
Abstract
Objective:
We aimed to assess the degree to which the American Academy of Pediatrics’ (AAP) clinical guidelines were followed when treating attention deficit/hyperactivity disorder (ADHD) in preschoolers.
Method:
Using Medicaid claims for children 4 to 5 years of age receiving their first dose of stimulants/alpha-2 agonists in 2017 (n = 836), we determined if BH was received prior to initiation of medication. We examined predictors after controlling for confounders.
Results:
More than half the sample did not receive first-line BH, which did not differ by demographics. Those receiving BH prior to medication had a higher rate of receiving an ADHD diagnosis. Only three diagnoses were significant in multivariate (OR 13.8, 95% CI [1.7–115.1]) analyses.
Conclusion:
More than half the sample did not, conservatively, meet the AAP clinical recommendations. Further research is needed to identify targets for intervention. Limitations are noted.
Attention deficit-hyperactivity disorder (ADHD) is one of the most frequently diagnosed neurodevelopmental disorders in children (Centers for Disease Control and Prevention, 2019b). For children ages 2 to 17 years, Kentucky ranked highest in the United States in the prevalence of ADHD (16.6%) and second in the prevalence of medication treatment for ADHD (6.4%) in 2011, which is the last year for which these data are available (Centers for Disease Control and Prevention, 2019a). There are approximately 300,000 children under age 6 years in Kentucky (U. S. Census Bureau, 2019) suggesting that there may be nearly 20,000 children (300,000 × 6.4%) being treated with stimulant medication. The total expenditure in 2016 for stimulant medications for all children on Kentucky Medicaid under 18 years of age was $215 million (Davis, 2017). It is not known if children in Kentucky differ from children in other states or if the high prevalence rates are due to differences in provider practices.
The American Academy of Pediatrics (AAP) has published guidelines recommending behavioral health (BH) interventions prior to prescribing medication for children 4 and 5 years of age (Wolraich et al., 2011, 2020). There are no recommendations for children less than four within this guideline. In a recent study of children ages 2 to 5 years who received Kentucky Medicaid and had a diagnosis of ADHD, 22% received at least one BH intervention as the only treatment and 28% received BH in combination with medication (Davis et al., 2020). However, that study did not examine the timing of medication initiation in relation to BH recommendations.
There are several reasons for concern regarding the diagnosis and treatment of ADHD in preschoolers. Of primary concern is the lack of evidence regarding the long-term effects of psychotropic medications on developing brains at such early stages of development (Davis & Williams, 2011; Ghuman et al., 2008; Johnston, 2004; Johnston et al., 2009). Another concern is related to the common use of “off-label” medications that have not been approved by the United States Food and Drug Administration (FDA) for that age or specific diagnosis, such as an alpha-2 agonist (Blum et al., 2018; Davis et al., 2019, 2020; Lohr et al., 2018). Two additional studies have shown that alpha-2 agonists are being used more frequently in younger (2–3 years) preschoolers compared to older (4–5 years) preschoolers (Blum et al., 2018; Davis et al., 2020). The long-term effects of these practices are unknown. However, one recent retrospective study of alpha-2 agonist use in preschoolers found this drug class safe and effective (Harstad et al., 2021). Large randomized clinical trials are needed to further determine the comparative effectiveness between alpha-2 agonists and stimulants (Harstad et al., 2021) and between behavioral health alone and with various medications. Lastly, diagnosing ADHD in preschoolers is difficult (Chacko et al., 2009; Parens & Johnston, 2009). Ambiguity in diagnosing ADHD in young children may relate to the wide range of individual differences in behavioral expression among typically developing children. This variation makes it hard to determine whether a behavior is atypical or within the range of behaviors that may be considered “normal” in young children (Davis & Williams, 2011; Martin, 2009). This difficulty in differentiating “normal” from atypical behavior, even between professionals, may result in over diagnosing of ADHD in preschoolers (Chacko et al., 2009; Parens & Johnston, 2009). In addition, professional guideline suggest that behavior ratings should be obtained from two or more settings, which may be difficult if children do not attend preschool. If a disproportionate number of children who do not attend preschool are from disadvantaged and minority-status families, the lack of an assessment in a preschool setting may delay diagnosis for some children, which could have long-term negative effects on their educational trajectories.
