
Abstract
Objective:
Exploring how abnormal brain function in children with ADHD affects executive function and ultimately leads to behavioral impairment provides a theoretical basis for clinically targeted neurotherapy and cognitive training.
Method:
Amplitude of low frequency fluctuations (ALFF), regional homogeneity (ReHo), and seed-based FC were analyzed in 53 ADHD and 52 healthy controls. The “brain-cognition-behavior” relationship was further explored using mediation analysis.
Results:
ADHD showed abnormal local activation in the middle temporal gyrus (MTG), inferior occipital gyrus and inferior frontal gyrus (IFG) and reduced FC between the IFG and the cerebellum. ADHD diagnosis may affect ALFF of MTG and further modulate shift and finally affect inattentive symptoms. It may also affect the total symptoms through the FC of the IFG with the cerebellum.
Conclusion:
ADHD showed extensive spontaneous activity abnormalities and frontal-cerebellar FC impairments. Localized functional abnormalities in the MTG may affect the shift in EF, resulting in attention deficit behavior.
Introduction
ADHD is a childhood-onset neurodevelopmental disorder with a prevalence of 5% (Sayal et al., 2018). Patients not only exhibit age-inappropriate attention deficits and hyperactive/impulsive behavior, but also accompanying executive function impairment. As a pressing public health issue, its neural mechanism is still not well understood. Therefore, it is important to explore the abnormal brain functional features in subjects with ADHD and the correlation with their cognitive and behavioral expression to establish the potential “brain-cognition-behavior” relationship.
Children with ADHD often show delayed brain development, characterized by abnormal local brain functional activation and functional connectivity (FC). Previous studies have found that ADHD exhibits local activation abnormalities in multiple regions, including the basal ganglia, sensorimotor cortex, and cerebellum, as indicated by alterations in the amplitude of low-frequency fluctuations (ALFF) and regional homogeneity (ReHo) (X. Wang et al., 2013; Zang et al., 2007). Moreover, medication treatment has been shown to normalize the ReHo in the frontal-parietal and cerebellar regions (An, Cao, Cao, et al., 2013). These findings collectively indicate the effectiveness of ALFF and ReHo in reflecting the local brain function of ADHD. However, ALFF and ReHo are complementary (An, Cao, Sui, et al., 2013), and most previous studies have analyzed a single local functional brain feature. This study aims to provide a more comprehensive analysis of local brain functional activation in patients by combining these two features.
Dysfunction of the prefrontal-striatal-cerebellar circuit is core functional connectivity (FC) abnormality in ADHD, often involving multiple brain networks such as the default mode network, frontoparietal network, and ventral attention network (Sripada et al., 2014). However, most FC analyses are calculated based on the connectivity matrix or ICA, ignoring the correlation with local activation, but it is worth noting that local neuronal activity can determine BOLD FC at rest (Abe et al., 2020; Riedl et al., 2014). Seed-based FC analysis allows a more targeted exploration of dysfunctional integration using abnormal local activation, but only one previous study examined FC abnormalities using ALFF (Li et al., 2014). The present study was conducted to comprehensively and systematically investigate the abnormalities of brain function in ADHD through local activation measures such as ALFF and ReHo, along with the corresponding FC.
Cognitive function is an important intermediate phenotype that links the brain to behavior. (Tripp & Wickens, 2009). As core cognitive functions in ADHD, executive functions (EF) broadly include cold EF, which involves inhibition, working memory, and cognitive flexibility, as well as hot EF, which is related to reward and emotion (Grafman & Litvan, 1999). Previous research has identified potential neural mechanisms underlying EF impairments. A meta-analysis of task-state MRI involving EF showed that ADHD patients exhibit reduced activation of the frontoparietal network (Cortese et al., 2012). Jin et al. (2019) found that genetic polymorphisms in ADHD patients may affect inhibition function through ALFF in the right superior frontal gyrus. These studies reflect the close relationship between abnormal brain function and EF impairments, but they have not yet integrated the exploration of the relationships between the brain, cognition, and behavior.
The Behavior Rating Inventory of Executive Function (BRIEF) was used to assess impairment of EF in daily life, which is more closely related to behavioral abnormalities and more suitable for constructing pathological models. In addition, the BRIEF also contains the emotional control-related hot EF, which can more comprehensively assess the EF of patients. Zhao et al. found alterations in the insular subregion FC in adults with ADHD and significant correlations with working memory in HC (Zhao et al., 2017). Preschool ecological EF predicts school-age ADHD symptoms, and EF deficits are significantly associated with FC (Hawkey et al., 2018). In conclusion, the close correlation between BRIEF-based ecological EF, clinical symptoms, and brain function suggests the presence of potential regulatory relationships among these three factors.
In summary, this study firstly explored brain regions with abnormal local activation by ALFF and ReHo, and further conducted FC analyses using the observed regions with altered brain spontaneous activation as seeds. Secondly, the correlation between imaging features and ecological EF and behavior were analyzed. Finally, we attempted to construct a “brain-cognition-behavior” mediating relationship to explore the neuropathological mechanisms underlying clinical symptoms.
