
Abstract
Purpose:
Investigate the quality of mothers’ interactions with children with ADHD and a marginal disturbance in socioemotional competence (MDSC).
Research Methods:
A total of 49 mother-boy dyads were included, and we observed their communication on neutral and conflict topics for children with ADHD and MDSC, children with ADHD alone, and children with typical development (TD). The Chinese version of the Specific Affect Coding System 20-code was used to examine the affective presentation in communication.
Results:
Mothers of children with ADHD and MDSC had less negative disengagement affect compared with those of children with ADHD alone. Boys with ADHD and MDSC and boys with TD had constant positive engagement between neutral and conflict conditions in parent-child interaction. Boys with ADHD and MDSC had significantly less positive affect and more neutral affect than children with ADHD only.
Conclusions and Implications:
Boys with ADHD and MDSC and their mothers had worse quality of observed mother-child communication than children with ADHD only and their mothers.
Introduction
ADHD is a prevalent developmental disorder associated with a range of current and long-term impairments (American Psychiatric Association, 2013). Parent-child interaction difficulties in children with ADHD have been observed across a wide range of developmental ages, from preschooler to adolescence (Deault, 2010; Johnston & Mash, 2001). A number of variables affecting the differences in parent-child interaction between children with ADHD and children with typical development (TD) have been identified, such as oppositional defiant disorder, parenting stress, and family conflicts (Deault, 2010).
Socioemotional competence requires skillful coordination of various mental processes such as the ability to successfully interact and communicate in a social context, to appropriately deal with emotions, and to utilize contextual resources to meet developmental goals (Iarocci et al., 2007). Children with ADHD are at high risk for difficulty in social and emotional competence, with estimates of between 50% and 75% having problems relating to others (Wehmeier et al., 2010). Children with ADHD frequently present deficits in emotional impulsivity and emotional self-regulation (Barkley, 2015; Faraone et al., 2018). Managing children’s behavioral problems and supporting emotion regulation in children with ADHD can be stressful for parents (Deault, 2010). Children’s behavioral problems and emotional dysregulation may elicit unresponsive, negative, or even punitive reactions from parents (Deault, 2010; Havinga et al., 2019). Unsupportive socialization practices in a negative family context could mutually maintain and reinforce a coercive parent-child interaction pattern (Havinga et al., 2019). However, the effect of difficulty in social and emotional competence on parent-child interaction of children with ADHD has rarely been addressed in research using an observational methodology.
Mother-son conflict is most frequent in preadolescence (e.g., 10–12 years old or fifth to seventh grade) compared with adolescence or young adults (e.g., 13–22 years old or eighth grade to college undergraduate; Laursen et al.,1998). Conflict resolution may facilitate expression of expectation from mothers and sons and is significant to parent–child relationships (Mastrotheodoros et al., 2020). Forth to sixth graders in Taiwan go to elementary school while seventh graders in Taiwan go to junior high school and have different educational and social interaction experiences (Lee et al., 2013). Therefore, this study recruited fourth to sixth grade children with ADHD and their mothers and examined their communication with neutral and conflict topics.
Studies of children with TD found gender differences in communication, socialization (Adani & Cepanec, 2019), emotional adjustment and empathy (O’Brien et al., 2013) with girls functioning ahead of boys. For children with ADHD, gender differences in the social domains were similar to those with TD. Girls with ADHD had better social skills than boys during school-aged years (Mahendiran et al., 2019). Although mothers interacted with their sons and daughters in a similar manner, boys with ADHD received more praise, fewer interactions, and reported to be more emotional than girls with ADHD in observed mother-child interaction (Beffra & Barkley, 1985).
In addition, the role of ethnic Chinese mothers is to provide a “secure” and loving environment within the home that is not seen between fathers and children (Jankowiak, 1992). Mothers have greater stress in supervising their children with ADHD, especially in managing their behavior and inattention problems at the same time as supervising their homework and academic performance (Gau, 2007; Liu et al., 2017). Since gender effects were noted and boys with ADHD likely have more significant socioemotional problems such as interaction with mothers than girls with ADHD, this study recruited boys with ADHD and boys with TD and compared their mother-child interaction.
