
Abstract
Objective:
To estimate the prevalence of PDs according to Millon’s evolution-based model among adult ADHD outpatients.
Method:
Cross-sectional study of consecutive patients referred to an adult ADHD clinic. PDs were evaluated with Millon Clinical Multiaxial Inventory–III (MCMI-III).
Results:
One-hundred-eighty-one participants had valid MCMI-III, of whom147 were diagnosed with ADHD. Mean age: 32.97, SD:11.56, females: 74 (50.3%). Among the 147 participants with ADHD, 29 (19.7%) did not meet criteria for any PD, 43 (29.3%) met the criteria for one PD, 34 (23.1%) for two PDs and the rest three or more. Most common PD was Dependent (n = 58) followed by Depressive (n = 45). Inattentive sub-type was associated with dependent PD, while combined type with antisocial, negativistic (passive/aggressive) and sadistic PD.
Conclusion:
Particular personality profiles were more common with different ADHD subtypes. Given the developmental origins of PD, further research may help identify possible links with childhood difficulties.
Introduction
Attention Deficit-Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder manifested in childhood and characterized by either significant symptoms of inattention or hyperactivity and impulsiveness, or a combination of the two. Although it has been seen as a disorder of childhood, evidence is evolving of persistence into adult life and about 60% of cases continue to be impairing during adulthood (Kooij et al., 2010; Turgay et al., 2012). However, the clinical presentation changes throughout the lifespan. Symptoms of hyperactivity/impulsivity are more likely to decline with increasing age while inattentiveness is more likely to endure, in addition to a range of common co-occurring issues such as mood dysregulation, mental disorders, sleep disturbance, obesity and injuries secondary to accidents. (Biederman et al., 2020; Cherkasova et al., 2022; Yadav et al., 2021). Personality Disorders (PD) are also common in adults with ADHD. PDs are characterized by enduring inflexible and maladaptive patterns of behavior, cognition, and inner experience, evident across many contexts and culturally atypical. These patterns develop early in childhood and are associated with significant distress or disability (American Psychiatric Association [APA], 2013). Previous research on the prevalence of PDs in adult ADHD has used varying methodologies: selective samples, retrospective or prospective designs, different theoretical models for personalities, (most frequently Cloninger’s model), both dimensional and categorical approaches, and varying characterization of personality such as personality traits and personality disorders. Other studies have focused on examining ADHD prevalence in one specific PD population (e.g., in borderline or antisocial). Unsurprisingly, given these starkly varying methodological approaches, inconsistent and conflicting results are reported which reinforces the lack of a clear and robust estimation of the prevalence and association between PDs and adult ADHD. For instance, in one review (Matthies & Philipsen, 2016), the prevalence range of PDs in ADHD was 10% to 75% while in studies of a specific subpopulation for example, university students with ADHD (McKinney et al., 2013), no personality disorders were reported. In marked contrast, in other studies examining specific populations such as the homeless or prisoners, the reported rate of antisocial and borderline PDs was 100% (Gudjonsson et al., 2012; Salavera et al., 2014).
Given the absence of a robust prevalence estimate, we aimed to examine the prevalence of PDs in a clinical sample of adult ADHD patients referred for the first time without previous diagnosis or ADHD medication. We also aimed to assess personality disorders in a categorical rather than dimensional way (yes/no) as this was deemed to be more clinically meaningful. Although there is a long-lasting debate in categorical approaches versus dimensional in the diagnosis of personality disorders (but also in other psychiatric disorders) with both having some merits, categorical approaches based mainly in severity of a cluster of symptoms have diagnostic meaning, are easier counted and estimated and are comparable between studies. For this reason, we chose the Millon’s Clinical Multiaxial Inventory (MCMI) which also gives diagnostic categories comparable to DSM classification.
Specifically, the aims of the study were: (a) to estimate the prevalence of all PD types in adult ADHD, (b) to investigate the prevalence of specific PD in ADHD, and (c) to examine the relationship between ADHD subtypes and PDs.
Method
Design
Cross-sectional, pragmatic, observational study.
