
Abstract
Objectives:
To explore the effect of health promotion program (HPP) on stress, quality of life, health-promoting lifestyles, and children’s attention-deficit/hyperactivity disorder (ADHD) symptoms in parents of children with ADHD.
Methods:
Sixty parents of children with ADHD were equally randomized into the intervention (health promotion program) and control (usual care) groups. Outcomes included parents’ stress, quality of life, health-promoting lifestyles, and children’s ADHD symptoms before, immediately after, and 1, 3, and 6 months after the intervention. The GEE was used to evaluate the effectiveness.
Results:
The intervention group reported significant improvement in the children’s hyperactivity/impulse and opposition at the 6- and 3-month, respectively. Parental overall stress significantly improved at 3 and 6 months. Parents’ quality of life had significant effects at the immediate, 3-month, and 6-month. Self-actualization behavior for health-promoting lifestyles had significant effects at the immediate follow-up.
Conclusion:
HPP can promote the mental well-being of parents of children with ADHD.
Introduction
Attention-Deficit/Hyperactivity Disorder and Its Impacts on Children and Their Families
Attention-deficit/hyperactivity disorder (ADHD) is among the most common neurodevelopmental behavioral conditions in children, it manifests as attention deficits, hyperactivity, and impulsivity (Perou et al., 2013). Its estimated prevalence in children is 7.2% worldwide (Thomas et al., 2015) and 5%–10% in Taiwan (Gau et al., 2005). A national population-based study in Taiwan including patients with ADHD aged <18 years revealed that the prevalence increased from 0.06% in 1996 to 1.64% in 2005 (Chien et al., 2012). Another nationwide survey in Taiwan from 2000 to 2011 observed that the prevalence of ADHD ranged from 0.11% to 1.24% (Wang et al., 2017). Among Taiwanese children, the prevalence of ADHD is higher in boys than in girls (Chien et al., 2012; Wang et al., 2017). A diagnosis of ADHD in children is often associated with long-term social, emotional, and cognitive function impairment (Barkley, 2014). Children with combined-type ADHD have poorer school performance and interpersonal interaction skills (Tzang et al., 2007). ADHD moderately influences the quality of life of children and seriously affects their psychosocial field, including emotions, society, and school (Lee et al., 2016). ADHD symptoms can persist through adulthood and affect the marital relationships of their parents (Harpin, 2005).
The challenges imposed by children with ADHD not only influence parent–child relationships but also affect family function and increase parental stress (Turan et al., 2022). ADHD severity in children negatively affects parents’ quality of life, especially psychological factors, personal satisfaction, family interactions, and daily activities (Cappe et al., 2017), and is associated with parental stress (Li et al., 2016). Families of children with ADHD have more interpersonal conflicts, depression, isolation, and negativity than those of children without ADHD (Ferrin et al., 2014; Kendall & Tabacco, 2011; Loren et al., 2015). Parents of children with ADHD experience frustration, stress, depression, and anxiety (Krahé et al., 2015; Lesesne et al., 2003). A higher level of parental stress was reported in the primary caregivers of children with ADHD who had a comorbidity than in those who did not have any comorbidity (Tzang et al., 2007). Parents of children with ADHD used more dysfunctional coping styles, such as avoidant-focused coping, than did parents of children without ADHD (Craig et al., 2020). A Brazilian study revealed a lower social and environmental quality of life in caregivers of children with ADHD than in the normative data (Andrade et al., 2016). In addition to psychosocial challenges, the parents of children with developmental disorders, such as ADHD, have elevated physical health risk because of sleep disturbances, headache, gastrointestinal and respiratory problems (Cantwell et al., 2014), and obesity (Gallagher & Hannigan, 2015). Accordingly, health promotion interventions are urgently needed for caregivers to obtain positive outcomes for both caregivers and children (Chafouleas et al., 2020).
The Parent Programs
Evidence-based treatment for ADHD includes both pharmacological and behavioral interventions, and complementary treatment strategies may be necessary for treating residual symptoms such as core symptoms and family stress (Turan et al., 2022). The most commonly accepted complementary strategies in children with ADHD are school-based interventions and parenting programs (Sonuga-Barke et al., 2013). Turan et al. (2022) reviewed 17 parenting programs, such as the Parents Plus Children’s Programme (Coughlin et al., 2009), and concluded that they significantly improved parental satisfaction, parental stress, and therapeutic goals (Carr et al., 2017; Nitsch et al., 2015; Sharry et al., 2005). However, the Parents Plus Children’s Programme was developed for parents and children to reduce behavioral problems and facilitate parent–child relationships, but it is not specific to ADHD (Coughlin et al., 2009). In addition, a Positive Parenting Program (Triple P) for parents of children with ADHD significantly decreased depression, anxiety, and stress compared with the control group (Tehranidoost et al., 2008). Franke et al. (2020) reported that the Online Parenting Program significantly improved symptoms of hyperactivity, inattention, disturbance, impulsiveness, despisal, attacking, and social function among children with ADHD; the improvements in parental satisfaction, self-efficacy, stress, and depression remained at the 6-month follow-up.
Health Promotion for Caregivers of Children With ADHD
Although most parental programs address children’s ADHD symptoms and parental domains such as stress, self-efficacy, depression, anxiety, and satisfaction, few interventions targeting caregiver health promotion have been conducted. Compared with the general adult population, caregivers of children with developmental disabilities, such as ADHD, autism spectrum disorder, and cerebral palsy, experience more physical health problems, including sleep problems, headaches, gastrointestinal problems, and respiratory problems (Cantwell et al., 2014; Khanna et al., 2011; Miodrag & Hodapp, 2010), and have a higher obesity risk (Gallagher & Hannigan, 2015). Acton (2002) reported that caregivers of children with developmental disabilities had more barriers to health promotion and practice fewer self-care behaviors than does the general population. However, caregivers who practice more health-promoting and self-care behaviors were better protected from stress and negative effects on well-being. Thus, interventions targeting caregiver health promotion are essential to ensure positive outcomes for both children and their caregivers (Chafouleas et al., 2020).
O’Donnell (2009) defined health promotion as the art and science of helping people find synergy between their core desires and optimal health, increasing their motivation to achieve optimal health, and supporting them in changing their lifestyle to move toward optimal health. On the basis of Pender’s health promotion model, health-promoting lifestyle behaviors can be classified into six dimensions: physical activity, nutrition, stress management, spiritual growth, interpersonal relations, and health responsibilities (Kamali et al., 2017). Anderson and Guthery (2015) observed that mindfulness-based psychological education significantly reduced parental stress, parental distress, and parental dysfunction among seven parents of children with ADHD diagnosis or symptoms. A study from Sydney, Australia, reported that Sahaja Yoga meditation improved the behavior, self-esteem, relationship quality, sleep, and anxiety of children with ADHD; in addition, the parents reported having less stress, being happier, and finding managing their children’s behavior easier (Harrison et al., 2004). Beart and Lessing (2013) reported that parents and teachers perceived yoga to positively influence the concentration and behavior of children with ADHD.