Methods
Participants
Children with ADHD were recruited from the outpatient department of Peking University Sixth Hospital from 2018 to 2021. Inclusion criteria: (1) Diagnosed by a psychiatrist in line with the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV) ADHD diagnostic criteria; (2) aged 6 to 17 years; (3) Right-handed; (4) Full-scaled intelligence quotient (IQ) assessed using the Wechsler Children’s Intelligence Scale Chinese Revised Version ≥80. Healthy controls were recruited from local primary and secondary schools during the same period. Inclusion criteria: (1) do not meet the previous and current diagnoses of ADHD according to the interview using K-SADS-PL; (2) aged 6 to 17 years; (3) Right-handed; (4) Full-scaled IQ ≥ 80.
The exclusion criteria for all participants were: (1) History of neurological disease or traumatic brain injury in the past; (2) Current history of psychotropic drug use; (3) The semi-determined diagnostic tool K-SADS-PL is used to exclude childhood behavioral disorders such as autism and Tourette’s syndrome, as well as common mental and psychological disorders such as affective disorders, anxiety disorders, and psychotic disorders; (4) Physical diseases or contraindications to MRI scans.
In order to determine the required sample size for our study, we conducted a power analysis based on previous research (Plichta & Scheres, 2014; J. B. Wang et al., 2017), where the effect size was set at 0.59. Using GPower software and a significance level of 0.05, we calculated that a sample size of 47 participants in each group would provide a minimum power of 0.80 to detect the expected effect. This study was approved by the Ethics Committee of Peking University Sixth Hospital. The children and their parents were fully informed of the purpose and process of the study, and their parents’ written informed consent was obtained.
Executive Functional and Behavioral Testing
Behavioral Rating Inventory of Executive Functioning (BRIEF)
The BRIEF is a behavioral rating scale of executive functioning developed by Gioia that contains 86 rated items, each rated from 1 (never) to 3 (often), in which the higher the rating, the more impaired the executive functioning. The scale is divided into two domains: the Behavioral Regulation Index and the Metacognitive Index, which contain a total of eight factors. Our present study focused on the most central impairment of cold and hot executive functions in ADHD, and then the scores of “inhibit,” “shift,” “working memory,” and “emotional control” factors were used for analyses. The BRIEF has been shown to have high concurrent and discriminant validity and adequate reliability in Chinese children (Qian & Wang, 2007).
Attention Deficit Hyperactivity Disorder Rating Scale-IV Home Version (ADHD-RS)
The scale is based on DSM-IV diagnostic criteria for ADHD and is widely used in the behavioral assessment of attention deficit and hyperactivity in patients with ADHD. The scale consists of 18 items. The first 9 items are symptoms related to attention deficit and the scores were summed to obtain the Inattention score (IA). The last nine items are symptoms related to hyperactivity and impulsivity, and the scores were aggregated to obtain the Hyperactivity-Impulsivity score (HI). The scores of IA and HI were summed to obtain the total score.
MRI Data Acquisition and Preprocessing
Scan Parameters
Imaging data were acquired at the Neuroimaging Center of Peking University Sixth Hospital, on a GE Discovery MR750 3T scanner (GE Medical Systems, USA) with an 8-channel head coil receiver. Before the examination, all subjects’ heads were fixed with sponge pads, and special anti-noise earplugs for MRI were worn. The subjects were instructed to lie on their backs, close their eyes, and breathe calmly. For anatomical reference, we acquired high-resolution structural images of the whole brain using the Fast Spoiled Gradient-Echo (FSPGR) sequence (192-slice sagittal scan, slice thickness = 1 mm, slice spacing = 1 mm, repetition time = 6.7 ms, echo Time = 2.9 ms, Inversion Time = 0.45 s, Inversion Angle = 12°, Imaging Matrix = 256 × 256, Intraslice Scan Field of View (FOV) =256 × 256 mm2, voxel resolution = 1 × 1 × 1 mm3). Echo Planar Imaging (EPI) sequence was used to collect resting-state functional images, parameters: 43-slice axial scan (sequence is odd-numbered slices first, then even-numbered slices), slice thickness = 3.2 mm, slice spacing = 3.2 mm, Repetition Time (TR) = 2000 ms, Echo Time (TE) = 30 ms, flip angle = 90°, imaging matrix = 64 × 64, Field of View (FOV) = 220 × 220 mm2. The entire rsfMRI scan lasted for 8 min which generated 240 volumes.
Preprocessing
The original data were preprocessed by Resting-State fMRI Data Analysis Toolkit (RESTplus) software (Jia et al., 2020), including (1) removal of the first 10 volumes; (2) slice timing; (3) head motion correction (excluding data with head movement >3 mm or rotation > 3°); (4) spatial normalization (applying EPI template, resampling to 3 mm × 3 mm×3 mm); (5) smoothing, 6 mm; (6) de-linear drift; (7) nuisance covariates regression of head motion parameters (using Friston 24 parameters ), white matter and cerebrospinal fluid signals; (8) temporal filtering (bandwidth 0.01–0.08 Hz to remove low-frequency drift and high-frequency noise). ALFF calculation was performed before filtering. In addition, smoothing is excluded from the preprocessing process when calculating ReHo. Five ADHD patients and two healthy controls were excluded due to head movement, and a total of 52 ADHD patients and 51 healthy controls were included for further analysis.