Study Motivation and Hypotheses
Although difficulty in social and emotional competence is evident and prevalent in children with ADHD, its impact on observed parent-child interaction remains underexplored. In addition, parent-child communication is a meaningful daily activity that is critical to the quality of family life (DeGrace, 2003). Parent-child interaction is also an important aspect related to the efficacy of developmental services, yet it has rarely been addressed in research with an observational methodology. Moreover, since gender effects are noted between boys and girls, and between mothers and fathers in families of children with ADHD, this study examined mother-boy interactions by recruiting three groups of dyads (i.e., boys with ADHD and a marginal disturbance in socioemotional competence (MDSC), boys with ADHD alone, and boys with TD). Based on previous studies (Deault, 2010; Johnston & Mash, 2001; Lee et al., 2013), we hypothesized that:
Boys with ADHD and MDSC and their mothers would have the highest percentages of time of negative engaging and negative disengaging emotions, and the lowest percentages of time of positive emotions when discussing conflict topics.
Boys with ADHD alone and their mothers would have higher percentages of time of negative engaging and negative disengaging emotions, and lower percentages of time of positive emotions when discussing conflict topics compared with mother-boy dyads in the TD group.
Boy’s and maternal affective presentations of the three groups would not be significantly different in neutral conditions.
Method
Participants
Participants were recruited from August 2013 to July 2015. Boys with ADHD and their mothers were invited from a child psychiatric out-patient clinic in central Taiwan. The boys in the ADHD only and ADHD and MDSC groups had their regular visits to the Department of Psychiatry, Chung San Medical University Hospital. Those who met the DSM-5 diagnostic criteria for ADHD as assessed clinically for at least three clinic visits were recruited. The clinical diagnosis of ADHD and psychiatric comorbidity were made based on the criteria of DSM-5 after comprehensive assessment including in-depth psychiatric interviews and evaluations of different areas of medicine, development, education, and psychosocial aspects with multiple sources of information provided from family, schools, and psychologists.
Boy-mother dyads with TD were recruited from three elementary schools or the community in central Taiwan by invitation and using a snowball technique. Participants were 49 boys and their mothers, including 11 dyads of boys with TD, 19 dyads of boys with ADHD only, and 19 dyads of boys with ADHD and MDSC. Children’s ages ranged from 9.08 to 12.92 years old and mothers from 31.92 to 51.83 years old (see Table 1 for demographic and clinical information).
Comparison of Sociodemographic and Clinical Variables Among Three Groups.

Note. TD = typical development; ADHD + MDSC = ADHD and a marginal disturbance in socioemotional competence; IA = inattention symptoms; SNAP = Swanson, Nolan, and Pelham Rating Scale; HI = hyperactivity/impulsivity symptoms; OP = oppositional symptoms; CBCL = Child Behavior Checklist; BERS = Behavioral and Emotional Rating Scale; BDI = Beck Depression Inventory.
p < .01. ***p < .001.
Inclusion criteria were: (1) boys in fourth to sixth grades with mothers as their primary caregivers and lived together in the previous 6 months; (2) boys in the ADHD group met the DSM-5 criteria by a psychiatrist’s interview (American Psychiatric Association, 2013); and (3) boys in the control group screened negative for ADHD and oppositional defiant disorder using the Chinese version of the Swanson, Nolan, and Pelham, version IV scale (SNAP-IV). The Chinese version of SNAP-IV is validated with good psychometric properties in Taiwan (Gau et al., 2008). All boys were screened with the Behavioral and Emotional Rating Scale (BERS; Epstein & Sharma, 1998; Yang, 2001). The BERS is a strength-based assessment to measure the social and behavioral skills important to the child’s significant relationships in homes, schools, and the community (Epstein & Sharma, 1988). Taiwanese norms and cut-off scores were used to screen children with marginal or severe ranges of socioemotional competence (Yang, 2001). Boys with behavioral and emotional quotient scores of BERS greater than 89 were screened as normal social and emotional development (Yang, 2001). MDSC was defined as the behavioral and emotional quotient scores of BERS between 89 and 71. No boy was screened as having severe socioemotional problems with BERS in this study. Exclusion criteria were presenting other neuropsychiatric disorders that might impact the parent-child interaction including bipolar disorder, schizophrenia, obsessive compulsive disorder, autism spectrum disorder, serious medical conditions, or sensory disorders.
