
Abstract
Objective:
Few studies of prescription stimulant non-oral, non-medical use (NMU) (defined by use not as prescribed) have been conducted in adults beyond the college population. The purpose of this study was to characterize prescription stimulant non-oral use, specifically intranasal (IN) use (snorting) in young adults.
Method:
Amazon’s MTurk platform was used to recruit participants for an online survey. Data were collected from March to April 2020.
Results:
Thirty-two percent (n = 157) of survey respondents (N = 975), aged 18 to 30, reported IN prescription stimulant use (average of 32.1 episodes of lifetime IN use). Adderall was the most-reported prescription stimulant used intranasally (89.2%). Most IN users (82%; n = 68) reported spending no more than 5 minutes tampering with prescription stimulants. Intranasal users said they would take the medication orally if unable to tamper or manipulate medication for IN use.
Conclusion:
These data help quantify a complex public health issue of ongoing IN use of prescription stimulants and suggest a potential role for manipulation-deterrent medications.
Introduction
Prescription stimulants (amphetamines and methylphenidates) are the most widely used class of medications prescribed for the treatment of ADHD (Clemow & Walker, 2014; Faraone et al., 2020). Recently, the National Survey on Drug Use and Health found among individuals aged 12 or older, 1.8% (or 5.1 million people) engaged in prescription stimulant misuse in the past year (2020) (SAMHSA, 2021). Prescription stimulant misuse, herein referred to as nonmedical use (NMU), is defined as use not as prescribed (SAMHSA, 2021). It includes both oral and non-oral routes of administration (Cassidy, Varughese et al., 2015; Faraone et al., 2020; Garnier-Dykstra et al., 2012; Weyandt et al., 2013), such as taking more medication than prescribed, in a way other than prescribed or via a non-oral route, such as intranasal (IN) use or intravenous (IV) use. As an indication of public health concern, a recent FDA Federal Register solicited new or additional information and perspectives on prescription stimulant misuse and abuse and associated harms (Schiller, 2019).
Reports of NMU persist in the scientific literature and in the popular press (Arria et al., 2011; Faraone et al., 2020; Friedman, 2010; Garnier-Dykstra et al., 2012; Italiano, 2011; McCabe & West, 2013; McCabe et al., 2004, 2005, 2006b, 2009; Peltz, 2012; Pratt-Kielley, 2020; Schepis, Ford et al., 2020; Schepis, Klare et al., 2020; Swanson & Volkow, 2008; Wilens et al., 2020). Prescription stimulant NMU has been associated with a number of risks that have been epidemiologically reported including behavioral risks such as possible off-label use (Burcu et al., 2016), diversion (Compton et al., 2018; Han et al., 2017), or dating violence (Whiteside et al., 2015), health risks such as aortic dissection (Westover & Nakonezny, 2010), acute myocardial infarction (Westover et al., 2008), or psychiatric disorders (Wilens et al., 2020) among others (Faraone et al., 2019, 2020). While the existence of non-oral NMU is well-documented, details surrounding use with specific routes of administration (ROAs) are less well understood.
Non-oral NMU has been examined in adolescents and college students (Arria et al., 2011; Arria, Caldeira, Vincent, et al., 2017; Arria et al., 2018; Austic, 2015; Cottler et al., 2013; DeSantis et al., 2008; Desantis et al., 2009; DeSantis et al., 2010; Dupont et al., 2008; Garnier-Dykstra et al., 2012; Lasopa et al., 2015; Lookatch et al., 2012; McCabe & Teter, 2007; McCabe et al., 2004, 2005, 2006b, 2011a; Rabiner et al., 2009a, 2009b, 2010; Schepis, Ford et al., 2020; Setlik et al., 2009; Teter et al., 2003, 2006, 2010; Vosburg, Faraone et al., 2021; Vrecko, 2015; Wang et al., 2015; Wilens et al., 2006, 2020). Fewer studies have been conducted with adult samples recruited beyond the college setting (Burtner et al., 2018; Cassidy, McNaughton et al., 2015; Cassidy, Varughese et al., 2015; Compton et al., 2018; Novak et al., 2007; Schepis, Klare et al., 2020; Schepis & McCabe, 2016). There is an increasing awareness that ADHD can persist throughout the adult years (Castells et al., 2018; Goodman, 2007; Goodman et al., 2016; Goodman, 2016), creating the potential for both NMU (McCabe et al., 2014; Poulin, 2007) and non-oral use of prescription stimulant medications in adults. This is an area in need of further research.
