
Abstract
Objective:
ADHD is associated with stigma, but whether stimulant medication use contributes to this is unknown. We examined how perception of a young woman may be influenced by visible ADHD symptoms and/or prescribed stimulant medication use (PSMU).
Method:
Three-hundred-fourteen undergraduates were randomly assigned to watch one of four videos: a woman portraying (a) neither symptoms of ADHD nor PSMU, (b) no ADHD symptoms but disclosing PSMU, (c) ADHD symptoms but no PSMU, or (d) both ADHD symptoms and PSMU. Participants then completed measures of their liking of and desire for affiliation with the woman.
Results:
Analyses suggest that visible symptoms of ADHD were perceived negatively and are associated with less liking and desire for affiliation. PSMU was associated with negligible additive stigma.
Conclusion:
This supports that noticeable ADHD symptoms may be the primary driver of the stigma associated with the disorder, and specifically that directed at young women with ADHD.
Keywords
Attention-Deficit/Hyperactivity Disorder (ADHD) is a relatively common neurodevelopmental disorder that emerges in childhood, with the Centers for Disease Control (CDC, 2022) currently estimating that 9.8% of children in the United States have been diagnosed by a healthcare provider. In general, the Diagnostic and Statistical Manual of Mental Disorders (5th edition text revision, DSM-5-TR; American Psychiatric Association, 2022) outlines that ADHD is characterized by problems with impulse control, hyperactivity, and inattention that impact the individual in multiple areas of life (e.g., school, work, social). The concept of ADHD as an enduring issue for adults is relatively new, with the body of literature about the persistence and effects of adult ADHD only growing in the past few decades (Zalsman & Shilton, 2016). In children, boys are two to three times more likely to be diagnosed than girls, but by adulthood, the incidence is more evenly distributed between the sexes (Zalsman & Shilton, 2016). However, this latter trend has only been established relatively recently, which reflects a historical conception that ADHD is a “boy’s disorder” that led to the underrepresentation of girls and women in related research. A focus on the outcomes and challenges of ADHD in girls and women, including stigma, is thereby particularly important. This is due to the possibility that girls and women with ADHD may draw even more negative social attention, as compared to boys and men affected by the disorder, due to divergence from cultural and societal expectations (Hinshaw, 2018).
Social impairment with ADHD
It is well established that individuals with ADHD often suffer impairment in social settings. This is, for instance, apparent in romantic relationships, with those affected by ADHD divorcing more frequently than those who do not have ADHD (Murphy & Barkley, 1996). People with ADHD may also struggle in other types of relationships and in everyday social interactions (e.g., in school; Zoromski et al., 2015). Regardless of gender, people with ADHD tend to have deficits in interpersonal skills that can lead to negative social outcomes, such as fewer friends and peer rejection (Aduen et al., 2018). Kok et al. (2016) found that girls with ADHD tend to have noted difficulties with peer interaction, social skills, externalizing behaviors, and increased bullying in comparison to their peers. It is therefore unsurprising that many individuals with ADHD report decreased quality of friendships, as well as greater difficulties in dealing with interpersonal conflict and providing others with emotional support (McKee, 2017). The severity of core ADHD symptoms seemed to positively predict such issues.
Ineffectively managing emotions and deficits in emotional knowledge may also contribute to social maladjustment in those with ADHD (Bunford et al., 2018; Zoromski et al., 2015). Notably, Bunford et al. (2018) found that there were three aspects of emotional dysregulation that were especially predictive of social impairment in this population, namely high excitability/impatience, difficulty in controlling behavior when experiencing a strong emotion, and a relatively slow return to emotional baseline (i.e., lack of emotional flexibility), all of which could be interpreted negatively by others (e.g., abrupt, intense anger; Sacchetti & Lefler, 2017). Masuch et al. (2018) suggest that such noticeable symptoms of ADHD can be interpreted by others as immaturity, a lack of interest in others, weakness of character, unpredictability, rudeness, and/or unreliability. Given the frequency and intensity of negative social interactions that can occur for people with ADHD, along with common knowledge that ADHD causes difficulty in school and work, it is perhaps unsurprising that people tend to stigmatize those with ADHD.
Stigma related to mental illness and ADHD
Mental illness, and, by extension, neurodevelopmental disorders like ADHD, have often been conceptualized as a double bind. Psychological symptoms themselves directly cause distress and, often, noticeable functional impairment. In addition, negative social stereotypes of psychological disorders can lead to stigma against affected persons (Brouwers, 2020; Rössler, 2016), which also has negative consequences. Several social processes facilitate such stigmatization, including labeling, negative stereotyping, and linguistic separation (i.e., separating “us” from “them”; Andersen et al., 2022). Although stigma for certain disorders such as depression has seemingly decreased since the 1990s due to differences in generational beliefs, the stigma surrounding psychological disorders is still widely prevalent today (Pescosolido, 2013, 2021).
Unfortunately, as noted above, many individuals across various cultures and societies endorse negative beliefs about those with psychological problems (Rössler, 2016). In addition to affecting a person’s self-regard, such stigma can reduce the number of opportunities a person may have in life. For example, stigma has been shown to impact the likelihood of those with a psychological disorder being hired for a job (Brouwers, 2020). Concerningly, there is a large body of evidence that supports that both public (i.e., visible discrimination) and self-stigma (i.e., internalization of others’ negative beliefs) reduce the likelihood that those with psychological disorders will seek medical or psychosocial treatment (Clement et al., 2015). As such, documenting and better understanding the presence and predictors of stigma for specific psychological disorders is critical to enhancing the quality of life and other outcomes for affected individuals.
