-communities), it is important to investigate our findings in a more racially, ethnically, and economically diverse sample. Second, all measures were completed by a parent in the household, which increases the possibility of monomethod bias and could inflate the observed relationships between parent factors and child outcomes. Additionally, the majority of reporters in the study were mothers, which may bias the results to predominately reflect mothers’ experiences during the pandemic and their perceptions of their children’s outcomes. Relatedly, objective data on school difficulties or academic performance were not collected because they would have been difficult to standardize given the recruitment of families from diverse schools, states, and regions of the country and likely heterogeneous approaches to remote learning (e.g., full days on remote learning platforms, primarily independent work, etc.). Third, ADHD diagnosis from a healthcare provider was parent-reported. While an ADHD symptom inventory confirmed greater symptoms among the ADHD group than the non-ADHD group, the reported diagnosis was not verified via a standard diagnostic interview given the use of online data collection to collect a large, diverse sample.
While previous work shows the impact of individual parent factors on the outcomes of children with and without ADHD during the COVID-19 pandemic, this work suggests that multiple parent factors contribute to difficulties with remote learning as well as child mental health outcomes. Overall, our findings suggest that supporting and improving parents’ mental health and confidence in helping their children succeed academically can benefit children’s outcomes, in addition to parents’ quality of life, in the context of a significant global environmental stressor and abrupt alternation to established routines and family dynamics. Further, given that remote learning is likely to remain more commonplace moving forward (e.g., growing numbers of permanently virtual schools or remote learning days due to inclement weather; Singer, 2021), understanding how parent factors relate to child outcomes, particularly for children with ADHD, in this context will benefit students’ academic and emotional well-being.
Supplemental Material
sj-docx-1-jad-10.1177_10870547221084670 – Supplemental material for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder
Supplemental material, sj-docx-1-jad-10.1177_10870547221084670 for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder by Melanie R. Silverman, Jill Stadterman, Danny Lorenzi, Leah Feuerstahler, Emily Hirsch and Amy K. Roy in Journal of Attention Disorders
Supplemental Material
sj-docx-2-jad-10.1177_10870547221084670 – Supplemental material for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder
Supplemental material, sj-docx-2-jad-10.1177_10870547221084670 for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder by Melanie R. Silverman, Jill Stadterman, Danny Lorenzi, Leah Feuerstahler, Emily Hirsch and Amy K. Roy in Journal of Attention Disorders
Supplemental Material
sj-docx-3-jad-10.1177_10870547221084670 – Supplemental material for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder
Supplemental material, sj-docx-3-jad-10.1177_10870547221084670 for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder by Melanie R. Silverman, Jill Stadterman, Danny Lorenzi, Leah Feuerstahler, Emily Hirsch and Amy K. Roy in Journal of Attention Disorders
Supplemental Material
sj-docx-4-jad-10.1177_10870547221084670 – Supplemental material for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder
Supplemental material, sj-docx-4-jad-10.1177_10870547221084670 for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder by Melanie R. Silverman, Jill Stadterman, Danny Lorenzi, Leah Feuerstahler, Emily Hirsch and Amy K. Roy in Journal of Attention Disorders
Supplemental Material
sj-docx-5-jad-10.1177_10870547221084670 – Supplemental material for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder
Supplemental material, sj-docx-5-jad-10.1177_10870547221084670 for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder by Melanie R. Silverman, Jill Stadterman, Danny Lorenzi, Leah Feuerstahler, Emily Hirsch and Amy K. Roy in Journal of Attention Disorders
Supplemental Material
sj-docx-6-jad-10.1177_10870547221084670 – Supplemental material for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder
Supplemental material, sj-docx-6-jad-10.1177_10870547221084670 for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder by Melanie R. Silverman, Jill Stadterman, Danny Lorenzi, Leah Feuerstahler, Emily Hirsch and Amy K. Roy in Journal of Attention Disorders
Supplemental Material
sj-docx-7-jad-10.1177_10870547221084670 – Supplemental material for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder
Supplemental material, sj-docx-7-jad-10.1177_10870547221084670 for Parental Factors That Confer Risk and Resilience for Remote Learning Outcomes During the COVID-19 Pandemic Among Children With and Without Attention-Deficit/Hyperactivity Disorder by Melanie R. Silverman, Jill Stadterman, Danny Lorenzi, Leah Feuerstahler, Emily Hirsch and Amy K. Roy in Journal of Attention Disorders
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.