
Abstract
Objective:
ADHD is associated with suboptimal health behaviors including physical activity (PA). LEAP is a parent BMT group program enhanced to focus on health behaviors, integrated with mHealth technology. Little is known about implementing BMT via telemedicine “telegroups.”
Methods:
Children ages 5 to 10 with ADHD and their caregiver wore activity trackers and participated in an 8 to 9 week parent BMT and social media group emphasizing PA, sleep, and screen use. A 7-day child accelerometer-wear and parent and teacher measures were completed pre- and post-group. Groups were in-person prior to the COVID-19 pandemic and in telegroup format during the pandemic.
Results:
Thirty-three families participated in person and 23 participated via virtual telegroup. Group attendance was superior for telegroup with equivalent satisfaction and skill use. Changes in health behavior and clinical outcomes were equivalent.
Conclusions:
LEAP is a feasible and novel BMT intervention that can be delivered in an accessible telegroup format with high participation and acceptability.
ADHD is among the most common behavioral disorders for children, with a population prevalence of around 10% (Polanczyk et al., 2014). Along with broad functional impairments, ADHD is associated with suboptimal health behaviors such as inadequate physical activity (PA) and increased risk for chronic health problems such as obesity, cardiovascular disease, and premature death (Nigg, 2013; Schoenfelder & Kollins, 2016). Evidence-based treatments (EBTs) for ADHD—namely stimulant medications and behavior management training (BMT)—generally focus on core ADHD symptoms and associated behavioral problems, and the extent to which they may affect health behaviors and long-term outcomes is unknown. A growing field of research indicates that optimization of positive health behaviors, such as physical activity, in combination with EBTs may improve functioning and long-term health for individuals with ADHD (Schoenfelder & Kollins, 2016).
Current recommendations suggest that school-aged children should achieve at least 60 min per day of moderate to vigorous physical activity, at least 8 hr of sleep, and minimize sedentary activities, including less than 2 hr/day of recreational screen use (Paruthi et al., 2016). On average, only one-third of children with ADHD meet any of these recommendations, and even fewer do so in adolescence (Ebenegger et al., 2012; Martinson et al., 2018; Tandon et al., 2019). Increasing PA has moderate-to-large effects on improving ADHD symptoms and functioning (Cornelius et al., 2017) and a moderate effect on executive functions that increases with PA duration (Vysniauske et al., 2020). For example, a before-school PA intervention in an ADHD-risk sample showed that exercise was associated with moderate effect sizes on parent- and teacher-reported measures of ADHD and functioning (Hoza et al., 2015). However, little is yet known about how introducing lifestyle changes that sustain PA increases may affect ADHD-related symptoms and functioning more broadly and how parents may mediate such changes.
In children with ADHD, PA is found to be interrelated with other health behaviors, including sleep duration and screen time (Hong et al., 2021), with a worsening in one area perpetuating worsening in other areas (Korioth, 2020). Prior studies demonstrate that treating sleep problems, which are commonplace for youth with ADHD (Yürümez & Kılıç, 2016), including through parent-focused sleep hygiene interventions, improves ADHD-related functioning (Huang et al., 2007; Sciberras et al., 2020; Weiss et al., 2006). Time spent on screen-based media is also linked to ADHD symptom severity and functional problems (Nikkelen et al., 2014; Thoma et al., 2020), as well as sleep problems (Becker & Lienesch, 2018). Thus, health behavior interventions for youth with ADHD are much needed, and a holistic model that considers all three interrelated health behaviors is likely to have more benefit.
As the well-established frontline EBT for ADHD (Evans et al., 2018), BMT offers an opportunity to introduce parent-mediated changes in children’s health behaviors through relationship building, added structure and positive contingencies. BMT offered individually or in a group improves parenting and externalizing behaviors (for a review, see Evans et al., 2018), though we are unaware of prior research on the effects of BMT on health behaviors of children with ADHD.
The Lifestyle Enhancement for ADHD Program (LEAP) adapts BMT to target health risk behaviors (PA, sleep, screen use) in youth with ADHD. The program incorporates wearable mobile Health (mHealth) technology and a social media group to increase motivation and engagement in the parent BMT group curriculum. When implemented in person, a previous investigation found that LEAP can be delivered with high fidelity and caregiver acceptability, and with high levels of participation in terms of attendance (over 90%), use of mHeath tools (parents and children exceeding 5 days per week on average), and weekly practicing of parenting skills (Ola et al., 2021).
