
Abstract
Objective:
To evaluate intervention characteristics and components within behavioral sleep interventions in school-aged children with ADHD and examine evidence related to effectiveness.
Method:
A systematic review was conducted using PsycINFO, Embase, MEDLINE, PubMed, and OpenGray. The subsequent meta-analysis used sleep outcomes to produce comparable effect sizes (Hedges’ g) and compare intervention effects between randomized controlled trials and pre-post studies.
Results:
Eleven articles satisfied the inclusion criteria (562 children, across all groups, aged 5–14 years, M = 8.71). Studies reported improvements in sleep although there was marked heterogeneity between studies and limited use of objective sleep measures within them. On average, intervention groups improved more than control groups in the five randomized controlled trials (−0.46, 95% CI = [−0.58, −0.35], k = 4).
Conclusion:
The findings support the use of behavioral sleep interventions for school-aged children with ADHD. Findings suggest that brief, individualized intervention may be more effective than standardized.
ADHD, characterized by inattention, hyperactivity, and impulsivity, is the most common neurodevelopmental disorder in children and adolescents (American Psychiatric Association [APA], 2013). ADHD affects approximately 5.3% of children worldwide (Polanczyk et al., 2007) and is associated with long-term, adverse functional outcomes (Feldman & Reiff, 2014). These include poor academic achievement through adolescence and young adulthood (Gadow et al., 2001; G. Weiss & Hechtman, 1993), and reduced executive functioning (Marx et al., 2010).
Sleep Disturbance in ADHD
By parent-reported subjective sleep measures, approximately 70% to 85% of children with ADHD are affected by sleep disturbances (Sung et al., 2008; Yürümez & Kılıç,2013). These disturbances are behavior-based, for example, bedtime refusal, night-time awakenings (Sung et al., 2008), and inconsistent sleep onset (Craig et al., 2020). Further, sleep difficulties in children with ADHD may partially arise from the development of unhealthy sleep practices, such as exposure to electronic devices in the bedroom or inconsistent bed and wake times (Craig et al., 2020). Sleep in ADHD is often less efficient and more disjointed than in the general population, as measured by polysomnography (Vigliano et al., 2016). In addition, polysomnography has shown decreased rapid eye movement sleep, and actigraphy has revealed increased nocturnal activity, and increased sleep onset latency in ADHD samples (Bullock & Schall, 2005; Konofal et al., 2001). Objective measures of sleep include polysomnography, night-time recording of physiological characteristics, and actigraphy, measurement of movement during sleep used to infer sleep or wake states (McCall & McCall, 2012). Subjective measures, such as parent-report sleep questionnaires, include parent evaluations of child sleep. There are discrepancies between objective and subjective measures of sleep (Cortese et al., 2009). For example, within sleep onset latency, Craig et al. (2020) posit a potential reason for this discrepancy may be due to parent reports of increased night-to-night variability, with difficulty falling asleep or bedtime resistance, that actigraphy would not identify.
The direction of this relationship is unclear: problems with sleep may be exacerbated by ADHD and may also exacerbate ADHD symptoms (Hvolby, 2015). For example, disrupted sleep can also lead to symptoms, functional impairments, or behaviors similar to those due to ADHD (Beebe, 2006; Gruber, 2009). Sleep difficulties in children with ADHD are found whether treated or not with psychostimulant medication. The association between stimulant medication use and sleep is complex, however, and studies have returned mixed findings. While some research has suggested an impact of stimulant medication on sleep in children with ADHD, this has not been the case for all children; and furthermore, other studies have been either inconclusive or non-significant (Cohen-Zion & Ancoli-Israel, 2004; Corkum et al., 1999; Kidwell et al., 2015).
In addition to environmental, behavioral, and potential pharmaceutical challenges, sleep in children with ADHD is often further impaired when the individual has a complex profile of one or more co-occurring disorders (Gruber, 2009; Ivanenko et al., 2004). Common comorbid disorders with ADHD include conduct disorder, oppositional defiant disorder, depression and anxiety disorders, and autism spectrum disorder (Reale et al., 2017). Such disorders can adversely impact sleep independently (Waxmonsky, 2003) and therefore, when comorbid with ADHD, may exacerbate sleep disturbances experienced by the child.
However, given the aforementioned behavioral challenges faced by children with ADHD in relation to sleep, the present review focused on interventions that aim to improve sleep-related behaviors, with emphasis on identifying the types of interventions and the common components of those interventions.
Behavioral Sleep Interventions
As sleep problems are common in children with ADHD (Sung et al., 2008), it is important for this cohort and their families to address such behaviors with appropriate intervention. The term “behavioral sleep intervention” is used in the literature to describe treatment using a range of cognitive, behavioral, and other strategies to improve sleep, often in addition to developing favorable healthy sleep practices. Difficulties initiating and/or maintaining sleep are common in children with ADHD (Corkum et al., 1998) possibly requiring intervention to target specific bedtime behaviors. For example, bedtime resistance may be improved by setting limits for the child to follow, such as ignoring child protests or providing the child with a bedtime pass to leave their bedroom once each night (Owens & Mindell, 2011; Phillips et al., 2020; Sciberras et al., 2020).
Moreover, cognitive strategies such as stimulus control and relaxation (Dewald-Kaufmann et al., 2019) may be used to assist the child to prepare for sleep. Healthy sleep practices, noted as sleep hygiene within the reviewed studies, broadly refers to cognitive, environmental, or behavioral modifications to improve sleep (Jefferson et al., 2005). There are two main areas of healthy sleep practices: sleep organization, that is, a suitable sleep-wake routine, and practices that prevent increased pre-bedtime arousal, that is, a sleep-conducive routine (Mindell & Meltzer, 2008). Further strategies include restrictions on naps, caffeine intake, and the use of electronic devices close to bedtime. Most, if not all, behavioral sleep interventions include psychoeducation on normal sleep patterns and appropriate sleep hygiene. Interventions may also use a combination of these strategies to attend to multiple sleep-related problems or in an individualized manner based on the sleep problem(s) the child experiences (Nikles et al., 2020). To the best of our knowledge, previous research has not examined methodological similarities and differences between interventions to provide information on common characteristics.