Parameter Calculation
ALFF
After preprocessing, the power spectrum is obtained by fast Fourier transform on the time series of each voxel. And the power spectrum of the voxel with the frequency of 0.01 to 0.08 Hz is squared, and the ALFF value of each voxel is obtained. Finally, the ALFF value of each voxel was divided by the whole-brain average to obtain the normalized ALFF value.
ReHo
The Kendall Concordance Coefficient (KCC) was used to calculate the local consistency of each voxel with neighboring voxel time series, and the KCC value for each voxel was calculated and divided by the whole-brain mean to obtain normalized results. The calculated values were smoothed with a Gaussian parameter of 6 mm × 6 mm × 6 mm full width and half height.
Function Connectivity
As described below, four brain regions with significant abnormality calculated by ALFF and ReHo (Table 2, Figure 1) (right middle temporal gyrus, left lingual gyrus, right inferior occipital gyrus, left inferior frontal gyrus) served as seed points for FC analysis in ADHD patients. After smoothing and filtering, the reference time series of each seed point is obtained by averaging the time series of voxels in its region. Correlation analysis was performed with the time series of each other voxel. The correlation coefficients between seed points and other voxels are then transformed using Fisher r-to-z transforms, resulting in a variant that approximates a normal distribution.
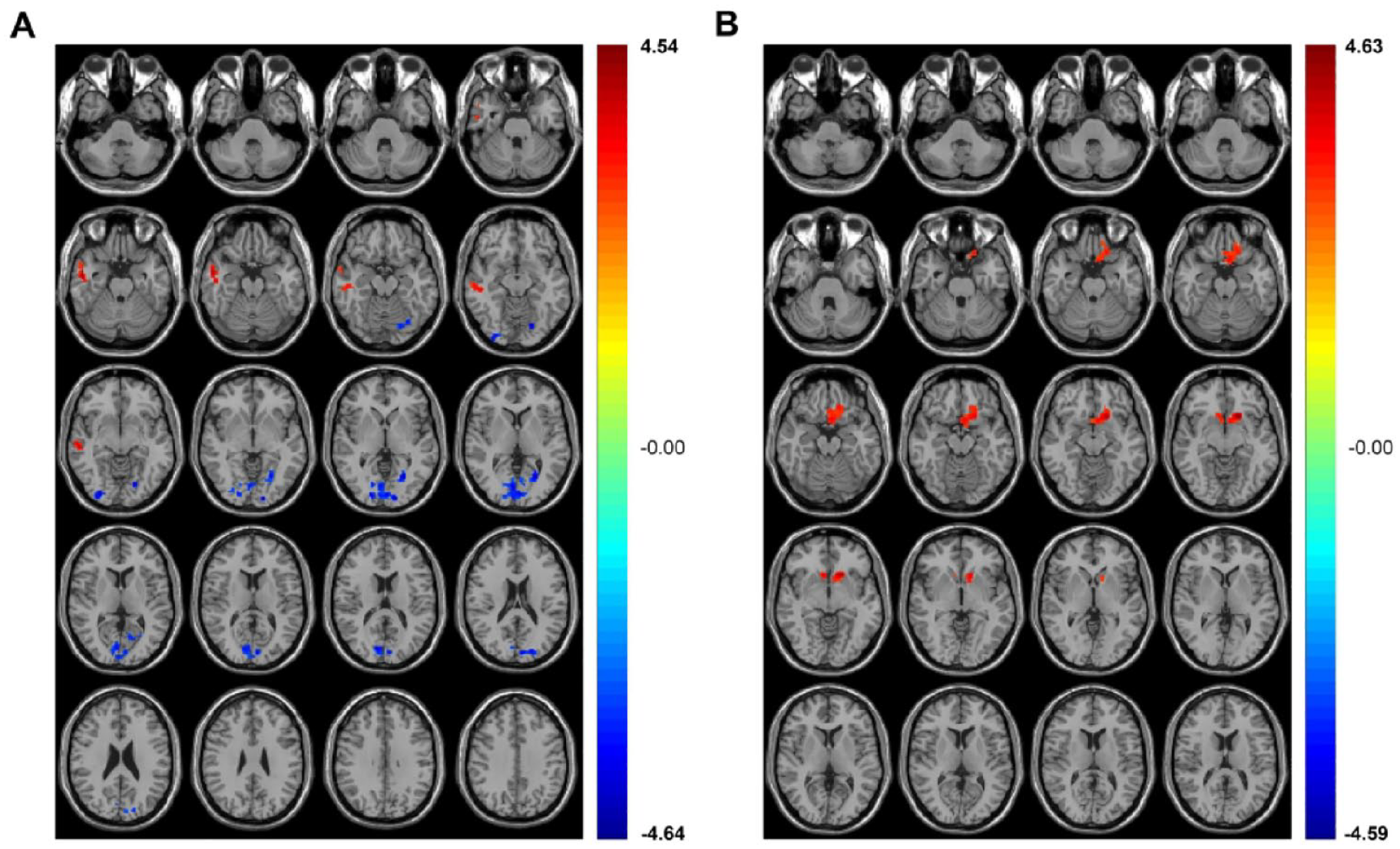
Differential brain regions between ALFF and ReHo. (A) Differential brain regions of ALFF. The ALFF in the right middle temporal gyrus of ADHD children was significantly increased, and the left lingual gyrus and the right inferior occipital gyrus were significantly decreased. (B) The ReHo in the left inferior frontal gyrus of ADHD children was significantly increased.