The COVID-19 pandemic has led to lower PA and worse mental health for children (Tandon et al., 2021), enhancing the timeliness of interventions to increase PA, especially for children with ADHD who are at higher risk of negative health outcomes. The pandemic has also accelerated the implementation of telemedicine delivery formats for mental health (Sharma et al., 2020). Telemedicine shows promise for increasing reach, access, and possibly engagement in behavioral treatments. Though individualized BMT can be delivered effectively via telemedicine (Tse et al., 2015), there are few prior studies on delivering BMT for ADHD in a telemedicine group (or “telegroup”) and how this implementation context affects participation and outcomes (Ros-DeMarize et al., 2021; Sullivan et al., 2021). One recent study compared in-person and telemedicine group delivery of an emotion regulation and conflict intervention for adolescents with ADHD, finding higher attendance but lower homework completion for telehealth, and generally equivalent effects on targeted teen and family outcomes (Breaux et al., 2021).
The current study compares the delivery of LEAP—BMT for children with ADHD enhanced to address child health behaviors—via in-person groups before the pandemic and telegroups during the COVID-19 pandemic. We predicted that telegroup delivery during the pandemic would be equivalent to in-person in acceptability and initial efficacy while serving a wider geographical range. This single-arm study also compares in-person versus telegroup pre-to-posttest changes in parenting practices, health behaviors (PA, sleep, and screen use), ADHD symptoms and executive functions.
Methods
We recruited children with ADHD ages 5 to 10 years (along with a custodial caregiver residing with the child at least 50% of the time) who were not meeting PA recommendations based on caregiver report. Caregivers completed an initial phone screening, and children and caregiver then attended a diagnostic screening visit to confirm eligibility, including ADHD and co-morbid diagnoses. Exclusion criteria were diagnosis of autism spectrum disorder, mood disorder, depressive disorder or psychosis, caregiver-reported child current MVPA exceeding 60 min daily at least 5 days per week, and medical restrictions on physical activity. Children could be taking medications for ADHD (stimulants or non-stimulants) or other conditions as long as the dose had been stable for at least 30 days. After the first pilot round of group, the study team added clinical severity as a screening criterion as measured by the Clinical Global Impairment-Severity, with participants scoring >3 and <7 being excluded. Enrolled caregivers completed pre-intervention and posttest (9–10 weeks later) surveys and children wore accelerometers for 7 days at each time point.
Intervention
The LEAP curriculum is based on BMT skills from the Defiant Children manual (Barkley, 2013), with adaptations to focus on physical activity, screen use, and sleep. A full description is provided in a previous publication (Ola et al., 2021). Caregivers in the “In-Person Cohort” (Sept 2018-Dec 2019) participated in 90-min parent group sessions (7–8 families per group) weekly for 8 weeks at a hospital outpatient clinic, facilitated by licensed psychologists. In response to the COVID-19 pandemic, group BMT sessions were offered via videoconferencing (Zoom) for the “Telegroup Cohort” (Sept, 2020-June, 2021), and content spacing was increased across 9, 90-min session based on feedback from previous participants. Each session consisted of homework review, introduction of new parenting skills, and skills practice. Up to three 30-min make-up sessions were offered to families who missed group sessions. Caregivers and children received Garmin Vivofit 4 and Garmin Vivofit Jr. activity-tracking watches, respectively, and were asked to wear them daily for the intervention period. After 1 week, average daily steps were calculated, and weekly goals were calculated based on an algorithm to increase steps by no more than 10% per week. Goals were sent to families via text. Caregivers were invited to join a private Facebook group moderated by their group co-leader with three posts per week focused on ADHD, group skills, and strategies to increase PA; families were invited but not required to post and comment freely.
Ethical Considerations
This study was approved by the Seattle Children’s Institutional Review Board. Following initial eligibility screening, interested families completed informed consent meetings via videoconference; parents signed informed consent and children gave verbal assent.
Measures
Screening
Children were evaluated by clinical psychologists for ADHD and psychiatric co-morbidities using the Schedule for Affective Disorders for School-Aged Children Present and Lifetime Version (KSADS), which has established validity and reliability (Kaufman et al., 1997).
Baseline clinical severity was evaluated by the assessor using the Clinical Global Impairment-Severity (CGI-S) scale, on which clinicians estimate functional impact on a 1 to 7 scale (Busner & Targum, 2007).