With the concern for over diagnosing ADHD, comes the problem of over medicating. Following the AAP guidelines, judicial medication use is recommended only after initiating BH treatment for 4- and 5-year-old children. Again, no recommendation has been made for children under 4 years of age within the AAP guidelines. A recent clinical trial for children 5 to 13 years diagnosed with ADHD (n = 127) found that those receiving BH were less likely to begin medication and, when initiated, used a lesser dose of medication (Coles et al., 2020). This reduction in use occurred without increases in symptomology and without an overall increase in cost because the cost of BH was offset by a reduction in medication and physician expenses (Coles et al., 2020). While these findings are encouraging, larger and more extensive studies with diverse samples are needed. No data were found describing the degree to which the AAP guidelines are being followed for this younger population. Therefore, the current study aims to examine the degree to which preschool children receive BH prior to medication and factors associated with using BH.
Methods
Study Design and Data Source
We performed a cross-sectional secondary data analysis utilizing the Kentucky Medicaid claims records from 2015 to 2017 (provided by the Kentucky Cabinet for Health and Family Services, Department of Medicaid Services). These data include all medical and pharmacy claims billed through Kentucky Medicaid insurance with health service information such as service date, provider type, and associated diagnosis codes, procedures, and prescriptions. Additionally, the data contain patient demographic information such as age, sex, date of birth, self-identified race and ethnicity, and residence zip code. The data belong to the Kentucky Department of Medicaid Services and cannot be shared without their explicit permission. The study was approved by the Institutional Review Board at the University of Louisville.
Cohort Composition
There were 693,942 Kentucky Medicaid enrollees for children under 18 years of age in 2017. We included in our analysis children aged 4 to 5 years who had their first dose of stimulants and/or alpha-2 agonists in 2017 (n = 1,863). Of these, we exclude children in the foster care system (n = 135) due to the practice of “bundling” the payments for some services for these children. Children with a previous history of receiving stimulant(s) and/or alpha-2 agonists from 2015 to 2016 were also excluded. Our cohort included only children