Behavior-focused interventions within children with ADHD have been shown to improve sleep problems, with studies citing reductions in bedtime resistance (Mullane & Corkum, 2006), sleep onset delay, and daytime sleepiness (Amin Shokravi et al., 2016). Furthermore, Keshavarzi et al. (2014) reported improvements in mood and social interactions in children with ADHD following intervention, compared to age-matched control groups with and without ADHD.
Prior Research and Current Review
Research into which sleep interventions are effective is necessary to ensure appropriate treatment is carried into clinical practice. Two review articles have been published in this area: a systematic review with meta-analysis (Phillips et al., 2020) and a systematic review (Nikles et al., 2020). Phillips et al. (2020) reviewed behavioral sleep interventions for children aged 5 to 18 years with neurological or neurodevelopmental disorders, including ADHD. This review reported improvements in sleep for children with neurological and neurodevelopmental disorders following a behavioral sleep intervention, however, the authors were unable to comment on whether those improvements were maintained given that no studies commented on maintenance. Whereas Nikles et al. (2020) examined sleep hygiene interventions for children, 5 to 18 years old, with ADHD. Nikles et al. (2020) recommended sleep hygiene for children with ADHD and disturbed sleep and noted that tailored interventions were likely to be more successful than providing only instructions or a brief intervention. The authors further commented on lack of consistency across study methodology providing insufficient data for comparison and meta-analysis.
The current review extends previous reviews with the inclusion of studies published after search completion by Phillips et al. (2020) and Nikles et al. (2020), including a sustained impact study examining maintenance of improvements in sleep post-intervention (Sciberras et al., 2020), and exploration of intervention methodologies, characteristics, and components to help guide future treatment recommendations. Further, the present review builds on that of Nikles and colleagues, by providing a meta-analytic assessment of improvements in sleep following intervention.
Thus, the aim of this review was to explore the effectiveness of behavioral sleep interventions for school-aged children (aged 5–15 years) with ADHD. The objectives were (a) systematically to identify and examine the quality of interventions, (b) explore methodological structure and intervention characteristics and components to inform future research and clinical practice, (c) use meta-analytic techniques to compare intervention effects, to determine if treatment improved poor sleep over no treatment, and to explore potential moderators to treatment, and (d) make recommendations for future research and clinical practice, based on the review findings.
Method
The current review was completed following the Synthesis Without Meta-Analysis (SWiM; Campbell et al., 2020) and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020; Page et al., 2021) guidelines.
Registration and Protocol
The protocol for this study was registered on Open Science Framework as a scoping review, but later updated to a systematic review and can be accessed at (https://osf.io/b328e). During data analysis, it was decided to incorporate a meta-analytic component. No deviations from the method of the originally registered study protocol occurred beyond the systematic review guidelines used and the addition of a meta-analysis.
Information Sources and Search Strategy
A search was conducted of the electronic databases PsycINFO, Embase, MEDLINE, and PubMed. The Google search engine and OpenGray were used to find gray literature. The search included all studies until 2 April 2022. Terms for the target cohort such as “ADHD,” “sleep disorder,” and “child” were used in combination with intervention terms such as “behavioral intervention,” “therapy,” and “treatment” (see Supplemental Table S1a, b, and c). A hand search of the reference lists of articles that met eligibility criteria and relevant meta-analyses and systematic reviews focusing on sleep interventions was conducted. Systematic reviews and meta-analyses were not included for review.
Inclusion Criteria
Articles included in this review met the following criteria: (a) published in English; (b) included participants between 5 and 15 years of age with diagnosed ADHD; (c) participants experienced at least one sleep problem (measured by objective sleep measures, sleep assessment scales, or by parent report); (d) utilized a behavioral intervention to improve sleep; (e) participants not receiving any other sleep intervention (pharmacological or non-pharmacological); and (f) reported quantitative and/or qualitative data on sleep outcomes. In addition, articles were excluded if participants had a diagnosis of intellectual disability.
Selection of Sources of Evidence
Title and abstract screening was completed together by the first author (80%) and author GH (20%) against eligibility criteria. Articles were then assessed at the full-text level for further eligibility by the first author. Screening and selection of studies was conducted using “Covidence systematic review software” (Veritas Health Innovation, Australia), which automatically removed duplicates.
Data Collection Process and Data Items
A data charting spreadsheet was developed by the first author in consultation with author AS. Data extraction was completed by the first author, with 45% of the included studies corroborated by author RB. Any discrepancies were to be evaluated by author AC, however, no discrepancies occurred. The following variables were extracted: sample size (N), participant characteristics (sex, mean age, medication use, and comorbid disorders), study design (randomized controlled trials, pre-post studies, case studies, case series); intervention characteristics (individual vs. group based, delivery type, individually-tailored vs. standardized, number of intervention sessions, and nintervention components), intervention length, session frequency, outcome measures (sleep related: (a) subjective measures and (b) objective measures; and non-sleep related) and outcome results (mean, standard deviation, t-values, F-tests, p-values, Cohen’s d, eta-squared, and partial-eta squared). Although gray literature was searched, strict guidelines were enforced to ensure the extracted data could aid in meeting the aims of this review, such as provision of intervention strategy information (objective b). Additional data were sought from two study authors, to no avail.
Critical Appraisal of Individual Sources of Evidence
All assessments of risk of bias and quality of evidence were conducted by the first author and discussed and corroborated with author CP. The methodological rigor of RCTs was assessed using the Cochrane Handbook of Systematic Reviews of Interventions (Higgins et al., 2021) and their associated Risk of Bias tool (RoB tool version 2; Sterne et al., 2019). Based on the algorithms provided in the RoB tool Version 2 (Sterne et al., 2019), studies were assessed as being at low, moderate, or high risk of bias on each RoB item. In addition, case series and pre-post studies were assessed using the RTI item bank for observational studies (Viswanathan et al., 2013). Due to lack of categorization guidelines, studies were then assigned an overall low, moderate, or high risk of bias score based on assigned points, described in Supplemental 4, under Supplemental Table S4c.