In an attempt to recruit children with socioemotional problems but without ADHD and other neurodevelopmental disorder, this study invited and screened children and mothers from three elementary schools and the community. However, the sample size of children with socioemotional problems or MDSC but without ADHD and other neurodevelopmental disorders (n = 3) was too small for group statistical comparison.
Mothers filled the aggressive and delinquent behavior subscales of the Chinese version of the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001) to assess boys’ levels of aggression and delinquency. The Chinese version of the CBCL was reported to have good psychometric properties (Yang et al., 2001). All mothers rated their levels of depression using the Chinese version of the Beck Depression Inventory–Second Edition (BDI-II; Beck, 1999; Chen, 2000). The Chinese version of the BDI-II is a sensitive tool shown to discriminate five different levels of depression (α = .92; Pan & Hsu, 2008). Only one mother was prescribed antidepressants.
This study was approved by the Institutional Review Board of Chung Shan Medical University Hospital. Researchers informed participants that they were to be recorded, described the detailed procedures including the topics of mother-child communications, and explained the possible negative consequences. Participants voluntarily joined the study procedures, were aware they were free to withdraw, and signed consent forms before starting data collection.
Measures
Issues Checklist
The Issues Checklist (IC) is used to select topics that mothers and boys may be concerned or argue about at home (Robin & Foster, 1989). Test-retest reliability of IC is .49 to .80 (Enyart, 1984). Mother-child dyads reported if they had discussed the conflict topics in the past 2 weeks at home and approximated the frequency and intensity of anger on a 5-point Likert scale. Topics for conflict discussion were selected by the weighted frequency/intensity scores and checked for the willingness of the dyads to discuss in the laboratory.
The Specific Affect Coding System 20-Code Version
The Specific Affect Coding System (SPAFF) is a reliable and valid research tool to capture the affect in parent-child interaction (Hollenstein et al., 2004; Hollenstein & Lewis, 2006; Lee et al., 2013). The SPAFF consists of 20 mutually exclusive codes including positive, negative disengagement, negative engagement, and neutral categories of affective expression (Jones et al., 2005; Shapiro & Gottman, 2004). Each code is based on a combination of facial expressions, gestures, posture, voice tone and volume, speech rate, and verbal/motor response content to capture a gestalt of the affective tone of behavior. Negative engagement affects are active and negative social engagement, whereas negative disengagement affects are more withdrawn or disengaged types of affective behavior. The neutral code is non-emotional in nature. The Chinese SPAFF was validated in a previous study of parent-child interaction of children with ADHD and their mothers in Taiwan (Lee et al., 2013).
Procedures
After signing informed consent, a senior child psychiatrist conducted a psychiatric interview with mothers and boys. Mothers filled out SNAP-IV, CBCL, BERS, IC, and BDI-II questionnaires. Boys selected topics from IC. Mother-boy communication was recorded in a laboratory of the first author’s university before a mother-son group training for children with ADHD. Participation in the training group was voluntary and about half of the participants in the ADHD group attended the training sessions. No payment was made for participation. For the control group, mothers were given a book on parenting preadolescents for compensation.
Mothers and sons selected conflict issues from IC before the observation session. For those children with ADHD and with medication, medication was taken 1 to 2 hours before the observation period. During each observation session, dyads first participated in a neutral discussion, and second in a conflict-solving discussion. Half of the dyads engaged in one of the child’s generated conflict problems first, followed by his mother’s, then the child’s, etc. The other half of the dyads started with one of the mother’s generated problems first. Dyads were requested to discuss each problem until they agreed on a practical solution, but only the first 10 minutes were included for data analysis.
Four undergraduate students coded the video-recordings of mother-boy interaction in a random order. Coders were blinded to the group status of the dyads and the study hypotheses. Observers were extensively trained to a criterion of 75% agreement between any two of the coders before formal coding. All the videos were coded by two coders individually. Disagreements between the two coders were discussed until they achieved consensus. Weekly recalibration training took place to minimize coder drift.
Duration scores of each participant in each condition were calculated by subtracting onset time from offset time for each entry and summing for each code and each affective category. Percentages of time were calculated by dividing the time of positive and negative engagement, negative disengagement, and neutral affect by the total interaction time in the neutral and conflict-solving condition, respectively.