Recent estimates are that ~0.55 million to 2 million adults use prescription stimulants intranasally each year (Faraone et al., 2020). IN use of prescription stimulants is associated with a rapid onset of physical and subjective effects (Lile et al., 2011; Stoops et al., 2003). Rapid onset of effects is linked to reinforcing effects and substances being considered as “addictive” (Compton & Volkow, 2006), which is a fundamental risk associated with non-oral use. Further, IN use of prescription stimulants is associated with medical risks ranging from being more likely to be admitted to a critical care facility, to adverse clinical effects and even death (Faraone et al., 2019; Massello & Carpenter, 1999) .
Another aspect associated with non-oral use is medication tampering—the process by which a substance, such as a tablet or capsule, is reduced to a form, such as a powder, that can be taken non-orally by an alternate route, such as intranasal administration. Although identified with prescription opioids (Katz et al., 2011), medication tampering also takes place with prescription stimulants (Vosburg et al., 2020). To address the need for information, the purpose of the present study was to characterize non-oral use, and specifically, IN use in an adult sample. This is important both for provider awareness and for targeted prevention efforts surrounding recognition and management of prescription stimulant misuse (Schedule II medications) (Schiller, 2019; Wilens & Kaminski, 2020).
Methods
Amazon.com’s Mechanical Turk (MTurk: https://www.mturk.com/) crowdsourcing platform was used for participant recruitment (Chandler & Shapiro, 2016; Strickland & Stoops, 2019; Strickland & Victor, 2020) during an approximately 2-month period between March and April 2020. The MTurk platform connects businesses with a need for rapid task completion of often difficult tasks to large numbers of individuals with the skills to complete the required work (Strickland & Stoops, 2019; Strickland & Victor, 2020). The tasks are referred to as Human Intelligence Tasks, or HITS. The HITs are broken down into incremental tasks that can be completed by multiple individuals at once. Common reported benefits of using MTurk for research purposes include enhanced participant diversity, reduced cost and faster data collection. MTurk is particularly useful in reaching hard-to-sample populations, such as substance users (Strickland & Stoops, 2019; Strickland & Victor, 2020).
As a group, MTurk workers tend to reside in the US or India (Chandler & Shapiro, 2016). They are mostly young: almost a third are between 18 and 29 years of age (31.2%) and 70% are under the age of 40 (Chandler et al., 2019). Most are male (Arechar & Rand, 2021), non-Hispanic (92.1%), white (75.3%), have incomes up to 39K per year (37.2%) or 40K to 79K per year (40.9%), single never married (50.8%) and without children (60.0%). More than half indicate they are not religious (45.3%) or, they consider themselves to be religious, but it is not important to them (13.2%). Over half (56.2%) consider themselves as politically liberal, and almost all (92.1%) are registered to vote (Chandler et al., 2019).
MTurk served as a portal for the eventual survey that was completed through Qualtrics Online Survey Software. It also distributed compensation payment to participants who completed either the screening or the entire survey. The present study’s survey opportunities (Human Intelligence Tasks: HITs) were posted in “batches” of approximately 200 to ensure the HIT was higher up on the list of available work opportunities and therefore found and completed in a timely manner by interested individuals.
The title of the survey (the HIT) was “($3.95 Bonus) Answer questions about your use of substances and stress.” Potential participants clicked the title after which they could read a cover letter describing the research and indicate their agreement to continue participation in the online survey. They were told that they would be asked to answer questions regarding stress, substance use, and decision making, and a brief demographic survey would determine their eligibility at the start of the survey. Potential participants were also told they would receive $0.05 in Amazon credits for completion of the brief screening survey and a $3.95 Amazon credit bonus if they qualified and completed the remainder of the survey. The survey was described as taking approximately 1 to 30 minutes depending on their eligibility. Potential participants were also provided with the contact information for the Principal Investigator of the study, as well as the University of Kentucky Office of Research Integrity and encouraged to contact these individuals if they had any concerns.
Procedures
Individuals with MTurk accounts can view available projects that require work to be performed by humans (HITs). Eligibility to view the present study was granted to individuals who had: received a 95% or higher approval rating on all previously submitted work, participated in over 50 approved projects HITs and resided in the United States.
Potential participants completed a brief questionnaire asking about demographics. Age had to be reported as being between 18 and 30 years to be eligible to complete the full survey. Purposive sampling was undertaken because misuse of prescription stimulants is estimated to be most prevalent among ages 18 to 25 (SAMHSA, 2021), misuse has been estimated to peak at age 21 (CBHSQ, 2016), or, in more recent estimates, in the 21 to 25 age group (CBHSQ, 2021). The age range was extended to 30 to expand beyond the typical college age range but recruit an enriched sample that was likely to exhibit non-oral use (the behavior of interest). If individuals did not screen out of the study, they were presented with 288 questions that queried demographic characteristics, including trauma, prescription stimulant non-medical use (NMU), with a focus on non-oral use, tampering behaviors with prescription stimulant medications and behavioral health economic relationships. Specific survey questions about NMU, IN Use and tampering appear in Table 1. At the end of the screening process or the completed survey, participants received payment codes. The University of Kentucky Medical IRB reviewed & approved this study.