To assess the quality of evidence, the Oxford 2011 Levels of Evidence (OCEBM Levels of Evidence Working Group, 2011) was used. Studies were categorized across five levels of evidence, based on study design, where 1 was the highest and 5 was the lowest.
Measures of Effect
A variety of effect measures for the included studies were reported, including mean, standard deviation, t-values, F-tests, p-values, and effect sizes (Cohen’s d, eta-squared, and partial-eta squared).
Synthesis of Results
As outlined in our registered protocol, a narrative synthesis was employed, in which all studies were included. The studies were grouped by criteria used to determine sleep disturbance (e.g., cut-off on questionnaire vs. formal diagnosis) to compare reported sleep changes from baseline, as well as delineation of RCT and non-RCT trials. Studies were also grouped as individualized treatment or standardized treatment between participants to inform suggestions for future research and clinical practice. Data, including descriptive variables and outcomes of each intervention and intervention characteristics, were tabulated and are provided in this review, grouped as RCT and non-RCT (pre-post tests and case series), then ordered from largest to smallest Hedges’ g effect.
Data for sleep outcome measures were combined using Comprehensive Meta-Analysis Version 3 (CMA; Borenstein et al., 2013) to produce an overall study effect size using Hedges’ g. Where studies reported subjective and objective sleep outcomes, data were input into CMA to provide a pooled study effect size. Of the 11 studies, 9 reported data suitable for calculating a Hedge’s g. Effect sizes were interpreted following Cohen’s (1992) guidelines such that 0.2 was considered a small effect, 0.5 a medium effect, and 0.8 a large effect.
Meta-Analysis
CMA was used to meta-analyze data using a random effects model, given that the interventions and study designs varied. This analysis used subjective and objective sleep outcome data reported by the reviewed articles to provide comparable results to the pooled effect size analysis. Due to the inclusion of both RCTs and non-RCTs, 1 the meta-analysis was completed in two stages. First, the RCTs and the pre-post studies were analyzed to assess the effect of intervention comparing baseline and follow-up in the intervention groups only. Second, the RCT sleep outcome data were analyzed to determine the differences in effect between the intervention and control conditions. For both analyses, where studies reported multiple follow-ups, data for each time point were included and combined by CMA. Sensitivity analyses were conducted to determine (a) whether effects were biased by inclusion of non-RCTs (which were excluded for one analysis) and (b) whether effects were biased based on inclusion of typically developing children. 2
A meta-regression-based moderator analysis was planned to examine factors that may influence intervention effects. Moderators to be examined were: (a) mean sample age, (b) percentage of girls, (c) presence of comorbid disorders, (d) ADHD medication use, (e) intervention length, (f) intervention delivery, (g) follow-up interval, (h) individual versus group, and (i) individualized versus standardized interventions. Clinical heterogeneity was explored visually using forest plots (Supplemental 2) and through discussion of study design (RCTs, pre-posttest, and case series), criteria used to define sleep disturbance, and intervention characteristics and strategies provided.
Results
Study Selection
The completed search identified 5,257 studies, including 1,583 duplicates. The remaining 3,674 were screened based on titles and abstracts. Sixty-nine were selected for full text review. Eleven articles met inclusion criteria (see Figure 1).
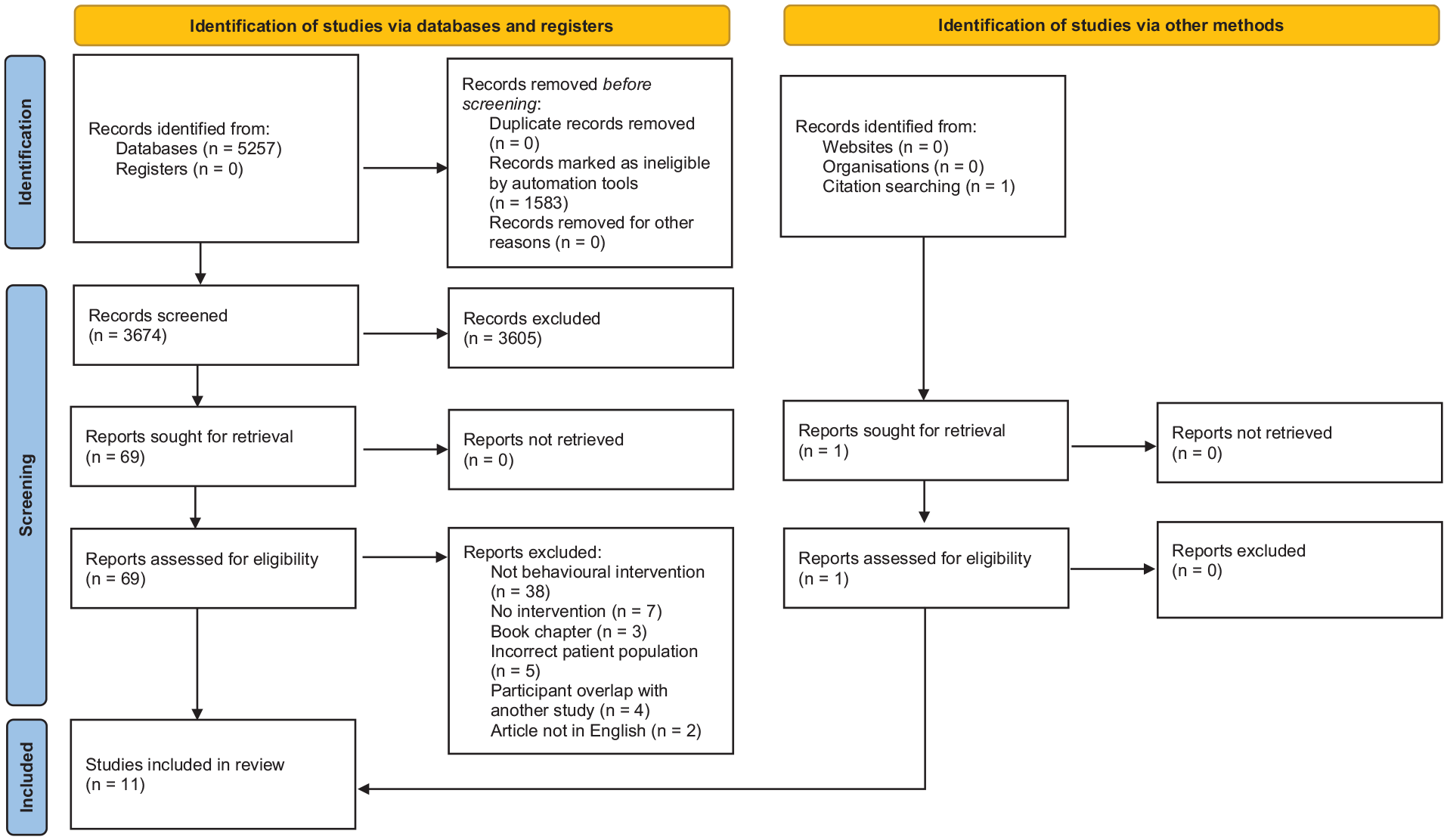
PRISMA 2020 flow chart.