Data Analysis
The affect variables were analyzed using a two-way 3 × 2 mixed analysis of covariance (ANOCVAs) with the diagnostic group (i.e., boys with ADHD and MDSC, boys with ADHD only, and boys with TD) as the between-subject factor and condition (i.e., neutral or conflict-solving) as the within-subjects factor. Covariables included child’s medication use and maternal BDI-II total score. Dependent variables were percentages of time of positive engagement, negative engagement, negative disengagement, and neutral affect categories.
Results
Boys with ADHD had significantly more inattention, hyperactivity, and delinquent problems and less social and emotional competency than boys with TD. Boys with ADHD and MDSC had significantly more aggressive behaviors than boys with TD. Table 1 reports the descriptive and inferential statistics of sociodemographic and clinical variables.
A significant and large interaction effect (F(2, 44) = 3.47, p = .04, η2 = .14) was found in children’s positive affect, indicating that the three groups of children had differential reactions to the neutral and conflict-solving conditions. Since a significant interaction effect was found, post hoc analyses were used to further explore how group and condition variables interact with children’s positive affect. There was significant simple main group effect in the neutral condition (F(2, 46) = 3.52; p = .04), but not in the conflict-solving condition (F(2, 46) = 1.79, p = .18). Post hoc comparison revealed that children in the ADHD only group had significantly higher positive affect than children with ADHD and MDSC in the neutral condition.
Post hoc analyses of simple main condition effect confirmed that children with ADHD only had significantly higher percentages of positive affect in the neutral condition compared with that in the conflict-solving condition (F(1, 16) = 7.89, p = .01, η2 = .33). Children with typical development (F(1, 9) = 1.11, p = .33, η2 = .14) and children with ADHD and MDSC (F(1, 16) = 3.81, p = .07, η2 = .19) had no significant difference of positive affect between these two conditions.
A significant and large interaction effect (F(2, 44) = 3.89, p = .03, η2 = .16) was found in children’s neutral affect, indicating that the three groups of children had differential reactions to the neutral and conflict-solving conditions. Since a significant interaction effect was found, post hoc analyses were used to further explore how group and condition variables interact with children’s neutral affect. There was a significant simple main group effect in the neutral condition (F(2, 46) = 3.28; p = .046), but not in the conflict-solving condition (F(2, 46) = 1.68, p = .20). Post hoc comparison revealed that children in the ADHD only group had significantly lower neutral affect than children with ADHD and MDSC in the neutral condition.
Post hoc analyses of simple main condition effect confirmed that children with ADHD only had significantly lower percentages of neutral affect in the neutral condition compared with that in the conflict-solving condition (F(1, 16) = 6.56, p = .02, η2 = .29). Children with typical development (F(1, 9) = .66, p = .44, η2 = .09) and children with ADHD and MDSC (F(1, 16) = 1.05, p = .32, η2 = .06) had no significant difference of neutral affect between these two conditions.
No significant interaction effects were found in the other two categories of child’s affect, indicating that the three groups of children did not have differential affective reactions to the neutral and conflict-solving conditions in terms of negative engagement and negative disengagement. There were no significant group differences in the other two affective variables (i.e., negative disengagement and negative engagement) among the three groups of boys. Means, standard deviations, and results of the two-way 3 × 2 mixed ANCOVAs of children’s affect are presented in Table 2.
Means, Standard Deviations, and Results of Mixed Design ANCOVA of Child’s Affect.