Given that a diagnosis of ADHD in children is likely to result in children’s impairment and parental stress, we used a health promotion practice for parents as a strategy to cope with their stress based on the psychological stress and coping theory proposed by Lazarus and Folkman (1984). Transactional explanations of stress emphasize the bidirectional nature of the transactions between people and their environment, experienced as disruptions in equilibrium and adaptive processes for resolving this disequilibrium, which produces stress (Folkman, 1984; Lazarus and Folkman, 1984). When a situation is stressful (primary appraisal) and requires effort to manage (secondary appraisal), coping actions are used (Folkman and Lazarus, 1988). The outcome of coping efforts, accompanied by new information from the environment, results in cognitive reappraisal of the situation to determine whether coping efforts are successful or the nature of the situation changes from stressful to irrelevant or benign-positive (Lazarus and Folkman, 1984). Results of successful adaptation may include positive affect, whereas unsuccessful adaptation may facilitate further coping (Edwards, 1992). Health behaviors, such as eating and exercise, are influenced by stress and often constitute effort to cope with stress (Park & Iacocca, 2014).
Most studies have employed a single intervention, such as yoga (Harrison et al., 2004) or mindfulness relaxation (Anderson & Guthery, 2015). No study has investigated the effects of multifaceted interventions for the caregivers of children with ADHD on parental stress, quality of life, and healthy lifestyles. In addition, few studies have explored the effects of health promotion programs (HPPs) on the stress and quality of life of caregivers of children with ADHD. Developing an HPP integrating knowledge of ADHD, physical activity, nutrition, parental training, related social welfare resources, and mindfulness relaxation and yoga is crucial for caregivers of children with ADHD. We created an HPP containing multiple interventions for parents of children with ADHD. We evaluated its effects on parental stress, quality of life, and health-promoting lifestyles and children’s ADHD symptoms. We hypothesized that the HPP would significantly reduce parental stress and children’s ADHD symptoms, improve quality of life, and enhance health-promoting lifestyles compared with the control treatment.
Methods
Setting and Participants
For this randomized controlled trial, we recruited participants from the outpatient department of the child and adolescent psychiatry department of a medical center in northern Taiwan between July 2017 and April 2018. The inclusion criteria were as follows: (1) Parents being 20–65 years of age and having 7–12years old children with ADHD diagnosed and referred by a pediatric psychiatrist; (2) living together with the children and spending the most time among parents caring for the children; (3) being able to talk, read, and write in Chinese; and (4) providing informed consent. Children between the ages of 7 and 12 are of elementary school age in Taiwan. We excluded (1) caregivers who came to the outpatient department for the first time for an undetermined ADHD diagnosis or (2) the presence of an intellectual disability.
The sample size was estimated using G power 3.1. Considering an α level of .05, β level of .2, and an effect size of .25, on the basis of related studies, and the main outcomes of parenting stress, quality of life, and health promotion lifestyles, the minimum total sample size was estimated to be 22 (Fritz et al., 2012). The attrition rate was estimated to be 35% on the basis of studies (Aghebati et al., 2014; Jones et al., 2015; Kemper et al., 2018), resulting in a minimum sample size of 30 for the intervention and control groups (i.e., N = 60).
Data Collection and Ethical Considerations
Eligible participants were referred by a child psychiatrist who was part of the research team. The trained researcher then arranged the proper time and location to explain the study’s purpose and procedures and obtain informed consent. Randomization into the intervention or control group was performed by a trained independent assessor who was not involved in data collection by using a computerized random-number generator. A single-blind design was employed because blinding participants was not possible and would lead to interference. We collected data in both groups at the following time points: before (pretest) the 8-week intervention and immediately (posttest) and 1, 3, and 6 months after the intervention. A pretest and posttest were administered to parents before and after the intervention, respectively. For follow-up data collection, study instruments were mailed to parents, and they were telephoned to ensure that they received and filled out the forms. Because of research recruitment, different researchers were involved in treatment intervention and follow-up data tracking.
Intervention
The group-based HPP included knowledge on ADHD (including etiology, signs and symptoms, treatment, and prognosis), physical activity, diet and nutrition, parental skills training/stress management, related social welfare resources, mindfulness relaxation, and yoga. A nursing professor with 17 year of experiences in child and adolescent psychiatric nursing and a PhD candidate with 16 years of pediatric nursing experience ran the group. We also invited qualified speakers with professional certificates, including pediatric psychiatrists, dieticians, psychologists, social workers, fitness coaches, yoga, and mindfulness teachers, to give lectures and discussions in the HPP. The intervention group underwent a 90-min HPP intervention a week for 8 weeks. Upon obtaining permission from speakers, group sessions of lecture exclude the section to discuss and disclose personal experience, were video recorded for those participants who could not attend to review after the class. Researchers also contacted parents between group sessions to determine their reasons for absence, needs for group sessions, and other special needs for each parent. In the third month, additional booster classes were arranged for parenting education intervention because of the major needs of this group. The control group received the usual care. We provided the HPP information and multimedia information to the participants in the control group after they completed all the questionnaires. The effectiveness of the intervention was evaluated before, immediately after, and at 1, 3, and 6 months after the intervention. The attendance rates were 83%–100% for every session. However, for participants who missed a certain session, we provided videos for them to review.
The Joint Institutional Review Board of Taipei Medical University approved this study (N201705072).
Measurements
Clinicodemographic and socioeconomic characteristics
For the children with ADHD, we collected data on sex, disease diagnosis, comorbidities, and treatment. For their parents, we collected data on sex, age, occupation, ethnicity, education level, marital status, relationship with their children, family structure, religion, and family income.
The Swanson, Nolan, Pelham, Version IV
The Swanson, Nolan, and Pelham, Version IV (SNAP-IV) is a scale developed based on DSM-IV and fully consistent with the DSM diagnostic criteria; it was translated into Chinese by Dr. Gao (Liu, 2006). DSM-IV approaches psychiatric assessment and the organization of biopsychosocial information by using a multiaxial formulation (Substance Abuse and Mental Health Services Administration, 2016). The questionnaires commonly used by clinicians are used as a reference to understand children’s attention condition. The scales can assist in clinical assessments, the diagnosis of ADHD, treatment effectiveness assessments, and community or school screening. The common version (MTA SNAP-IV) has 26 questions for 6–13-year-old children across the following subscales: inattention (questions 1–9), hyperactivity/impulse (questions 10–18), and opposition and defiance (questions 19–26). The three subscales of the Chinese version of SNAP-IV had high correlation coefficients with the CBCL (r = .51–.72), with good internal consistency (Cronbach’s α >.88; Liu, 2006). In this study, SNAP-IV was administered to parents to measure their children’s ADHD symptoms.
Parenting Stress Index-Short Form
Our study used a modified version of Abdin’s Parenting Stress Index-Short Form, with 24 questions (Liu, 2015). The short-form version is divided into three subscales: parental distress, parent–child dysfunctional interaction, and difficult child, with Cronbach α for the Chinese version (total score) being .95 (Jen, 1995), indicating reliability.
World Health Organization Quality of Life Questionnaire
We used the brief version of the World Health Organization’s Quality of Life (WHOQOL-BREF) Taiwan version, which has 28 questions that are similar and well associated psychometrically with the global version (Yao, 2002), for the quality of life assessment of the primary caregivers. The Cronbach α for the total score in this questionnaire is .95. The score of the question was calculated from 1 to 5 points. All the questions are turned in the same direction. The higher the total score is, the better the quality of life is. The Taiwan Concise Questionnaire Development Group emphasizes that the Taiwan version of the WHOQOL-BREF is characterized by a subjective feeling of culture and values and reflects the multifaceted and refined nature of health-related quality of life.