Stigma in ADHD
The research on the stigma of psychological disorders has historically focused on other disorders (e.g., schizophrenia, depression), with sparse attention given to stigmatization of adults with ADHD (Masuch et al., 2018). Rather than resting on a foundation of national or international-level data regarding acceptance and/or prejudice toward ADHD, the current understanding of ADHD-specific stigma stems from the results of a relatively small number of experimental investigations (Lebowitz, 2016). For instance, Canu et al. (2008) demonstrated that the mere mention of a person having challenges with ADHD, in a written vignette, led to participants endorsing a lower desire to interact with the person (i.e., increasing social distance). Indeed, the most prevalent form of stigma displayed toward those with ADHD is a high desire for social distance, resulting in reduced social interaction; in essence, ostracism (Lebowitz, 2016). It has also been shown that situations that involve teamwork (e.g., those involved in academic or other work) are ones in which stigma toward those with ADHD appears more consistently, perhaps due to reluctance to rely on another who is perceived so negatively (Canu et al., 2008). The desire for social distance is not the only manifestation of stigma seen with ADHD. Paulson et al. (2005) examined perceptions of ADHD, depression, and social anxiety in relation to “normal” behavior via videos that displayed aspects of each. As expected, ADHD elicited greater rejection than the control (non-symptomatic) video, but in addition, a hostile mood was observed more in reaction to ADHD than to the other psychiatric conditions. In other words, behavior that is consistent with ADHD symptoms can result in greater hostility and rejection from peers than normal behavior, lending to the idea that ADHD symptoms are stigmatized.
Stigma toward people with ADHD is so prevalent that those with the disorder have grown to expect negative treatment by others. It has been documented that 88.5% of adults with ADHD expected to face discrimination in everyday life for having the disorder. For adults with ADHD, then, the perception and subsequent subjective interpretation of stigma seems likely, and itself might be a significant driver of ADHD-related social dysfunction that exists apart from the impairing symptoms of the disorder (Masuch et al., 2018).
Stigma toward use of stimulants and other psychiatric medication
Stimulant medications, such as methylphenidate (e.g., Ritalin), have been on the market since the 1950s (Frank & Glied, 2006), and are a common initial method to treat ADHD that has been shown to be effective in reducing the symptoms of ADHD. For instance, Cortese et al. (2018) conducted a meta-analysis of randomized controlled trials that included data from participants of various ages, documenting that stimulant medication use yields significant treatment effects across age ranges. Despite such utility, stigma for stimulant medication use has been reported to exist. In adults specifically, a meta-review showed that despite the efficacy of stimulant medications these were not well-accepted (De Crescenzo et al., 2016). This echoes the often-mixed parental opinions regarding ADHD medication (Davis et al., 2011). Anecdotally, the authors have encountered parents and other adults who like stimulant medication to “uppers” or other forms of illicit street drugs (e.g., cocaine) and believe it to share their addictive and other negative properties. Beliefs about stimulant medication akin to these (i.e., that their use is dangerous or unwarranted) could further dampen the public’s opinion of people with ADHD who use it.
Somewhat surprisingly, it seems that there is scant published research regarding stigma against ADHD medication use, specifically. However, Bisset et al. (2022) highlight that the existent research suggests that one- to two-thirds of adults in Western countries (i.e., Australia, Germany) hold negative views toward the use of psychostimulants. Interestingly, one study suggested that having more formal education as well as being younger predicted more positive views toward ADHD medication treatment amongst adult participants (Partridge et al., 2014). Overall, however, broader research regarding the use of psychiatric medications emphasizes the likelihood of negative appraisal. For example, antidepressant use is often stigmatized; therefore, so are those that use them (Castaldelli-Maia et al., 2011). The stigma seems to be related to the perception that the user is emotionally weak and unable to handle problems. It also appears to stem from a lack of belief in the therapeutic ability of antidepressants.
What little related research is available points to the influence of misinformation in possible stimulant medication stigma. Scuttio (2015) found that more accurate knowledge regarding stimulant medications is associated with more positive attitudes about their use. As suggested above, there could be many misunderstandings regarding stimulant ADHD medication. Still, perhaps the most noted is the idea that these medications directly or indirectly result in substance abuse later in life, or that patients may become “addicted” to them. Indeed, Scuttio (2015) specifically determined that when one (accurately) does not believe stimulant medications result in substance abuse or addiction, fewer negative responses are endorsed regarding stimulant medication usage.
Finally, it is worth considering that stigma toward a person could manifest from knowledge of their stimulant medication use, alone, due to its implicit association with ADHD. After all, Canu et al. (2008) found that people with ADHD are subject to stigma even when the disorder was only signaled with its diagnostic label. College students rated their peers with ADHD more negatively than those without and even appraised them more negatively than peers with minor chronic medical issues. This points to the idea that simply knowing one has ADHD results in a less favorable view of that person, even when the appraiser does not see the target’s symptoms. In sum, if it is known that someone takes prescribed stimulant medication, it may result in stigmatization.
