
Abstract
Objective:
To report the burden of ADHD in the Middle East and North Africa (MENA) region from 1990 to 2019.
Methods:
Publicly available data on the burden of ADHD were retrieved from the Global Burden of Disease study 2019. The counts and age-standardized rates (per 100,000) were presented.
Results:
In 2019, ADHD had an age-standardized point prevalence of 1245.1 and a years lived with disability (YLD) rate of 15.1 per 100,000 in MENA, which were 7.2% (−11 to −3.3) and 7.2% (−11.2 to −2.7) lower, respectively, than in 1990. The highest YLD rate of ADHD was found in the 10 to 14 age group and there were no remarkable differences between males and females. No clear association was found between the YLD rate and the socio-demographic index.
Conclusion:
The burden of ADHD in the MENA region decreased over the period 1990 to 2019, and regularly updating the epidemiological information is suggested.
Keywords
Introduction
Attention-deficit hyperactivity disorder (ADHD) is a chronic externalizing disorder that is characterized by inattention and/or hyperactivity-impulsivity (American Psychiatric Association, 2013). Although the definitive pathogenesis of ADHD is still unknown, genetic and neuroanatomical findings appear to play an important role in the disorder. ADHD is known as a familial disorder (Thapar & Cooper, 2016) whose recurrence risk is about five times higher for first-degree relatives than that of the non-ADHD population (Faraone et al., 2000). In addition, twin studies from several different countries have found a heritability rate of about 76%, which is similar to other neurodevelopmental disorders (Thapar et al., 2013). Furthermore, a recent study revealed a genetic overlap in loci between ADHD and bipolar disorder (O’Connell et al., 2021). Moreover, polymorphisms in the dopamine transporter gene and dopamine 4 receptor gene have been found to be related to ADHD (Franke et al., 2012). Neuroimaging has shown that abnormalities in the prefrontal and parietal circuits, and smaller areas of the frontal cortex, cerebellum, and subcortical structures, are common in those with ADHD (Kasparek et al., 2015). Moreover, studies have found abnormal functioning in the caudate, putamen, and globus pallidus, areas that are involved in executive functioning, behavior inhibition, and the modulation of reward pathways (Schweitzer et al., 2000; Valera et al., 2005). Moreover, due to the catecholaminergic nature of most of the brain’s neural circuits, dopamine and norepinephrine agonists can regulate the dopamine and norepinephrine hypoactivity in the frontal-subcortical circuits of ADHD patients, which treats the impulsivity, inattention, and hyperactivity (Arnsten, 2006; Wilens, 2006).
Many environmental and maternal pre-pregnancy risk factors can contribute to the development of ADHD, such as maternal pre-pregnancy obesity and overweight, hypertensive disorders during pregnancy, pre-eclampsia, maternal acetaminophen exposure during pregnancy, maternal smoking during pregnancy, childhood asthma, and low serum vitamin D concentration (Kim et al., 2020). Children and adolescents with ADHD have higher rates of intentional and unintentional self-injury (Dalsgaard et al., 2015; Hinshaw et al., 2012), motor vehicle crashes (Curry et al., 2017), nicotine usage (Lee et al., 2011), alcohol and substance use disorder (Lee et al., 2011), and academic impairment (Fleming et al., 2017; Hinshaw et al., 2012), particularly in the inattentive and combined subtypes (Pingault et al., 2011).
Although ADHD is mainly known as a childhood disorder, the majority of ADHD-diagnosed children continue to meet the ADHD criteria into adulthood (Fayyad et al., 2007; Karam et al., 2015; Roy et al., 2016). The most significant predictors of the persistence of ADHD into adulthood are the severity of the symptoms (Karam et al., 2015; Roy et al., 2016), comorbid conditions (Roy et al., 2016), parental mental health problems (Roy et al., 2016), and co-occurring oppositional defiant disorder (Karam et al., 2015). Adults with ADHD have a higher risk of unemployment and workplace impairment (Küpper et al., 2012), academic impairment (Küpper et al., 2012), trauma (Küpper et al., 2012), motor vehicle crashes (Küpper et al., 2012), self-injury and suicide attempts (Hinshaw et al., 2012), and substance use disorder (van Emmerik-van Oortmerssen et al., 2012). A recent meta-analysis found that people with ADHD had a mortality rate that was almost two times higher than the general population (Larson et al., 2011). In addition, those with ADHD had an almost three times higher risk of death from unnatural causes, while the risk of death from natural causes was not significantly different from the general population (Larson et al., 2011). People with ADHD often have other psychiatric disorders, such as mood disorders (Kessler et al., 2006; Larson et al., 2011; Tung et al., 2016), anxiety disorders (Kessler et al., 2006; Larson et al., 2011; Tung et al., 2016), oppositional defiant disorder (Pliszka, 2007; Tung et al., 2016), conduct disorder (Larson et al., 2011; Tung et al., 2016), and learning disabilities (Larson et al., 2011; Yoshimasu et al., 2010, 2011). Moreover, there is an association between the severity level of ADHD and the number of comorbid disorders (Fayyad et al., 2007), as well as between the subtype of ADHD and the type(s) of comorbidities (Wolraich et al., 1996, 1998). As people with ADHD get older, the number of comorbid conditions increases (Cumyn et al., 2009; Kessler et al., 2006), and the symptoms of those other conditions become more obvious, making ADHD harder to identify and treat (Bukstein, 2022). Globally, in 2019 the age-standardized point prevalence of ADHD for both sexes was 1131.9 per 100,000 population (GBD 2019 Mental Disorders Collaborators, 2022), while in the Middle East and North Africa (MENA) region this figure was 1245.1 per 100,000 (GBD 2019 Mental Disorders Collaborators, 2022). ADHD usually develops in children and adolescents and is more common in males than in females (GBD 2019 Mental Disorders Collaborators, 2022; Olusanya et al., 2018). In addition, ADHD has been found to have a higher age-standardized prevalence in regions with higher levels of income and social development (GBD 2019 Mental Disorders Collaborators, 2022; Olusanya et al., 2018).