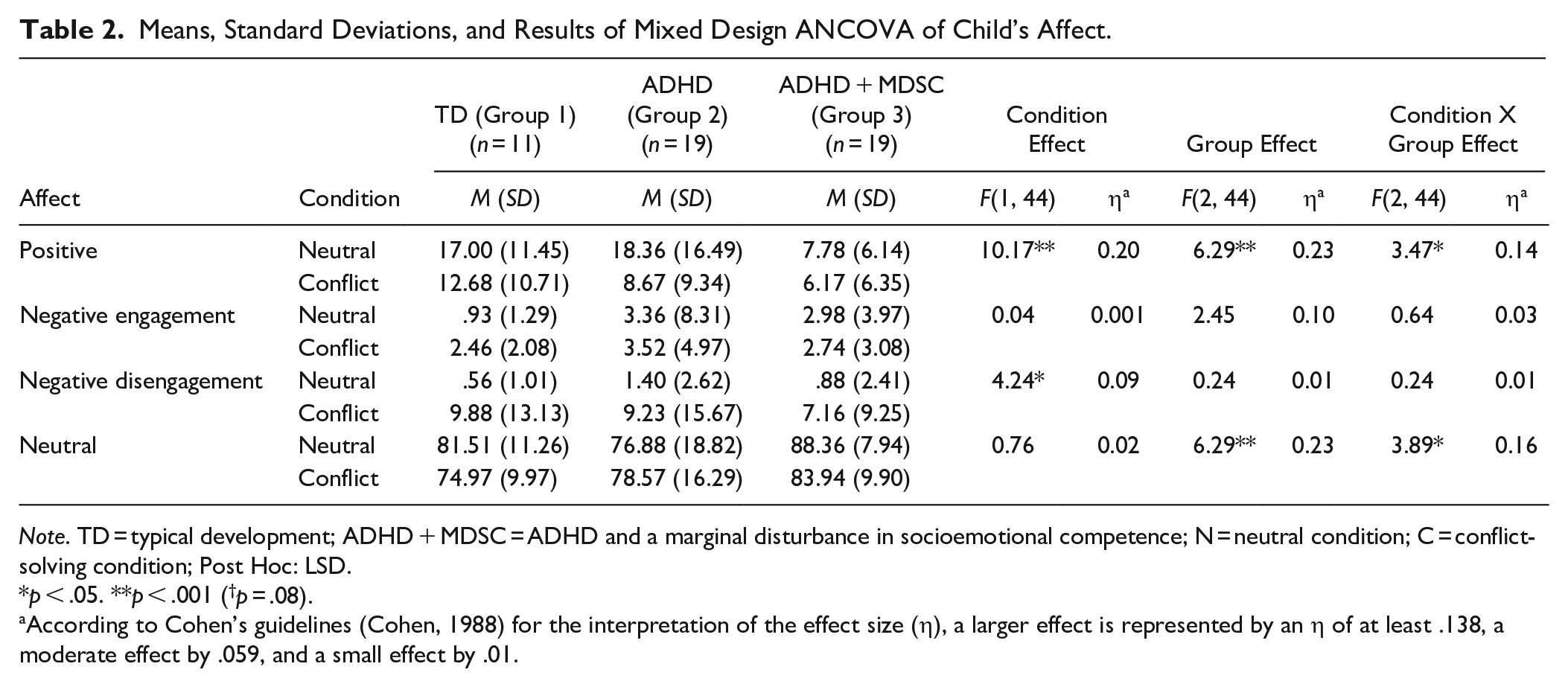
Note. TD = typical development; ADHD + MDSC = ADHD and a marginal disturbance in socioemotional competence; N = neutral condition; C = conflict-solving condition; Post Hoc: LSD.
p < .05. **p < .001 (†p = .08).
According to Cohen’s guidelines (Cohen, 1988) for the interpretation of the effect size (η), a larger effect is represented by an η of at least .138, a moderate effect by .059, and a small effect by .01.
No significant interaction effects were found in the four categories of maternal affect, indicating that the three groups of mothers did not have differential affective reactions to the neutral and conflict-solving conditions. A significant group effect (F(2, 44) = 4.66, p = .02, η2 = .19) was found in the maternal negative disengagement affect. Post hoc pairwise analyses revealed mothers of children with ADHD and MDSC displayed less negative disengagement affect than mothers of children with ADHD only. There were no significant group differences in the other three affective variables (i.e., positive engagement, neutral, and negative engagement) among the three groups of mothers. Means, standard deviations, and results of the two-way 3 × 2 mixed ANOVAs of maternal affect are presented in Table 3.
Means, Standard Deviations, and Results of Mixed Design ANCOVA of Mother’s Affect.