Acceptability
Acceptability was measured with attendance rates (including and excluding make-up sessions) and average days of Garmin wear for children and caregivers. At posttest, caregivers completed the Client Satisfaction Questionnaire (CSQ), a reliable questionnaire on which they rate the program using a 1 to 4 scale on eight dimensions (e.g., quality, helpfulness, etc.) (Attkisson & Greenfield, 2004; Larsen et al., 1979). Caregivers also completed 23 acceptability questions asking them to rate the helpfulness of each program skill/component on a 1 to 5 scale (e.g., “How helpful was daily active time?” or “How helpful was creating a family media plan?”). Acceptability of telemedicine delivery was assessed with two questions for the telegroup cohort: “How satisfied were you with the group being run online with teleconferencing?”; “How much were you able to follow along and participate in the online group?”
Parenting
The Alabama Parenting Questionnaire (APQ)—Short Form, (Elgar et al., 2007) a 9-item caregiver rating, was used to assess the frequency with which caregivers implement parenting practices from three categories (Positive Parenting, Inconsistent Discipline, and Poor Monitoring) on a 5-point scale. Each subscale was analyzed separately.
Health Behavior Outcomes
Physical Activity
Participating children were asked to wear an ActiGraph GT3X+ accelerometer (Actigraph, Pensacola, FL) on their right hip for 1 week pre and post-intervention. After removing sleep hours, data were classified into sedentary time, light-intensity PA (LPA), and MVPA using validated Evenson cut points, and average daily minutes in each of these categories was compared pre to post-intervention. In addition, we examined what proportion of children were meeting the 60 min/day of MVPA recommendation.
Screen Use
Via survey, parents estimated their child’s average number of hours spent daily on screens (estimates for TV, videogames, computer, and mobile devices reported separately and then added) on weekdays excluding time in school.
Sleep Problems
The Children’s Sleep Habits Questionnaire (CSHQ) is a caregiver-report measure of sleep problems in school-aged children that has been frequently used in ADHD populations (Bonuck et al., 2017; Owens et al., 2000). The Total Sleep Disturbance score was used. A Total Sleep Disturbance score of >41 identifies 80% of children with a clinical sleep disorder (Markovich et al., 2015).
Clinical Outcomes
Parent-Reported ADHD Symptoms
The Conners-Third Edition Parent Rating Scale (Conners-3), a 93-item measure with high reliability and validity, was completed by caregiver to assess the core features of DSM-5 ADHD. The measure yields t-scores to indicate clinical elevations on Inattention and Hyperactivity/Impulsivity subscales (Conners, 2008).
Teacher-Reported Symptoms
Teachers completed the Vanderbilt ADHD Rating Scale, a DSM-5-based scale that assesses Inattentive and Hyperactive/Impulsive ADHD symptoms on a 0 to 3 scale (Becker et al.,2012). Symptom count scores (number of symptoms endorsed at a 2 to 3 out of 3 severity) were calculated for each subscale. Internal consistency is good to excellent for the VADTRS (Wolraich et al., 2013).
Executive Functions
Caregivers completed the Behavior Rating Inventory of Executive Function-Second Edition (Gioia et al., 2000; Roth et al., 2014) an 86-item, reliable and valid measure of everyday executive functioning that yields index T-scores. The Global Executive Composite score was utilized.
Analyses
Demographics and baseline characteristics were summarized using descriptive statistics, with means and standard deviations reported for continuous variables, counts and proportions for categorical variables. Comparisons between in-person and telegroup cohorts were conducted using Wilcoxon rank sum test for continuous variables, and chi-squared test for categorical variables. When calculating scale scores, we used mean imputation when there were less than 50% of the items missing. For a subject with 50% or more of items missing, no scale score were calculated and the subject was dropped from corresponding analysis. Outcomes at baseline and post-intervention follow-up were compared using paired t-test. Changes in outcomes from baseline to follow-up were compared between in-person and tele-delivery with two-sample t-test. All analyses were conducted using the R statistical software version 4.1.2 (RC TEAM, 2013). Given sample size limitations and goal of detecting preliminary trends, we focused on confidence intervals and thus did not adjust for multiple tests.
Results
Participants
A total of 61 (37 In-Person, 24 Telegroup) caregiver/child dyads were enrolled in the study. Demographics are shown in Table 1. Demographics were comparable across cohorts, except that Telegroup cohort children were older and parents had higher levels of educational attainment. For the in-person cohort, 77% were from the host county, and 23% resided in 3 other counties. For the Telegroup cohort, 67% were from the host county, and 33% parents represented 7 other counties. Four in-person and one telegroup family withdrew before the intervention; two in-person and zero telegroup families started LEAP but withdrew from the program before posttest measurements (Figure 1).