Survey Questions Used to Identify Prescription Stimulant NMU and IN use.

Note. The same series of questions was posed about injecting and vaping.
Analyses
Data were descriptively summarized with Microsoft Excel v. 2019 and IBM SPSS Statistics (v. 20). Demographics are presented for the group of survey respondents who endorsed any prescription stimulant NMU (n = 496) and for the group of survey respondents who endorsed any prescription stimulant IN use (n = 157), which is a subset of the “Any NMU” group. To investigate whether there were any potentially meaningful differences in demographic characteristics, chi-square analyses were conducted between the n = 157 individuals who reported prescription stimulant IN use and the remaining n = 339 who reported prescription stimulant NMU but not IN use. Statistical significance was considered at p < .01 because of the sample size and multiple comparisons.
Results
Sample Demographics
Between March and April 2020, 975 individuals between the ages of 18 and 30 responded to and completed the Mturk platform survey. Approximately half of the survey respondents, n = 496 (51%) reported prescription stimulant NMU. Of these, n = 157 (32%) reported IN use of prescription stimulants. Table 2 summarizes the demographic characteristics and compares those who reported IN use (n = 157) and the remainder of the sample with NMU who did not report IN Use (n = 339). Both groups were primarily heterosexual, white, non-Hispanic males who were approximately 26 years of age, employed, and living with others (parents, spouses/partners, or friends/roommates). More individuals who reported IN use were divorced (6% vs. 2%), while fewer reported attending graduate school additional education (6% vs. 16%). Individuals reporting IN use reported more substance use than those without IN use, including marijuana (60% vs. 46%), tobacco cigarettes (35% vs. 14%), sedative/hypnotic/anti-anxiety medications (16% vs. 8%), opioids (11% vs. 3%), cocaine (18% vs. 2%), or methamphetamines (9% vs. 2%).
Demographics.
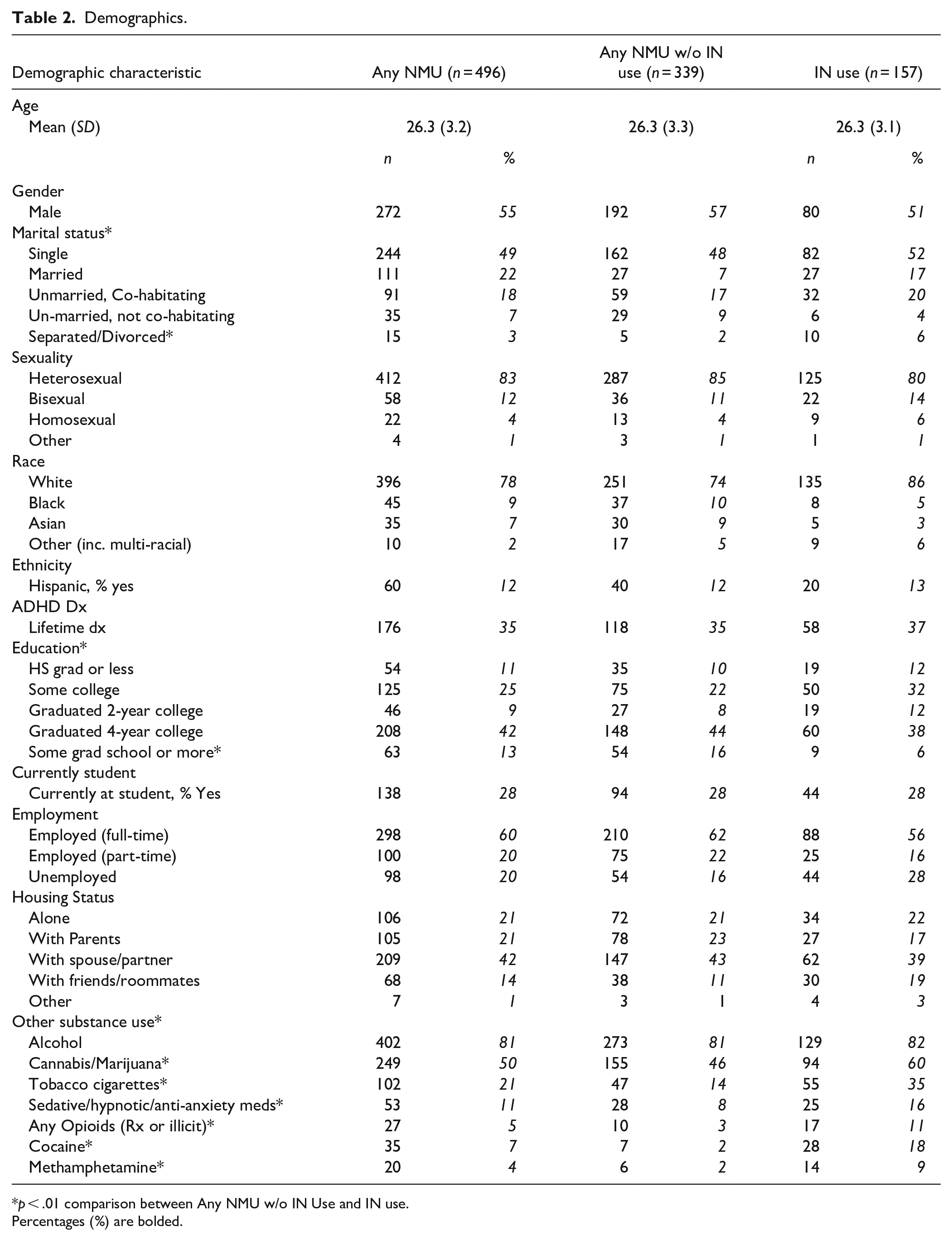
p < .01 comparison between Any NMU w/o IN Use and IN use.