Statistical Analysis
Clinical Data Measurement
Statistical analysis was performed using SPSS, using the Kolmogorov–Smirnov test for normality of demographic and clinical variables. For normally distributed variables, two-tailed independent samples t-test were used. Non-normally distributed data were assessed using the Mann-Whitney U test. Significance level was set at p < .05.
Brain Function Data Analysis
Two-sample t-test was used to compare ALFF, ReHo, and seed-based functional connectivity information between ADHD patients and controls, respectively. When comparing groups, age and gender were included as covariates to eliminate potential effects on the results. Results were corrected for multiple comparisons by GRF, with p < .005 at the voxel level and p < .05 at the clump level. The most significant peak voxel coordinates within the differential brain regions were described using the Montreal Neurological Institute standard coordinates.
Correlation Analysis
Two-tailed Pearson correlation analyses were performed separately for ADHD and HC using SPSS software. After regression for age and sex, correlations between EF and symptom scores and brain imaging characteristics were assessed. Based on previous studies we selected the most central cold executive functions in BRIEF: inhibit, shift, and working memory; and the hot executive function: emotional control, for correlation analysis.
Mediation Analysis
Use the PROCESS plug-in (http://www.afhayescom/public/process) in Spss to conduct mediation analysis to explore the direct correlation between brain function data, EF, and clinical performance data. Bootstrapping was used to assess confidence intervals for sample distributions and indirect effects of mediation. The data were sampled5,000 times, and the 95% CI of indirect effect was obtained. If the 95% CI is not 0, the mediating effect is significant, p < .05. Age and gender were used as covariates to exclude the effect on the results.
Results
A total of 111 subjects were recruited. Four ADHD and two HC were excluded due to excessive head motion during MRI acquisition. Finally, 53 children with ADHD and 52 healthy controls were included in the study. Among the ADHD group, 33 cases were inattentive type, 5 cases were hyperactive-impulsive type, and 15 cases were combined type. Three patients had comorbid oppositional defiant disorder. The ADHD included in this study were unmedicated first-time patients. The mean duration of ADHD was 4.17 ± 1.79 years. The demographic information of the participants is shown in Table 1. There was no significant difference in age (p = .10) and gender (p = .20) between the two groups. As found in clinical observations, the IQ of ADHD patients was significantly lower than that of healthy controls (p < .001); while the scores of each factor of the BRIEF and ADHD-RS were significantly higher than those of normal controls (p < .001). This suggests that children with ADHD have poorer IQ performance, as well as severe executive function impairment and behavioral problems.
Clinical and Demographic Characteristic of ADHD Patients and HC.

Note. ADHD = attention-deficit/hyperactivity disorder; HC = healthy controls; SD = standard deviation; FIQ = full-scale intelligence quotient.
Regional Brain Function Analysis
Compared to HC, ALFF in ADHD patients increased significantly in the right middle temporal gyrus and decreased significantly in the left lingual gyrus and right inferior occipital gyrus; ReHo increased significantly in the left inferior frontal gyrus (Figure 1, Table 2).
Statistically Different Brain Regions Between ADHD Patients and HC.
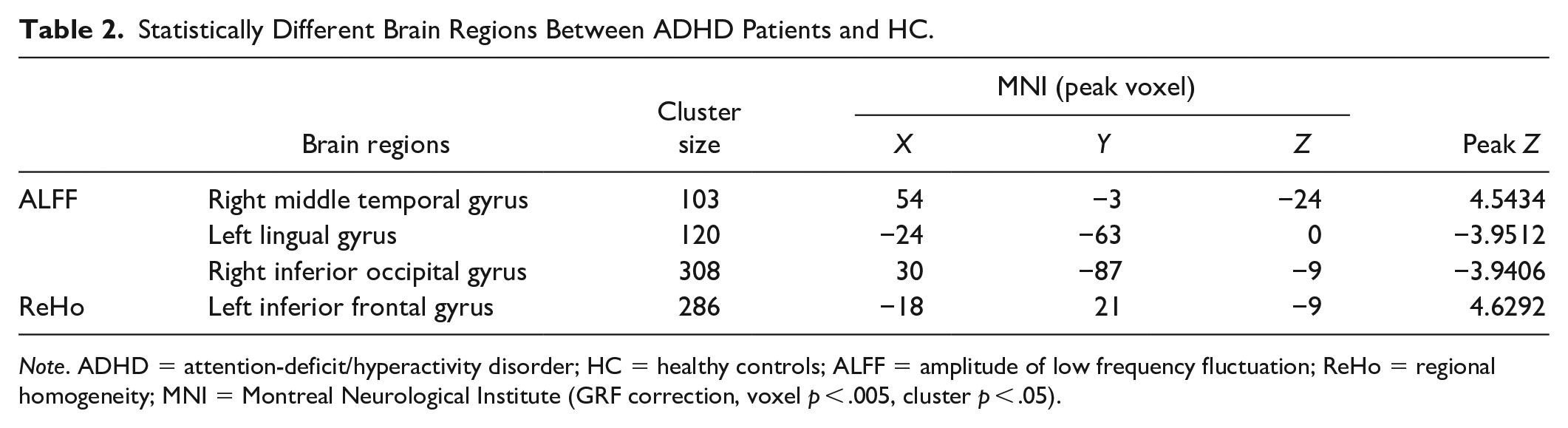
Note. ADHD = attention-deficit/hyperactivity disorder; HC = healthy controls; ALFF = amplitude of low frequency fluctuation; ReHo = regional homogeneity; MNI = Montreal Neurological Institute (GRF correction, voxel p < .005, cluster p < .05).