Current study
The current study evaluated college students’ relative perceptions and acceptance of a young woman who displayed readily visible ADHD symptoms and/or was known to be taking prescribed stimulant medication for ADHD, versus a portrayal with no such indications (i.e., control). The relative social acceptance (and, by extension, stigma) toward the different presentations was measured by two dependent variables: desire for affiliation (DFA) and how much the individual was liked (degree of liking, or DOL). Accordingly, this study expanded the relatively limited literature that specifically examines the social consequences of ADHD in girls and women and seeks to parse apart the potential contributions of stimulant treatment and ADHD symptoms, themselves, to negative social evaluations.
Based on the literature review, it was hypothesized that (a) when the appraised target depicts ADHD behaviors, she would be perceived less positively than when she had no visible symptoms, reflected by lower DFA and DOL scores. It was also expected that (b) when the target indicated prescribed stimulant medication use (PSMU) she would be perceived less positively than when no PSMU was apparent. Further, it was hypothesized that (c) the depiction of ADHD symptoms alone would be perceived more negatively than the mention of medication alone. Finally, it was specifically anticipated that (d) when the target who displayed ADHD behaviors and mentions PSMU she would be perceived more negatively than in any other condition.
Method
Participants
A sample of 314 undergraduates was recruited through the psychology research participant pool at a large public university in the Southeastern United States. Class credit was given for participation. 1 All were aged 18 or older (M [SD] = 19.33 [2.67] years) and did not have a physical disability or impairment that could hinder their ability to complete the procedure. Many were first-year students (42.7%; 23.9% second year, 19.1% third year, 14.2% fourth or higher-year). The participants tended to be female (84.1%), heterosexual (87.9%), and White (84.7%). Further demographic detail can be noted in Table 1.
Means (Standard Deviations): Descriptive Statistics (Overall Sample).
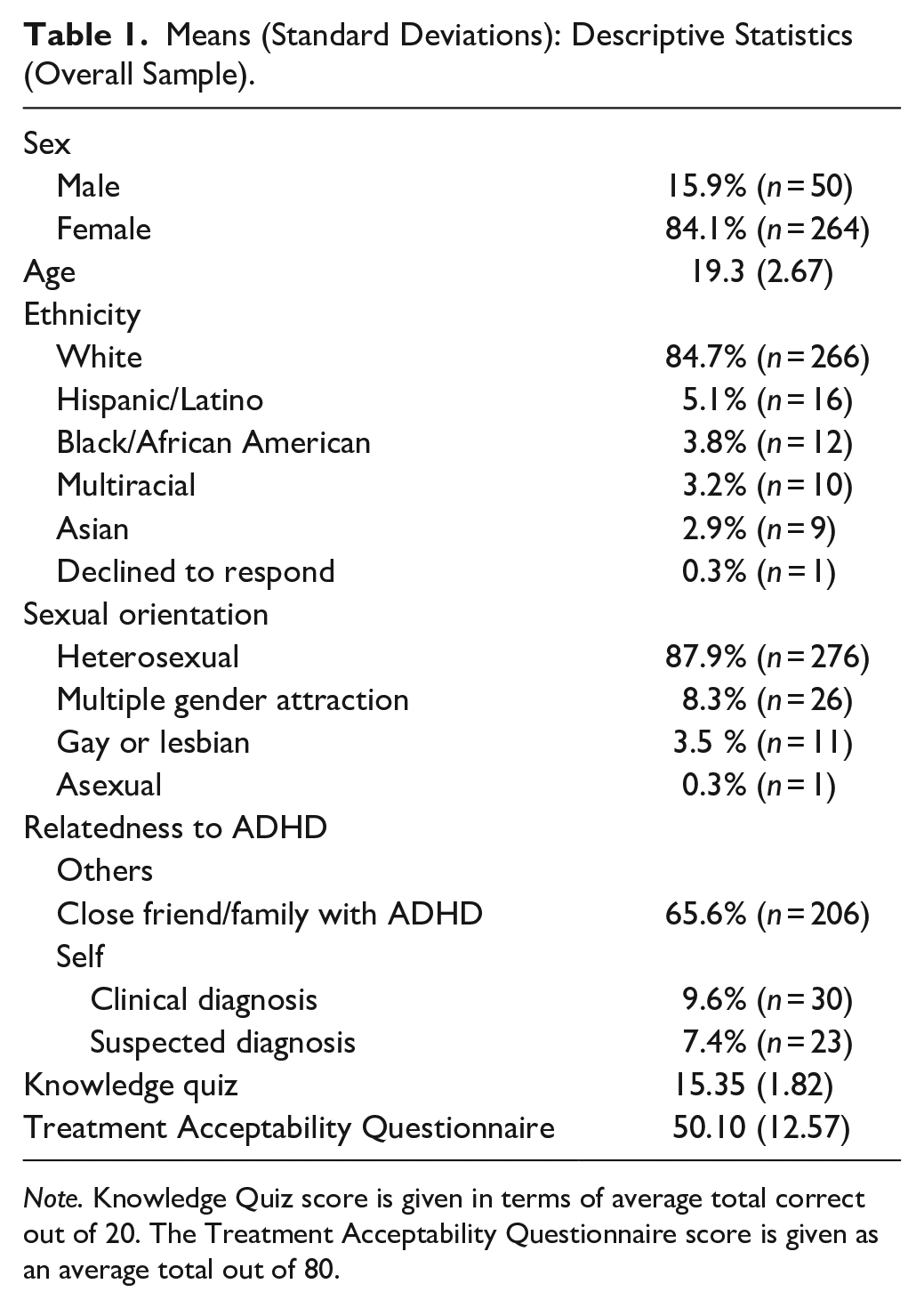
Note. Knowledge Quiz score is given in terms of average total correct out of 20. The Treatment Acceptability Questionnaire score is given as an average total out of 80.