Health-Promoting Lifestyle Profile
We used the Chinese version and revised it on the basis of the Health-Promoting Lifestyle Profile by Chen et al. (1997), originally developed by Walker et al. (1987). It has 40 items across six dimensions: self-actualization, health responsibility, exercise, nutrition, interpersonal support, and stress management. It has been used by many domestic research institutes and has satisfactory reliability and validity. The Cronbach’s α of the total scale was .92, and that of the subscales was .69–.84. This scale can explain 48.19% of the total variance in health promotion lifestyles (Chen et al., 1997).
Statistical Analysis
SPSS v22 was used for the data collation and statistical analysis. We used an intention-to-treat analysis. Categorical variables are presented as percentages, and continuous variables are presented as means and standard deviations (SDs). The chi-square, independent t test, and single-factor variation numerical analysis were used for within-group and between-group comparisons. The effect of the HPP intervention was analyzed using the generalized estimating equation (GEE). According to Cohen’s guidelines, phi coefficients of .10, .30, and .50 were interpreted as indicating small, medium, and large effect sizes, respectively (Cohen, 1988; Cohen, 1992).
Results
Of the 72 participants initially deemed eligible, 12 refused to participate because they did not have time to join the courses. Ultimately, 60 parents of children with ADHD were included and randomly and equally divided into the intervention (HPP) group or the control (usual care) group (n = 30 each). None of the participants had taken any courses related to HPP. Two participants in the control group refused to attend the 6-month follow-up because they found the follow-up period too long and did not have free time to complete the questionnaires (Figure 1).
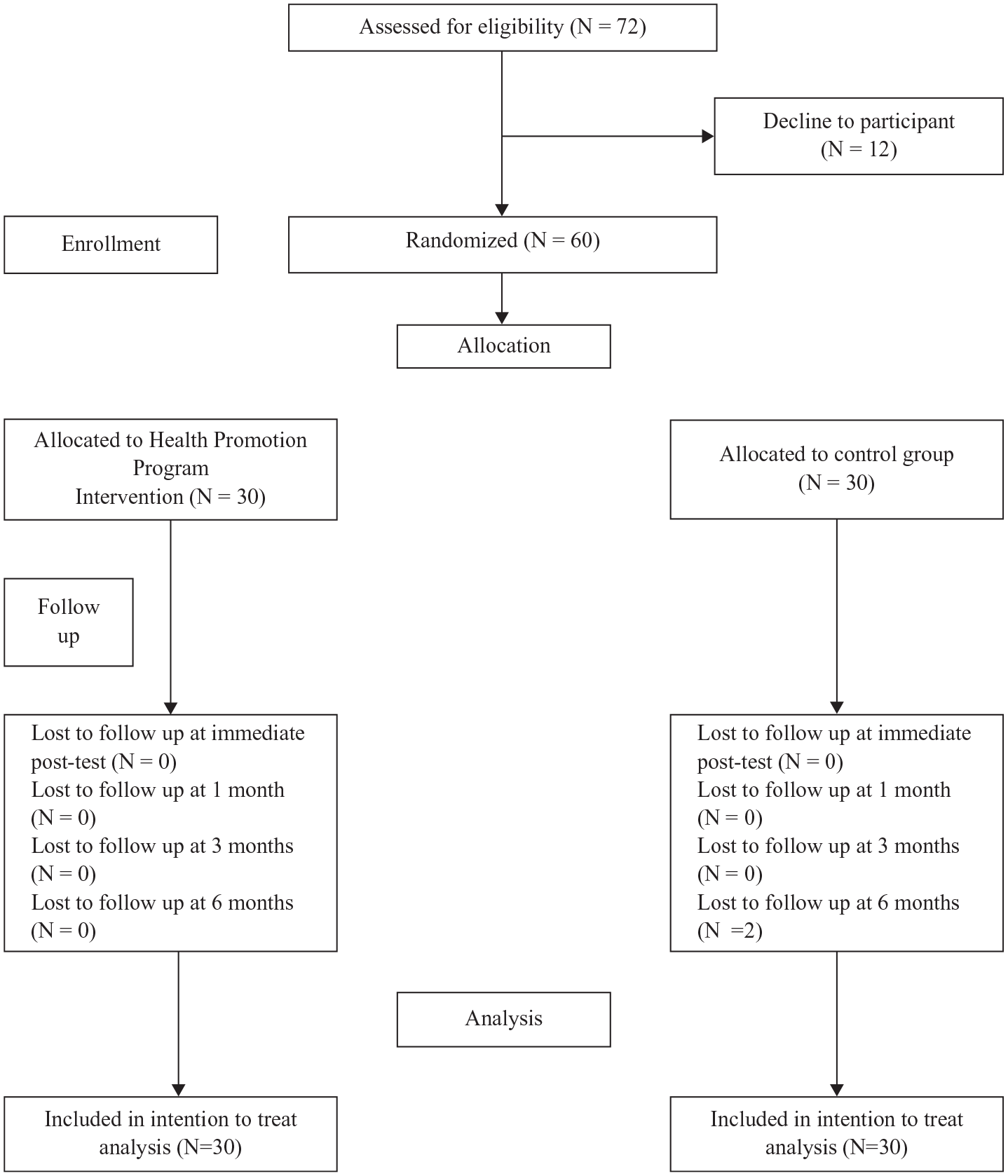
CONSORT 2010 flow diagram.