FC Analysis
The FCs were calculated and analyzed with the above identified brain regions as seeds. Compared with controls, the FCs of the right middle temporal gyrus with the right superior occipital gyrus, the left middle occipital gyrus, the left precuneus and the right cerebellum decreased significantly in children with ADHD. In addition, decreased FC was also observed between the left inferior frontal gyrus and right cerebellum (Table 3).
Significant Difference in FCs Between ADHD Patients and HC.
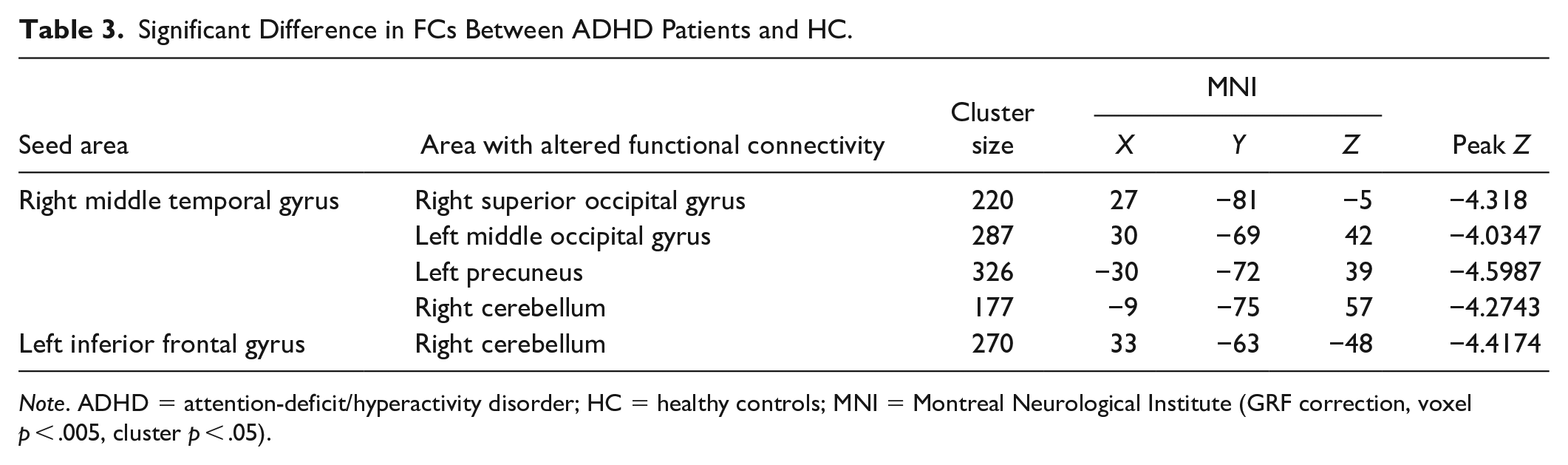
Note. ADHD = attention-deficit/hyperactivity disorder; HC = healthy controls; MNI = Montreal Neurological Institute (GRF correction, voxel p < .005, cluster p < .05).
The Correlation of the Brain Functional Alteration With the Executive Functions and ADHD Core Symptoms
In children with ADHD, the ALFF of right middle temporal gyrus was significantly correlated with shift (r = .344, p = .016) (Figure 2A); while the ALFF of right inferior occipital gyrus (r = −.306, p = .032) was correlated with emotional control (Figure 2B). In contrast, no correlation was found in HC. No correlation was found between the altered FC and EFs, either in ADHD or in HC.