Percentages (%) are bolded.
Individuals who reported lifetime IN use were asked to estimate the number of times in their lifetimes, number of days in the past month and number of days in the past week that they had undertaken prescription stimulant IN use. Table 3 summarizes these results. Individuals with IN use reported an average of 32.9 (Median 5.0) episodes of lifetime IN use, 6.04 (Median 2.0) episodes of past month IN use, and 2.0 (Median 1.0) episodes of past week use. Prescription stimulants were used intranasally to improve performance (n = 70, 45%), to get high (n = 35, 22%), to stay awake longer (n = 21, 13%), or to party (n = 11, 7%). Most individuals were given the medication for NMU from friends (n = 69, 44%), relatives (n = 3, 2%) or someone else (n = 4, 3%). If medication was purchased for NMU, it was typically purchased from a friend (n = 36, 23%), someone else who was not a relative (n = 20, 13%), or a relative (n = 5, 3%).
Characterizing Prescription Stimulant IN Use.

Doses and Amounts Used During IN Use
Participants were asked to indicate which prescription stimulants they used IN. Figure 1 summarizes that most (86.0%) of individuals who reported IN use of prescription stimulants used Adderall for IN use, Ritalin (14.6%) and Adderall XR (14.6%). Vyvanse was snorted by less than 10% of the sample (6.4%). Dexedrine and Concerta were each snorted by less than 2% of the sample.
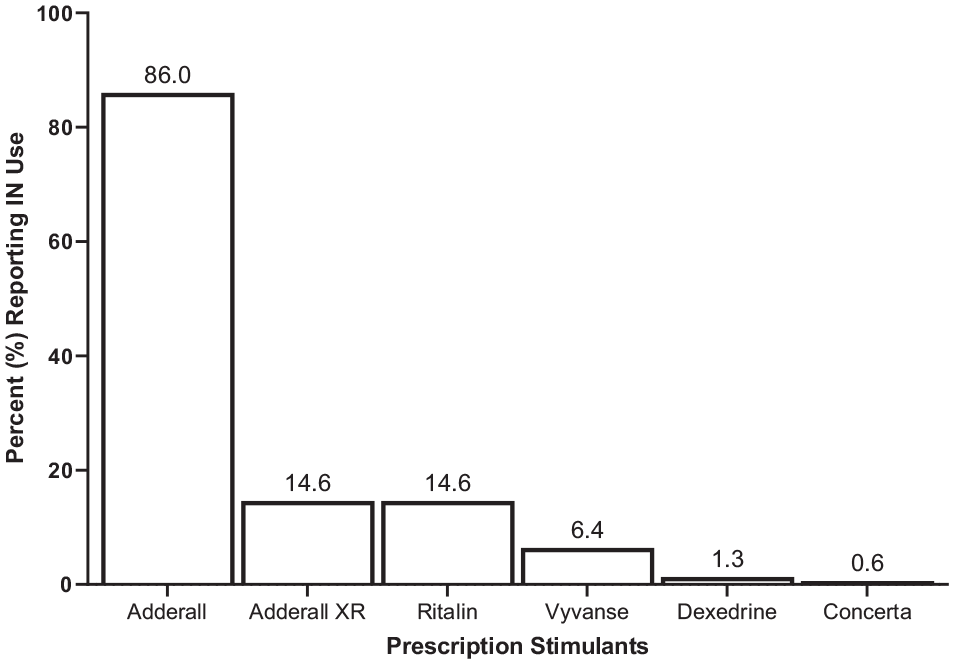
Prescription stimulants reported for IN use (n = 157).