Study Characteristics
Tables 1 to 3 describe characteristics of six RCTs (#1, Amin Shokravi et al., 2016; #2, Corkum et al., 2016; #3, Hiscock et al., 2015; #4, Keshavarzi et al., 2014; #5, Mehri et al., 2020; #6, Sciberras et al., 2011; #7, Sciberras et al., 2020), two case series (#8, Mullane & Corkum, 2006; #10, Vetrayan et al., 2017), and two pre-post studies (#9, Peppers et al., 2016; #11, Weiss et al., 2006). For the remainder of the review, included studies will be referred to by the aforementioned reference numbers.
Research Design of Included Studies.

Note. Studies ordered from largest to smallest effect size (Hedge’s g). Where studies note 0 follow-up time, outcomes were assessed immediately after intervention ceased. RCT = randomized controlled trial; ODD = oppositional defiant disorder; CD = conduct disorder; ASD = Autism spectrum disorder; ADD = attention deficit disorder; NR = not reported; N/A = not applicable; No loss* = no loss to follow up was reported.
Study reported 12-month follow up data from original intervention published in Hiscock et al. (2015).
p < .05. ‡p < .01.
Intervention Design of Included Studies.

Note. Studies ordered from largest to smallest effect size (Hedge’s g). BSI = behavioral sleep intervention.
Study reported 12-month follow up data from original intervention published in Hiscock et al. (2015).
p < .05. ‡p < .01.
Study Outcomes.

Note. Studies ordered from largest to smallest effect size (Hedge’s g). CSHQ = Children’s Sleep Habits Questionnaire; SDSC = Sleep Disturbance Scale for Children; PedsQL 4.0 = pediatric quality of life inventory 4.0; SDQ = Strengths and difficulties questionnaire; DPREMB = daily parent rating of evening and morning behavior; ADIS-C = Anxiety Disorders Interview Schedule for Children/Parent Version-IV; CPRS-R = Conners’ Parent Rating Scale, Short Form; CBCL = child behavior checklist; QoL = quality of life; ADIS-C = Anxiety Disorders Interview Schedule, Child Version; SOL = sleep onset latency.
Study reported 12-month follow up data from original intervention published in Hiscock et al. (2015).
p < .05. ‡p < .01.
Table 1 summarizes participant characteristics and research design. In total 562 3 children ranging from 5 to 14 years, with a mean age of 8.71 years 4 participated. Ten studies included participants taking stimulant medication for their ADHD (n = 433). One study used a combination of children with ADHD and typically developing (TD) children, split almost equally over the intervention and control groups (#2). Another study also recruited TD children, reporting three separate groups: an ADHD intervention group, an ADHD control group, and a TD group as an age-matched control group (#4).
Inclusion criteria and problem sleep were defined differently throughout the 11 included studies. Two studies (18%) classified disrupted sleep based on results from the Children’s Sleep Habits Questionnaire (CSHQ; #5 and #9). Some (27%) categorized participants based on moderate/severe sleep problem(s) reported by the parent, per the diagnostic criteria from the American Academy of Sleep Medicine (#3, #6, and #7). Two studies (18%) used criteria defined by Mindell and Durand (1993): (a) the child demonstrates the primary sleep concern a minimum of three nights per week and (b) the sleep problem is persistent (minimum duration of 4 weeks). This was used in conjunction with an additional assessment tool, either the DSM-IV-TR criteria for adult dyssomnia (#8) or the Sleep Disturbance Scale for Children (SDSC) total sleep score (#10). Two studies (18%) assessed sleep via quantitative methods of sleep onset latency either greater than 25 minutes, over a minimum of three nights per week (#2) or greater than 60 minutes averaged over 10 nights (#11). One study (9%) required a formal diagnosis of at least one sleep disorder provided by a child psychiatrist (#1). Finally, Keshavarzi et al. (2014, #4) aimed to use sleep training to improve emotional, social, and behavioral functioning, rather than focusing on improving sleep and therefore did not report a classification for problem sleep.
Tables 2 and 3 summarize intervention-specific parameters and outcomes respectively. Intervention structure varied between the studies, with parents and children following an instruction manual independently or completing standardized intervention with a trained clinician (n = 5) or attending an information or training session(s) (n = 6). Two studies (#2 and #8) used a distanced format, requiring no face-to-face elements. Follow-up measures were completed immediately (n = 4), and/or 2 to 6 months later (n = 5), with one intervention measuring outcomes 12 months post-intervention. Across the studies, improved sleep was measured by total scores on the CSHQ (n = 8) or SDSC (n = 2), with some studies incorporating sleep diaries (n = 5), actigraphy (n = 4), or both (n = 4). Actigraphy was used to measure differing aspects of sleep: sleep duration (#2, #3, and #11), sleep onset latency (#2 and #11), sleep efficiency (#3), wake after sleep onset (#3), and mean sleep latency (#8).