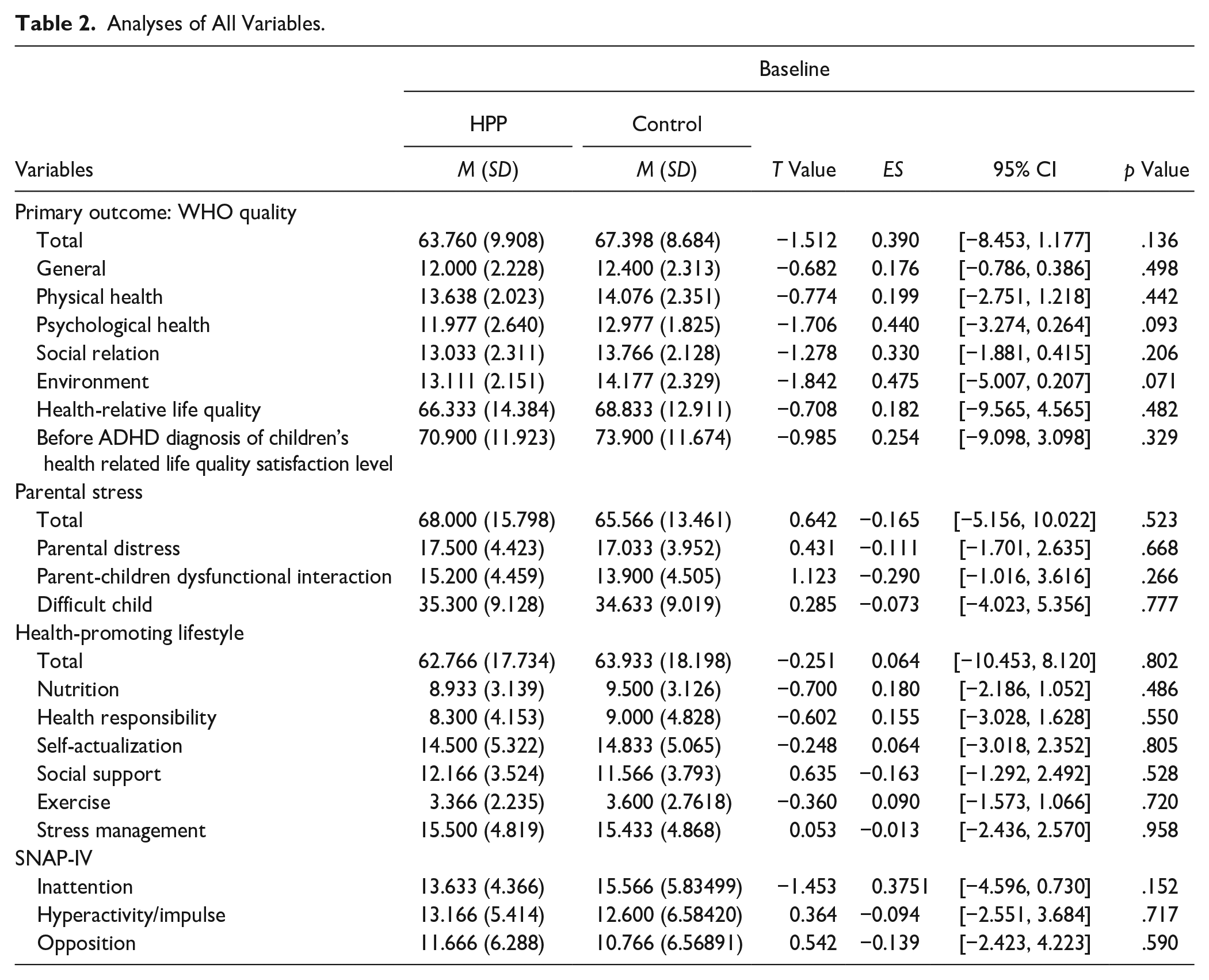
Table 1 presents the demographic data of both groups. No significant between-group differences were observed in age, health condition, number of children, education level, and medical treatment (all p > .05). Table 2 presents the baseline mean and SD; the baseline outcome variables did not differ between groups. Table 2 presents the effect sizes and 95% confidence intervals (CIs). Figure 2 illustrates significant changes in the hyperactivity/impulse and opposition subscales of SNAP-IV and the self-actualization behavior subscale of the Health-Promoting Lifestyle Profile. Changes in parental stress are presented in Figure 3. Figure 4 reveals significant changes in the WHO quality of life. The three figures compare the scores of the intervention and control groups at baseline, the immediate posttest, and at the 1-, 3-, and 6-month follow-ups.
Characteristics of Study Participants (N = 60).

Independent t tests.
Chi-squared test.
Analyses of All Variables.
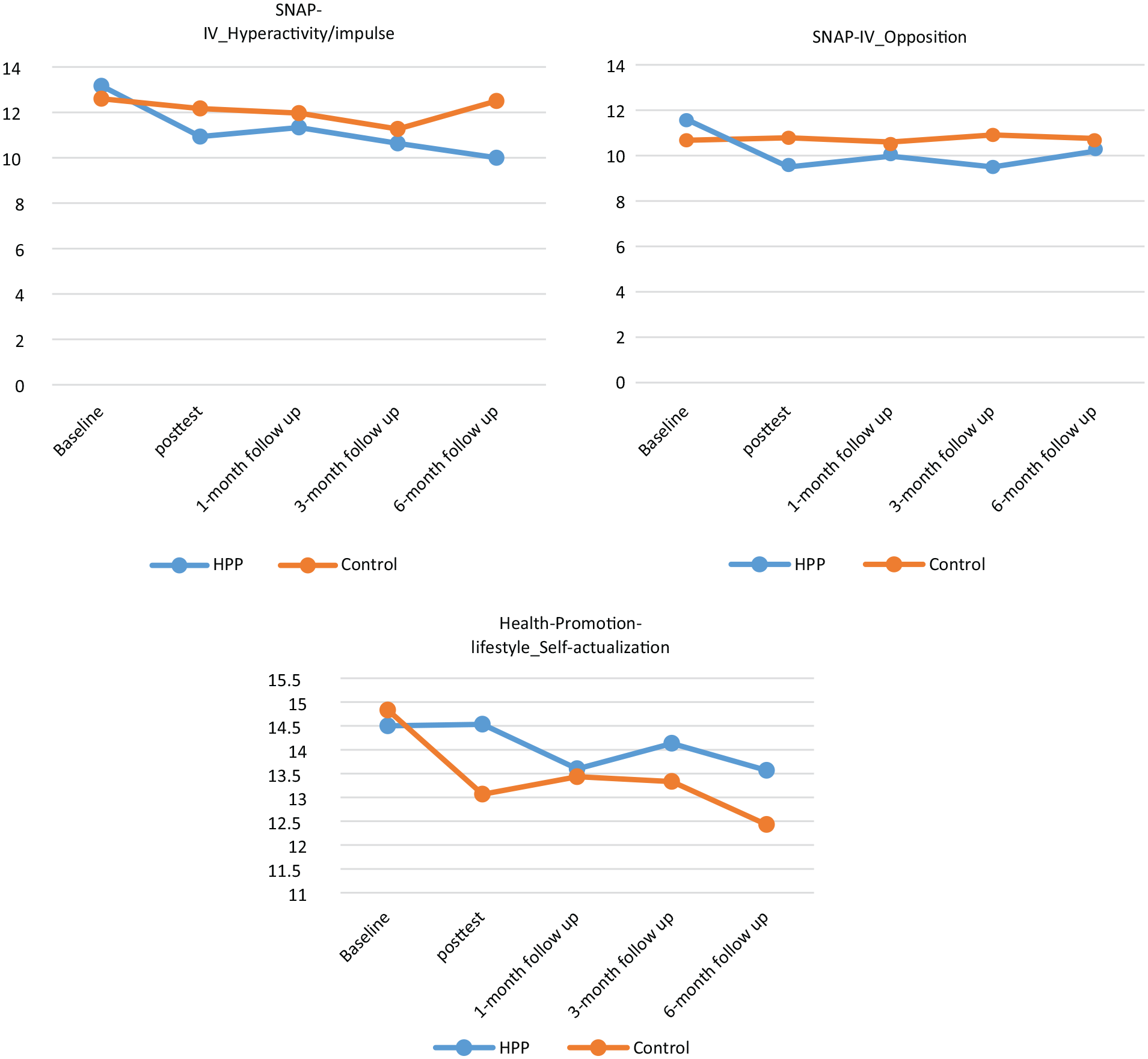
Changes in SNAP-IV and health promotion lifestyle scores.