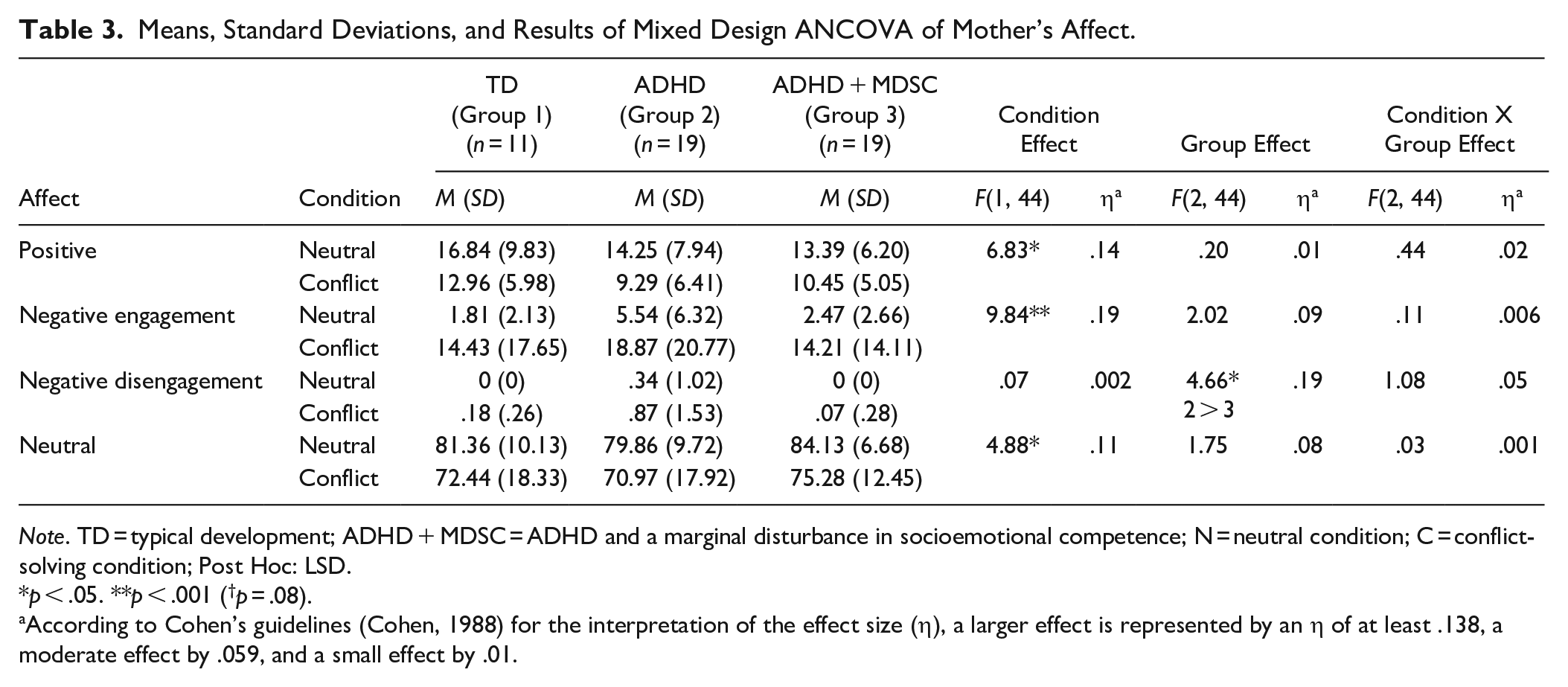
Note. TD = typical development; ADHD + MDSC = ADHD and a marginal disturbance in socioemotional competence; N = neutral condition; C = conflict-solving condition; Post Hoc: LSD.
p < .05. **p < .001 (†p = .08).
According to Cohen’s guidelines (Cohen, 1988) for the interpretation of the effect size (η), a larger effect is represented by an η of at least .138, a moderate effect by .059, and a small effect by .01.
Discussion
To the best of our knowledge, this is one of the first studies examining the role of child’s MDSC on mother-child interaction of children with ADHD. This study found boys with ADHD and MDSC had significantly less positive engagement affect than boys with ADHD only in the mother-child interaction. Boys with ADHD and MDSC and boys with typical development had constant positive affect between neutral and conflict conditions. Mothers of children with ADHD only had significantly more negative disengagement than mothers of children with ADHD and MDSC with a large effect size (η2 = .16). The findings support the transactional model (Granic & Patterson, 2006) that emphasizes the linkage between affect in mothers and boys related to boy’s ADHD and MDSC.
Comparison of Mother-Child Dyads of Children With ADHD Only and Those of Children With TD
In contrast to our hypotheses, constant positive affect was noted in boys with typical development compared with boys with ADHD only. A small sample size of the typical development group (n = 11) may account for the non-significant findings between neutral and conflict conditions. In addition, stimulant medication may account for the significant findings in the ADHD only group since over 70% of children with ADHD only took a stimulant 1 to 2 hours before recording. Research indicates mother-child interaction of children with ADHD improved with stimulant medication (Danforth et al., 1991).