Setting
Consecutive outpatients attending an Adult ADHD clinic were approached and recruited for the study. The adult ADHD clinic is a tertiary level service for counties Sligo/Leitrim/Donegal which was set up as a research clinic and was subsequently developed under the National Clinical Programme into a multidisciplinary team. Referrals are accepted from the Adult Mental Health Services (AMHS) in line with the Republic of Ireland Health Service Executive (HSE) model of care (HSE, 2020). These guidelines direct that patients are screened in AMHS using the Adult ADHD Self-Report Scale (ASRS), (Kessler et al., 2007) and Wender Utah Rating Scale (WURS), (Ward et al., 1993) scales. Those screening positive on both scales are referred to the ADHD Adult Clinic for further clinical assessment for diagnosis and treatment.
Inclusion-Exclusion Criteria
All referred and consented patients with a minimum of 6 years of education (to be able to read and understand the self-rating Inventory) were eligible for inclusion. Exclusion criteria were: (a) patients with a prior ADHD diagnosis or exposure to ADHD medications (b) patients with a severe learning disability, cognitive impairment or severe brain injury, and (c) patients not able to speak or read in the English language. Patients with other psychiatric disorders were included if they had scored positive in the screening scales (ASRS and WURS).
Measurements/Scales
Demographics
Demographic data provided by the respondent included age, gender and age at the onset of symptoms.
Conners’ Adult ADHD Diagnostic Interview for DSM-IV (CAADID) Part II
The CAADID (Epstein et al., 2001) is a structured interview for diagnosing adult ADHD and is based on DSM-IV criteria. Diagnostic accuracy is reported at about 91.46%. The kappa coefficient concordance between the clinical diagnosis and the CAADID is also reported as high (0.88) (Epstein & Kollins, 2006; Ramos-Quiroga & Arif, 2015). It takes about 60 to 90 min to be completed.
Conversion of DSM-IV (CAADID) to DSM-5
The Conners’ Adult ADHD Diagnostic Interview for DSM-IV (CAADID) was converted to DSM-5 criteria, in line with previously reported studies (e.g., Adamis et al., 2023; Deberdt et al., 2015; Karlsdotter et al., 2016; van de Glind et al., 2014). To convert the diagnosis from DSM-IV to DSM-5, we adapted the diagnostic algorithm of the CAADID by using a different cut-off for the age of onset (<12 instead of 7) and different cut offs for the number of symptoms (five or more instead of six) in DSM-IV criteria.
Psychiatric Clinical Evaluation
All participants also had a psychiatric clinical evaluation incorporating DSM-5 criteria. The psychiatrist used all available information (not blind to the administered scales), collateral history from parents or other family members (where possible) and detailed semi-structured neurodevelopmental history.
Millon Clinical Multiaxial Inventory-III (MCMI-III)
This inventory is based on Millon’s evolutionary theory and it is very close to DSM-IV criteria of personality disorders (PD) and consequently to current DSM-5. The MCMI-III is composed of 175 true-false questions and takes on average 30 min to complete. It contains 24 clinical scales which are divided into four groups: Clinical Personality Patterns (11 scales), Severe Personality Pathology (three scales), Clinical Syndromes (seven scales) and Severe Clinical Syndromes (three scales). The last two correspond to clinical syndromes as defined in DSM-IV (Axis I), while the first 2 to personality disorders (Axis II of DSM-IV). In addition, it contains one invalidity scale and three modifying indices, (disclosure, desirability, and debasement index) which access bias in the completion of the inventory (Jankowski, 2002). For the purposes of this paper, only the Clinical Personality Patterns and Severe Personality Pathology scales were considered. The Clinical Personality Patterns are schizoid, avoidant, depressive, dependent, histrionic, narcissistic, antisocial, sadistic, compulsive, negativistic, (passive/aggressive) and masochistic (self-defeating). Severe Personality Pathology include three personality disorders: schizotypal, borderline, and paranoid representing greater levels of personality pathology. A base rate (BR) score of 85 and above in one scale indicates that the individual is likely to be affected by the particular PD indicated by the scale. All BR scores were adjusted for the modifying indexes and those deemed invalid or inconsistent were excluded in line with standard applications of this method (Millon et al., 2009).