Figure 2, top, depicts the doses of prescription stimulants most often employed for IN use of Adderall or Ritalin. Figure 2, bottom, indicates the amounts paid for doses purchased for IN use of Adderall or Ritalin. Most individuals reported using ≤30 mg of Adderall or Ritalin: 28.1% and 21.7% reported using up to 10 mg of Adderall or Ritalin, respectively; 16.3% and 34.8% reported using from 11 to 20 mg, and 20.7% and 13.0% reported using 21 to 30 mg of Adderall or Ritalin, respectively. Most individuals reported paying ≤$10.00 per dose. A substantial proportion obtained the medications for free (14.8% Adderall 21.7% Ritalin), while most others reported paying up to $5.00 a dose (32.6% Adderall, 30.4% Ritalin) or from $5.00 to $10.00 per dose (17.0% Adderall, 21.7% methylphenidate).
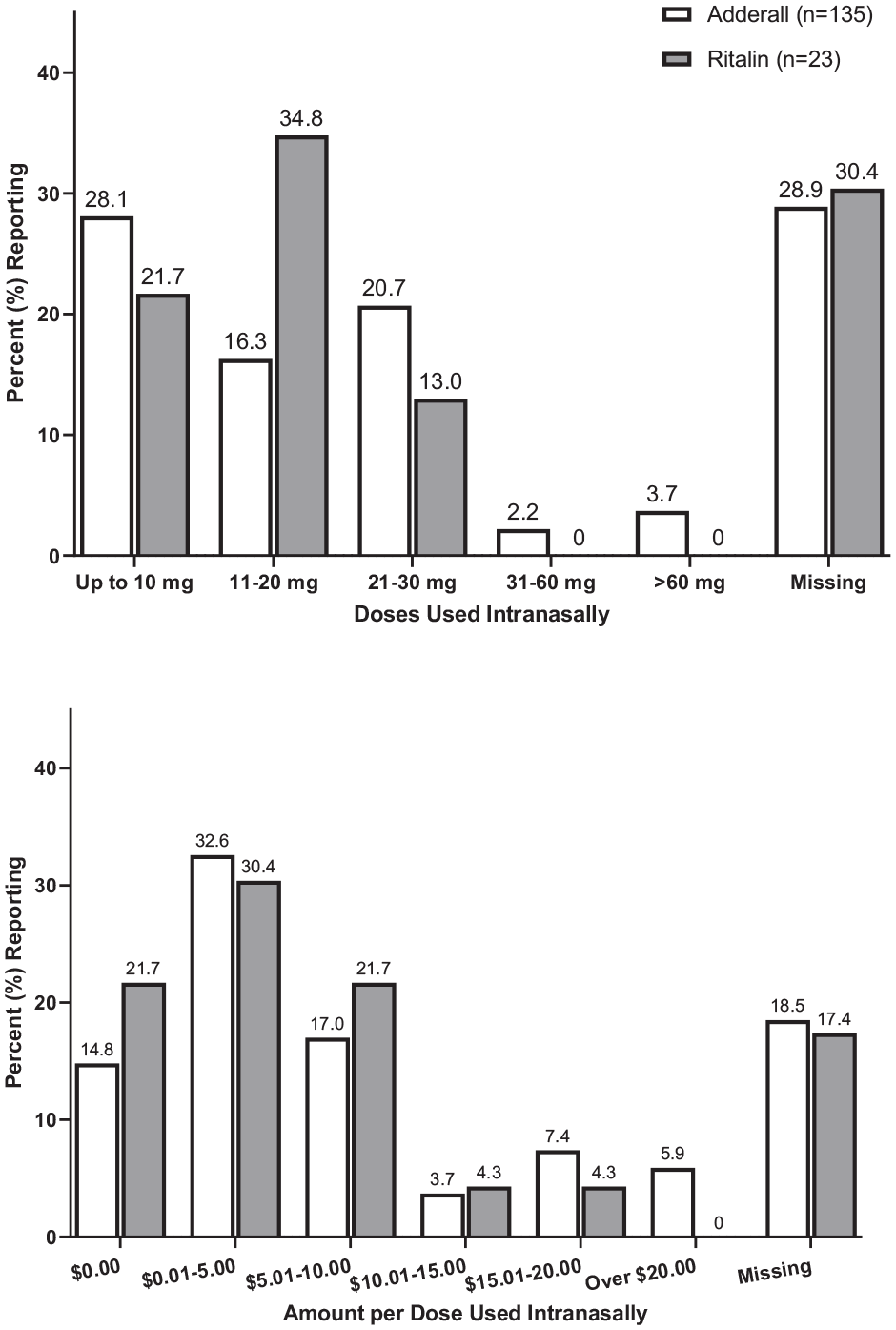
Doses and amounts paid for doses used intranasally.