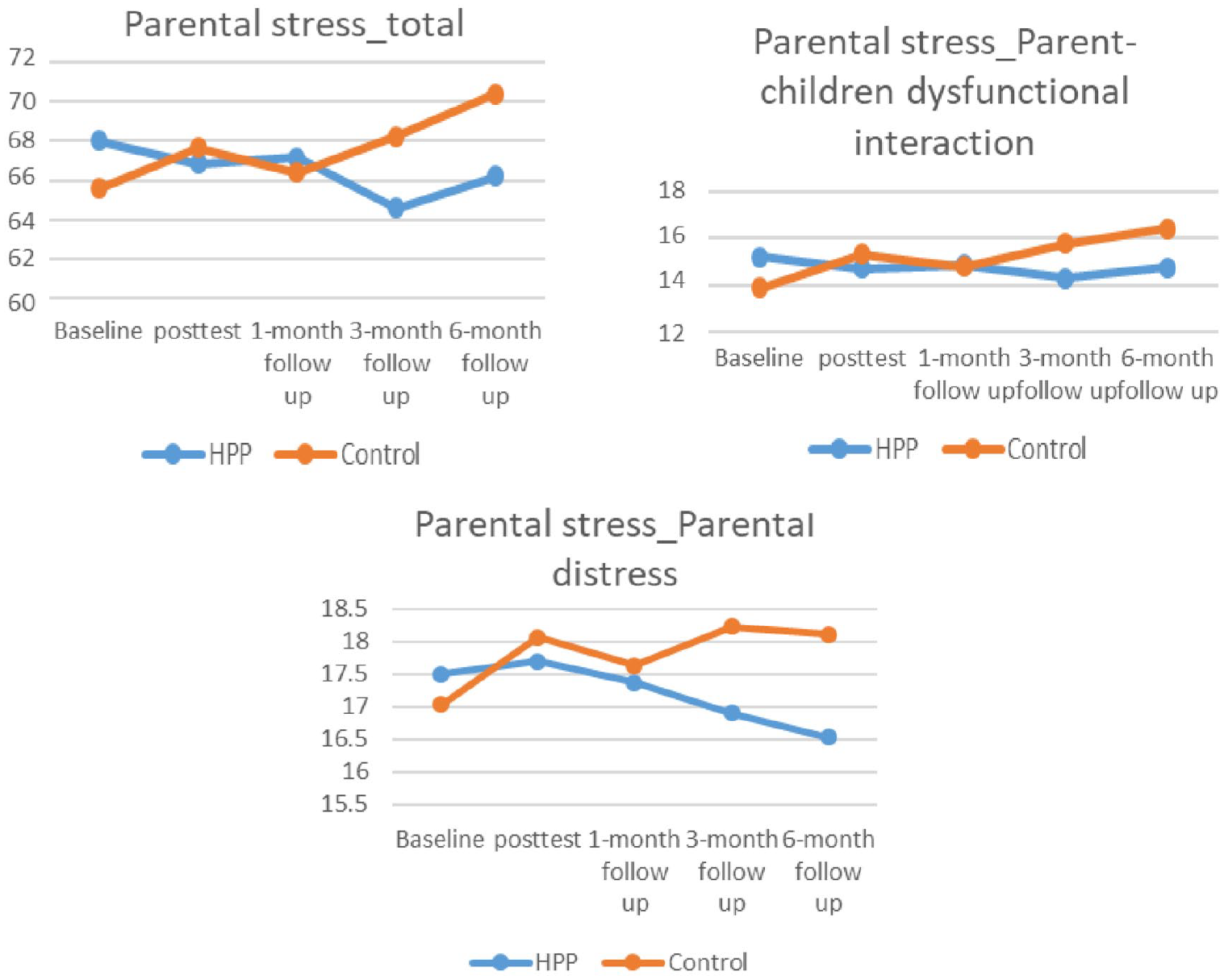
Changes in parental stress.

Changes in WHO quality of life.
The GEE analysis for the SNAP-IV revealed that the intervention and control groups had a significant interaction effect in hyperactivity/impulse subscale scores at the 6-month follow-up (p = .020, ES = 0.300, CI [−7.426, −0.634]) and opposition subscale (p = .036, ES = 0.270, CI [−5.264, −0.173] at the 3-month follow-up (Table 3), indicating that the HPP intervention significantly reduced the children’s hyperactivity and impulsiveness at the 6-month follow-up and opposition at the 3-month follow-up.
GEE Analysis of SNAP-IV.
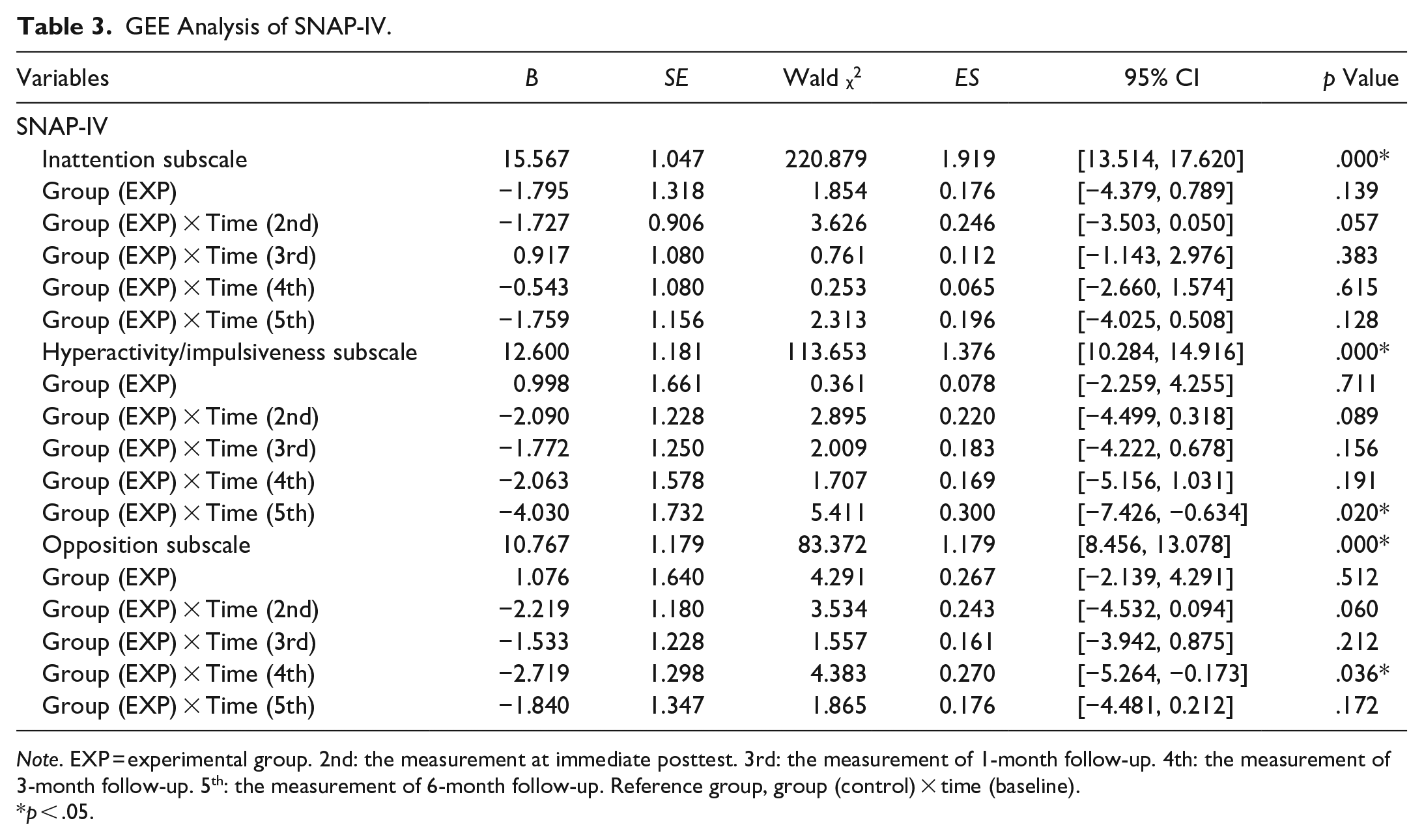
Note. EXP = experimental group. 2nd: the measurement at immediate posttest. 3rd: the measurement of 1-month follow-up. 4th: the measurement of 3-month follow-up. 5th: the measurement of 6-month follow-up. Reference group, group (control) × time (baseline).
p < .05.