MENA is a region with a number of special social and cultural features. For example, there are currently armed conflicts in areas like Yemen and Palestine, as well as large variations in socioeconomic development, which can affect mental health (Dimitry, 2012; Naal et al., 2020). Several previous studies have reported the burden of mental disorders in the Eastern Mediterranean Region (EMR) using data from the Global Burden of Disease (GBD) study 2013 and 2015 (Charara et al., 2017, 2018). However, they did not include all countries from the MENA region and they did not concentrate on ADHD. Furthermore, there is a need to regularly update the epidemiological information in order to provide the most recent and up-to-date data for health policy makers. Therefore, we aimed to report the prevalence, incidence and years lived with disability (YLDs) attributable to ADHD in the MENA region from 1990 to 2019, by age, sex and socio-demographic index (SDI).
Methods
Case Definition and Data Sources
ADHD is an externalizing disorder that is characterized by persistent inattention and/or hyperactivity-impulsivity. The Diagnostic and Statistical Manual of Mental Disorders—Fourth Edition, Text Revision (DSM-IV-TR) criteria requires six or more symptoms of inattention or hyperactivity-impulsivity that have persisted for at least half a year in at least two different settings and have caused substantial impairment to functioning, with some of these symptoms appearing before 7 years of age (12 years in DSM-5). The defining symptoms of ADHD are presented in Tables S1 (GBD 2019 Diseases and Injuries Collaborators, 2020). The GBD study only included cases diagnosed using the DSM or International Classification of Diseases (ICD) (called “hyperkinetic disorder”) diagnostic criteria. The codes for the DSM-IV-TR (314.0, 314.01) and ICD-10 (F90) were used, but different DSM (DSM-III, DSMIII-R, DSM-IV, DSM-IV-TR, and DSM-5) and ICD (ICD-9 and ICD-10) versions were also included (GBD 2019 Diseases and Injuries Collaborators, 2020).
An updated systematic literature review was undertaken in GBD 2019 to find epidemiological studies that were published between September 2016 and December 2018 and reported the prevalence, remission, incidence, duration, and/or excess mortality associated with ADHD. The systematic review was undertaken in conjunction with conduct disorder, since they are both childhood behavioral disorders and are frequently reported together. The literature review involved searching the electronic databases of peer-reviewed literature (i.e., using PsycInfo, Embase, and PubMed), the gray literature, and consultation with an expert. The IHME only included studies that met the following inclusion criteria: (1) were published in or after 1980; (2) cases were defined using a clinical threshold, such as those provided by the DSM or ICD; (3) reported adequate details about their study methodology and sample characteristics to evaluate study quality; (4) sample was representative of the general population (i.e., case studies, inpatient or pharmacological treatment samples, veterans, or refugee samples were not included). All publication languages were accepted. The data sources that were used can be found here: https://ghdx.healthdata.org/gbd-2019/data-input-sources (GBD 2019 Diseases and Injuries Collaborators, 2020).
Data Processing and Disease Model
All estimates were split into sex and age groups, in accordance with the available data. In studies where prevalence was reported in wide age groups by sex (e.g., 15–45 year old males and 15-45 year old females), and also for combined sexes in specific age groups (e.g., 15–29 years olds, and in 30–60 years olds, for males and females together); the reported sex ratio and bounds of uncertainty were used to provide age-specific estimates by sex. The remaining combined-sex estimates in the dataset were split using Meta-Regression with Bayesian priors, Regularization, and Trimming (MR-BRT) analysis. Sex specific estimates, matched by year, age, location, and a MR-BRT network meta-analysis were used to estimate the pooled sex ratios and the uncertainty level for each parameter. These were then used to separate the combined sex estimates in each dataset. The prevalence ratio of male: female was estimated to be 2.52 (GBD 2019 Diseases and Injuries Collaborators, 2020).
DisMod MR 2.1 was then used to estimate the epidemiological data for ADHD, using the normal GBD 2019 decomposition structure. At each step, the new model was compared with the best model in GBD 2017 and the top model from the prior step. Any large changes between models were investigated and explained. Where appropriate, amendments were made to model priors or the data. In the case of outliers, the study’s methodology and quality were re-assessed before IHME made a decision about whether to retain the data. At first, all epidemiological parameters were included in the estimation process. It was assumed that there was no incidence of ADHD before 3 years of age or after 12 years of age. The minimum age was established based on the literature and following consultation with experts, while the upper age limit was selected in accordance with DSM-5 criteria. Prior to 12 years of age, remission was set to zero, in line with the incidence restrictions. Although a recently published meta-analysis reported that individuals with ADHD have higher risk of mortality, during the compilation of the GBD 2019 results there was not enough research evidence to firmly establish that those with ADHD had a higher risk of mortality, so excess mortality was set to zero. There were no national-level covariates used to inform the estimation of ADHD prevalence in locations without data (GBD 2019 Diseases and Injuries Collaborators, 2020).
Severity and Years Lived With Disability
The disability weight (DW) for ADHD was 0.045 (95% confidence interval: 0.028–0.066) and its lay description was “Is hyperactive and has difficulty concentrating, remembering things, and completing tasks.” The findings from the Great Smoky Mountains Study were used to estimate the proportion of time symptomatic and asymptomatic (Ezpeleta et al., 2001). Almost half (48%) of those with ADHD reported a disability and 20% of those without a diagnosis also reported a disability. Therefore, the proportion of time symptomatic was estimated for the “average case” by subtracting the proportion of disability in children without a diagnosis from the proportion of those with ADHD, giving an adjusted proportion of 28% (48–20 = 28). Additional information on their methodology has previously been published (Erskine et al., 2014).
The years lived with disability (YLD) was estimated by multiplying the prevalence estimates by the DW. The YLD is a frequently used indicator of disease burden, with one YLD being the equivalent of 1 year of healthy life lost because of disability or poor health. The YLD and years of life lost (YLL) are also normally summed to estimate the disability-adjusted life year (DALY), another frequently used indicator of disease burden. There was no mortality attributable to ADHD, and thus the YLDs were the same as the DALYs. The GBD standard population was used to standardize all estimates. In addition,1,000 draws at each step of the modeling process were made to produce 95% uncertainty intervals (UIs). The 95% UIs consisted of the 25th and 975th values of the ordered draws. Smoothing Splines were used to examine the relationship between the ADHD burden and the socio-demographic index (SDI) (Wang, 2011). The SDI ranges from 0 (lowest development) to 1 (highest development) and is comprised of the total fertility rate under 25 years old, the average number of years at school for those over 15 years old, and the lag-distributed average income per capita (smoothed over the previous decade) (GBD 2019 Diseases and Injuries Collaborators, 2020). The following website can be used to find the incidence, point prevalence, and YLD estimates http://ghdx.healthdata.org/gbd-results-tool. R software (Version 3.5.2) was used to create all figures.