Ethics
The Local Research Ethics Committee approved the study. The procedures and rationale for the study were explained to all participants and written informed consent obtained.
Statistical Analyses
The data were anonymized and the IBM (SPSS) v25 package was used for the statistical analysis. Continuous variables are reported as means plus standard deviation, while categorical variables are reported as counts and percentages. Comparison between groups was conducted with parametric or non-parametric test as appropriate. To facilitate descriptive statistics, The Clinical Personality Patterns of MCMI-III (11 scales) were summarized into two (the two highest scores among the 11 scales) and the Severe Personality Pathology (three scales) in one (the highest score among the three). When x2 test was used for comparison in more than two categories (2 × 3 tables) the Adjusted Residuals was used to discover statistical differences between two categories. Adjusted residuals equal 2 or higher indicate significant difference (Agresti, 2018).
Results
Sample
The number of recruited participants was 216, from which 181 (83.8%) had valid MCMI-III, while the rest 35 (16.2%) had invalid MCMI-III (2 incomplete, 29 invalid, and 4 inconsistent/invalid); therefore, those 35 were excluded from the analysis. There were no differences (bias) between those excluded/ included regarding diagnosis of ADHD (x2 = 0.883, df:1, p = .347), gender (x2 = 0.065, df:1, p = .799) and age (t = 0.648, df:214, p = .518)
Descriptive Statistics
The mean age of those included (n = 181) was 32.94, of which 87 (48.1%) were females. One hundred forty-seven (n = 147, 81.2%) were diagnosed with ADHD according to DSM-5 criteria [mean age 32.97, SD: 11.56, females: 74 (50.3%)]. The majority had combined ADHD subtype (n = 88; 59.9%), followed by inattentive type (n = 53; 36.1%) with very few hyperactive-impulsive only type (n = 6; 4.1%).
Examining Severe Personality Pathology of MCMI-III, most participants did not have severe personality pathology (130;71.8%), 32 (17.7%) had one severe personality disorder, 15 (8.3%) had two severe PDs and 4 (2.2%) had three severe PDs. Regarding the Clinical Personality Patterns of MCMI-III (n = 181), 35 (19.3%) participants had no PD (BR scores in MCMI-III < 85) while 57 (31.5%) had one PD elevated (85 and above), 38 (24.0%) had two, 29 had (16%) three, and 22 had (12.1%) four or five. Table 1 shows the counts and the percentages of personality scales between those with and without ADHD.
Counts and Percentage of MCMI-III in Those With and Without ADHD.

Note. In bold significant differences. NS = No significant.
From Table 1, it seems that the most common Severe Personality Pathology of MCMI-III in those diagnosed with ADHD was the borderline PD (n = 30, 20.4%) followed by schizotypal (n = 17, 11.6%) and paranoid (n = 13, 8.8%). From the Clinical Personality Patterns scales the most common were the dependent (n = 58, 39.5%), depressive (n = 45, 30.6%), avoidant (n = 38, 25.9%), antisocial (n = 29, 19.7%) and negativistic (n = 28, 19%).
(See also Table 1 and Figure 1). When the Severe Personality Pathology scales were collapsed to one (with the highest BRs of each scale), the majority of participants (107; 72.8%) had none of the three severe personality disorders (schizotypal, borderline, paranoid), with a small number having borderline (22; 15.1%), schizotypal (10; 6.8%) or paranoid (8; 5.4%) PD.