Routes of Administration
IN use was the most frequently reported non-oral route of administration (n = 157, 32%). Vaping and IV use were infrequently endorsed: ~6% reported vaping (n = 28) and ~2% reported IV use (n = 8).
Tampering Behaviors for NMU
Participants were asked specifically to indicate the number of times they had tampered with or manipulated a prescription stimulant for IN (or IV) use, and the amount of time it typically took for them to prepare prescription stimulant medications for IN (or IV) use. Figure 3 depicts responses from respondents who reported both tampering with prescription stimulant medication and episodes of IN use; IV use is also presented for comparison. Figure 3 (top) depicts that slightly more than half of the n = 157 individuals who reported IN use reported tampering (54%, n = 84). Of these, half (50%, n = 42) tampered 5 times or less, while the remaining half tampered 6 times or more. The median number of times individuals reported tampering was 6, and the mean number of times individuals reported tampering was 35.1 (SD = 70.7) (Data not shown).
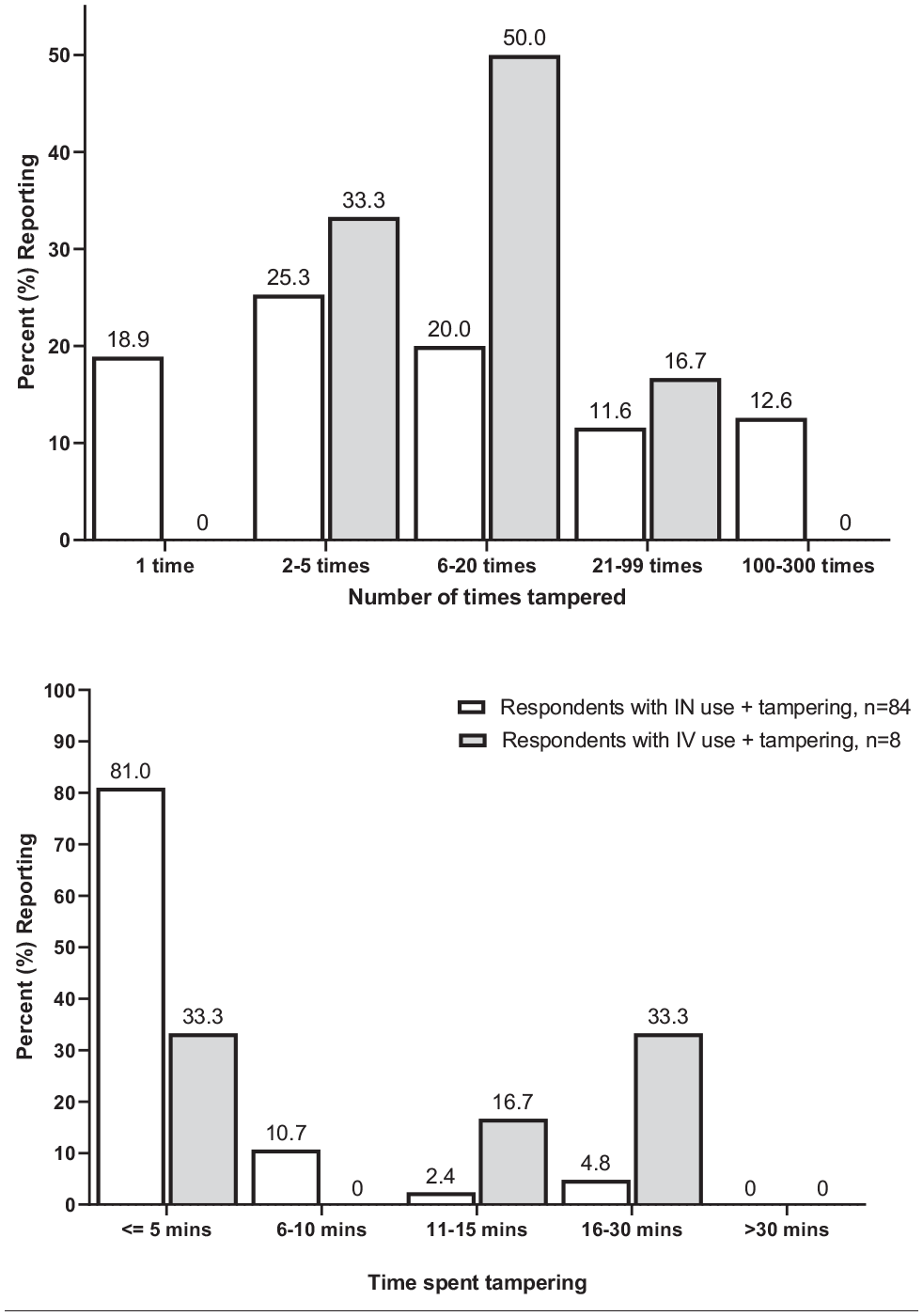
Number of times and length of time spent tampering with stimulant medications for intranasal (white bar) and intravenous (gray bar) use.