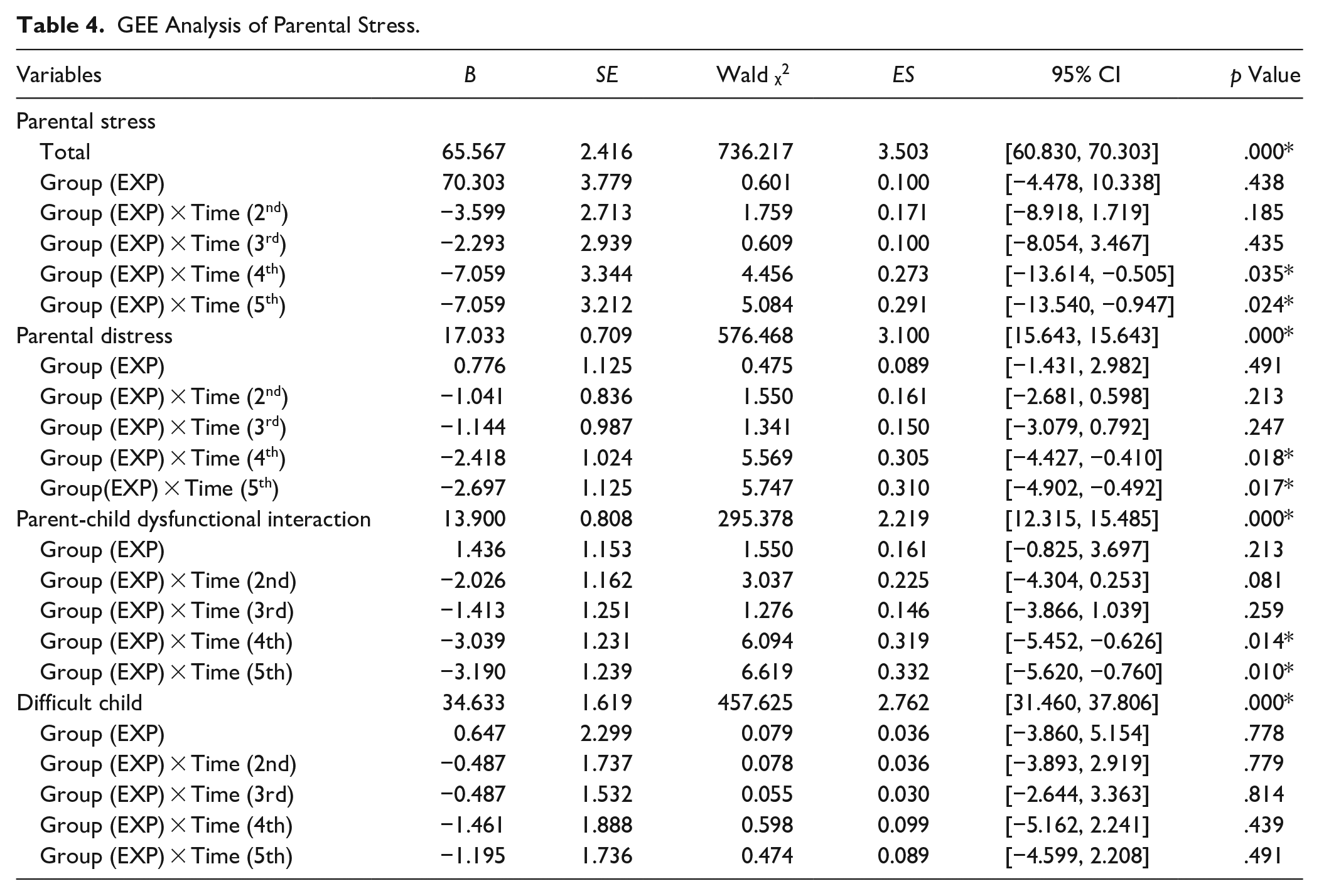
The GEE analysis of the Parenting Stress Index-Short Form revealed that the total score of parental stress had a significant interaction effect at 3- and 6-month follow-up (p = .035, ES = 0.273, CI [−13.614, −0.505] and p = .024, ES = 0.291, [−13.540, −0.947] respectively). The parental distress subscales had a significant effect at the 3- and 6-month follow-ups (p = .018, ES = 0.305, CI [−4.427, −0.410] and p = .017, ES = 0.310, [−4.902, −0.492], respectively). The parent–child dysfunctional interaction subscales exhibited significant differences at the 3- and 6-month follow-ups (p = .014, ES = 0.319, [−5.452, −0.626] and p = .010, ES=0.332, [−5.620, −0.760], respectively), indicating that the HPP intervention significantly reduced parental distress and parent–child dysfunctional interaction at the 3- and 6-month follow-ups (Table 4). The difficult child subscale scores did not significantly differ at any time.
GEE Analysis of Parental Stress.
The GEE analysis of the WHOQOL-BREF revealed that total scores significantly differed at the posttest and 3- and 6-month follow-ups (p = .038, ES = 0.268, [0.190, 6.704]; p =.049, ES = 0.254, [0.014, 9.259]; and p =.016, ES = 0.311, [1.211, 11.746], respectively), indicating that the HPP intervention significantly improved the quality of life of the parents at the posttest and 3- and 6-month follow-ups. The psychological health domain scores significantly differed at the posttest (p = .024, ES = 0.290, [0.143, 2.085]), implying that the HPP intervention significantly improved the psychological health domain of the parents at the posttest. The social relation domain scores exhibited significant differences at the 3- and 6-month follow-ups (p = .044, ES = 0.260, [0.026, 2.033] and p = .038, ES = 0.268, [0.060, 2.070]), implying that the HPP intervention significantly improved the social relation domain of the parents at the 3- and 6-month follow-ups. The environment domain scores exhibited significant differences at the posttest and 1-, 3-, and 6-month follow-ups (p = .004, ES = 0.370, [0.307, 1.634]; p =.017, ES = 0.307, [0.184, 1.917]; p = .015, ES = 0.313, [0.246, 2.327] and p = .038, ES = 0.267, [0.068, 2.480], respectively), indicating that the HPP intervention significantly improved the environment domain of the parents at the posttest and 1-, 3-, and 6-month follow-ups. For the health-related quality of life, satisfaction level was significantly different at the 6-month follow-up (p = .019, ES = 0.303, [1.750, 19.508]), indicating that the HPP intervention significantly improved the satisfaction level of the parents at the 6-month follow-up (Table 5).