Further information on these measures is provided in Supplemental 3, outlining the assessment domains and reliability of the measures. Within the two parent-reported sleep measures (CSHQ: #1, #2, #3, #4, #5, #6, #7, and #9; and SDSC: #8 and #10), most domains were consistent across the surveys: disordered breathing, sleep initiation and maintenance, somnolence, and parasomnias. ADHD and behavior were assessed using 1 of 3 measures: the ADHD Rating Scale 4.0 (#3 and #6), the Child Behavior Checklist (CBCL; #2), or the Conners’ Parent Rating Scale (CPRS; #8). The first assesses domains of inattention and hyperactivity-impulsivity, whereas the remaining two provide a more comprehensive assessment of behavior, for example, including anxiousness and social problems.
Summary of Interventions
Interventions included elements of parent education, cognitive and behavioral adjustments, sleep hygiene, and other strategies to help the child initiate or maintain sleep, summarized in Table 4. All studies incorporated multi-component interventions, either provided as standardized treatment (i.e., all participants received the same education and treatment strategies; #1, #2, #4, #5, #8, #10, and #11) or individualized techniques, provided based on the specific sleep problem(s) reported (#3, #6, #7, and #9).
Intervention Strategies Used in Reviewed Studies.
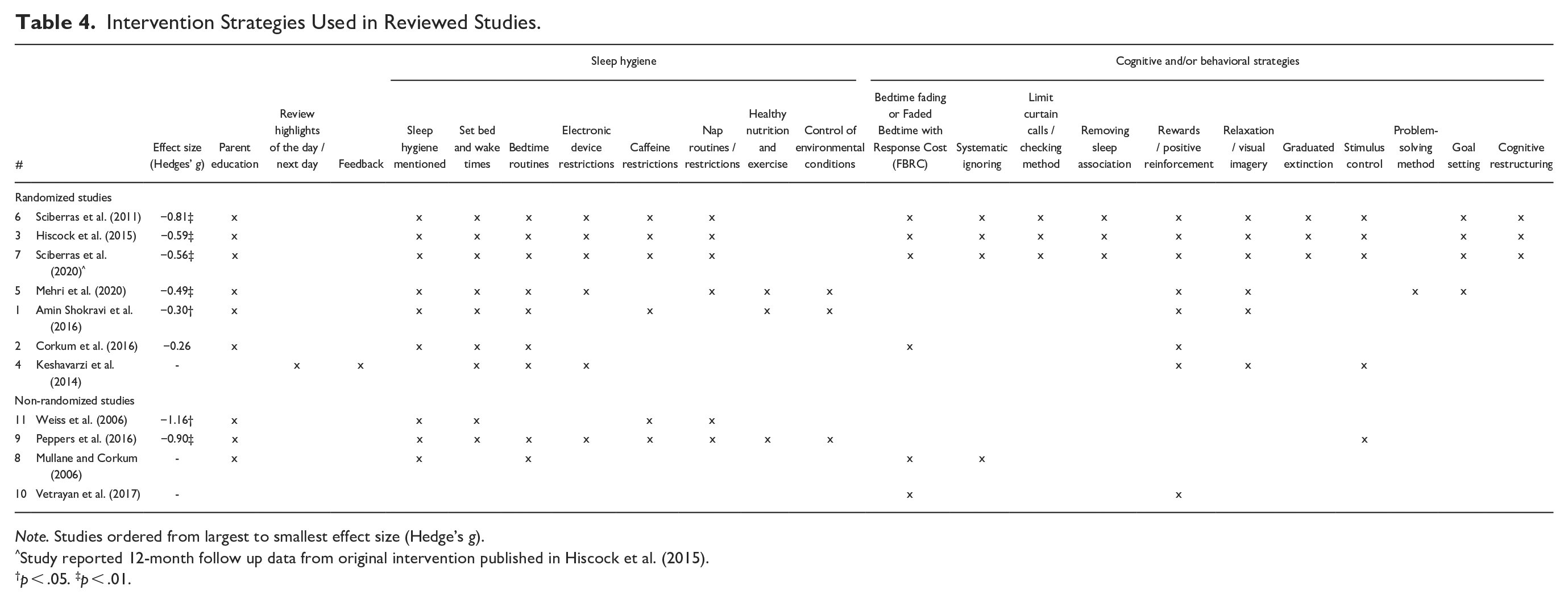
Note. Studies ordered from largest to smallest effect size (Hedge’s g).
Study reported 12-month follow up data from original intervention published in Hiscock et al. (2015).
p < .05. ‡p < .01.
Parent education on normal sleep and appropriate sleep practices was used in the majority of the interventions (n = 9). Sleep hygiene education (n = 9) included discussion of healthy sleep habits, such as health practices (e.g., diet, exercise, and caffeine use), and environmental factors (e.g., room temperature, noise, and light; Irish et al., 2015; Posner & Gehrman, 2011; Sutton et al., 2019). Given the two aspects of healthy sleep practices, sleep organization was targeted using techniques such as setting sleep and wake times (n = 9) and limiting or restricting naps (n = 6). Whereas practices to prevent or reduce pre-bedtime arousal included having consistent bedtime routines (e.g., having a hot bath or shower, getting into pajamas, etc.; n = 9), removal of technology from the bedroom, with restrictions on how close to bedtime electronic devices can be used (n = 6), caffeine restrictions (n = 6), and control of environmental conditions (n = 3).
The most common cognitive and/or behavioral strategy was rewards or positive reinforcement (n = 8). Additional common strategies included relaxation or visual imagery (n = 6) and bedtime fading or Faded Bedtime with Response Cost (FBRC; Piazza & Fisher, 1991) (n = 6 bedtime fading; 3 with a response cost component).
Risk of Bias and Quality Assessment
Supplemental 4 provides a summary of the RoB assessment and level of evidence assessment for the RCTs (Supplemental Table S4a), case series and pre-post studies (Supplemental Table S4b). The seven RCTs were assessed as having low risk of bias. The case series and pre-post studies were classified as having moderate risk of bias. The studies offered differing levels of evidence within a range of 1 to 5, where Level 1 studies hold the highest level of evidence.
Results of Individual Studies
All studies reported a reduction in sleep problems and an overall improvement in sleep for intervention participants, suggesting clinical homogeneity of effect. Improvement in sleep was classified based on changes from pre-intervention sleep to post-intervention. Quantified outcomes from the included studies are provided in Supplemental 5.