Demographics and Cohort Differences.
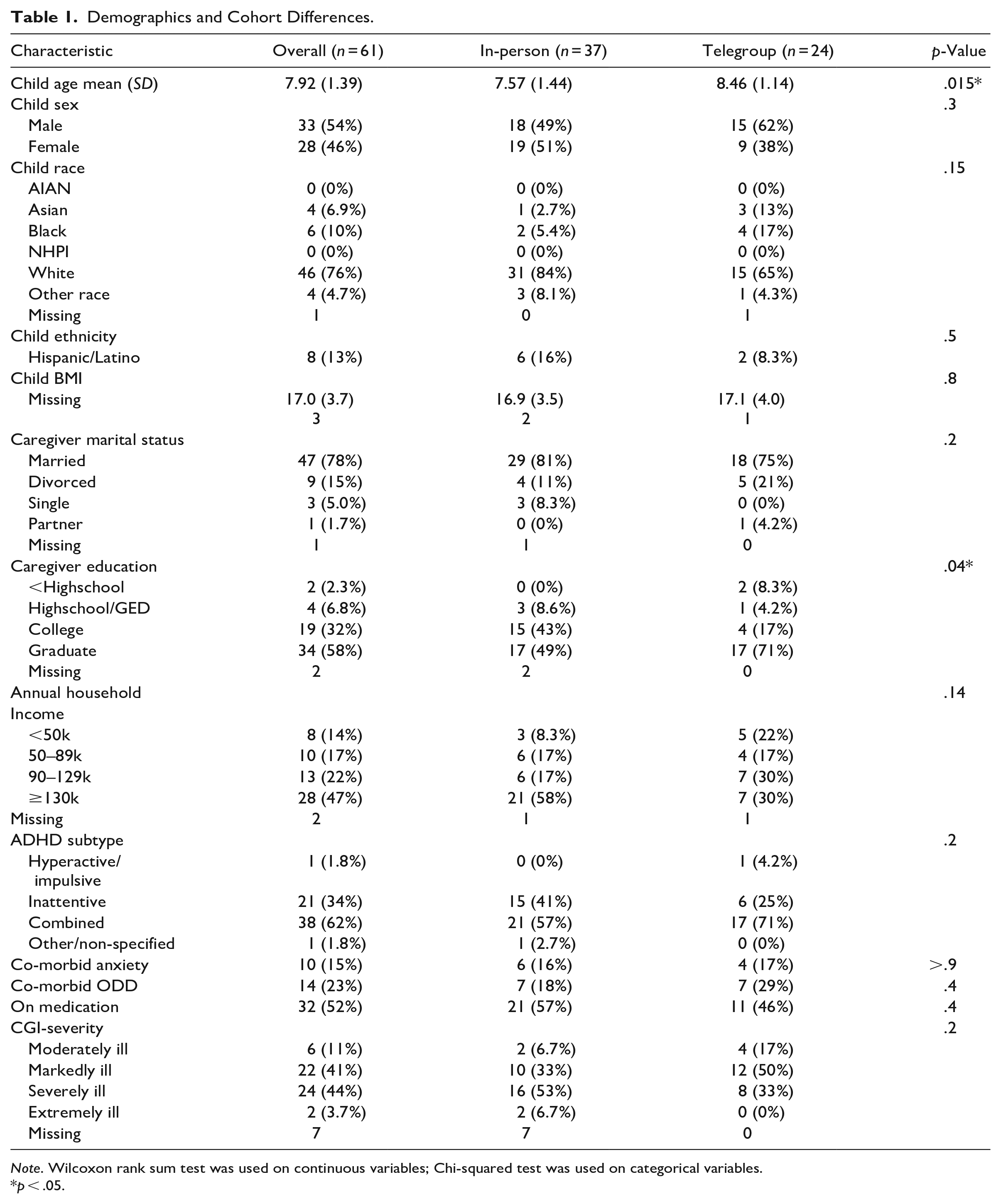
Note. Wilcoxon rank sum test was used on continuous variables; Chi-squared test was used on categorical variables.
p < .05.