with continuous enrollment with Medicaid for 3 years from 2015 to 2017 with maximum gap in coverage of no more than 4 days. We then reviewed the data retrospectively from 2017 to determine if behavioral therapy was received prior to receipt of medication. Children who received behavioral therapy after medication were excluded (n = 72), resulting in our analytic cohort of children (n = 836; see Figure 1). Children who received behavioral therapy prior to medication (n = 352; 42.1%) were compared to those who received only medication (n = 484; 57.9%).
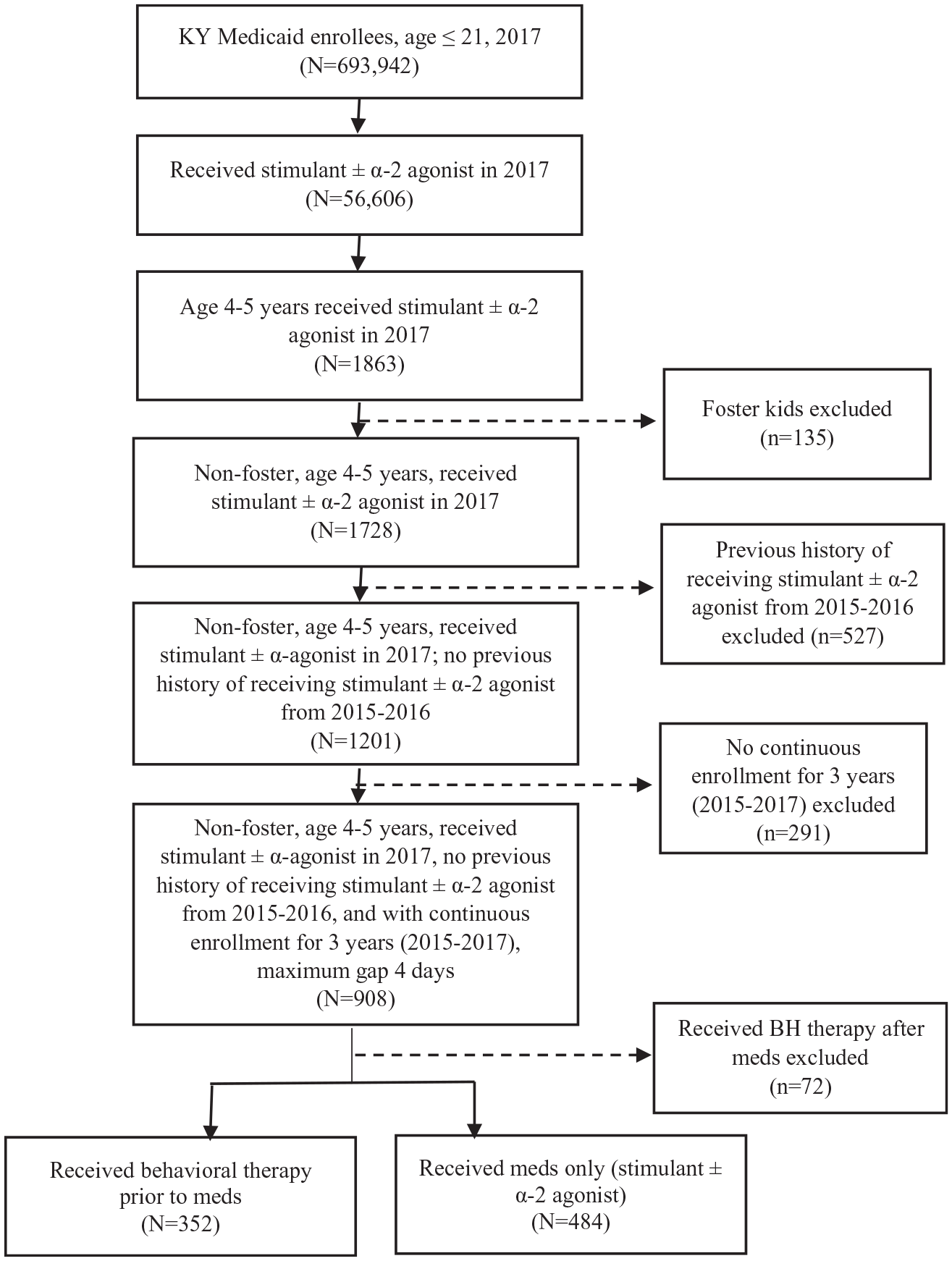
Analytic sample inclusion/exclusion flow chart.
Definitions and Diagnosis
We identified diagnoses using the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes within the medical claim records. Psychiatric cases were identified by an ICD-10 code for each of the psychiatric disorders in any of the four available diagnostic code fields on either inpatient or outpatient claims, rather than using the primary diagnostic field only. A full list of the ICD codes can be found in Appendix 1 (Supplemental table).
Behavioral therapy was defined as the child receiving a behavioral health intervention at least once within the year as indicated by a medical claim. Behavioral health interventions were identified in the medical claims by one of the following Current Procedural Terminology (CPT) codes: 90832-34, 90836-40, 90840, 90845-49, 90853, 90875-76, and 90880. These codes included both inpatient and outpatient visits and visits for individual or/and group therapy.
Psychotropic medications were verified by two child and adolescent psychiatrists and indicated by the National Drug Code (NDC) description found in Medicaid pharmacy data (see Supplemental table). Psychotropic medications other than stimulants and alpha-2 agonists, were defined in the following categories: antipsychotics, antidepressants, mood stabilizers, and anxiolytics (benzodiazepines and hypnotics).
Annual Kentucky Medicaid enrollment data files for 2012 to 2017 provided race and ethnicity and sex. Race and ethnicity were grouped as follows: non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, non-Hispanic other (including American Indian, Native Hawaiian, and other races), and Hispanic. Geography of child residence was defined as urban or rural using the 2013 Rural Urban Continuum Codes (RUCC). As defined by the U.S. Department of Agriculture, county of residence with RUCC of 1 to 3 was classified as “urban” and 4 to 9 as “non-urban.”