Measures
Video vignettes 2
Participants were randomly assigned to view one of four video vignettes. All videos featured the same actress answering the same nine general personal information questions (e.g., “What do you like to do in your spare time?” and “What are some of your weaknesses?”) The actress was a 21-year-old, White-appearing woman of Hispanic ethnicity. Videos ranged from 4 to 8 minutes long. Longer videos were needed for conditions that displayed ADHD symptoms so that symptoms such as excessive talking and distracted thinking could be adequately portrayed. Participants were asked how much they perceived the actor to be physically attractive, measured on an 11-point Likert scale from 0 (not at all) to 10 (very much).
The video vignettes portrayed the actor as either (a) having normative behavior and not mentioning PSMU (control), (b) normative behavior and mentioning PSMU of Adderall (medication only, or MedO), behavioral symptoms of ADHD but not mentioning PSMU (symptoms only, or SxO), or behavioral symptoms of ADHD and mentioning PSMU of Adderall (SxnMed). Videos were described to participants as impromptu interviews; participants were not told that possible videos varied in the portrayal of ADHD-related behaviors or medication usage.
The videos of those with behavioral symptoms (SxO and SxnMed) depicted enough behavioral ADHD symptoms to meet DSM-5-TR criteria for diagnosis and fitting the Combined presentation. Specifically, five symptoms of inattention and five symptoms of hyperactivity/impulsivity were portrayed. Inattentive symptoms were as follows: difficulty sustaining attention, not seeming to listen when directly addressed, difficulty with organization, frequently losing things, and being easily distracted by extraneous stimuli. Hyperactive/impulsive symptoms were fidgeting and squirming, leaving the seat that the person was expected to remain in, feelings of restlessness, acting as if being driven by a motor, and excessive talking. In addition, the actor in the SxO and SxnMed videos made it known that she experienced her symptoms before the age of 12, the symptoms were present and impairing in multiple contexts, and that the only disorder the symptoms were attributed to was ADHD (see Supplementary Materials for condition scripts).
The scripts of the videos were evaluated by four licensed psychologists who specialize in the assessment and treatment of college students with ADHD, and these experts uniformly deemed these scripts to accurately portray the selected symptoms. Responses to each question during the “interview” were filmed independently and edited together as a series of clips. This was done to ensure that the videos displayed behavior in the same way except when indicated (e.g., SxO and SxnMed responses that involve medication use). The only difference between videos that displayed the same level of ADHD behavior (i.e., [a] control and MedO, [b] SxO and SxnMed) was the inclusion of two mentions of prescribed use of Adderall. Specifically, in the MedO video the actor mentioned that she had taken it, but in the SxnMed video the actor mentioned forgetting to take it that day. Adderall was chosen to signal stimulant medication use because (a) brand names are likely better recognized in the general population and (b) Adderall is one of the most prescribed stimulant medications (41.4 million prescriptions in the United States in 2021; Chuck, 2022) and one that participants would be likely to have heard of. Scripts for each of the video vignettes are included in Supplementary Materials.
Desire for affiliation
DFA was measured with three questionnaire items that were completed immediately after participants viewed their randomly assigned video. The questions measured how likely the participant would be to affiliate with the portrayed individual in three contexts: as an
Degree of liking
Selecting to engage in an ongoing affiliation with someone (i.e., DFA) may be a different type of judgment than simply deciding whether one “likes” another. As such, the variable of DOL was included and measured with the Interpersonal Liking Measure-6 (Veksler & Eden, 2017). One item from the measure, regarding enjoying interactions with the person in the past, was omitted. The five remaining items assessed how much the participant liked the portrayed individual, asking participants to rate their agreement to statements on an 11-point Likert scale from 0 (strongly disagree) to 10 (strongly agree; adapted from the original 9-point scale). The statements included measures of admiration (e.g., There are aspects of this person’s personality that I admire), similarity (e.g., I think that this person and I may have a lot in common), and desire for future interaction (e.g., I would like to get to know this person better and I think that future interactions with this person would be pleasurable). The internal reliability of the scale was good (α = 0.86).
Treatment acceptability questionnaire
The Medication Treatment subscale of the Treatment Acceptability Questionnaire (TAQ; Krain et al., 2005) was used to assess pre-existing stigma against PSMU. The eight items on this subscale were adapted to tap the participant’s opinions on the acceptability of PSMU to treat ADHD. Specifically, items on the original subscale were changed so “a person with ADHD” replaced “my child” for relevance. Participants indicated their agreement to statements on the same 11-point Likert scale as described for the DFA (adapted from the original 6-point scale). Statements included judgments of the effectiveness of medication (e.g., This treatment should be effective in changing someone with ADHD’s behavior), the necessity of the medication (e.g., ADHD-related problems are troublesome enough to justify the use of this treatment), as well as their personal support of its usage (e.g., I would be willing to use this treatment if I had ADHD and I like or support this treatment). The internal reliability of the measure was good (α = 0.88).