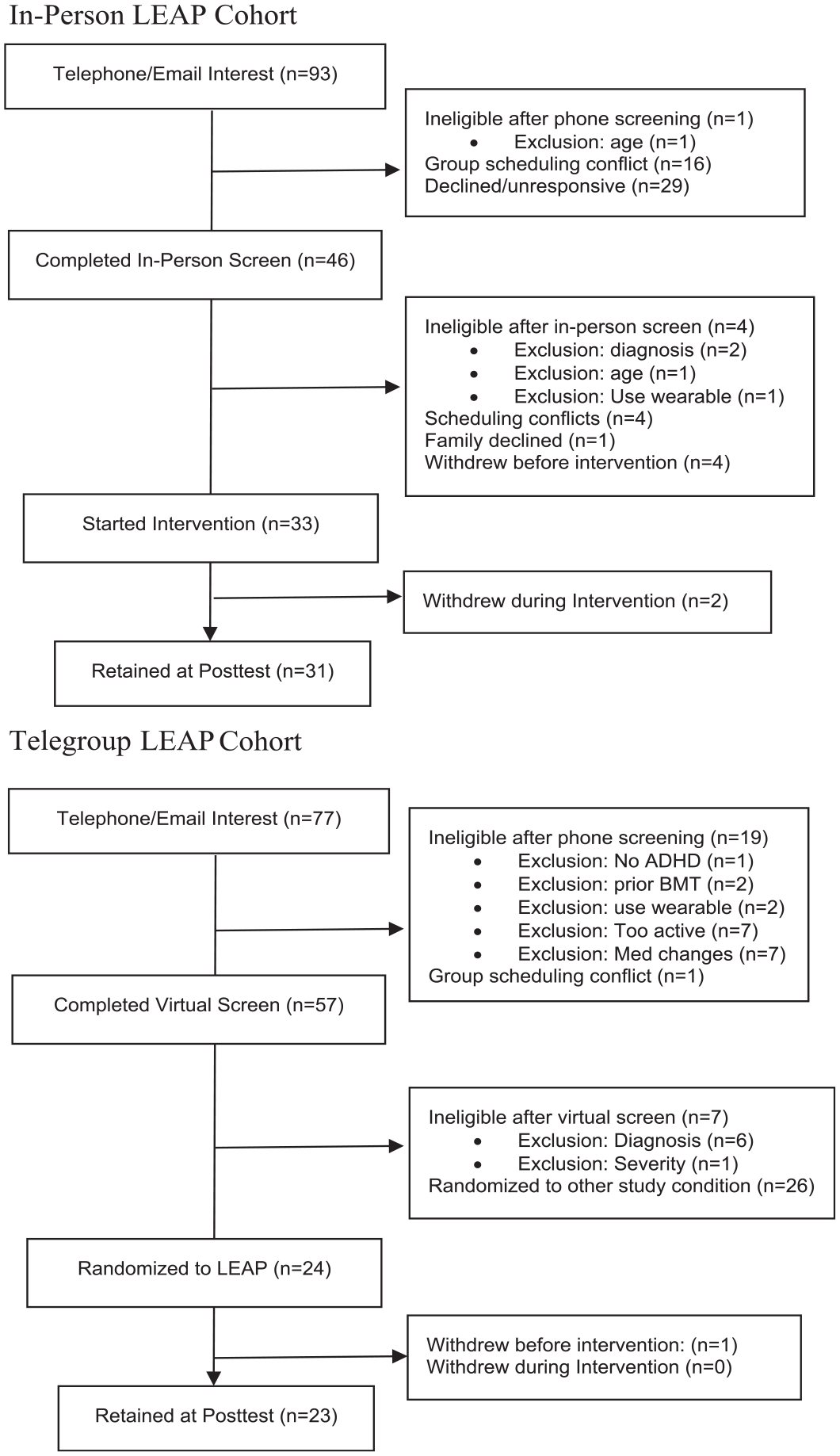
LEAP study consort diagram.
Acceptability
Acceptability for each cohort is shown in Table 2; a full discussion of the in-person cohort’s acceptability is reported in a previous publication (Ola et al., 2021). As shown, attendance excluding make-up sessions was significantly higher for the telegroup than for in-person cohort; attendance was equivalent when factoring in make-up sessions. Telegroup Garmin wear was equivalent to the in-person cohort, as was mean satisfaction on the CSQ and overall parent-reported skill use and perceived skill helpfulness. Just as in the in-person cohort, the telegroup cohort rated consistent sleep routine to be the most helpful skill. Telegroup families rated praise (Catch ’em in the act) and Daily Active Time to be the second and third most helpful skills, which differed from the in-person cohort’s report of screen time limits and wearing the Garmin as the second and third most helpful skills.
In-person Versus Telegroup LEAP Acceptability.