Statistical Analysis
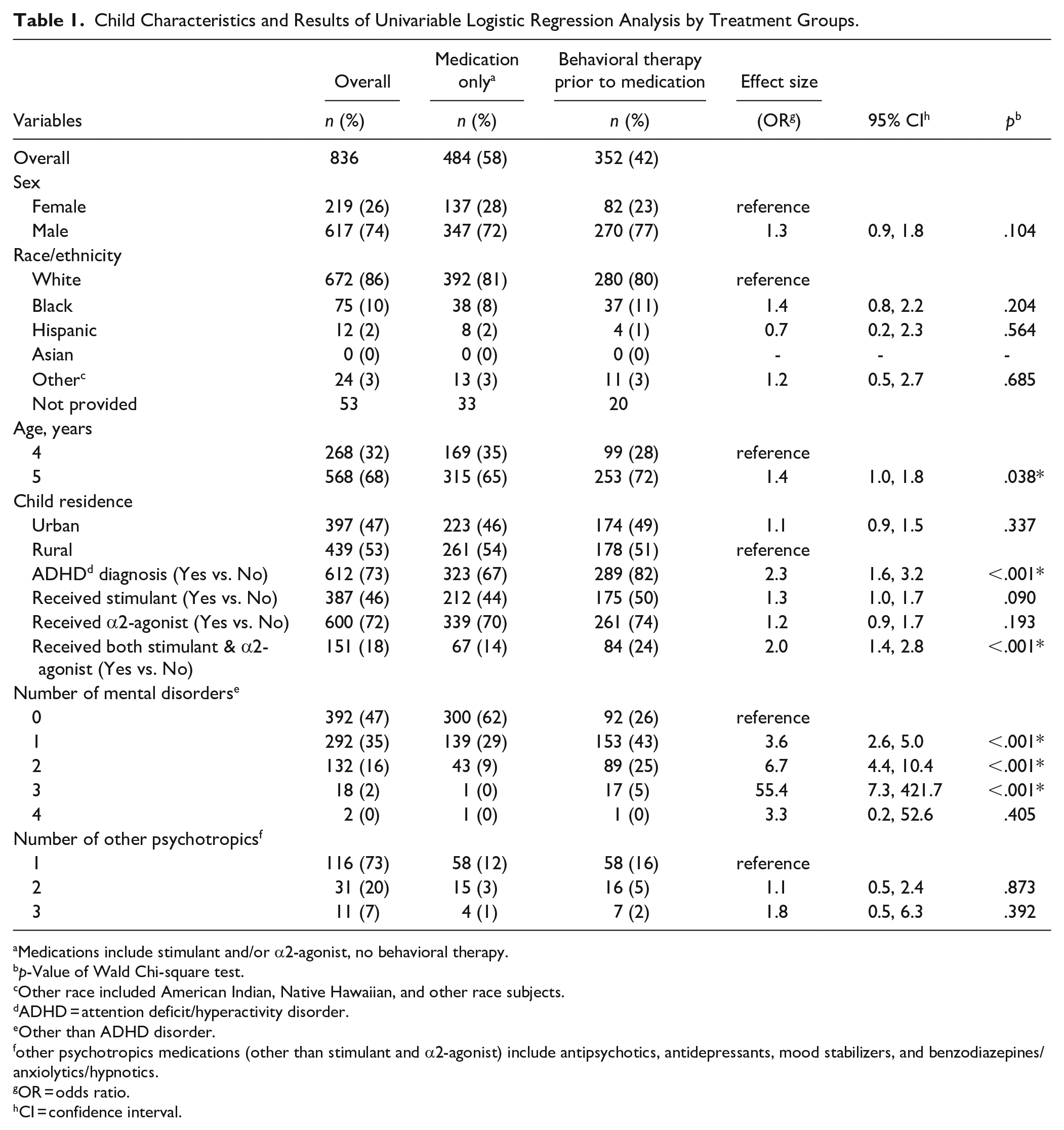
Descriptive analyses were performed to summarize the demographic characteristics and assess the difference between the two groups: children who received behavioral therapy prior to medication compared to those who received only medication (Table 1). Univariable logistic regression analysis was performed for comparison analysis and to examine for potential predictors for receipt of behavioral therapy prior to medications. Potential predictors included sex, race/ethnicity, child residence (urban/rural), receipt of both stimulant and alpha-2-agonist, having attention deficit/hyperactivity disorder (ADHD), number of mental disorders, and number of other psychotropic medications (defined above). Using a forward stepwise multivariable logistic regression model, statistically significant predictors were further analyzed, and adjusted odds ratios and their 95% confidence interval (CIs) were reported (Table 2). A two-sided p value <0.05 was considered statistically significant. Statistical analyses used SAS software (Version 9.4; SAS Institute Inc., Cary, NC, USA).
Child Characteristics and Results of Univariable Logistic Regression Analysis by Treatment Groups.
Medications include stimulant and/or α2-agonist, no behavioral therapy.
p-Value of Wald Chi-square test.
Other race included American Indian, Native Hawaiian, and other race subjects.