ADHD knowledge quiz
The ADHD Knowledge Quiz (KQ; Bramham et al., 2009) was used to assess the level of knowledge that participants had about ADHD, and consisted of 20 true/false general knowledge questions concerning etiology (e.g., ADHD is a disorder present from childhood), behavior and symptoms (e.g., People with ADHD have difficulties concentrating), assessments of value (e.g., ADHD is a problem of motivation), as well as demographic features (e.g., More females than males have ADHD). Because the answer key for this measure was not supplied by its authors (either in publication or by personal request), an answer key was created by the first and second authors, and then reviewed by five licensed psychologists who specialize in the assessment and treatment of ADHD. Despite this step, internal consistency was poor for this measure (α = 0.24). Given that this measure was included for potential statistical control purposes only, and that at the time of data collection no better-validated option to tap ADHD-related knowledge was available, KQ data was retained and used as planned.
Demographics
General demographic information (e.g., gender, age, sexual orientation, ethnicity) was collected on a questionnaire form. In addition, the participant’s prior exposure to ADHD was measured by asking whether (a) the participant, (b) someone in their family, or (c) a friend had been clinically diagnosed with ADHD (or another psychological disorder). They were also asked whether they suspected that they had ADHD (or another psychological disorder) without having a clinical diagnosis. The personal clinical diagnosis and self-suspected diagnosis were combined into one variable for analysis (0 = no, 1 = yes), as were the friends and family questions (0 = no, 1 = yes).
Procedure
The study used a between-groups experimental design. In a private laboratory room, participants first completed a consent procedure, during which they were told that the goal of the study was to measure perceptions of behavior when examined from different points of view. The goal of examining ADHD stigma was not disclosed to avoid biased responses to the video-related measures. Participants then watched one of the four videos (described above), which was selected via random assignment. Participants then completed the measures in a standardized order: DFA, DOL, TAQ, Knowledge Quiz, and demographics. Upon completion, the researcher (undergraduate or graduate student research assistant) debriefed the participant by explaining the aspect of the study examining ADHD-related stigma. This procedure was approved by the host institutional review board.
Results
Preliminary analyses
As a check to ensure that random assignment yielded groups equivalent in background and other personal characteristics, ANOVA and chi-square analyses were conducted to test for demographic differences across groups; as expected, none were detected (see Table 2).
Means (Standard Deviations): Descriptive Statistics Across Video Subgroups.

Note. For videos: 1 = control video condition, 2 = medication mention only video condition, 3 = symptom display only video condition, 4 = symptom display and medication mention condition.
p < .001.
Although these results suggested there could be minimal influence on cross-group differences in DFA and DOL, correlational analyses were conducted between personal variables that have some basis for theoretical relation to these study outcome variables to ascertain whether primary analysis should perhaps take these into account. Pearson correlational analyses were conducted between (a) the Knowledge Quiz total score, (b) Treatment Acceptability Questionnaire (TAQ) total score, and (c) DFA and DOL scores. DFA was significantly correlated with the TAQ score (r = .158, p = .005), as was DOL was likewise associated with TAQ (r = .208, p < .001). Similarly, Spearman correlational analyses were conducted to determine whether (a) gender, (b) sexual orientation, or (c) having close friends or family who are diagnosed with ADHD related meaningfully to DFA and DOL. No statistically significant correlations were detected in any of these analyses. Additionally, as perceived physical attractiveness has long been known to be a general predictor of liking (e.g., Walster et al., 1966), we examined whether this related to DFA and DOL in the sample. Significant Pearson correlation results indicated an association with perceived attractiveness to be present for both DFA (r = .12, p = .04) and DOL (r = .21, p < .001). To better understand any observed group differences in DFA and DOL, primary analyses were conducted with control variables that fit with these preliminary results (see below).
Finally, the primary experimental manipulation of the study, assignment to video condition, involved differences in scripted content that also meant variation in length (i.e., to include mention of medication use, verbal depiction of ADHD symptoms). Scripts varied in length from 680 (control) to 1,317 spoken words (SxnMed). Analysis showed the participants did perceive different lengths across conditions, F (3, 314) = 7.44, p < .001, η2 = .07 (see Table 2). Given that perceived length of video could hypothetically influence liking of and desire for affiliation with the actor, perceived length was utilized as a covariate in subsequent analyses.
Primary analyses
Analyses of desire for affiliation across groups
An analysis of covariance (ANCOVA) was conducted to compare the effect of ADHD behavior and/or medication endorsement by the video target on DFA across video conditions (control, MedO, SxO, SxnMed), controlling for TAQ score, perceived physical attractiveness, and perceived video length. This overall model was found to be statistically significant, F (6, 311) = 23.32, p < .001. TAQ accounted for some variability in DFA, F (1, 311) = 6.04, p = .02, ηp2 = .02, physical attractiveness somewhat more, F (1, 311) = 16.76, p < .001, ηp2 = .05, and video condition much more, F (3, 311) = 34.25, p < .001, ηp2 = .25, Perceived length of video, however, made no significant contribution to the model, F (1, 311) = 2.53, ns. Tukey test comparisons indicated that the mean DFA scores for the control (M = 6.74, SD = 1.54) and MedO (M = 6.73, SD = 1.34) targets differed significantly (p < .001) from the SxO (M = 5.12, SD = 1.59) and SxnMed (M = 4.95, SD = 1.37) targets. No other statistically significant differences on DFA were detected across groups. Calculations of Cohen’s d values showed a large effect for all significant differences (see Tables 3 and 4 for more detail).