Results
The Middle East and North Africa region
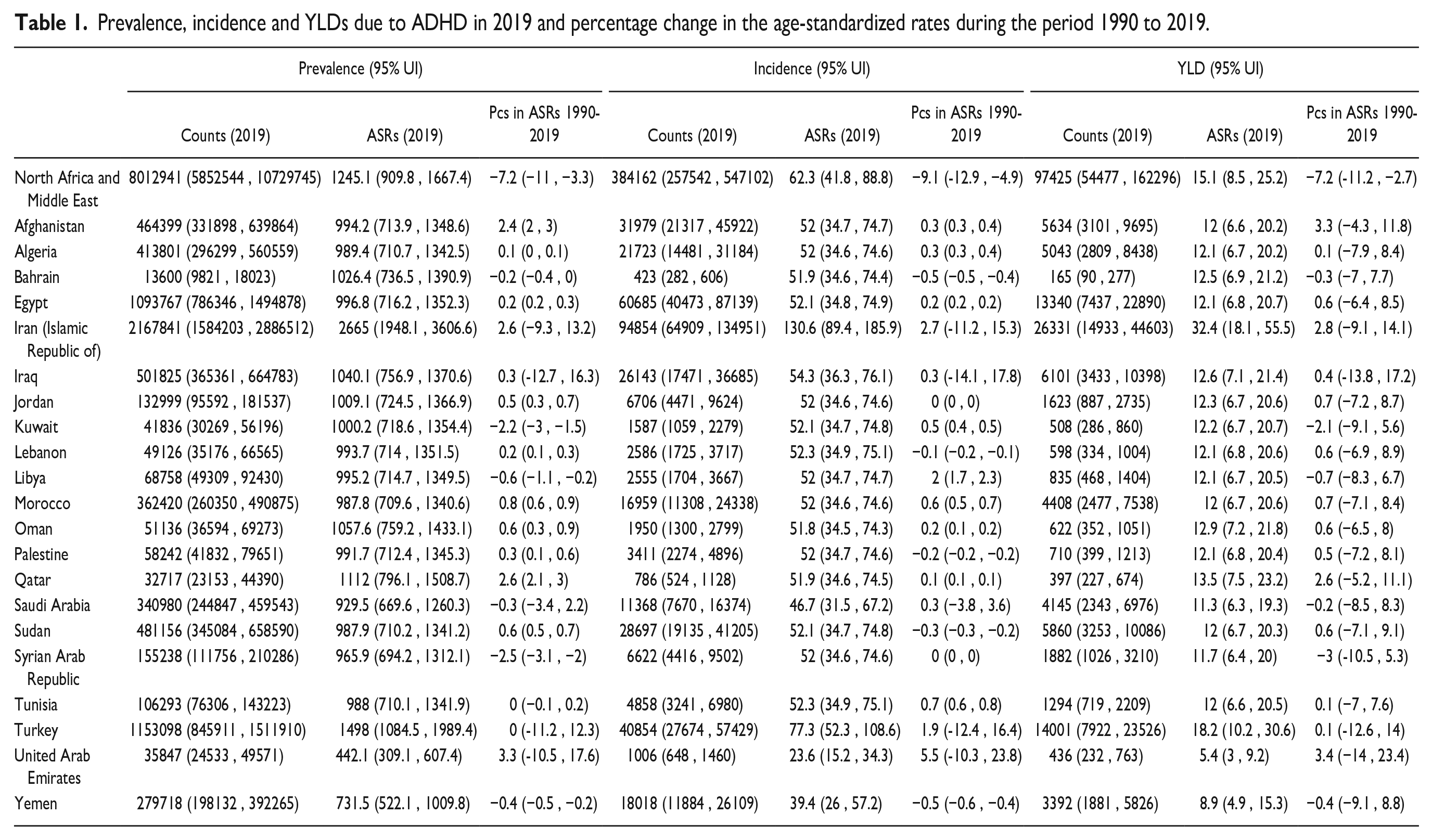
In 2019, there were 8 million (95% UI: 5.8–10.7) prevalent cases of ADHD in MENA, with an age-standardized point prevalence of 1.2 thousand (0.9–1.7) per 100,000 population, which was 7.2% (−11 to −3.3) lower than in 1990 (Table 1 and Table S2). ADHD accounted for 384.1 thousand (257.5–547.1) incident cases in 2019, with an age-standardized incidence rate of 62.3 (41.8–88.8), which was 9.1% (-12.9 to −4.9) lower than in 1990 (Table 1 and Table S3). Also in 2019, there were 97.4 thousand (54.5–162.3) YLDs that were due to ADHD, with an age-standardized rate of 15.1 (8.5–25.2), which was 7.2% (-11.2 to −2.7) lower than in 1990 (Table 1 and Table S2).
Prevalence, incidence and YLDs due to ADHD in 2019 and percentage change in the age-standardized rates during the period 1990 to 2019.
National Level
In 2019, the national age-standardized point prevalence of ADHD among MENA countries ranged from 0.4 to 2.7 thousand cases per 100,000 population. Iran [2665 (1948.1–3606.6)], Turkey [1498 (1084.5–1989.4)], and Qatar [1112 (796.1–1508.7)] had the highest age-standardized point prevalence in 2019. In contrast, the United Arab Emirates [442.1 (309.1–607.4)], Yemen [731.5 (522.1–1009.8)], and Saudi Arabia [929.5 (669.6–1260.3)] had the lowest rates (Table S2). The national age-standardized point prevalence of ADHD in 2019 is presented for both sexes in Figure 1A.