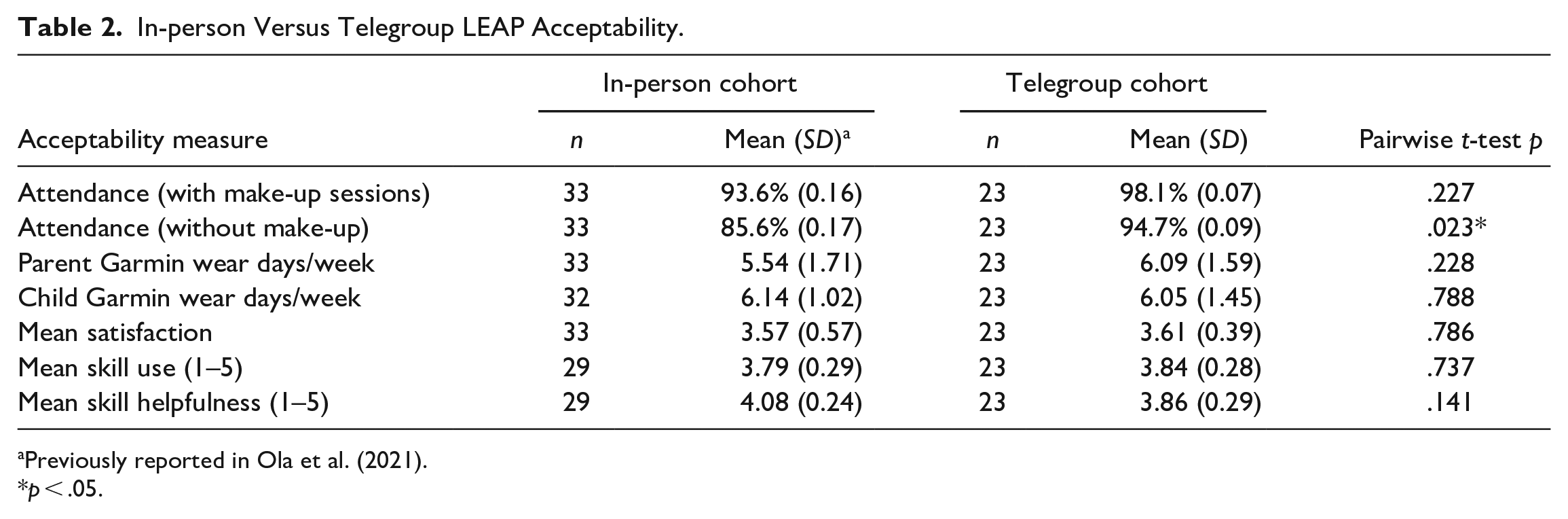
Previously reported in Ola et al. (2021).
p < .05.
For telegroup families, average satisfaction with telemedicine format was 4.48 out of 5 (SD = 0.59). Most participants (91.3%) reported they were “somewhat” to “very” able to follow along and participate in the telegroup format.
Parenting
As shown in Table 3, APQ poor monitoring improved by posttest, and this effect was consistent across cohorts.
LEAP Outcomes by Cohort.
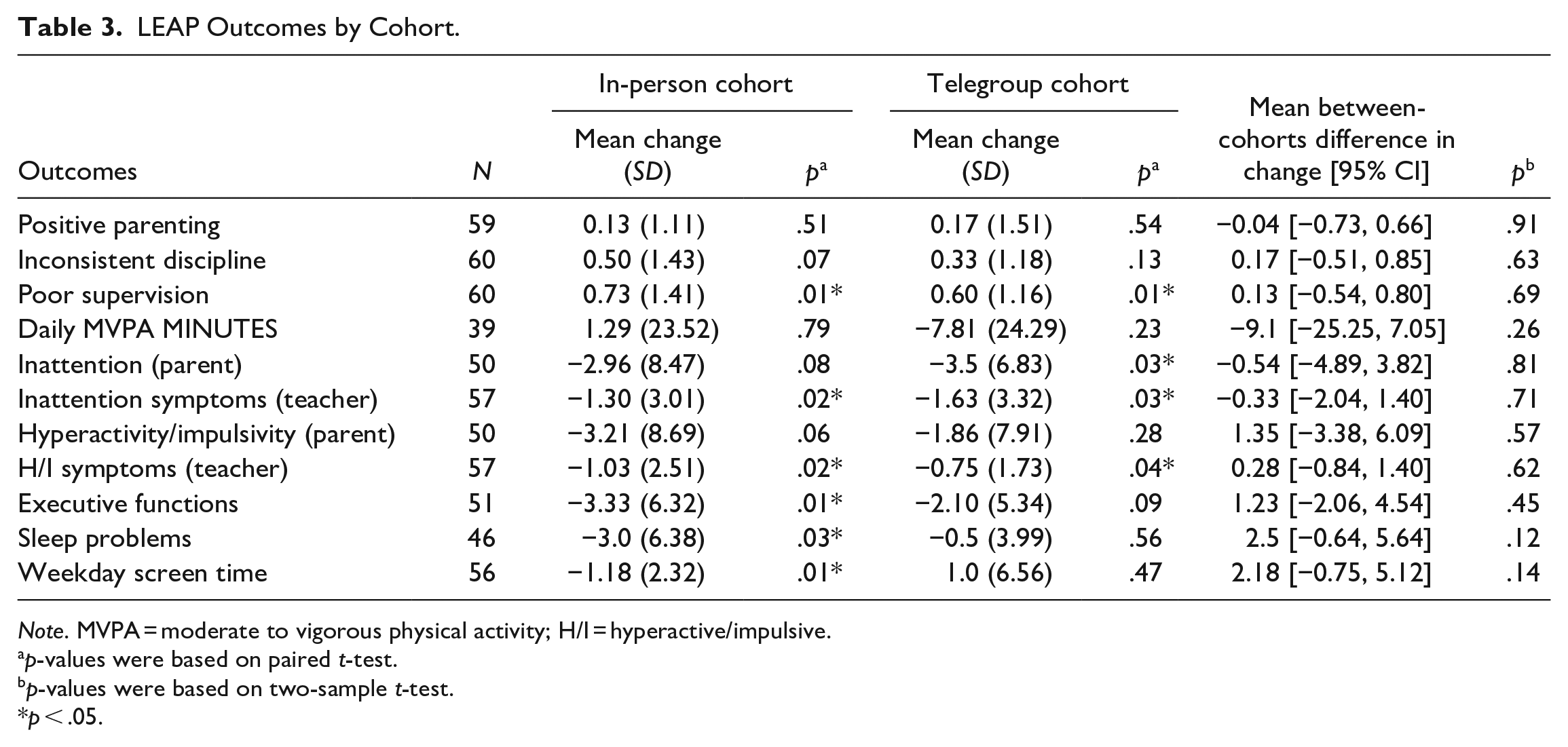
Note. MVPA = moderate to vigorous physical activity; H/I = hyperactive/impulsive.
p-values were based on paired t-test.
p-values were based on two-sample t-test.
p < .05.
Health Behavior Outcomes
Mean accelerometer-measured MVPA at baseline was equivalent across cohorts, with 52.9 (SD 26.29) min/day for in-person and 50.7 (SD 22.88) min/day for telegroup children. The percentage of children meeting daily MVPA guidelines per accelerometry at baseline was 35.3% for the in-person and 40% for the telegroup cohort. Daily MVPA at baseline did not differ by child gender, ADHD medications, ADHD subtype, or family income. As shown in Table 3, hip-worn accelerometry data indicated that children’s average MVPA was stable from baseline to posttest, and there was no difference across cohorts.