Results of Syntheses
Based on Hedges’ g, the study with the largest overall effect (−1.16) was Weiss et al. (2006, #11); a pre-post study. Of the RCTs, Sciberras et al.’s (2011, #6) intervention displayed the largest overall effect (−0.81); however, it should be noted that this study compared two intervention groups (brief vs. extended) with no control group. Whilst at 2 months the extended intervention produced the larger effect, by 5 months there was no difference. Finally, the RCT with the next largest overall effect (−0.59) was reported by Hiscock et al. (2015, #3).
Although a Hedges’ g effect size could not be calculated for Keshavarzi et al. (2014, #4) as total score data were not provided for the CSHQ, they reported significant improvements in total sleep time and frequency and length of night awakenings based on CSHQ scores.
Of the interventions that catered individually to the child’s sleep problem, all reported improvement in sleep: studies using the Sleeping Sound with ADHD intervention (#3, #6, and #7; Sciberras et al., 2010) and one pre-post study (#9). Whilst Sciberras et al. (2020, #7) reported a reduction in moderate/severe sleep problems in participants, a larger effect was noted in the original 2015 study (#3) compared to the 12-month 2020 follow-up. 5 Sciberras et al. (2011, #6) reported clinical improvements in moderate/severe sleep problems for both the brief and extended intervention groups; however, they noted a greater improvement for individuals in the extended group. One pre-post study reported a significant reduction in sleep problems based on CSHQ total sleep scores (#9).
The remaining studies used a standardized intervention structure for participants. Of which three RCTs (#1, #2, and #5) reported significant improvements in sleep based on lower CSHQ total scores at follow-up compared to baseline scores and to their control groups. Two case series (#8 and #10) reported clinically significant improvements in sleep problems moving children from the “clinically significant” to the “normal” range. One pre-post study (#11) found 5 (18.5%) participants experienced reduced actigraphy-measured initial insomnia to below 60 minutes. As a result, these five did not participate in the second phase of treatment, melatonin, not analyzed in the present review.
In seeking to explore the effect of the intervention strategies used, two RCTs, Hiscock et al. (2015, #3) and Corkum et al. (2016, #2), were compared as they had the largest and smallest effect sizes of the RCTs with control groups, respectively. The two studies had six intervention strategies in common, with Hiscock et al. (2015, #3) including numerous additional strategies aimed at sleep improvement. This finding tentatively suggests that the inclusion of further strategies may account for the larger effect size found for #3. Of the two non-randomized studies with Hedges’ g effect sizes (#9 and #11), there were five common strategies, with an additional five incorporated in #9. Both displayed large effect sizes, however, contrary to the overall pattern (mirrored in the comparison between #2 and #3), the study employing a standardized intervention (#2) had the larger effect.
Meta-Analysis: Overall Effects
The overall effect of intervention was assessed by aggregating intervention group pre-post effects from six RCTs (#1, #2, #3, #5, #6, and #7) and two studies without control groups (#9 and #11). Given Hiscock et al. (2015, #3) and Sciberras et al. (2020, #7) used the same cohort of participants, the latter was used as a third follow-up time point within the Hiscock et al. (2015) data. The effect using intervention data only was moderate and significant (−0.73, 95% CI = [−0.62, −0.41], k = 7), reflecting improvement with treatment. Heterogeneity (Q[6] = 3.69, p = .719, T2 = 0.00, I2 = 0.00) suggested a moderate level of variability between studies was inherent in nature, rather than due to measurement error and confirms the choice of a random-effects model.
Sleep outcomes for five of the RCTs were meta-analyzed to assess group effects to compare the effect of intervention versus control. One RCT (#6) was removed from this analysis as it did not include a non-treatment control group, and as above, the Sciberras et al. (2020, #7) data were included as a third follow-up for Hiscock et al. (2015, #3). The average intervention effect was significant and moderate (−0.68, 95% CI = [−0.84, −0.51], k = 4), with no marked statistical heterogeneity (Q[3] = 1.95, p = .583, T2 = 0.00, I2 = 0.00). Whilst there was a significant average control group effect of −0.28, this was smaller than the intervention effect, and marked heterogeneity was found across studies (Q[3] = 8.86, p = .031, T2 = 0.05, I2 = 66.13). This difference in the effect of interventions for sleep in ADHD between intervention and control groups was significant (−0.46, 95% CI = [−0.58, −0.35], k = 4), suggesting that the interventions improved sleep to a greater degree than the control condition (Q[3] = 5.93, p = .115). 6
We were interested in the contrast between individualized and standardized interventions for sleep outcomes from RCTs. One intervention was individualized (data provided over two publications: #3 and #7) and displayed a moderate, significant intervention effect of −0.67 (95% CI = [−0.90, −0.44], k = 1). Three RCTs used a standardized approach to intervention (#1, #2, and #5), and displayed a small to medium, significant intervention effect (−0.35, 95% CI = [−0.50, −0.19], k = 3).
Whilst moderation analysis was planned, this was not completed due to fewer than the 10 studies recommended for assessing potential contributions to heterogeneity (Higgins et al., 2021).
Discussion
This review aimed to explore intervention characteristics and components and to assess the effectiveness of behavioral sleep interventions in school-aged children (5–15 years) to inform future practice. A secondary aspect of assessment of effectiveness occurred via a meta-analysis of the studies. Just 11 studies met inclusion criteria, suggesting this is still an emerging intervention approach for children with ADHD. Of these, seven studies (all RCTs) were rated as having a low risk of bias, and the remaining four (all non-controlled designs) were rated as having a moderate risk of bias and were noted to have methodological design limitations. Given the presence of factors that impact the quality of evidence, such as lack of control groups, less emphasis should be placed on the non-randomized controlled studies reported. Although the total number of studies is limited, the majority displayed good methodological quality and rigor. All studies found improvements in sleep, clinically and/or via statistical significance.