GEE Analysis of WHO Quality of Life.
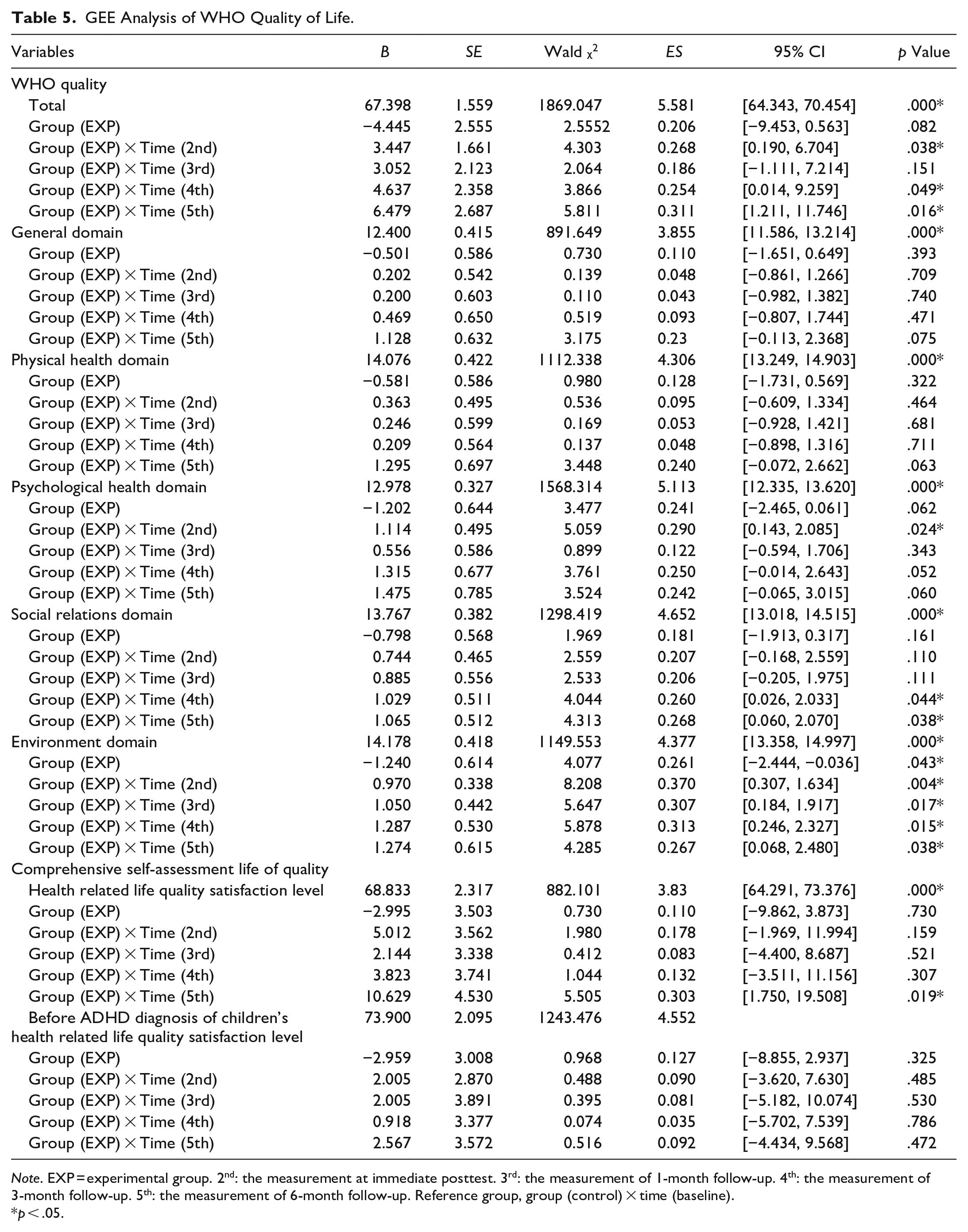
Note. EXP = experimental group. 2nd: the measurement at immediate posttest. 3rd: the measurement of 1-month follow-up. 4th: the measurement of 3-month follow-up. 5th: the measurement of 6-month follow-up. Reference group, group (control) × time (baseline).
p < .05.
The GEE analysis of the Health-Promoting Lifestyle Profile revealed that the self-actualization behavior subscale scores significantly improved at the posttest (p = .032, ES = 0.177, [1.681, 4.001]) (Table 6).
GEE Analysis of Health-Promoting Lifestyle.
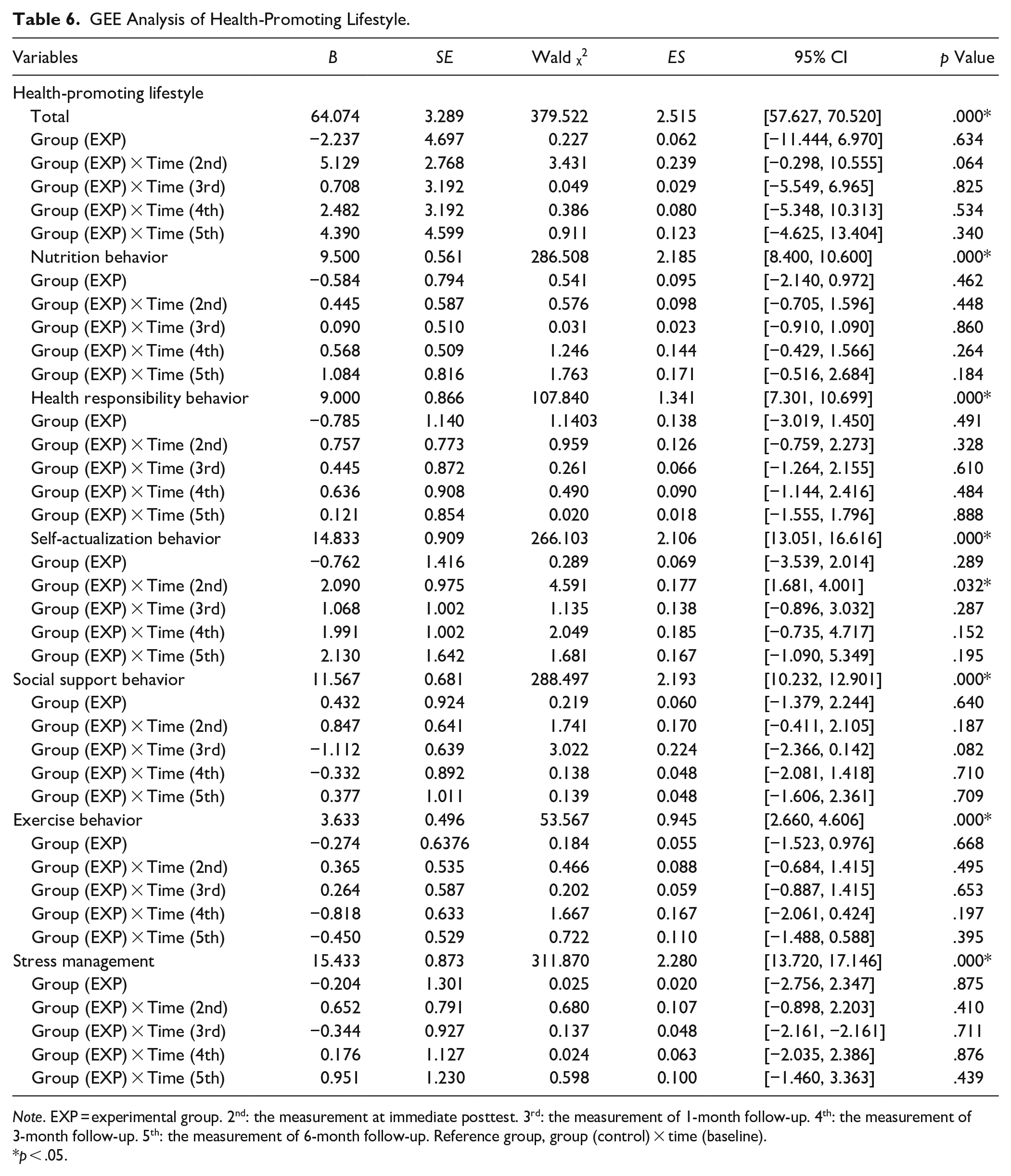
Note. EXP = experimental group. 2nd: the measurement at immediate posttest. 3rd: the measurement of 1-month follow-up. 4th: the measurement of 3-month follow-up. 5th: the measurement of 6-month follow-up. Reference group, group (control) × time (baseline).