Means (Standard Deviations), ANOVA Results, and Post-Hoc Analysis Results for Dependent Variables for Desire for Affiliation and Degree of Liking.
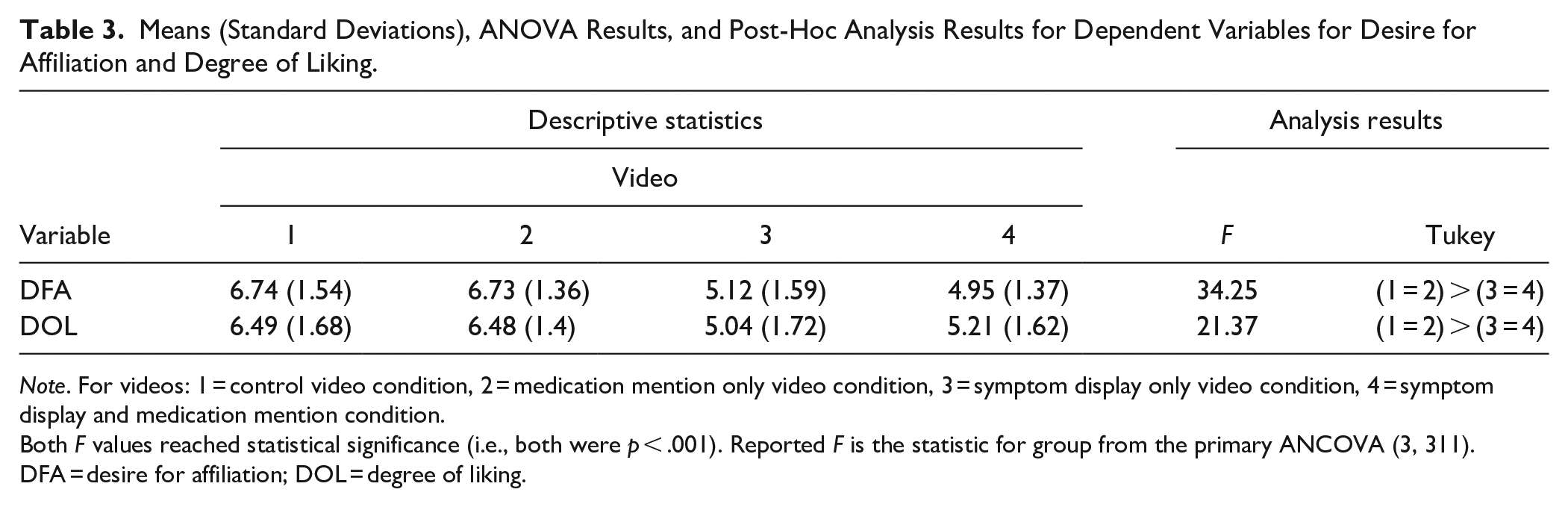
Note. For videos: 1 = control video condition, 2 = medication mention only video condition, 3 = symptom display only video condition, 4 = symptom display and medication mention condition.
Both F values reached statistical significance (i.e., both were p < .001). Reported F is the statistic for group from the primary ANCOVA (3, 311).
DFA = desire for affiliation; DOL = degree of liking.
Measures of Effect Sizes (Cohen’s d) Between Groups for Desire for Affiliation (DFA) and Degree of Liking (DOL).
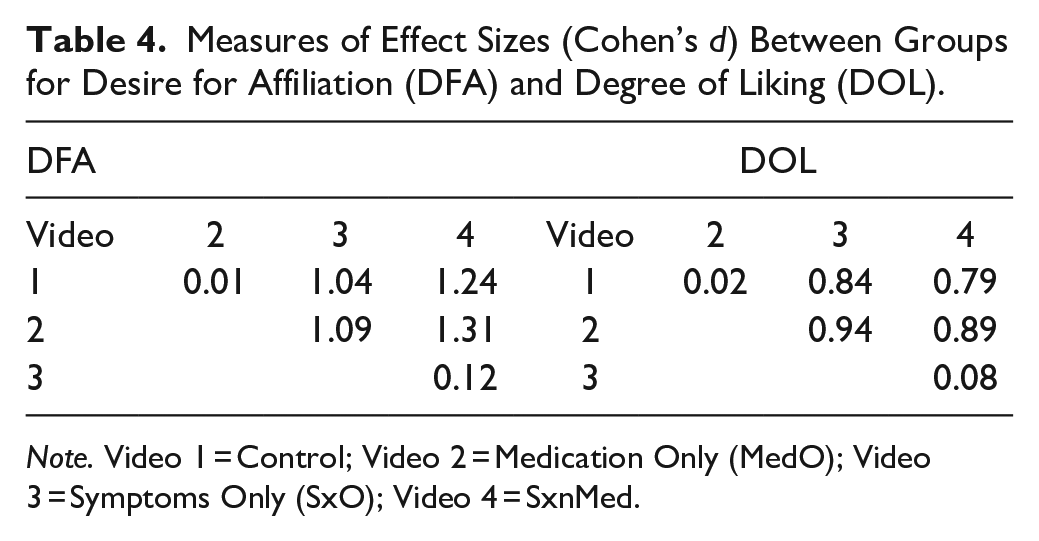
Note. Video 1 = Control; Video 2 = Medication Only (MedO); Video 3 = Symptoms Only (SxO); Video 4 = SxnMed.