ADHD = attention deficit/hyperactivity disorder.
Other than ADHD disorder.
other psychotropics medications (other than stimulant and α2-agonist) include antipsychotics, antidepressants, mood stabilizers, and benzodiazepines/anxiolytics/hypnotics.
OR = odds ratio.
CI = confidence interval.
Odds Ratios—Univariate Logistic Regression Model.

OR = odds ratio.
CI = confidence interval.
ADHD = attention deficit hyperactivity disorder.
Other than ADHD disorder.
Results
Table 1 summarizes the cohort characteristics. In total, 352 (42%) children had received behavioral therapy prior to medication (stimulant and/or α2-agonist) in 2017, compared to 484 (58%) who received stimulant or alpha-2 agonist only. The sample was predominantly non-Hispanic White (86%), male (74%), aged 5 years (68%), and nearly half of the children lived in an urban area (Table 1).
In univariable analysis, an ADHD diagnosis, receipt of both stimulant and α2-agonist medications, and the number of mental disorders were shown to be statistically significant predictors of receipt of behavioral therapy prior to medication. After multivariable analysis, receipt of both stimulant and α2-agonist medications, and the number of mental disorders remained statistically significant predictors of receiving behavioral therapy prior to medication. Children were more likely to receive behavioral therapy prior to medication if they had received both a stimulant and an alpha-2 agonist (aOR: 2.9, 95% CI: 1.2, 7.0) and if they had three additional mental health diagnoses (aOR for three diagnoses: 13.8, 95% CI: 1.7, 115.1).
Discussion
While large, randomized clinical trials are needed to determine the safest, most effective, and cost-efficient management options, the current study fills a gap in the literature by describing the degree to which the AAP clinical guidelines are being followed related to the use of BH as the first-line treatment for preschoolers with ADHD receiving Kentucky Medicaid. Only 42% of the 4- to 5-year-old children in our sample received BH prior to medication despite our very conservative definition of at least one BH intervention in the 2 years prior. Children receiving both a stimulant and an alpha-2 agonist and children with three mental health diagnoses in addition to ADHD were more likely to have received BH prior to medication. While treating these children with more complex ADHD with BH is important, there are missed opportunities to treat all young children with first-line BH, which may reduce or eliminate the need for initiation of medication.
The AAP clinical practice guidelines suggest that a diagnosis of ADHD is not necessary to initiate parent training in behavior management (PTBM) as it is effective for all types of challenging behaviors (Wolraich et al., 2020). As discussed previously in this paper, there are some inconsistencies in diagnosing “abnormal” behavior in young children as there is a wide range of behaviors that may be considered “normal” (Chacko et al., 2009; Parens & Johnston, 2009). Numerous structural and environmental factors may interfere with the development of self-regulatory behavior, including attention regulation (Hodel, 2018), which can contribute to behavioral expressions that may be confused with ADHD. Children living in poverty, who are disproportionately of minority status, are at a greater risk of experiencing these environmental risks. Behavioral health interventions prior to medication may support the identification of modifiable environmental risk factors that may be contributing to differences in behavior.
For the same reason that there is concern related to the long-term effects of giving psychotropic medications to young children, developing brains are positively susceptible to the effects of non-pharmaceutical interventions (Belsky & Pluess, 2009; Mangina & Beuzeron-Mangina, 2004; Rosenzweig & Bennett, 1996). Specifically, the AAP recommends parent training in behavior management (PTBM) and/or behavioral classroom interventions as first-line therapy for children ages 4 to 6 years with a diagnosis of ADHD (Wolraich et al., 2020). According to the Centers for Disease Control and Prevention, only therapy that focuses on training parents is recommended for young children with ADHD because young children are not mature enough to change their own behavior without their parents’ help (Centers for Disease Control and Prevention, 2022b). Developed by Dr. Sheila Eyberg, Parent-Child Interaction Therapy (PCIT) is one evidence-based parent training program for children (PCIT-TCIT Training, 2021). Traditionally, PCIT is delivered in a clinic setting, with the therapist behind a one-way mirror providing live instruction and coaching during family interactions using a parent-worn earpiece (Comer et al., 2014; PCIT-TCIT Training, 2021). Delivery has now been expanded to include additional formats (Beveridge et al., 2015; Comer et al., 2014). These behavioral strategies improve family functioning and, therefore, may moderate the need for medication in young children.