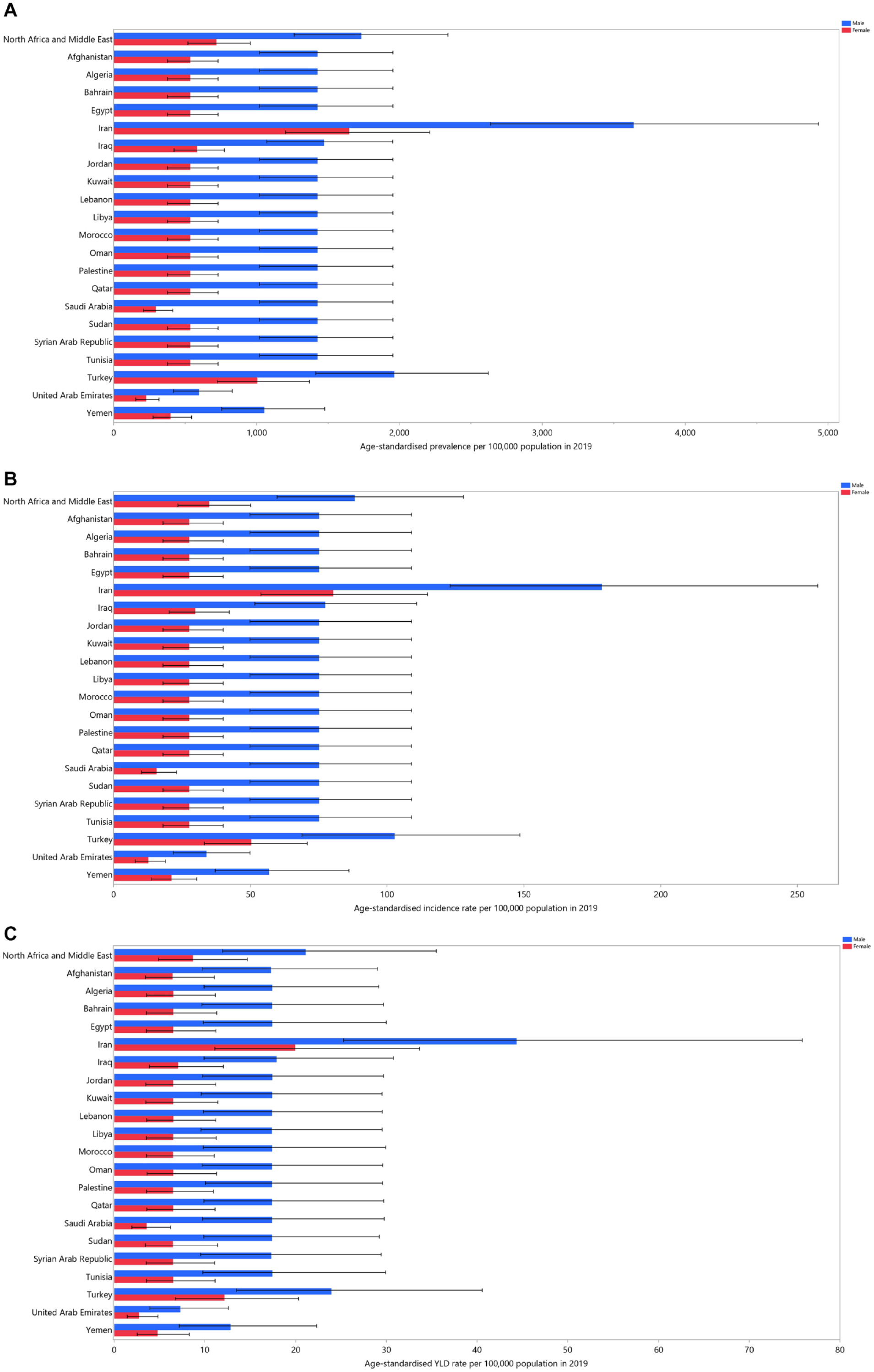
Age-standardized point prevalence (A), incidence (B), and YLDs (C) for attention-deficit hyperactivity disorder (per 100,000 population) in the Middle East and North Africa region in 2019, by sex and country. YLD = years-lived-with-disability. (Generated from data available from http://ghdx.healthdata.org/gbd-results-tool).
In 2019, the national age-standardized incidence rate of ADHD among MENA countries ranged from 23.6 to 130.6 cases per 100,000 population. The highest age-standardized incidence rates were found in Iran [130.6 (89.4–185.9)], Turkey [77.3 (52.3–108.6)], and Iraq [54.3 (36.3–76.1)], while the lowest were observed in the United Arab Emirates [23.6 (15.2–34.3)], Yemen [39.4 (26–57.2)], and Saudi Arabia [46.7 (31.5–67.2)] (Table S3). The national age-standardized incidence rates of ADHD in 2019 are presented for both sexes in Figure 1B.
In 2019, the national age-standardized YLD rate of ADHD among MENA countries ranged from 5.4 to 32.4 cases per 100,000 population. Iran [32.4 (18.1–55.5)], Turkey [18.2 (10.2–30.6)], and Qatar [13.5 (7.5–23.2)] had the highest age-standardized YLD rates, while the United Arab Emirates [5.4 (3 –9.2)], Yemen [8.9 (4.9–15.3)], and Saudi Arabia [11.3 (6.3–19.3)] had the lowest (Table S4). The national age-standardized YLD rates of ADHD in 2019 are shown for both sexes in Figure 1C.
The age-standardized point prevalence of ADHD increased from 1990 to 2019 in nine of the MENA countries and decreased in four, while no significant differences were found in the remaining countries. Qatar [2.6% (2.1–3)], Afghanistan [2.4% (2 –3)], and Morocco [0.8% (0.6–0.9)] had the largest increases in the age-standardized point prevalence rate. In contrast, the Syrian Arab Republic [−2.5% (−3.1 to −2)], Kuwait [−2.2% (−3 to −1.5)], and Libya [−0.6% (−1.1 to −0.2)] had the largest decreases (Figure S1 and Table S2).
The age-standardized incidence rate has increased substantially in nine of the MENA countries since 1990 and decreased in five. The largest increases in the age-standardized incidence rates of ADHD were observed Libya [2% (1.7–2.3)], Tunisia [0.7% (0.6–0.8)], and Morocco [0.6% (0.5–0.7)], while the largest decreases were found in Yemen [−0.5% (−0.6 to −0.4)], Bahrain [−0.5% (−0.5 to −0.4)], and Sudan [−0.3% (−0.3 to −0.2)] (Figure S2 and Table S3). There were no significant changes in the age-standardized YLD rate of ADHD in the MENA countries between 1990 and 2019 (Figure S3 and Table S4).
Age and Sex Patterns
In 2019, the regional point prevalence and total prevalent cases of ADHD increased dramatically with advancing age, reaching their peak in the 10 to 14 age group and then steadily declined to the oldest age group for both sexes. In addition, the regional point prevalence and total prevalent cases of ADHD were substantially higher in males in the 1 to 39 and 1 to 49 age groups, respectively (Figure 2A).