Analyses of degree of liking across groups
An ANCOVA was conducted to compare DOL score across the video conditions, controlling for TAQ, perceived physical attractiveness, and perceived length of video. The overall model was statistically significant, F (6, 311) = 17.6, p < .001. TAQ, F (1, 311) = 12.59, p < .001, ηp2 = .04, and perceived attractiveness, F (1, 311) = 29.15, p < .001, ηp2 = .09, accounted for significant variance; however, again, video condition accounted for more, F (3, 311) = 21.37, p < .001, ηp2 = .17. Perceived length of video did not contribute significantly to the predictive model, F (1, 311) = .39, ns. Post-hoc comparisons using Tukey tests indicated that the control target (M = 6.49, SD = 1.68) and the MedO target (M = 6.48, SD = 1.4) were both preferred more than the SxO (M = 5.04, SD = 1.72) and SxnMed targets (M = 5.21, SD = 1.62), as measured by DOL. No other statistically significant differences in DOL were detected across groups. Examinations of Cohen’s d showed a large effect for all significant differences (see Tables 3 and 4).
Discussion
This study aimed to investigate whether negative perceptions of ADHD were influenced by both the use of stimulant medication (i.e., Adderall) and by the observation of core ADHD symptoms themselves. Specifically, it was anticipated that either would result in negative perceptions, that symptoms would be more influential than medication usage, and that the stigma would be strongest when both were present. The data support that visible ADHD symptoms are associated with negative social stigma, both in terms of a desire to affiliate with the observed individual and how much the individual was liked. Further, these results held even when considering the meaningful influences of opinions regarding stimulant medication use for ADHD as well as the perceived attractiveness of the target (i.e., actress “being interviewed”). It was not supported that stimulant medication usage had the same effect. Thus, it is suggested that the symptoms of ADHD are substantially influential when considering negative personal perceptions of affected individuals, whereas stimulant medication use is not. A more detailed discussion of individual hypotheses follows, as well as an analysis of study limitations and suggestions for further research.
ADHD behavior is perceived negatively
As expected, the data evidenced that depictions of ADHD behavior were perceived less positively than depictions of normative behavior. In terms of DFA, the control and MedO conditions were rated higher than both the SxO and SxnMed conditions. The same is true for DOL, as both the control and MedO conditions were rated higher than the SxnMed condition, and the control was rated better than SxO. This evidence aligns with the existing literature regarding perceptions of ADHD. For instance, Canu et al. (2008) noted a reluctance to form social bonds with individuals with ADHD. This closely aligns with the current data, as participants who directly observed ADHD behavior consistently indicated less of a desire to affiliate with the actress than when symptoms were not evident. Visible ADHD behaviors seem to deter others from wanting any type of bond with an affected individual. It could be that the observation of disordered behavior triggers a negative mood in the observer (Paulson et al., 2005). Such an affective response could very well result in liking the observed person less, which fits with the lower DOL scores seen herein.
It is crucial to note that much of the current sample (84.1%) identified as female. This mostly female sample could possibly have judged the actress more harshly due to common gender stereotypes, influencing the lower DOL and DFA scores for the conditions exhibiting ADHD symptoms. Internalized gender stereotypes, or internalized sexism, occurs when women enact learned sexist actions and behaviors upon other women, or even themselves (Bearman et al., 2009). Episodes of internalized sexism and gender stereotypes are common among women (Bearman et al., 2009). Gender stereotypes involve both descriptive and prescriptive components. Descriptive components involve ideas about what people typically do based on their gender (Koenig, 2018). Prescriptive components involve beliefs about what people should do based on their gender (Koenig, 2018). Both descriptive and prescriptive gender stereotypes can lead to discrimination if a perceived incongruency arises (i.e., between gender and behavior; Koenig, 2018). For women, emphasis has traditionally been placed, for example, on traits such as interpersonal sensitivity, kindness, sociability, and modesty (Prentice & Carranza, 2002).
Research has repeatedly shown that women who violate typical gender stereotypes often face social backlash (Costrich et al., 1975). In the conditions exhibiting ADHD symptoms, the actress violated a gender norm; this is so because (a) many people still regard ADHD as a “boy’s disorder,” a misunderstanding that has some basis in the skewed prevalence in childhood (Biederman et al., 2002; Gudjonsson et al., 2014), and (b) even among girls and women with bona fide ADHD the most common presentation is the predominantly inattentive subtype (Biederman et al., 2002; Biederman & Faraone, 2004; Quinn, 2005; Waite, 2007). In this instance, the actress portrays inattention as well as significant hyperactivity-impulsivity, and does so unapologetically, which runs against gender-linked expectations. As such, it is possible that these ADHD portrayals elicit a particularly negative response in the mostly female viewers.