All studies incorporated multiple strategies in differing combinations to improve the child’s sleep, making it challenging to determine which components led to sleep changes. However, certain strategies were implemented frequently across the interventions including parent education, sleep hygiene (e.g., set bed and wake times, bedtime routines, restrictions on caffeine, electronics use, and naps), and positive reinforcement/rewards suggesting these may be key components. Consequently, these strategies appear to be used commonly in behavioral sleep interventions for children with ADHD. Although there is not yet clear consensus on which intervention strategies are most effective or crucial for sleep improvement, an individualized approach to treatment may be especially useful by way of providing strategies for the specific difficulties experienced by a child. For example, the Sleeping Sound intervention (Sciberras et al., 2010; #3, #6, and #7) provides evidence that a brief, individualized behavioral intervention is effective at improving sleep difficulties in children with ADHD, displaying small, sustained benefits. This finding suggests that lengthy or intensified manualized interventions may not be required, rather a brief intervention can be effective if it is tailored to the requirements of the specific child and family.
Further, many of these techniques have been highlighted as useful for individuals with ADHD and proven effective in typically developing samples in a literature review (Hvolby, 2015) and a systematic review with meta-analysis (Meltzer & Mindell, 2014). In a framework for assessment and treatment of sleep problems for children with ADHD (Corkum et al., 2011), the authors highlighted four areas of treatment that could be used in this population: parent-involved behavioral interventions, sleep hygiene, positive bedtime routines, and bedtime fading with response cost.
The present review adds to this literature and informs future practice by assessing the effectiveness of these strategies, in combination with others, to improve sleep in children with ADHD through meta-analysis. From the RCTs analyzed, the intervention groups improved moderately (−0.68), and the control groups improved slightly (−0.28). Therefore, the intervention groups improved by 0.4 of a standard deviation more than controls, confirming Meltzer and Mindell’s (2014) suggestion that such behavioral interventions can improve sleep in children with ADHD. The studies applying the Sleeping Sound intervention (Sciberras et al., 2010; #3, #6, and #7) appear to be the most reliable given higher methodological rigor and quality of evidence in the studies. Moreover, this is the only intervention to be used in a long-term follow-up study (#7).
As sleep difficulties are common in children with ADHD and are often related to poor pre-sleep behavior, intervention targeting such behaviors may be particularly beneficial. Behavioral management strategies, such as creating a structured environment, rule setting, and rewarding positive behavior, in children with ADHD have proven effective in reducing oppositional and non-compliant behaviors (e.g., Van Den Hoofdakker et al., 2007; Webster-Stratton et al., 2011). In a literature review conducted by Rajwan et al. (2012), behavioral parent training informing parents on how to adjust undesired behaviors in children with ADHD displayed benefits in improving behaviors such as noncompliance, and disruptive and oppositional behaviors. Further, there may be differing mechanisms underlying non-pharmacological treatments for children with ADHD (Evans et al., 2018). Evans et al. (2018) discuss various mechanisms of action which may be pertinent to behavioral sleep interventions for children with ADHD. The authors comment that behavior management approaches target the reduction of undesired behaviors and increase of the frequency, rate, or intensity of desired behaviors. Evans et al. (2014) note that training interventions use the practice and repetition of altered or new behaviors until they become commonplace. Behavioral sleep interventions appear to incorporate a combination of behavior management strategies and training intervention and therefore these mechanisms are possibly associated with improved sleep following intervention.
That said, as each child with ADHD often experiences differing sleep disturbances, using the same intervention for all may not be ideal in clinical practice. Such an argument is consistent with the finding that, overall, the individualized interventions produced stronger effects than interventions using a standardized intervention structure. Individualized interventions may allow for more time spent on specific strategies to target identified problems, such that time is not spent implementing strategies that may not be useful for that child.
Few studies used both subjective and objective sleep measures. Fewer than half used actigraphy, with most focusing on parent-reported measures. Although we recognize that parent-reported sleep changes are important and valid, it may be best to conduct research into which interventions are most effective using objective sleep outcome measures (e.g., actigraphy) to ascertain quantitative data on elements of sleep improved, for example, total sleep time and sleep efficiency. This is emphasized given the discrepancies between data obtained from subjective and objective measures (Cortese et al., 2009). Despite findings from both forms of measure indicating improved sleep in children with ADHD, subjective measures often reveal more favorable outcomes than objective sleep measures (e.g., Corkum et al., 2016; Hiscock et al., 2015). Further, as it is challenging to implement participant blinding in behavioral interventions (Juul et al., 2021), objective sleep measures could be used more widely in research to provided blinded outcome data, albeit, it is acknowledged this may not be feasible in clinical practice.
Further, there was considerable variability in diagnostic criteria for disrupted sleep which, ideally, should be consistent between studies to allow for greater comparisons of potential sleep improvements and between-study assessment of intervention effectiveness. Standardized diagnostic criteria may be modeled from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; APA, 2013) diagnostic criteria for Insomnia Disorder. Criteria may include frequency and duration of the sleep disturbance, a predominant complaint of dissatisfaction with quantity or quality of sleep, and the sleep disturbance causing significant distress in other areas of functioning. Additionally, further detail of experienced sleep problems would provide more information on what the intervention is attempting to improve. This would provide valuable information for clinicians choosing an appropriate intervention for a particular client.
Our review suggests that brief, individualized sleep treatments can be highly effective in children with ADHD. However, there is an opportunity for future research to determine which children benefit from brief interventions versus those who may require a more lengthy or stepped care approach. For example, for a child who experiences bedtime anxiety, the initial strategy may be checking in on the child at regular intervals, leading into a more intensive approach such as camping out. Therefore, families that do not benefit sufficiently from a brief intervention, given challenges such as more intense behavioral or emotional difficulties, higher levels of family dysfunction, or a higher likelihood of attachment difficulties, may be offered additional intervention in a stepped care approach to address these more adverse or complex challenges.
The majority of studies were conducted face-to-face, with only two run as “distanced” (#2 and #8), that is, participants were not required to attend a clinic for any part of the intervention. Although some studies appeared not to require large amounts of face-to-face time, travel to receive treatment may not be practicable or feasible for all clients. Research into the effectiveness of delivering behavioral sleep interventions to children online is an area for investigation given the increased use of technology and the Internet (International Telecommunication Union, 2022) in recent years and difficulties of those living in regional areas to access necessary services (Australian Bureau of Statistics, 2021). Further, due to the current worldwide COVID-19 pandemic, it is important to ensure that online delivery of such interventions is effective.