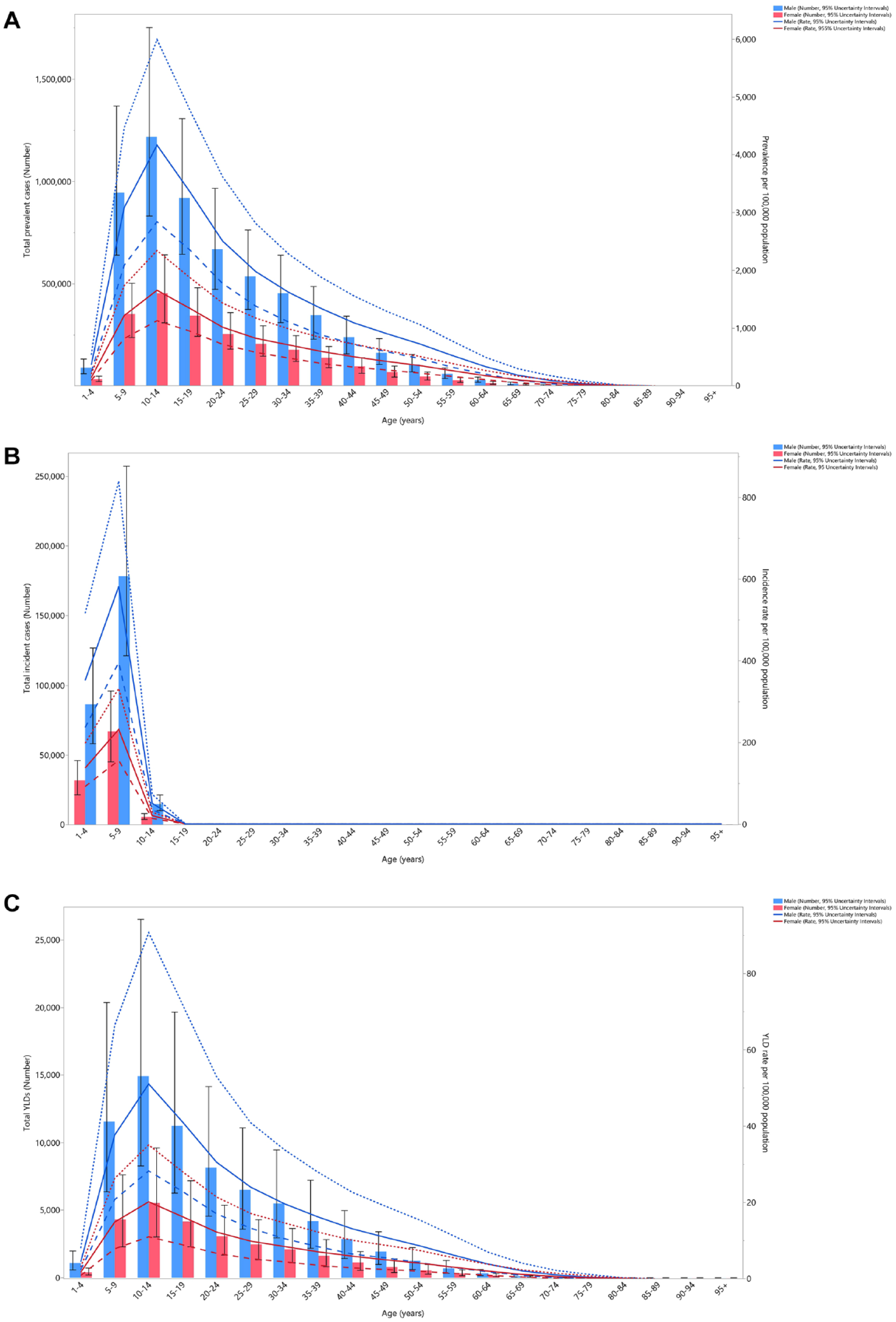
Number of prevalent cases and prevalence (A), number of incident cases and incidence rate (B), and the number of YLDs and YLD rate (C) for attention-deficit hyperactivity disorder (per 100,000 population) in the Middle East and North Africa region, by age and sex in 2019; Dotted and dashed lines indicate 95% upper and lower uncertainty intervals, respectively. YLD = years-lived-with-disability. (Generated from data available from http://ghdx.healthdata.org/gbd-results-tool).
In 2019, the regional incidence rate and total incident cases of ADHD rose up to the 5 to 9 age group and then decreased up to the 15 to 19 age group, were there were no incident cases in either sex. Moreover, the regional incidence rate and total incident cases were substantially higher in males in all age groups (Figure 2B).
The regional total YLDs and YLD rate in 2019 increased with increasing age, peaking in the 10 to 14 age group, and then decreased to the oldest age groups for both sexes (Figure 2C). Furthermore, there were no remarkable differences between males and females in the YLD rate or total YLDs.
In 2019, the ADHD-associated YLD rate in MENA was similar to the global YLD rate for males in the 1 to 19 age groups. However, the YLD rate was higher than the global YLD rate (ratio of MENA/Global YLD rate >1) in males older than 20 and females in all age groups, and the rate ratio increased dramatically in both sexes for those older than 75 years old. Also in 2019, the MENA/Global YLD rate was higher in females in all age groups except for the 20 to 34 and 85 to 89 age groups. Compared to 1990, the MENA/Global YLD rate was similar to the 2019 ratio for both sexes up to the 70 to 74 age group, while the 2019 rate was higher for all remaining age groups (Figure 3).

Ratio of the Middle East and North Africa region YLD rate to the global YLD rate of attention-deficit hyperactivity disorder by age group and sex, 1990 to 2019. YLD = years-lived-with-disability. (Generated from data available from http://ghdx.healthdata.org/gbd-results-tool).
Association With the Socio-demographic Index (SDI)
During the period 1990 to 2019, the burden of ADHD did not change up to an SDI of around 0.4, then increased slightly up to an SDI of around 0.65, but then decreased again as SDI increased. Countries such as Iran, Turkey, and Afghanistan had higher than expected burdens, while Yemen, Tunisia, Libya, Lebanon, Jordan, Egypt, and Algeria had lower than expected burdens (Figure 4).