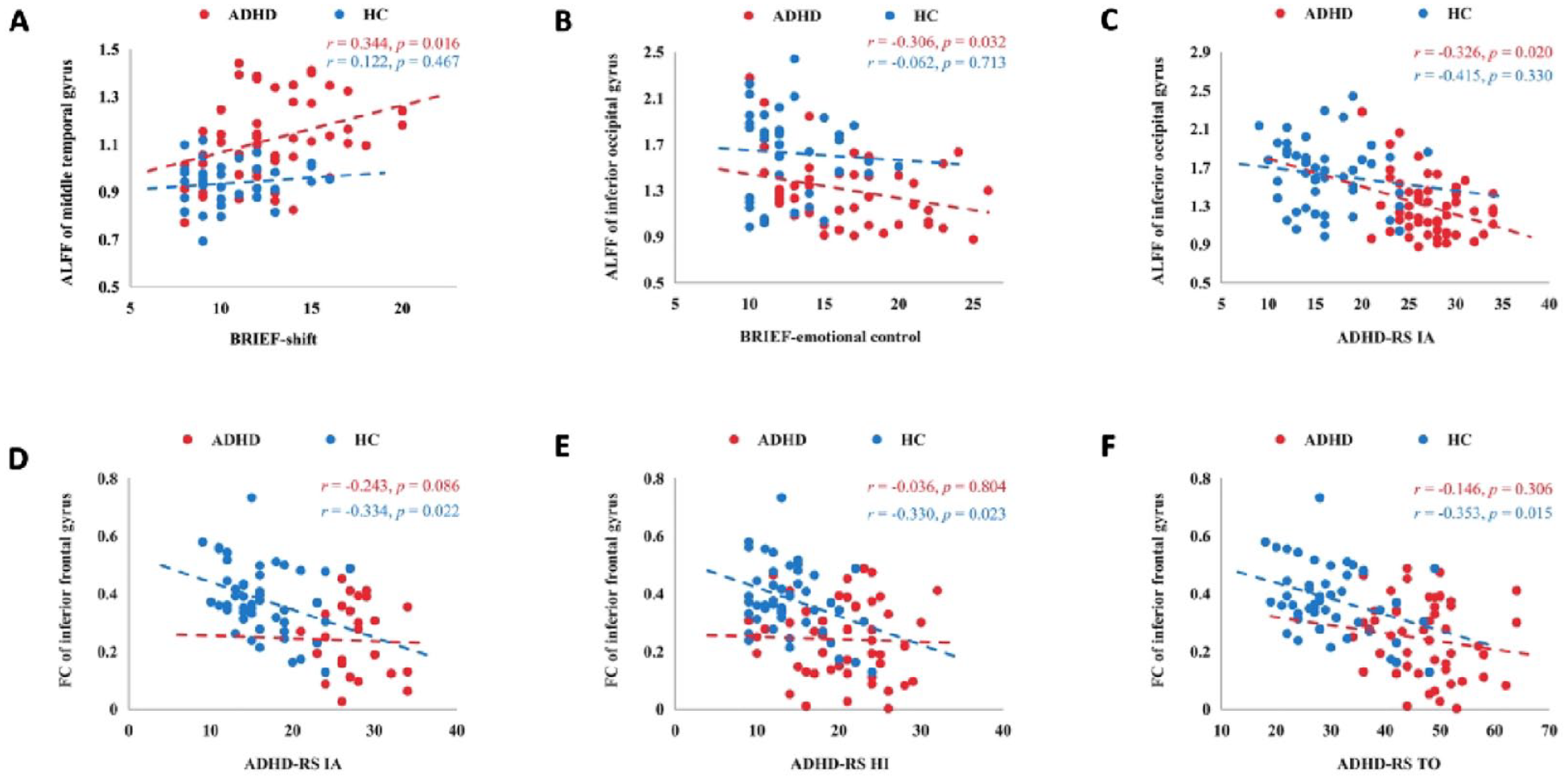
The imaging features were correlated with executive function and symptoms. In ADHD, (A) ALFF of the middle temporal gyrus was significantly correlated with conversion, (B) ALFF of the inferior occipital gyrus was significantly correlated with emotional control, and (C) ALFF of the inferior occipital gyrus was significantly correlated with IA. In contrast, HC was not correlated. In HC, FC of the inferior frontal gyrus to cerebellum was significantly correlated with IA (D), HI (E) and total score (F), and ADHD was not correlated.
For the core symptoms of ADHD, a significant correlation was found between ALFF values in the right inferior occipital gyrus and IA (r = −.326, p = .020) (Figure 2C). It was not significant in HC. However, FC of left inferior frontal gyrus to cerebellum in HC was significantly correlated with IA (r = −.344, p = .022), HI (r = −.330, p = .023) and total score (r = −.353, p = .015) (Figure 2D–F), while no significant correlations were found in ADHD.
Mediation Analyses
Based on the association of brain function with ecological EF and behavioral symptoms, a mediated analysis of diagnosis, brain imaging features, and EF/symptoms was performed. Different groups of subjects influenced the shift through the ALFF of middle temporal gyrus and finally modulating the IA scores. In which local brain function and EF play a partially indirect mediation role in the process of symptom formation [β = −.46 (SE = 0.21), 95% CI [−0.96, −0.11]] (Figure 3).

Mediation analysis. The mediation model indicating a partially indirect effect of ADHD diagnosis on IA via ALFF of middle temporal gyrus and shift.