Limitations of the present review include lack of multiple independent investigators screening within the article selection process, or at the data extraction phase according to best practice. This was not achieved due to limited resources and may reduce the objectivity in study selection or unintentionally allow for mistakes. Further, study designs and intervention characteristics were heterogeneous between the studies making isolation of techniques associated with the strongest clinical outcomes challenging. The limited number of studies contributed to the challenge of drawing clear clinical conclusions.
It was only possible to meta-analyze some of the studies included in this review. Statistics including the pre-post studies should be interpreted cautiously. Additionally, the limited sample size (N < 20; Huedo-Medina et al., 2006) of analyzed studies reduced power for analysis of variability in effect estimates due to heterogeneity and hindered an analysis of possible causes of statistical heterogeneity (e.g., presence of comorbid disorders, intervention length, and follow-up intervals).
Secondly, further inconsistencies impacted the generalizability of study findings. Control of stimulant medication for ADHD was inconsistent and, due to the small number of studies, could not be investigated as a moderator. In addition, some studies only sampled children taking medication, and others had a combination of medicated and non-medicated participants, perhaps to improve generalizability within the ADHD population. Furthermore, differences in total treatment time made it challenging to ascertain ideal levels of intensity of intervention, which, likewise, we could not explore as a moderator of outcome. Future studies may further explore the potential impact of medication use and effect of treatment time as the field, and publications of clinical trials grows. Future research of these factors has the potential to inform clinical care and practice guidelines for improving sleep in children with ADHD.
Additionally, compliance with intervention strategies was rarely reported. This extended to limited data on the frequency with which intervention strategies were used. This data could assist in interpreting different findings between studies and speak to treatment fidelity. For example, an intervention strategy that is not used frequently or conscientiously may appear to be less effective if fidelity is overlooked, leading to inappropriate decision by clinicians about whether to use that strategy in their practice.
With the exception of Sciberras et al. (2020), at 12 months, the longest time period between intervention cessation and final follow-up was 6 months. Results from this study suggest sustained benefits are possible, however, further research is required to determine whether sustained improvements are found consistently.
Lastly, deeper analysis into the possibility of individual differences in the child’s life affecting their response to treatment is suggested. For example, many studies included participants with comorbid disorders, such as other behavioral disorders, or mood disorders (Corkum et al., 2016; Hiscock et al., 2015; Sciberras et al., 2011, 2020; M. D. Weiss et al., 2006). It may be beneficial to ascertain whether the co-occurrence of these conditions affects intervention implementation and response to treatment and whether adjustments are required to account for such conditions. Further, current research has found that improvements in sleep can improve ADHD symptoms (Hiscock et al., 2015), however, it is also important to assess if improvements in sleep can reduce symptoms associated with comorbid conditions.
Sleep problems are common for children with ADHD and can significantly impact both the child and their families. All reviewed interventions displayed improvements in sleep, however, due to varying risk of bias and quality of evidence, results should be interpreted with caution. Though there are common intervention strategies, the particular successful elements of the intervention could not be ascertained. Furthermore, due to the complex natures of ADHD and sleep problems independently of each other, when experienced together it can be challenging to ascertain the best treatment. However, behavioral sleep interventions show promise in improving sleep in children aged 5 to 15 years with ADHD, with some evidence from our review suggesting that brief intervention can be effective if it is individualized. Further research opportunities are abundant in areas such as the complex relationship between ADHD medications and sleep, the utility of a stepped care approach, and the exploration of online intervention delivery.
Supplemental Material
sj-docx-1-jad-10.1177_10870547221106239 – Supplemental material for Behavioral Sleep Interventions for Children With ADHD: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-jad-10.1177_10870547221106239 for Behavioral Sleep Interventions for Children With ADHD: A Systematic Review and Meta-Analysis by Maya K. Malkani, Carmela F. Pestell, Andrew M. C. Sheridan, Alison J. Crichton, Georgia C. Horsburgh and Romola S. Bucks in Journal of Attention Disorders
Supplemental Material
sj-docx-2-jad-10.1177_10870547221106239 – Supplemental material for Behavioral Sleep Interventions for Children With ADHD: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-jad-10.1177_10870547221106239 for Behavioral Sleep Interventions for Children With ADHD: A Systematic Review and Meta-Analysis by Maya K. Malkani, Carmela F. Pestell, Andrew M. C. Sheridan, Alison J. Crichton, Georgia C. Horsburgh and Romola S. Bucks in Journal of Attention Disorders
Supplemental Material
sj-docx-3-jad-10.1177_10870547221106239 – Supplemental material for Behavioral Sleep Interventions for Children With ADHD: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-jad-10.1177_10870547221106239 for Behavioral Sleep Interventions for Children With ADHD: A Systematic Review and Meta-Analysis by Maya K. Malkani, Carmela F. Pestell, Andrew M. C. Sheridan, Alison J. Crichton, Georgia C. Horsburgh and Romola S. Bucks in Journal of Attention Disorders
Supplemental Material
sj-docx-4-jad-10.1177_10870547221106239 – Supplemental material for Behavioral Sleep Interventions for Children With ADHD: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-4-jad-10.1177_10870547221106239 for Behavioral Sleep Interventions for Children With ADHD: A Systematic Review and Meta-Analysis by Maya K. Malkani, Carmela F. Pestell, Andrew M. C. Sheridan, Alison J. Crichton, Georgia C. Horsburgh and Romola S. Bucks in Journal of Attention Disorders
Supplemental Material
sj-docx-5-jad-10.1177_10870547221106239 – Supplemental material for Behavioral Sleep Interventions for Children With ADHD: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-5-jad-10.1177_10870547221106239 for Behavioral Sleep Interventions for Children With ADHD: A Systematic Review and Meta-Analysis by Maya K. Malkani, Carmela F. Pestell, Andrew M. C. Sheridan, Alison J. Crichton, Georgia C. Horsburgh and Romola S. Bucks in Journal of Attention Disorders
Footnotes
Data Availability Statement
Supporting data for this article can be made available by the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.