Figure 3 (bottom), shows that 82% (n = 68) of IN users reported spending no more than 5 minutes tampering with prescription stimulants and 11% reported spending between 6 and 10 minutes doing so. The median time spent tampering for IN use was 3 minutes and the mean time spent tampering was 4.9 (SD = 5.4) minutes (Data not shown). The median number of minutes spent tampering was 15.
If Medication Manipulation Were Not Possible
When asked what they would do if they had purchased a prescription stimulant with the intent of IN use and could not tamper or manipulate it for this purpose, most individuals with a history of intranasal use, n = 131 (83.4%) indicated that they would take the medication orally instead (among those who reported tampering and using intranasally, 89.3% indicated they would use orally). Other responses were to take nothing (n = 16, 10.2%), to try to prepare the prescription stimulant for injection (n = 7, 4.5%), or to take another drug instead (n = 3, 1.9).
Discussion
Prescription stimulant NMU has been associated with a number of risks that have been epidemiologically reported including behavioral risks such as possible off-label use (Burcu et al., 2016), diversion (Compton et al., 2018; Han et al., 2017), or dating violence (Whiteside et al., 2015), health risks such as aortic dissection (Westover & Nakonezny, 2010), acute myocardial infarction (Westover et al., 2008), or psychiatric disorders (Wilens et al., 2020) among others (Faraone et al., 2019, 2020). While the existence of non-oral NMU is well-documented, details surrounding use with specific routes of administration (ROAs) are less well understood.
The primary contribution of this study is to address the non-oral NMU of prescription stimulants, including questions about medication tampering. We focused on IN use because, after oral ROAs, IN use is the most widely reported prescription stimulant NMU ROA among adults (Burtner et al., 2018; Cassidy, McNaughton et al., 2015; Cassidy, Varughese et al., 2015). Individuals in the present study who reported prescription stimulant IN use also reported a greater degree of other substance use (marijuana, tobacco cigarettes, sedative/hypnotic/anti-anxiety medications, opioids, cocaine, and methamphetamines) similar to other samples reporting IN use (Faraone et al., 2019; McCabe & Teter, 2007; Wilens et al., 2020). The onset of additional substance use was not investigated in the present study, however, non-oral prescription stimulant use has been identified as a precursor to illicit substance use in other samples (Sweeney et al., 2013; Vosburg et al., 2020). This finding is also in keeping a reported trajectory of substance use that begins during college and continues into the young adult years (Arria, Caldeira, Allen, et al., 2017). Participants reported prescription stimulant IN use on a monthly basis. Previous reports have described individuals undertaking prescription stimulant NMU on an occasional basis (Schiller, 2019), and the present study could be considered as one possible operationalization of this term.
The primary source of diverted medication was family and friends, while most of the medication that was diverted was given or shared rather than purchased. Diversion is a public health concern because it is invisible (Garcia et al., 2022; Lam et al., 2020; Lasopa et al., 2015), and yet must be balanced with the recognized need and medical benefit of prescription stimulants. Most IN users reported performance enhancement as their primary reason for NMU (Compton et al., 2018; Faraone et al., 2020; Wilens et al., 2008), however, a sizeable proportion of IN users reported IN use to get high or to “party longer.” An interaction between route of administration and motivation for use has been recently reported in other literature and bears further examination to better characterize this relationship (Vosburg, Robbins et al., 2021).
Individuals who tampered with their medications reported using a range of doses, but most were in the low dose range (up to 30 mg). Time reported spent tampering for IN use was, for the most part, no more than 5 minutes, a similar time reported among individuals with prescription opioid IN use (Vosburg et al., 2012, 2013). These data support the notion that most IN use is typically conducted with regularly prescribed doses and quickly (Cone et al., 2013).
Prescription stimulants containing amphetamine are more prescribed (Safer, 2016; Scripts, 2014), arrive in more forensic laboratories (U.S. Drug Enforcement Administration Office of Diversion Control, 2012, 2021) and, in the present study, were endorsed for IN use more than medications with methylphenidate. Further, IR formulations were endorsed more than ER / long-acting formulations for IN NMU. Amphetamine has been reported as more liked than methylphenidate (Faraone et al., 2019), and, as such, is a ready candidate for non-oral NMU, without consideration of formulation, which is consistent with our findings.
Lastly, in a question addressing a significant concern accompanying the introduction of manipulation-resistant formulations (Cicero et al., 2012), most individuals reported that they would take a prescription stimulant orally if they could not tamper with the prescription stimulant medication that they had obtained. While these data are preliminary, that most would be unlikely to escalate their use is an encouraging finding that supports continued development of abuse deterrent products.