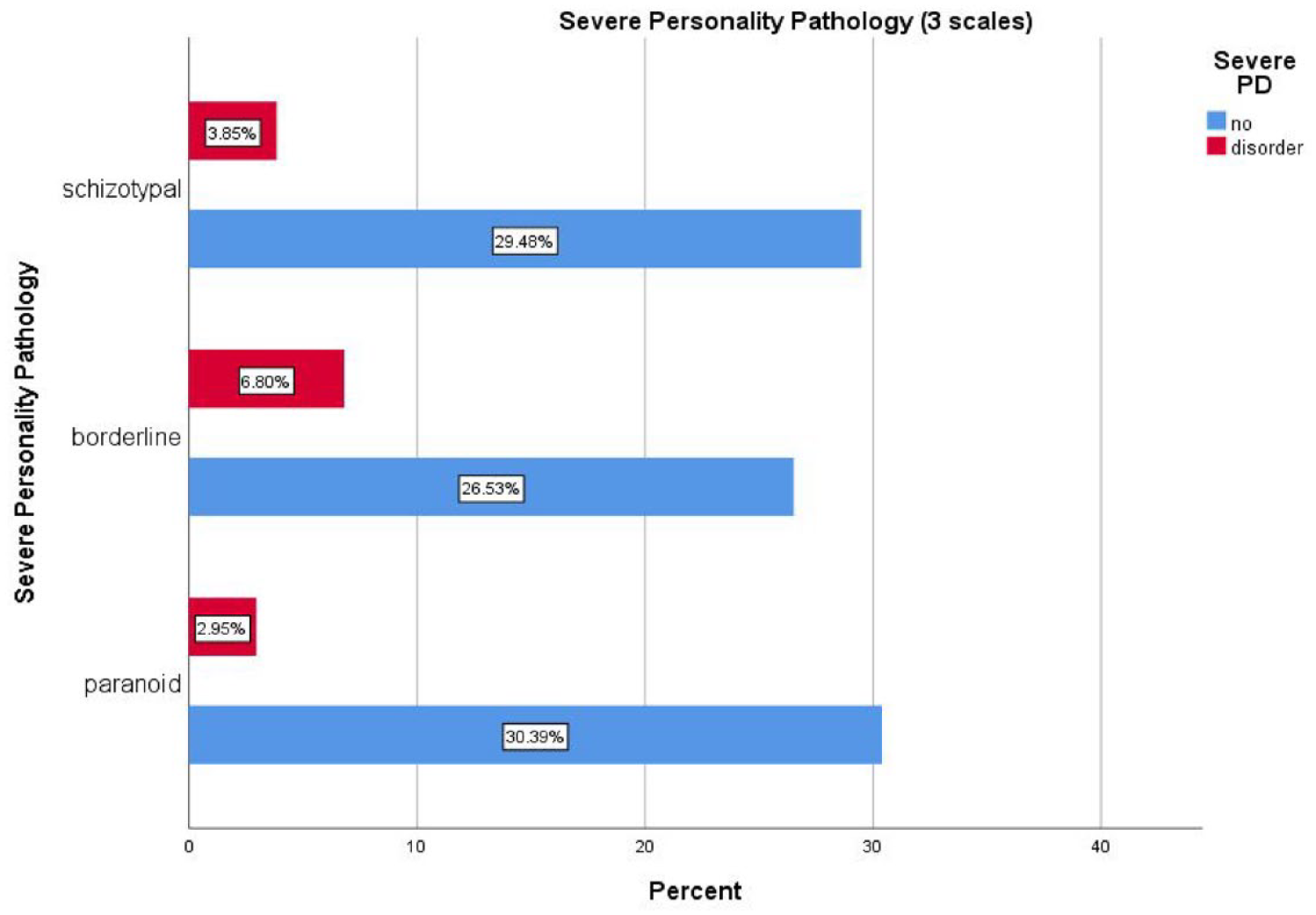
Percentages (grand total) of each type of personality disorder of the Severe Personality Pathology of MCMI-III in those diagnosed with ADHD (n = 147).
In addition, in those diagnosed with ADHD, 29 (19.7%) did not show any personality disorder in Clinical Personality Patterns, while 43 (29.3%) had one scale elevated, 34 (23.1%) had two, 23 (15.6%) had three and the remainder of the cohort 18 (12.3%) four or five. The counts of each PD scale are presented in Table 1 and the percentages (grand total) are pictured in Figure 2.