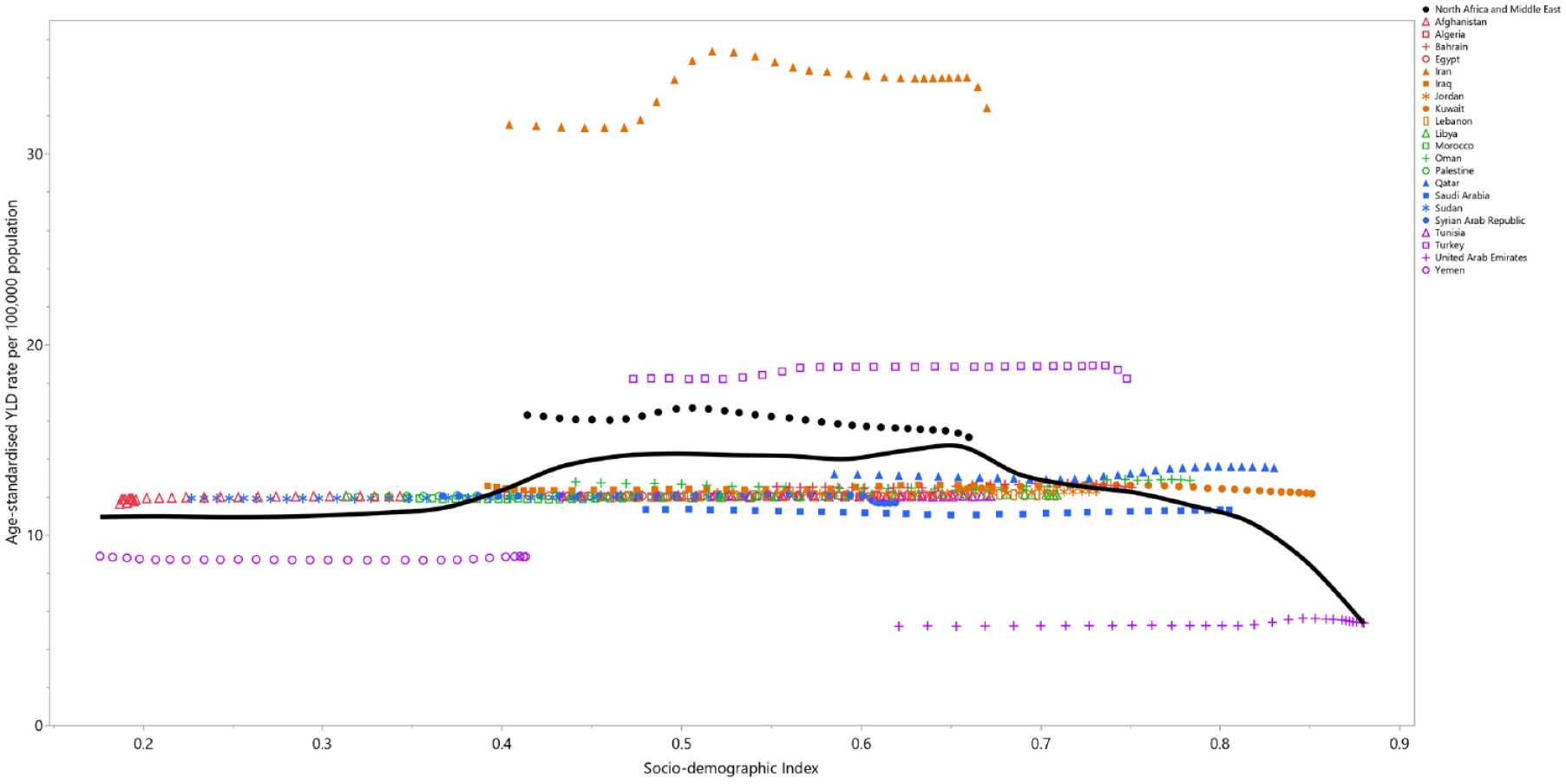
Age-standardized YLD rates of attention-deficit hyperactivity disorder for the 21 countries and territories in 2019, by SDI; Expected values based on the Socio-demographic Index and disease rates in all locations are shown as the black line. Each point shows the observed age-standardized YLD rate for each country in 2019. YLD = years-lived-with-disability. SDI = Socio-demographic Index (Generated from data available from http://ghdx.healthdata.org/gbd-results-tool).
Discussion
To our knowledge, this is the first study to report the burden of ADHD using GBD 2019 data, and to report the prevalence, incidence, YLD counts and age-standardized rates from 1990 to 2019 in the 21 MENA countries. While no comprehensive regional and national scale studies have reported the burden of ADHD in MENA, there have been global (GBD 2019 Mental Disorders Collaborators, 2022), regional (Charara et al., 2018), and some national studies (Amendola, 2022; Ma et al., 2020). In 2019, the National School-Based Screening Program in Saudi Arabia systematically screened schoolchildren for a number of health problems, including ADHD (Al Daajani et al., 2021). A total of 219,218 first-grade students were tested for ADHD using the Vanderbilt ADHD Rating Scale, which was completed by both parents and teachers of each suspected student (Al Daajani et al., 2021). They found that the prevalence of ADHD was 2.81%, among students suspected of having ADHD (Al Daajani et al., 2021). This high prevalence may be due to the fact that only first grade students suspected of having ADHD were screened, instead of all first grade students, and that children were evaluated using a screening scale, which can lead to overestimation. Furthermore, unlike our study they found the prevalence among females to be higher than among males (1.2%vs. 0.7%). This may be due to bias in the selection by teachers (Al Daajani et al., 2021).
In 2017, a national community-based study with 30,532 children and adolescents was performed, The Iranian Children and Adolescents’ Psychiatric Disorders Study (IRCAP), in order to estimate the prevalence of psychiatric disorders in all provinces of Iran (Mohammadi et al., 2019). The participants were randomly selected, using a multi-stage stratified cluster random sampling method, from children and adolescents living in both urban and rural areas. Trained psychologists assessed the children and adolescents using a semi-structured diagnostic interview—the Kiddie-Schedule for Affective Disorders and Schizophrenia-PL (K-SADS-PL) (Mohammadi et al., 2019). They calculated the weighted prevalence based on the 2017 national census (Mohammadi et al., 2019). They reported that the weighted prevalence of ADHD was 3.97% (3.75–4.2), and that almost 60% of people with ADHD also had another psychiatric disorder, with almost 50% of the comorbidly diagnosed individuals having two or more disorders (Mohammadi et al., 2019).