Telegroup families reported that the most common barriers to PA at baseline were their child not having interest (45.5%), needing 1:1 supervision (36.4%), and not having activities available (31.8%), and at posttest were no interest (40.9%), not having time (36.4%) and their child not being athletic (31.8%). This differed from the in-person cohort’s report of top barriers being 1:1 supervision and cost at both time points, as well as not having time at baseline.
A majority of the in-person cohort (66.7%) and nearly half of the telegroup cohort (45.5%) reported total baseline sleep disturbance on the CHSQ that exceeded clinical cut points for a sleep disorder. As shown in Table 3, improvement in total sleep problems was found at posttest for the In-Person cohort and this effect did not significantly differ across cohorts.
Telegroup parents estimated 6.30 hr/day of weekday screen time (SD = 5.56), which was more than double the 2.67 hr/day (SD = 2.32) of weekday screentime reported by the in-person cohort parents. As shown in Table 3, weekday screen time deceased at posttest for the in-person but not telegroup cohort, though the effects were not statistically different across cohorts.
Clinical Outcomes
As shown in Table 3, improvement was found at posttest in teacher-reported inattention and hyperactivity/impulsivity across both cohorts; parents reported a decrease inattention symptoms in the Telegroup cohort only.
Global executive functioning problems decreased for the in-person group at posttest, though this was not significant for the telegroup.