Percentages (grand total) of each type of personality disorder of the Clinical Personality Patterns in those diagnosed with ADHD.
Bivariate Statistics
Comparison of MCMC-III scales (Severe Personality Pathology and Clinical Personality Patterns) between those diagnosed with and without ADHD were examined using x2 test (See also Table 1, last column). Significant differences were found in schizoid category in that people with ADHD were less likely to have schizoid PD (x2 = 5.635, df:1, p = .018) and narcissistic PD (x2 = 5.726, df:1, p = .017), compared to those without a diagnosis of ADHD. Given the numbers in the narcissistic PD group was small, the Fisher’s exact test was also used, revealing marginal significance (p = .047). No significant differences were found in other personality disorders between those with and those without ADHD.
Finally, the distribution of each scale of MCMI-III across the three different subtypes of ADHD is presented in Table 2.
ADHD Subtypes and PD According to MCMI-III.

Note. In bold significant differences. +,
Where the significant exists among the groups (Adjusted residuals).
Further, a comparison among the three subtypes of ADHD and the distribution of PD was conducted (2 × 3 table) using x2 and inspecting also the adjusted residuals (See also Table 2 last column). Those with combined ADHD subtype were significantly more likely to have sadistic, antisocial and negativistic (passive/aggressive) PDs and less likely to have dependent PD (adjusted residuals two and above). Those with hyperactive/impulsive subtype were more likely to have masochistic (self-defeating) PD and those with inattentive subtype were more likely to have dependent PD and significantly less likely to have sadistic PD.
In addition, because some personality disorders are more often related to one gender a x2 test was used to compared the distribution of PD between the genders. Results are presented in Table 3 and show significant gender specific differences. Dependent, depressive, masochistic and borderline (marginal significance) PDs were more common in females than males (Table 3). In contrast, significantly more males were found with antisocial PD compared to females.
Distribution of PDs According to Gender and Significant Differences.

Significant difference.
Multivariable Statistics
Finally, a logistic regression analysis was conducted to assess if any personality disorder (yes/no) can be predicted from demographic variables (age, gender), subtype of ADHD and years of symptoms. The regression analysis showed that none of those variables was significantly associated with personality disorder.
Discussion
In summary the results show that the majority of people with ADHD attending AMHS have at least one PD, with borderline PD being most prevalent among the Severe Personality pathology. Examining the Clinical Personality Pattern group, dependent, depressive, avoidant, antisocial and negativistic were most common. Those with combined subtype of ADHD were significantly more likely to have sadistic, antisocial and negativistic PD and less likely to have dependent PD. Those with hyperactive/impulsive subtype were more likely to have masochistic PD while those with inattentive subtype were more likely to have dependent PD and significantly less likely to have sadistic PD. There was a preponderance of antisocial PD among males, while dependent, depressive, masochistic and borderline (marginal significance) PDs were more common in females. Finally, no predictive pattern was found from the examined variables (age, gender, subtype of ADHD and years of symptoms) to be associated with the presence or not of a personality disorder.
Comparison of Study Findings With Previous Studies
First of all, regarding the prevalence of PD in ADHD this study shows a high prevalence of PD among those diagnosed with ADHD. Prevalence rates can be affected by the sample, (e.g., selected populations), scales used (e.g., MCMI, NEO-PI-R, Five Factor), definition of PDs (categorical vs. dimensional) and other factors, and thus direct comparison between studies is difficult. Despite these methodological differences, most of the extant data indicate that the prevalence of PDs is high in ADHD, for example, Matthies and Philipsen (2016) in their review reported prevalence between 10% and 75% and definitely higher than in the general population (Bernardi et al., 2012; Tyrer et al., 2015; Volkert et al., 2018 reported a rate of 62.79%; and Salavera et al. (2014) a rate of 100%. Contrary to other studies mentioned, a study by Oliva et al. (2020) in Italy using similar methodology (ADHD clinical outpatient population of 70 participants, using MCMI-III) reported a lower prevalence of PDs (57.1%) compared to the present study in adults with ADHD. This study also found no patient had borderline PD raising the possibility of sample bias.