A nationwide study in Turkey examined psychiatric disorders in 5,842 second, third, and fourth grade students (Ercan et al., 2019). ADHD was diagnosed using the DSM-IV-based Screening Scale for Disruptive Behavior Disorders in Children and Adolescents, and impairment was independently assessed by parents and teachers using a 3-point Likert-type scale (Ercan et al., 2019). They found that the overall prevalence of ADHD with and without impairment were 19.5% (18.47–20.5) and 12.4% (11.55–13.24), respectively (Ercan et al., 2019), which was also higher than our estimation. The reason for the higher prevalence is that children in rural areas and those that did not attend school were not able to participate in the study. Furthermore, this study also used screen-based diagnoses, which could also lead to an overestimation (Ercan et al., 2019).
The present study showed the burden of ADHD in MENA was high in terms of the point prevalence, age-standardized incidence, and YLD rates, although they have all substantially decreased since 1990. Although previous studies have reported a high global burden of ADHD (Thomas et al., 2015), they have also reported an increase in prevalence of the disorder (Abdelnour et al., 2022). The increases in ADHD were mainly related to the release of a new DSM edition (Thomas et al., 2015). Furthermore, the estimated prevalence of ADHD has been found to be associated with the source of information (Polanczyk et al., 2014), impairment criteria (Polanczyk et al., 2014), diagnostic criteria (Polanczyk et al., 2014; Thomas et al., 2015), and geographic location (Thomas et al., 2015). Moreover, improved awareness and case identification by primary care professionals, teachers, and parents, as well as more frequent exposure to some of the putative etiologic factors (discussed below) are a few possible explanations for the apparent rise in the prevalence of ADHD over time (Krull, 2022a). The primary source of the discrepancy between our study and previous studies is that age and gender were standardized in our studies, whereas previous studies did not adjust their results based on age. Accordingly, our findings should be interpreted with some degree of caution.
The economic burden of ADHD has been found to range from $US831.38 to $20,538 annually per person in high-income countries (Chhibber et al., 2021), and delays in diagnosis and treatment lead to higher long-term costs (Daley et al., 2019). For children, the cost burden was primarily related to health care and educational services, whereas for adults the costs were primarily related to lost wages and productivity (Doshi et al., 2012). More research needs to be done in the MENA region and its constituent countries, in order to more accurately estimate the economic effects and improve the standardization of the cost. Considering the high epidemiologic and economic burden of ADHD, and its long-term consequences, ADHD is a serious public health issue.
National guidelines recommend using stimulant and non-stimulant pharmacotherapy as the first line of treatment (Wolraich et al., 2020; Cortese, 2020), since previous meta-analysis have found favorable outcomes and that they are safe (Cortese, 2020). ADHD pharmacotherapy improves clinician-rated core symptoms (Cortese et al., 2018), as well as caregiver-child interactions, academic performance, and aggressive behaviors (Floet et al., 2010). Methylphenidate and amphetamine are the preferred stimulant drugs for children and adults (David Brent & Solanto, 2023; Krull, 2022b), respectively, and are more potent than non-stimulant drugs like atomoxetine (Cortese et al., 2018). Although amphetamines are slightly more efficacious than methylphenidates, they have more adverse effects and a higher risk of treatment cessation (Cortese et al., 2018). Treatment tolerability plays an essential role in the long-term treatment of chronic conditions. Even though combined medication and behavior/psychological therapy were not superior to pharmacotherapy alone in improving core symptoms (Van der Oord et al., 2008), combined treatment could address some problems that medication treatment alone was insufficient to address, such as organizational skills and co-occurring emotional and behavioral symptoms (Chan et al., 2016). Many countries have reported an increasing use of psychostimulant prescriptions for ADHD (Bachmann et al., 2017), which has highlighted concerns about the misdiagnosis of non-ADHD individuals. A recent systematic review and meta-analysis found that the pooled pharmacological treatment rates for people with ADHD and people without ADHD were 0.191 (0.115 to 0.299) and 0.009 (0.005 to 0.017), respectively (Massuti et al., 2021). This means that people with ADHD are not getting enough medication, while people without ADHD are getting too much medication or are misusing it (Massuti et al., 2021).
Tertiary healthcare and psychiatric services in most resource-limited countries are only available in large cities, and most of the population does not have access to these centers. In this situation, primary health care physicians can play a pivotal role in diagnosing and managing ADHD. However, several studies have revealed that primary healthcare physicians have inadequate knowledge of about ADHD (Al-Ahmari et al., 2018; Beheshti et al., 2021; Ghanizadeh & Zarei, 2010; Jawaid et al., 2008). Therefore, physicians should be empowered to properly diagnose and treat ADHD by revising curricula and providing additional educational courses on ADHD. Furthermore, in order to provide valid and practical solutions, especially for primary health care services in resource-limited countries, adapting clinical practice guidelines to their local health context, instead of de-novo developing clinical practice guidelines, can help improve evidence-based healthcare quality and safety (Amer et al., 2019; Bashiri et al., 2021).
The early detection and treatment of ADHD can reduce its burden (Daley et al., 2019), meaning that screening for ADHD in the pre-school setting could help to reduce the burden of ADHD. The Adult ADHD Self-Report Scale and ADHD-specific rating scales are suitable practical tools to assess ADHD in primary care for adults (Chamberlain et al., 2021; Kessler et al., 2006) and children (Collett et al., 2003), respectively. It is important to remember that these tools have a validated age limit and can only be used as screening tools, and that further testing is needed to confirm an ADHD diagnosis.
Study Strengths and Limitations
The current study provided the first and most recent information about the burden of ADHD and the trends associated with this disorder at the national and regional level by age, sex, and SDI. However, this study also has limitations, which are similar to those of earlier GBD studies (GBD 2019 Demographics Collaborators, 2020; GBD 2019 Diseases and Injuries Collaborators, 2020; GBD 2019 Risk Factors Collaborators, 2020). Firstly, it should be noted that in some nations the estimates reported here were based on models created in DisMod-MR 2.1, due to the dearth of population-based national data on the incidence and prevalence rates of ADHD (GBD 2019 Diseases and Injuries Collaborators, 2020). In order to create the most accurate estimate possible, models based on some predictor factors from nations with comparable conditions were created (GBD 2019 Diseases and Injuries Collaborators, 2020). Therefore, the national estimates should be treated with some caution, especially for nations that are dealing with the negative effects of conflict, like Yemen, Afghanistan, and Sudan.