Discussion
We compared engagement and preliminary outcomes for the LEAP intervention delivered in-person pre-pandemic versus telegroup during the first year of the COVID-19 pandemic. We found that LEAP is a feasible, novel intervention for parents of children with ADHD that can be delivered in an accessible telegroup format with high levels of participation and acceptability, and that attendance was higher when the program was delivered via telemedicine. There were no significant differences between the in-person and telegroup cohorts in pre to post change in outcome variables, though sample size and power were limited. Our preliminary analyses revealed indicators of improvement in both cohorts in teacher- and parent-reported ADHD symptoms and executive functioning that should be further evaluated in a larger study.
When delivered in a telegroup format, LEAP group session attendance was higher and a wider geographical region was served, while measures of Garmin wear, skill use, perceived skill helpfulness, and satisfaction were equivalent to in-person LEAP. The findings on attendance are consistent with a similar recent comparison of adolescent ADHD group attendance by Breaux et al. (2021), though we did not find lower rates of skill use or differences in outcomes as these researchers did. Telegroup parents rated satisfaction with telegroup delivery highly and most found the telemedicine platform allowed for adequate participation. Our findings are encouraging in light of the increased relevance and popularity of telemedicine services since the start of the pandemic. Telemedicine delivery of BMT offers the potential to reduce treatment access barriers such as travel time, transportation, and need for child care, and improve access for underserved geographic regions. Furthermore, telemedicine groups have added benefits of increasing cost-effectiveness and reducing caregiver isolation when circumstances make in-person services difficult. Future efforts should focus on identifying and mitigating technological access barriers for families with limited access to these resources.
Preliminary outcome analyses indicated improvement in clinical outcomes, though minimal change in the health behavior outcomes. This single-arm treatment study does not allow for determination of whether changes in outcome variables are attributable to the treatment or other factors, or whether trajectories differ compared to untreated children. Notably, the telegroup cohort participated during a time when public schools and most workplaces were remote across Washington state and families were experiencing extreme disruptions to daily structure and schedules. For example, average daily screen use was nearly 3 times higher in the telegroup cohort and the percentage of children with clinical sleep disturbance was lower than pre-pandemic. Pandemic circumstances may have impacted parents’ abilities to set limits on screen time, while the lack of school commute may have engendered more lax bedtimes and wake times. Furthermore, both cohorts were comprised of majority families with high caregiver education and household SES, and half of the children were also taking medication for ADHD. Thus, it is possible that we were not able to observe some program-induced changes in this higher-resourced sample during this unique pandemic time period.
Consistent with study screening parameters that selected for children with sub-optimal PA, a minority of participating children exceeded PA guidelines at baseline or posttest. More research is needed to compare the PA trajectories observed during the study to those of families who are not receiving PA intervention. We observed many factors potentially associated with PA levels that could be controlled for in a randomized trial—including weather/seasonality, daylight hours, and school breaks/holidays. In addition, numerous pandemic-related factors likely influenced the PA of children in the telegroup families, making it challenging to compare this outcome across the cohorts. More pre-pandemic parents reported that child behavior (needs 1:1 supervision) was the primary barrier to PA, whereas lack of child interest was the primary barrier for families during the pandemic. A larger trial would also allow for exploration of other potential covariates that affect PA trajectories, such as walkability and safety of the neighborhood, socioeconomic resources, and involvement in or availability of organized sports.
Study strengths include the novel mHealth-enhanced intervention and telegroup delivery format, unique opportunity to compare baseline health behavior data and treatments before versus during the pandemic, and use of data from multiple sources (parents, teachers, accelerometers). Study limitations include the single-arm design and small sample size, which precluded us from drawing statistical conclusions about program outcomes and controlling for demographic differences or cultural/lifestyle impacts of the pandemic. Children with higher PA-levels were excluded from the study based on parent estimations of average weekly PA, and the validity of such parent estimates is not established. Missing data, especially posttest accelerometer data is also a limitation and should be taken into account when interpreting findings.
The current study highlights the emerging role of technology-integrated and digitally-delivered interventions and the use of objective measures such as accelerometry. Future studies will examine the additive effects of LEAP health behavior components to BPT and compare changes in health behavior trajectories during participation. Subsequent recruitment efforts must focus on engaging underrepresented groups, including racial and ethnic minority families that were underrepresented in the current sample, and ascertain whether the telegroup modality remains acceptable and feasible for a more diverse population and in non-pandemic circumstances. It will also be important to identify subgroups—such as those with more significant PA or sleep deficits or with lower access to PA resources—for whom LEAP is most valuable to inform a future targeted or supplemented intervention strategy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Center for Complementary and Integrative Health (NCCIH; 4R33AT010041-03).