The Impacts of Children’s MDSC on Affect in Parent-Child Interaction of Children With ADHD
Consistent with our hypotheses, low levels of positive emotional expressivity in parent-child interaction were associated with children with ADHD and MDSC. It is possible that children with ADHD and MDSC do not have adequate communication skills or behaviors to engage in discussion with their mothers (Gresham, 1986), and therefore have less positive interaction with their mothers.
Constant positive affect between neutral and conflict conditions are noted in children with ADHD and MDSC. This raises concerns if those children with ADHD and MDSC have a certain level of depression. Insufficient competence for socioemotional development may be frustrating to children with ADHD and MDSC. Further studies may be needed to screen children with ADHD and MDSC with depression and examine the impact of depression on mother-child interaction.
On the other hand, in contrast to our hypotheses, MDSC was not related to a child’s negative behaviors or affective presentation in parent-child interaction. Previous observational studies (Barkley et al., 1991, 1992) have found negative or conflictual child behaviors in parent-child interaction were not related to children’s ADHD, but oppositional defiant or conduct problems. Both children with ADHD and MDSC and children with ADHD only had significantly higher levels of oppositional defiant problems, delinquency, and aggressive problems than children with TD but the symptom severities were not high (Table 1).
The Impacts of Child’s MDSC on Maternal Affect in Parent-Child Interaction
This study found mothers of children with ADHD only had significantly more disengaged or withdrawn behaviors than mothers of children with ADHD and MDSC. One possible explanation is less disagreement or conflictual discussion between children with ADHD and MDSC and their mothers. Alternately, it is also possible that a history of unsuccessful maternal efforts to communicate with their children results in a reduction of maternal efforts and a disengagement from mother–child interactions, a strategy that may have short-term benefits for the mother but long-term costs for both the mother and the child.
Strengths and Limitations
This study has a number of strengths. Firstly, this is one of the first studies examining the influence of marginal socioemotional disturbance on mother-child interaction of children with ADHD. Secondly, quantitative and microsocial methodology was used to examine the impacts of children’s ADHD and level of socioemotional competence on parent-child interaction. Thirdly, this study examined the impact of MDSC on parent-child interaction in two contrasting contexts, namely neutral and conflict conditions.
In addition to a relatively small sample size, this study has several limitations. Firstly, over 70% of the children with ADHD took medication on the day of video recording and their parents received parenting consultation, thus influencing the findings. Future studies may include children with ADHD before the implementation of any treatment or medication. Secondly, this study screened children’s socioemotional competence with parent reports. Future studies may use professional reports such as teacher or clinically standardized assessments of children’s socioemotional competence. Thirdly, there were not sufficient participants to include a group of children without ADHD but with MDSC in the study (n = 3). Fourthly, this study included only mothers’ and boys’ evaluations of parent-child interactions. As a result, gender effects (i.e., mothers compared with fathers and boys compared with girls) were not observed. Future studies may include fathers and girls and examine the impact of children’s (i.e., the differences of boys and girls) and parental (i.e., the differences of mothers and fathers) gender when examining the impact of children’s socioemotional competence on parent-child interaction. Fifthly, although mothers of children with ADHD were found to have more depressive symptoms, we did not examine the impact of maternal depression on the quality of parent-child interaction.
Implications for Developmental Disabilities Practice
Assessment of children’s socioemotional competence and its impacts on the quality of significant interpersonal relationships (e.g., parent-child interaction) is needed in children with ADHD.
The assessment and intervention may be tailored to not only the children, but also the significant others such as mothers.
Therapists working with children with ADHD and MDSC should pay attention to parent-child interaction especially in cases where mothers may potentially overlook children’s subtle responses to conflictual issues.
Conclusion
Boys with ADHD and MDSC and their mothers have worse quality of parent-child interaction than children with ADHD only and children with TD and their mothers. Further studies are needed to replicate and extend this study by including children with ADHD and multiple levels (e.g., normal, marginal, and clinical ranges) of socioemotional disturbance and examine their impacts on parent-child interaction.
Footnotes
Acknowledgements
The authors gratefully acknowledge all the families who participated in this study. We also thank all the clinical, school, and research staff involved in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by grants from National Science Council (NSC 102-2410-H-040 -008 -MY2).