Borderline PD (BPD) was the most frequent Severe Personality Pathology in the present study. Apart from an absence of any BPD reported by Oliva et al. (2020), previous research has shown results similar to ours (Ferrer et al., 2010; Jacob et al., 2007; Matthies et al., 2011; O’Malley et al., 2016, and Ditrich et al., 2021) with estimates of BPD ranging from 18% to 27% (O’Malley et al., 2016) to 30% to 60% (Ditrich et al., 2021). Furthermore, a number of papers have suggested that there is a link between childhood ADHD symptoms and borderline PD in adulthood (Miller et al., 2008; Smith & Samuel, 2017; Tiger et al., 2022). Shared genetic factors have been posited to explain this association (Kuja-Halkola et al., 2021). However, despite some common symptoms, such as impulsivity, and emotional dysregulation, attentional problems are more evident in those with ADHD compared to those with borderline PD (Koerting et al., 2016; O’Malley et al., 2016). It has also been proposed that the impulsivity of ADHD reflects a neurocognitive disorder while the impulsivity of borderline PD is characterized as more behavioral (Ditrich et al., 2021). Further exploration of these characterizations of impulsivity are required to allow a determination of the validity or otherwise of this conceptualization. Although borderline PD in the general population is reported more commonly in females (Paris, 2004), in our sample this difference was marginal. It is reasonable to consider, as has been suggested by other authors, that gender bias, sampling bias and comorbidity can influence this gender difference in borderline PD (Paris, 2004; Sansone & Sansone, 2011). However, a recent large-scale Swedish study on the co-occurrence of ADHD and borderline PD reported that the association between ADHD and borderline PD as being similar in females and males. (Kuja-Halkola et al., 2021).
Furthermore, the high prevalence of dependent personality found (nearly 40%) of our cohort (cluster C in DSM-5) is unsurprising. People with dependent personality disorders have difficulties in making everyday decisions, and feel helpless, incompetent and immature. They struggle to be autonomous and perceive a need to be taken care of by another person. They live persistently in fear and anxiety of being abandoned. Given that some people with ADHD have variable cognitive difficulties since early childhood, low self-esteem and dependency may be conceptualized as psychologically understandable. Previous studies have shown a higher prevalence of dependent personality in adult ADHD compared to the present study (59.1%, in Spanish homeless people, Salavera et al., 2014), but lower in psychiatric inpatients (18.4%, Miesch & Deister, 2019) and psychiatric outpatients (27%, Oliva et al., 2020).
Similarly, avoidant PD (cluster C in DSM-5), found in 26% of our sample, is fundamentally characterized by fear of rejection, tension in social situations, permanent anxiety, feelings of inadequacy and inferiority, and sensitivity in criticism. Similar rates (21.7%) were reported by Matthies et al. (2011) and even higher (59.1%) by Salavera et al. (2014). In addition, a high rate of depressive PD was found in our sample (30.6%). The depressive PD (not included in DSM-5) is characterized by extremely low self-esteem, permanent feelings of hopelessness, guilt, impotence, pessimism and a sense of worthlessness. Somatic complaints maybe often be used to offer an excuse for the worthlessness and objective evidence of disability. (Davis & Patterson, 2005). As above, a number of studies also reported similar rates of depressive PD in ADHD participants (e.g., Hamzeloo et al., 2016; Oliva et al., 2020). Similarly, a higher prevalence of depressive PD was reported in females compared to males (Cumyn et al., 2009).
In addition, a number of studies have shown similar results regarding antisocial and negativistic (passive/aggressive) PDs (e.g., Oliva et al., 2020). Higher rates of antisocial and negativistic PDs in ADHD were found in specific populations such as prisoners and homeless, (Gudjonsson et al., 2012; Hamzeloo et al., 2016; Salavera et al., 2014) and a link with male gender and antisocial PD was reported in ADHD studies (Cumyn et al., 2009; Edvinsson et al., 2013) as well as in the general population (Paris, 2004). Both of those PDs are characterized by impulsivity, anger and oppositional and disruptive behaviors (Millon et al., 2009). Indeed, an association of conduct and oppositional defiant disorders in childhood with later development of antisocial PD in adulthood in patients with ADHD has been reported (Biederman et al., 2008; Dowson, 2008; Rosa-Justicia et al., 2022).