p < .05.
Discussion
This study explored the effects of HPP on parental stress, quality of life, and health-promoting lifestyles among parents of children with ADHD and on their children’s ADHD symptoms. Our results revealed that the eight weekly sessions of the HPP intervention significantly reduced the children’s hyperactivity and impulsiveness (as evidenced by SNAP-IV scores) at the 6-month follow-up and opposition at 3-month follow-up. In addition, parental overall stress, parental distress and parent–child dysfunction interaction significantly improved at the 3- and 6-month follow-ups. Parents’ overall quality of life demonstrated significantly improved effect at the immediate, 3-month, and 6-month follow-ups. Parents’ self-actualization behavior of the health promotion lifestyle had significant effects at the immediate post-intervention follow-up.
Children’s ADHD Symptoms
We observed that the HPP intervention significantly reduced the children’s hyperactivity and impulsiveness at the 6-month follow-up and opposition at 3-month follow-up. Consistently, a study indicated children’s symptoms of inattention/hyperactivity decreased after a 6-month online parenting program compared with baseline (Franke et al., 2020). Similarly, a systematic review by (Zwi et al., 2011) stated that parent training may positively affect the behavior of children with ADHD. Behbahani et al. (2018) reported that mindfulness training administered to the parents of children with ADHD reduced parenting stress, making them calmer and preventing parent–child conflict, leading to a decrease in ADHD symptoms in their children.
Parenting Stress
Parental overall stress, parental distress and dysfunctional parent–child interaction significantly decreased at the 3- and 6-month follow-ups, consistent with other studies. Elgendy et al. (2021) and Behbahani et al. (2018) reported that mindful parenting training reduced parenting stress in an intervention group compared with a control group and improved the mindfulness of parents of children with ADHD. Another study concluded that an online parenting program reduced parenting stress in the intervention group compared with the delayed-intervention group (Franke et al., 2020). By contrast, Wiener et al. (2016) discovered that parents of adolescents with ADHD had more stress regarding their children’s challenging behaviors than did parents of adolescents without ADHD. Another study concluded that parenting stress was associated with the ADHD symptoms of their children and adolescents (Biondic et al., 2019). Parents attribute their high stress to the behavior of their children with ADHD, lack of support, and social stigma (Leitch et al., 2019). Thus, interventions such as the HPP in the current study can provide the support that parents need to reduce their stress related to their children’s condition.
Parental Quality of Life
A Brazilian study reported that ADHD caregivers had lower WHOQOL scores in all domains except the physical domain (Andrade et al., 2016). A meta-analysis revealed that parents of children with mental impairments including ADHD had lower quality of life than did those of healthy children (Dey et al., 2019). However, in our study, total scores in the quality of life for parents significantly improved at posttest and the 3- and 6-month follow-ups and environment domains for parents significantly at posttest and the 1-, 3- and 6-month follow-ups. In addition, the scores in the psychological health domain significantly improved immediately after the HPP, and the health-related quality of life satisfaction level was significantly high at the 6-month follow-up. Consistently, Velõ et al. (2019) observed that the quality of life of parents of children with ADHD increased after multimodal treatment. Another study indicated that therapeutic conversation significantly improved the quality of life of parents of adolescents with ADHD (Gisladottir & Svavarsdottir, 2017). To mitigate the negative effects of the child’s ADHD on the parents’ quality of life, Cappe et al. (2017) recommended that parents undergo training programs to improve their parenting skills, parental functions, and perceptions of their children’s behavior. This can help them pay attention to their children’s good behavior, use positive reinforcement, and provide effective directives, thereby improving quality of life. Our data indicate that our HPP intervention can be useful in this regard.
Parental Health-Promoting Lifestyles
Our results indicate that self-actualization behaviors of health-promoting lifestyles among parents of children with ADHD had significantly improved at the posttest, likely because they interacted with therapists and other parents during the HPP. According to our review of the literature, this study is the first to explore the effects of HPP on health-promoting lifestyles. Self-actualization involves individuals harnessing their abilities and potential to create a purposeful life, work toward their goals, remain optimistic about life, and foster positive growth and change (Walker et al., 1987). Parents in the HPP group interacted with the therapists and other parents, and the social environment helped them identify their ideals and talents and harness their physical and mental potential. The effects of the intervention were positive but had a small effect size (0.177, CI [1.681, 4.001]).
Conclusion
Our findings indicate that the eight-session HPP intervention significantly reduced hyperactivity/ impulsiveness and opposition in the children with ADHD, lowered parental stress, increased the quality of life of the parents, and improved the self-actualization behaviors of health promoting lifestyles among parents.
This study has several strengths. Our self-developed HPP integrated multimodal interventions, including knowledge of ADHD and medication, physical activity, nutrition, parental training, related social welfare resources, and mindfulness relaxation and yoga. By integrating multiple dimensions of interventions, parents’ outcomes such as parental stress, quality of life, and health-promoting lifestyles as well as children’s ADHD symptoms can be improved.
Our results have valuable implications for clinical practice. Group interventions, such as health promotion for parents, should be offered in the outpatient department to provide proper education and support for parents of children with ADHD. Studies should adopt health promotion materials and programs to effectively support parents in various settings, including homes, schools, and community organizations, and to prevent disparities in chronic disease and promote health in this population.
Limitations
This study has some limitations. We did not validate SNAP-IV with a clinical diagnosis interview in this population. This is important because the wording of SNAP-IV may not always be understood in all populations. Therefore, the tool’s accuracy remains unclear until it is validated against interview-based diagnosis. Second, because the sample was small and the effect sizes were small to medium, additional studies with larger samples are warranted to support the results of this study. Third, all participants were parents, which limits the generalizability of the results to all caregivers of children with ADHD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.