Lastly, more research is needed to inform the development of family-centered interventions and strategies to engage families in behavioral parent training (Spencer et al., 2021). Much remains unknown about the timing, dose, duration, and delivery method (face-to-face, virtual, or combination) (DuPaul et al., 2018; Spencer et al., 2021; Tarver et al., 2022). Spencer et al. (2021) developed a framework describing six stages of engagement in care for children with ADHD. The framework suggests that parents must be supported in resolving barriers in each stage before they can be successful in navigating subsequent stages (Spencer et al., 2021). The framework also provides important considerations for ensuring that the provider and the caregiver are aligned in their understanding and acceptance of the problem, the treatment goals, and the treatment options (Spencer et al., 2021). For example, if a parent has concerns about stigma and discrimination, these issues must be addressed before the parent can be totally engaged in the treatment protocol. This concern may be addressed by providing antiracism training to providers, discussing common misconceptions about ADHD, and focusing on ways to minimize stigma (Spencer et al., 2021). The six stages of engagement framework identifies some important considerations, but more research is needed with larger samples to validate the phases and to better understand the drivers that move caregivers along the continuum.
Although we present new findings related to the receipt of BH for preschoolers with ADHD, this study has some limitations. Administrative claims data are known to have limitations (Research Data Assistance Center, 2018), including that data are captured only when a claim is submitted. For some services known to be frequently denied or for which reimbursement is low, such as psychosocial care, a claim might not be submitted (Research Data Assistance Center, 2018). In addition, if payments are “bundled” for groups of services, a claim is not filed. The bundling of services is known to occur for some children in foster care, such as those in residential facilities. Data cannot be captured to determine if BH was prescribed, but parents chose not to complete it, if parents were on a waitlist to receive BH therapy, or if services were provided through a program that does not direct-bill for services. Children in foster care were excluded from our sample due to the provision of “bundled service” for this population. Data on the types of services provided or the quality of such services are unavailable. Claims data also offer little insight into disease characteristics, severity, symptoms, etc. (Research Data Assistance Center, 2018). We identified cases if a child had one medical claim with a diagnosis of ADHD. Using only a single claim could result in overreporting due to coding errors or use of codes when ruling out the diagnosis of ADHD. Another limitation is that race/ethnicity is an optional field in the claims data. As such, 6% of our sample had unknown race/ethnicity. In addition to the limitations of the dataset, we coded the area of child residence as urban/nonurban. Future studies would benefit from a finer examination of geographic location, as well as an examination of available community resources, such as pediatric mental health providers within a 50-mile area. More specific assessment of the characteristics of available behavioral health services, such as timing, duration, quality, provider type, whether the behavioral health therapy was behavioral parent training, and specific components of the intervention, would also strengthen future studies.
Lastly, the data represent only one state, and it is not known whether the findings are generalizable to other states. While Kentucky, in general, is a poor state, the children on Kentucky Medicaid would likely be of a similar socioeconomic status as children on Medicaid in other states.
Despite the limitations, the current study provides new information that has important policy and practice implications. In Kentucky, 82% of the counties do not have a child and adolescent psychiatrist and the remaining 18% are considered shortage areas (American Academy of Child & Adolescent Psychiatry, 2017; Davis et al., 2020). More importantly, for this group of children, 44% of the counties in Kentucky do not have a pediatrician and another 21% have three or fewer pediatricians per 10,000 children aged birth through 17 years (Centers for Disease Control and Prevention, 2022a). Likewise, 40% of the counties do not have a child psychologist (Centers for Disease Control and Prevention, 2022a). Although these data are helpful, they may not provide the granularity needed to fully capture the resource deficits to serve this population. Mental health professionals with expertise in assessing and treating children, especially young children, with mental health concerns, are needed. Therefore, one policy implication is for pediatric mental health workforce development. More qualified professionals are needed to evaluate and treat young children and to support their caregivers to meet the growing demand for mental health services and to provide those services earlier. Ways to address this shortage could include additional pediatric mental health training for nurse practitioners, pediatricians, and clinical psychologists, as well as providing incentives for providers to enter these fields. Related to workforce development, enhanced reimbursement has the potential to attract more professionals to provide pediatric mental health services. Although data are not available for many services, there is some evidence that pediatric mental health services are reimbursed at a lower rate that other services (Herndon et al., 2020).