This study had limitations and unique contributions. The survey sample is a convenience sample, limited by the self-selection of participants and self-reported data (Mellis & Bickel, 2020). Not every individual who reported prescription stimulant non-oral NMU reported tampering with prescription stimulants. To address this data characteristic and to provide a more precise estimate of medication tampering, subgroups were formed with individuals who endorsed both characteristics. These limitations are balanced by several strengths. Even though a convenience sample (Mellis & Bickel, 2020), recruitment using the MTurk platform resulted in a larger sample size that enabled a sole focus on IN use. Benefits of using MTurk for research purposes include enhanced participant diversity, reduced cost and faster data collection (Strickland & Stoops, 2019) as well as it an effective tool for reaching populations that are underrepresented through traditional recruitment techniques (Chandler & Shapiro, 2016). Particularly relevant for the present study, rates of clinical diagnoses such as ADHD among samples recruited with MTurk have been reported as similar to other community samples (Chandler & Shapiro, 2016). While these findings are encouraging, they do not mean the present data are fully generalizable to the population of adult individuals who use prescription stimulants intranasally (McCredie & Morey, 2019; Mellis & Bickel, 2020). The data suggest, however, that non-oral use and prescription stimulant tampering is an area worthy of future study.
To the best of our knowledge, this is the first study that focused on querying specific medications, tampering times and dose associated with prescription stimulant intranasal use. This study was conducted in a sample that extended beyond the college age and was able to capture and model behaviors that are difficult to find. Our results indicate that prescription stimulant IN use is likely to occur beyond the college years with diverted IR amphetamine products (as opposed to methylphenidate products), in doses typically up to 30 mg. Prescription stimulant IN use is accompanied by medication tampering, although typically no more than 5 minutes are spent on preparing the capsule or tablet for IN use. If tampering were not possible, most individuals who report IN use report they would take instead take the medication orally. These data are important steps toward quantifying a complex public health issue (Arria & Compton, 2017): ongoing and risky IN use of prescription stimulant medications that are designed for oral use in a clinical population. Manipulation resistant medications may confer an advantage toward deterring the non-oral use of prescription stimulant medications.
Footnotes
Acknowledgements
The authors would like to acknowledge Jill Baker who provided initial data management and analysis for this manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Suzanne Vosburg is an independent scientific writer and consultant who contracts with multiple companies. In the past 36 months, Dr. Faraone received income, potential income, travel expenses continuing education support and/or research support from Aardvark, Rhodes, OnDosis, Tris, Otsuka, Arbor, Ironshore, KemPharm/Corium, Akili, Supernus, Takeda, Atentiv, Noven and Genomind. With his institution, he has US patent US20130217707 A1 for the use of sodium-hydrogen exchange inhibitors in the treatment of ADHD. He also receives royalties from books published by Guilford Press: Straight Talk about Your Child’s Mental Health, Oxford University Press: Schizophrenia: The Facts and Elsevier: ADHD: Non-Pharmacologic Interventions. He is Program Director of ![]() . Elizabeth Riley has no potential conflicts of interest to report. Tim Whitaker, Jessica Kardish, and David Baker are employees of Vallon Pharmaceuticals. Scott H. Kollins has no potential conflicts of interest to report. Craig R. Rush is a paid consultant for Vallon Pharmaceuticals.
. Elizabeth Riley has no potential conflicts of interest to report. Tim Whitaker, Jessica Kardish, and David Baker are employees of Vallon Pharmaceuticals. Scott H. Kollins has no potential conflicts of interest to report. Craig R. Rush is a paid consultant for Vallon Pharmaceuticals.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Vallon Pharmaceuticals (Philadelphia, Pennsylvania, USA). Vallon Pharmaceuticals funded this study and was involved with the initial study conceptualization and analysis. However, final data analysis, interpretation and writing up of results was the sole discretion of the authors. Vallon Pharmaceuticals reviewed the final manuscript.
Statement About Prior Postings and Presentations
Previous presentations: Poster presented at the 68th Annual AACAP Meeting (held virtually), October 18–30, 2021.
Poster presented at the APSARD 2022 Annual Conference (held virtually), January 14–16, 2022.
Clinical Trials Registration
This research was not a clinical trial; therefore, this survey was not registered with ClinicalTrials.gov.
Author Biographies
David Baker, MBA, is CEO of Vallon Pharmaceuticals. He has helped develop and commercialize multiple ADHD medications including Vyvanse®, Adderall XR®, Intuniv®, Mydayis®, Metadoxine XR, and ADAIR.He has worked at Vallon, Alcobra, Shire, and Merck.