In a behavior-specific mediation analysis, a significant partial indirect effect of ADHD diagnosis on IA via ALFF of the inferior occipital gyrus [β = −.87 (SE = 0.42), 95% CI [−1.71, −0.04]] was found (Figure 4A). In addition, ADHD diagnosis had a significant partial indirect effect on total score [β = −1.96 (SE = 0.83), 95% CI [−3.63, −0.37]] (Figure 4B) and IA [β = −1.13 (SE = 0.43), 95% CI [−2.01, −0.30]] via FC of the inferior frontal gyrus.

Mediation analysis: (A) the mediation model indicating a partially indirect effect of ADHD diagnosis on IA via ALFF of inferior occipital gyrus and (B) the mediation model indicating a partially indirect effect of ADHD diagnosis on total score via FC of the inferior frontal gyrus.
Discussion
In this study, we investigated the brain local activation and seed-based FC features in ADHD and further analyzed their mediating relationships with ecological EF and symptoms to explore possible underlying “brain-cognition-behavior” relationships. The study found that the ALFF of the right middle temporal gyrus was increased in children with ADHD; the ALFF of the right inferior occipital gyrus was decreased. ReHo in the left inferior frontal gyrus was increased and its FC with the right cerebellum was reduced. Further analysis found that ALFF of the right middle temporal gyrus might affect shift, and finally mediate inattentive symptoms. In addition, ALFF of the inferior occipital gyrus and FC of the inferior frontal gyrus to cerebellum mediated the relationship between ADHD diagnosis and inattention and total score, respectively.
The present study identified abnormal local activation in the inferior frontal gyrus (IFG), which was also found to be a key functionally impaired brain region in ADHD patients in previous studies. Previous studies have found that IFG in ADHD patients exhibits decreased gray matter volume as well as reduced activation in the task state (Depue et al., 2010; Samea et al., 2019). Samea et al. suggested that increased FC of IFG may reflect reduced or delayed functional segregation of prefrontal brain regions (Bos et al., 2017). And the analysis based on brain network graph theory also showed that the efficiency of IFG nodes in ADHD decreased (Chen et al., 2019). More importantly, symptoms in ADHD patients with lower levels of the monoamine oxidase A gene were associated with a BOLD response in the IFG. This further highlights that the neural activity of IFG has some neurotransmitter-related genetic basis. The meta-analysis found that transcranial direct current stimulation targeting the IFG improved inhibitory control and provided further evidence that this brain region may be an important target for neurotherapeutics (Schroeder et al., 2020).
Although the middle temporal gyrus (MTG), lingual gyrus (LG), and inferior occipital gyrus (IOG) are not the most consistent areas of brain function impairment, local activation abnormalities in these brain regions may be related to the heterogeneity of neural mechanisms in ADHD. Previous studies have pointed out that the degree-centrality features of the MTG in ADHD patients show a significant interaction between age and diagnosis, and single photon emission computerized tomography-based local cerebral blood flow in the MTG was also found to be reduced (J. Hong et al., 2017; Lee et al., 2005). A topological study based on brain structure found that nodal betweenness was significantly decreased in the left IOG and correlated with clinical symptom severity of ADHD (Su et al., 2022). What is more important is the finding in studies of drug therapy that reductions in inattentive symptoms were related to increased fALFF in the left LG and left IOG for ADHD children treated with atomoxetine (Shang et al., 2016). Additionally, the ReHo of MTG and LG was changed after the use of methylphenidate in HC (Zhu et al., 2013). This suggests that the local activation of these brain regions may also be modulated by drugs.
This study found reduced FC between the MTG and precuneus, superior occipital gyrus (SOG), and middle occipital gyrus (MOG). the MTG and precuneus are located in the default network (DMN), while the SOG and MOG are located in the dorsal attention network (DAN), which may reflect abnormal functional connectivity between as well as within brain networks. A meta-analysis found that ADHD was characterized by hyperconnectivity between the FPN and regions of the DMN (Gao et al., 2019). Reduced segregation of DMN and DAN has been proposed as a mechanism for cognitive deficits (Owens et al., 2020). This finding may seem contrary to the present study, but previous studies have also indicated that the medial prefrontal cortex, posterior cingulate cortex and precuneus are the core regions of the DMN (Davey et al., 2016; Raichle, 2015). Therefore combining the results of the present study can further complement and refine the findings of previous brain network studies. Patients with ADHD exhibited decreased connectivity between core and non-core regions of the DMN, increased connectivity between core and DAN, and decreased connectivity between non-core and DAN. In addition, decreased FC in the IFG and cerebellum reconfirmed the classic prefrontal-striatal-cerebellar loop injury in ADHD (Biederman & Faraone, 2005; S. B. Hong et al., 2014). Previous studies have also found that cognitive training is effective in improving prefrontal and cerebellar activation, so frontal-cerebellar circuits may be an important neural basis for treatment improvement (Hoekzema et al., 2010).