Another area for prevention of disruptive behavior is ongoing psychoeducation for both parents/caregivers and teachers. A greater understanding of the complex array of factors that may influence the regulation of attention and behavior may identify modifiable environmental factors that can be addressed such as sleep hygiene, diet, and stress; to name a few. There is a growing body of literature supporting the need to imbed BH interventions within primary care settings to improve access and acceptability and to minimize the stigma associated with seeking mental and behavioral health services (Sheldrick et al., 2022; Walter et al., 2019). Again, more data are needed to determine optimal intervention strategies.
More data are needed on the barriers to receiving BH services. There is a large literature related to effect of stigma on help-seeking behavior for mental health problems (Cheng et al., 2013; Cooper et al., 2003; Corrigan, 2004; Zhang et al., 2019). Concerns over stigma are intensified for children with behavioral and mental health problems as the parent may have concerns regarding stigma toward themselves as well as stigma toward their children (Dempster et al., 2013, 2015; Hinshaw, 2005) and there is additional complexity related to stigma in ethnic/racial minority-status families (Corrigan & Watson, 2007; Turner et al., 2015; Xu et al., 2018; Zhang et al., 2019). Integrated BH treatment within the primary care setting has been implemented to reduce the experience of stigma, provide greater access, and to minimize health disparities in the uptake of mental health services (de Voursney & Huang, 2016; Olufs et al., 2016; Wissow et al., 2017, 2021).
Telehealth is growing in acceptability due, in part, to the global pandemic. Telehealth can potentially to increase access to care for those in low-resourced areas (Contreras et al., 2018; Pradhan et al., 2019). It may also provide a platform for those who prefer a more confidential or private setting. The American Academy of Child and Adolescent Psychiatry (2017; AACAP Committee on Telepsychiatry and AACAP Committee on Quality Issues, 2017) updated their practice parameters to allow greater use of telepsychiatry after reviewing the available evidence. A systematic review demonstrated a broad-base of evidence for the efficacy of PCIT in various settings, including the home (Matos et al., 2009). More recently, research shows that PCIT is particularly amenable to a telehealth format (Comer et al., 2014). PCIT researchers have developed Internet-delivered PCIT (iPCIT), a telehealth format of PCIT using videoconferencing with promising outcomes in overall family functioning (Gurwitch et al., 2020). While literature is quickly emerging related to the use of telehealth for a variety of childhood mental and behavioral health concerns (Agazzi et al., 2021; Camden et al., 2020; Gurwitch et al., 2020; Tse et al., 2015), more data are needed to address current telehealth policies, billing procedures, and the barriers to technology utilization especially in the context of rural and low-resourced neighborhoods and families with low income, education, and/or literacy levels.
Our study shows that many preschoolers in our sample with ADHD do not receive behavioral therapies prior to stimulant or alpha-agonist treatment. Failure to receive these behavioral therapies represent missed opportunities to recognize and address modifiable risk factors that can improve child and family functioning and moderate the use of psychotropic medications in this population. This is particularly concerning in this sample of children from low-income families as they are more vulnerable due to poverty, which differentially impacts racial/ethnic minorities leading to health inequities. More research is needed to ensure that programs are tailored to the needs of the families, which may include neighborhood access, more racial/ethnic providers, and other factors to improve parental engagement of both mothers and fathers (Chronis et al., 2004). Additional information is needed to understand the reasons for delays in BH referrals, potential bias in referrals for BH, and the barriers to access, implementation, and uptake of BH therapies.
Supplemental Material
sj-docx-1-jad-10.1177_10870547221147543 – Supplemental material for First-line Behavioral Health Treatment Prior to Stimulant or Alpha-2 Agonist Use for Preschoolers on Kentucky Medicaid in 2017
Supplemental material, sj-docx-1-jad-10.1177_10870547221147543 for First-line Behavioral Health Treatment Prior to Stimulant or Alpha-2 Agonist Use for Preschoolers on Kentucky Medicaid in 2017 by Deborah Winders Davis, Kahir Jawad, William David Lohr, Marie Trace, Jennifer Le, Yana Feygin and Veronnie Faye Jones in Journal of Attention Disorders
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded, in part, by a State-University Partnership with Kentucky Medicaid. The study sponsor had no involvement in the (1) study design; (2) the collection, analysis, and interpretation of data; (3) the writing of the report; or (4) the decision to submit the paper for publication.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.