GBD 2019 calculated the YLD of ADHD using its disability weight (GBD 2019 Diseases and Injuries Collaborators, 2020). The disability weight was equal to 0.045 (0.028–0.066) with a lay description of hyperactivity and difficulty in concentrating, remembering, and completing tasks, which indicates a mild ADHD presentation (GBD 2019 Diseases and Injuries Collaborators, 2020). However, ADHD is a disorder with a broad spectrum of presentations and adverse effects, so it is not correct to summarize the disability of ADHD into one narrow-interval disability weight. GBD 2019 estimated the proportion of time with disability in ADHD individuals as an “average case” based on data from only one survey (Erskine et al., 2014; GBD 2019 Diseases and Injuries Collaborators, 2020). Using only one survey to estimate the case average is insufficient to generalize survey findings to other ADHD patients with diverse ethnicities and geographical differences. In addition, ADHD subtypes have various clinical presentations and correlated comorbidities, which alters its burden. Therefore, further studies are needed to categorize and estimate the burden of ADHD based on its severity, case average across various locations, and subtypes.
The maximum onset age of ADHD was set at 12 years old (GBD 2019 Diseases and Injuries Collaborators, 2020), but adult ADHD onset can occur in individuals older than 12 years old. Further studies are needed to estimate the incidence in people older than 12 years. In addition, studies using different ADHD diagnosis methods could alter the results, particularly the diagnostic criteria of ADHD at various time intervals. Further studies are also needed to adjust the results based on the method used to diagnose ADHD.
Conclusions
The present study found a substantial decrease in the epidemiological burden of ADHD in MENA over the period 1990 to 2019. However, the epidemiological burden of ADHD in MENA is higher than the global burden and ADHD remains a serious public health issue in the region. Given the high epidemiological and economic burden of ADHD, and its various complications, there is an increasing need to regularly update epidemiological information and to design efficient, practical guidelines for the early detection and treatment of ADHD in the MENA countries.
Supplemental Material
sj-docx-4-jad-10.1177_10870547231187161 – Supplemental material for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019
Supplemental material, sj-docx-4-jad-10.1177_10870547231187161 for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019 by Saeid Safiri, Seyed Ehsan Mousavi, Seyed Aria Nejadghaderi, Maryam Noori, Mark J. M. Sullman, Shahrokh Amiri and Ali-Asghar Kolahi in Journal of Attention Disorders
Supplemental Material
sj-docx-5-jad-10.1177_10870547231187161 – Supplemental material for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019
Supplemental material, sj-docx-5-jad-10.1177_10870547231187161 for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019 by Saeid Safiri, Seyed Ehsan Mousavi, Seyed Aria Nejadghaderi, Maryam Noori, Mark J. M. Sullman, Shahrokh Amiri and Ali-Asghar Kolahi in Journal of Attention Disorders
Supplemental Material
sj-docx-6-jad-10.1177_10870547231187161 – Supplemental material for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019
Supplemental material, sj-docx-6-jad-10.1177_10870547231187161 for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019 by Saeid Safiri, Seyed Ehsan Mousavi, Seyed Aria Nejadghaderi, Maryam Noori, Mark J. M. Sullman, Shahrokh Amiri and Ali-Asghar Kolahi in Journal of Attention Disorders
Supplemental Material
sj-docx-7-jad-10.1177_10870547231187161 – Supplemental material for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019
Supplemental material, sj-docx-7-jad-10.1177_10870547231187161 for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019 by Saeid Safiri, Seyed Ehsan Mousavi, Seyed Aria Nejadghaderi, Maryam Noori, Mark J. M. Sullman, Shahrokh Amiri and Ali-Asghar Kolahi in Journal of Attention Disorders
Supplemental Material
sj-jpg-1-jad-10.1177_10870547231187161 – Supplemental material for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019
Supplemental material, sj-jpg-1-jad-10.1177_10870547231187161 for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019 by Saeid Safiri, Seyed Ehsan Mousavi, Seyed Aria Nejadghaderi, Maryam Noori, Mark J. M. Sullman, Shahrokh Amiri and Ali-Asghar Kolahi in Journal of Attention Disorders
Supplemental Material
sj-jpg-2-jad-10.1177_10870547231187161 – Supplemental material for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019
Supplemental material, sj-jpg-2-jad-10.1177_10870547231187161 for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019 by Saeid Safiri, Seyed Ehsan Mousavi, Seyed Aria Nejadghaderi, Maryam Noori, Mark J. M. Sullman, Shahrokh Amiri and Ali-Asghar Kolahi in Journal of Attention Disorders
Supplemental Material
sj-jpg-3-jad-10.1177_10870547231187161 – Supplemental material for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019
Supplemental material, sj-jpg-3-jad-10.1177_10870547231187161 for The Burden of Attention-Deficit Hyperactivity Disorder (ADHD) in the Middle East and North Africa Region, 1990 to 2019 by Saeid Safiri, Seyed Ehsan Mousavi, Seyed Aria Nejadghaderi, Maryam Noori, Mark J. M. Sullman, Shahrokh Amiri and Ali-Asghar Kolahi in Journal of Attention Disorders
Footnotes
Acknowledgements
We would like to thank the Institute for Health Metrics and Evaluation staff and its collaborators who prepared these publicly available data. We would also like to thank the Clinical Research Development Unit of Tabriz Valiasr Hospital, Tabriz University of Medical Sciences, Tabriz, Iran for their assistance in this research.
Authors’ Note
This study is based on publicly available data and solely reflects the opinions of its authors and not that of the Institute for Health Metrics and Evaluation.
Authors’ Contributors
SS and AAK designed the study. SS analyzed the data and performed the statistical analyses. SS, SEM, SAN, MN, MJMS, SA and AAK drafted the initial manuscript. All authors reviewed the drafted manuscript for critical content. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Bill and Melinda Gates Foundation, who were not involved in any way in the preparation of this manuscript, funded the GBD study. The Shahid Beheshti University of Medical Sciences, Tehran, Iran (Grant No. 43003462) also supported the present report.
Ethics Approval and Consent to Participate
The present study was approved by Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (IR.SBMU.RETECH.REC.1401.582).
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.