In correlation studies, local activation of MTG in ADHD patients was found to be significantly correlated with shift, whereas HC was not. Further mediation analysis revealed that the diagnosis of ADHD may modulate shift through ALFF of MTG and ultimately affect IA scores. And a close association between MTG and shift in ADHD patients was also found in previous studies. Dibbets et al. (2010) found that adults with ADHD engaged more strongly the middle temporal gyrus than did the healthy controls during task switching. Also in the DTI study of patients with temporal lobe epilepsy, white matter features were found to be significantly associated with task-switching performance (Kucukboyaci et al., 2012). This suggests that the abnormal brain function in this region in ADHD patients may have caused the impairment of shift and finally exhibited attention deficit behavior.
The discovery of this mediated relation may provide some theoretical basis for neurotherapeutics and cognitive training. Previous reviews have shown that the effectiveness of repetitive transcranial magnetic stimulation and direct current stimulation for ADHD patients is not conclusive and further individualized treatment is needed (Rubia et al., 2021). Based on the results of this study, neurotherapeutics for MTG in patients with attention deficit and shift impairment may be a promising treatment approach. In addition, some studies suggest that cognitive training not only improves clinical symptoms but even improves functional brain activation, however, some studies also suggest that cognitive training is ineffective (Salmi et al., 2020; Shuai et al., 2017). Therefore, targeted cognitive training is particularly important. Based on the mediating relationships in this study, cognitive training targeting the shift for patients with ADHD, who exhibit abnormal local functioning of the MTG and attention deficits, may lead to better improvements in behavioral disorders.
In addition this study also found that ALFF of IOG in ADHD patients was significantly associated with IA. The mediation model indicating a partially indirect effect of ADHD diagnosis on IA via ALFF of IOG. Abnormal local activation in the IOG may be the neural basis of attention deficit behavior, especially with visual attention, which could be closely related (Hietanen et al., 2006). Xiao et al. (2016) performed a topological analysis of HC by DTI and found that the IOG is involved in the orienting component of attention. Because disease heterogeneity in ADHD may involve functional abnormalities in different brain regions, abnormal local activation of IOG may also be an important neural basis for attention deficit behavior.
In this study, we found that FC from IFG to cerebellum in HC is significantly correlated with both IA, HI and total score and also mediated the diagnosis to total score in the mediation analysis. This may further confirm that the prefrontal-cerebellar circuits is the core functional impairment in ADHD patients and its FC may be the neural basis of multidimensional behavioral impairment, which is closely related to the integrated symptom presentation (Durston et al., 2011; Rapin et al., 2017). Bakhshi et al. (2022) found that ADHD group had different choline/creatine and glutamate/creatine ratios in the fronto-cerebellar circuit, compared to HC. These results suggest that alterations in fronto-cerebellar metabolites may be related to cognitive and behavioral deficits in ADHD. More importantly compared to HC, MPH normalized differences during vigilant attention in fronto-cerebellar connectivity (Rubia et al., 2009). Although specific cognitive functions were not found to be involved in the modulation of attentional deficits by local activation of the IOG and the modulation of total symptoms by prefrontal-cerebellar FC in the present study. This may involve other cognitive functions or the superposition of multiple cognitive functions and needs to be explored in further studies.
Limitation
The current study still has some limitations. Firstly, the sample size of this study is not large, and it can be further expanded for analysis. Secondly, due to the potential for different brain dysfunction among subtypes of ADHD, further analysis of brain imaging differences between subtypes can be performed after expanding the sample size. Finally, considering that lower IQ may be a manifestation of cognitive-behavioral impairment in ADHD, IQ matching was not performed between groups. In the future, matching will be performed on subdivided IQ dimensions to observe differences in brain imaging.
Conclusion
Neuropathological mechanisms in ADHD patients may involve local functional abnormalities in several brain regions of the prefrontal, temporal, and occipital lobes, as well as abnormal FC of the DAN with the DMN and the frontal-cerebellar circuits. Abnormal local activation of the MTG and IOG, as well as decreased prefrontal-cerebellar FC may underlie the neural basis of symptoms in ADHD. More importantly, abnormal local activation in the MTG may affect shift, which in turn leads to attention deficit behaviors.
Footnotes
Acknowledgements
We thank all the authors for their contributions in this study and all the children and their parents who participated in the experiment.
Author Contributions
Li Sun, Lu Liu, Yufeng Wang and Yuan Feng developed the study concept. Yuan Feng, Yu Zhu, Xiaojie Guo, Xiangsheng Luo, Chen Dang, Qianrong Liu, Chenyang Xu, Simin Kang, Gaohan Yin and Taizhu Liang performed testing and data collection. Yuan Feng performed the data analysis and interpretation. Yuan Feng drafted the manuscript. Li Sun and Lu Liu provided critical revisions. All authors approved the final version of the manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Sciences Foundation of China (L.S., 81971284; 81771479 ); the Key scientific research projects of capital health development (L.S., 2020-1-4111); the Beijing Municipal Science and Technology Program (L.S., Z171100001017089); the National Natural Science Foundation of China (L.L., 81873802); the Capital’s Funds for Health Improvement and Research (L.L., CFH: 2022-2-4114).