However, most of the above studies (including ours) are cross sectional and assess ADHD retrospectively, thus being unable to examine any neurodevelopmental link. A small number of studies have investigated the relationship between childhood ADHD and later development of personality disorders (Klein et al., 2012; Mannuzza et al., 1993, 1998; Miller et al., 2008). Despite the mixed methodologies and the small sample sizes, some of these studies have shown a link between childhood ADHD and adult personality disorders more consistently with borderline PD, antisocial and avoidant PDs (Cherkasova et al., 2022; Smith & Samuel, 2017).
Similarly, the association which was found between subtypes of ADHD and certain PDs, mainly between combined subtype and sadistic, antisocial and negativistic PDs and between inattentive subtype and dependent PD in this study, has been reported in a number of previous studies both cross-sectional (Cumyn et al., 2009; Jacob et al., 2016; McKinney et al., 2013; Salgado et al., 2009) and longitudinal (Cherkasova et al., 2022).
Finally, we did not find many significant differences between those diagnosed with ADHD and those without in terms of personality disorders except for schizoid and narcissistic. Given that the control sample was small and also that they have been referred for ADHD evaluation (therefore biased and not a true control) those results may not reflect true differences.
Overall, the results of the present study support the premise that ADHD correlates with personality pathology more generally, rather than with one specific PD type. Further, the present study suggests that perhaps it is better to examine categorical models for assessing personality disorders even if there is a risk of lowering the prevalence rates of PDs because categorical approaches have more clinical meaning than dimensional. Categorical approaches are based to a certain degree on severity of symptoms and therefore do not ignore the dimensionality of psychopathology but make it more meaningful. In addition, categories are more easily summarized in future meta-analyses as well as providing greater specificity in distinguishing personality pathology among those with adult ADHD.
Clinical Implications
The present study suggests that the majority (80%) of patients referred and subsequently diagnosed with ADHD had at least one PD. Additionally, rates were high (25%) for those referred but who did not meet ADHD diagnosis.
Careful assessment of personality disorders within ADHD clinical services are essential to plan comprehensive treatment plans and optimize clinical outcomes in those with both confirmed and suspected ADHD.
Limitations and Strengths of the Study
One important limitation of the study is the sample. The sample is a biased sample as it investigates only those referred for an ADHD evaluation. It is expected that this population has more severe problems and complexity and thus the rates of PD may be higher in the present study than community norms. In addition, the sample includes patients with other comorbid psychiatric disorders for which we did not control and they may influence the rate of PDs in any direction. However, this limitation is also a strength of the study because it is more pragmatic and reflects everyday clinical situations. The cross-sectional design of the study does not allow inference of causality. Genetic and environmental factors need to be evaluated longitudinally to establish the characterization of these associations of PDs and ADHD. The strength of the study is that it includes people diagnosed for the first time in adulthood and naive to ADHD medications. It remains unclear if early diagnosis and treatment from childhood can alter the trajectory of development of PDs in adulthood, although there are indications that early treatment can prevent the development of comorbidities (e.g., Able et al., 2007; Halmøy et al., 2009). A final strength of the study is that clinically meaningful diagnostic categories have been used.
Conclusions
The present study is an observational, pragmatic study investigating rates of personality disorders in a sample referred for the first time in adulthood for ADHD evaluation. A high rate of PDs was found, most notably dependent, depressive, avoidant, antisocial, negativistic and borderline. Why those personality disorders are more frequently found in ADHD patients remains the subject of debate and needs further investigations. However, because of the high impact of personality disorders in the everyday functioning of those with ADHD it is important to take them into account when treating patients with ADHD (and perhaps those with other conditions) and to offer specific psychotherapy. Further research on developmental trajectories of personality disorders in those with ADHD are required to consider therapeutic options.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.