Prescription stimulant medication use is not really perceived negatively
The data did not support that PSMU is perceived less positively than a lack thereof. In both DFA and DOL, there were no significant differences between conditions that varied only by medication status. That is, there were no significant differences in ratings between conditions that did not depict ADHD behavior (control and MedO), nor in those that did (SxO and SxnMed). This result is somewhat surprising since previous literature indicates that those who use psychiatric medications like antidepressants tend to be the targets of stigma (Castaldelli-Maia et al., 2011). However, perhaps PSMU may be less stigmatized among college students. Notably, there is a robust body of research that indicates stimulant medications are frequently (and illicitly) used in college by those that do not have ADHD, usually in attempts to enhance academic performance (Edinoff et al., 2022; Fairman et al., 2020), with approximately 17% of undergraduates endorsing such use (Benson et al., 2015)). Furthermore, this rate of illicit use seems to have increased in the past decades (Edinoff et al., 2022). Such trends may suggest a kind of positive cognitive bias toward stimulant medications because they may be perceived to enhance academic performance, as college students are primarily misusing these medications for academic reasons (Benson et al., 2015; Edinoff et al., 2022; Fairman et al., 2020). At a minimum, the observed willingness of many college students who are not diagnosed with ADHD to seek out and use stimulant medications indicates that there may be greater acceptance of medications like Adderall or Ritalin in this population, compared to the broader community (Judson & Langdon, 2009). As such, further study in non-college populations to test whether stimulant medication use is associated with stigma is warranted.
Another speculative rationale for why PSMU did not result in measurable negative reactions may relate to other common knowledge regarding these medications: That they can work. In other words, while disclosing Adderall use does raise a flag regarding a likely ADHD diagnosis, it is still an indicator that “this woman is doing something about it.” Participants’ opinions may therefore be swayed more toward a neutral opinion on PSMU, as it represents both a con (potential visible symptoms) but also a pro (medically improved behavior).
Displaying ADHD symptoms is perceived more negatively than disclosing PSMU
Given the results related to the first two hypotheses, it is not surprising that the third one was confirmed. For both DFA and DOL, the condition that only mentioned medication (MedO) was rated more positively than the condition that only displayed symptoms (SxO). Considering the work of Masuch et al. (2018), it was expected that symptoms alone would be more impactful to DOL and DFA than the mention of prescription medication use. The core symptoms of ADHD may appear to others as dislikable aspects of personality, such as irresponsibility and rudeness. Therefore, beyond the stigmatization relating to awareness that one has ADHD, a person with readily visible ADHD symptoms may be perceived as having characterological weaknesses. This may precipitate a person’s judgment that the observed woman would make a less desirable employee, roommate, or friend. These areas of affiliation intrinsically require continued interaction over time, and such an observer may want to distance themselves from the young woman because they anticipate awkward, disappointing, or risky interactions given a negative appraisal of traits that she exhibits. Such beliefs and reactions seem possible given existent research that documents public overpathologizing of adult ADHD (Godfrey et al., 2021), psychological diagnoses being associated with greater risk of criminality (Garcia et al., 2020), perceptions of psychological symptoms being publicly shameful (Lloyd & Panagopoulos, 2022), and trends of finding adults with ADHD annoying and also unwillingness to support them in ways such as renting a room or giving an employment recommendation (Speerforck et al., 2019).
Displaying ADHD symptoms and disclosing PSMU may be most negatively perceived
The data provides limited support for this hypothesis. In both DFA and DOL, the control and MedO conditions were rated higher than SxnMed. While the trend (i.e., raw data) was for the SxnMed portrayal to be most negatively rated, statistical analyses indicated that ratings for the SxO condition were not significantly different from the SxnMed condition (Cohen’s d < .13). These results were contrary to expectations. Despite the lack of research regarding ADHD medication stigma, the signal that one is diagnosed with ADHD (due to stimulant prescription) combined with visible ADHD symptoms was expected to worsen perceptions of the afflicted individual. Canu et al. (2008) found that even without the presence of visible symptoms, a label of having ADHD contributed to negative perceptions. Though the observed effects in Canu et al. tended to be moderate, this still points to the idea that simply knowing one has ADHD could result in a less favorable view of that person, even if the appraiser does not directly detect ADHD symptoms. Considering the sum of the results, it may be that the mention of medication or label of having ADHD is not as significant a contributor to negative perceptions or stigma as was anticipated, particularly if ADHD symptoms are already visible and obvious. In other words, a label may possibly have some negative effects for stigma but seeing the symptoms of ADHD may trump any such effect. This result reinforces that visible symptoms are an important determinant of ADHD stigma, with medication mention playing a much less influential role, if any.
Limitations and future directions
There were several limitations of note in this research. A limiting factor was that the Knowledge Quiz used to assess the participant’s level of familiarity with ADHD concepts, was not adequately reliable. This measure was adapted from the published literature, and several studies have previously relied on it. Herein, the assumption that KQ scores are a “true” indicator of knowledge about ADHD must clearly be taken with a grain of salt. While it was not a statistically robust measure, its lack of association with DFA and DOL may not entirely be a fluke. In fact, preliminary analyses found no influence of having a close friend or relative with the disorder on ratings of DOL or DFA, despite that possibly resulting in greater knowledge about ADHD. Still, the question remains open as to whether “true” knowledge about ADHD is related to DOL and DFA toward social targets with ADHD.
Further, the “attractiveness” of the actress was gauged with a question regarding how attracted the participant was to the actress. Different wording, such as asking how attractive the actor is, may have yielded a better index, particularly given that the bulk of the sample ended up being heterosexual women. Attractiveness, however, was important to gauge in this study regarding social perceptions and opinions. People who are judged as more attractive tend to be viewed more positively and are also considered more “normal,” which influences perceived desirability (Lorenzo et al., 2010). This occurs regardless of sexual orientation, perceiving someone to be less “different” influences liking even in the absence of sexual attraction. Even though the wording of the measure was not perfect, it is keeping in line with this prior work that the degree of liking was influenced by perceived attractiveness.
The demographic makeup of the sample is another limitation; as noted, most participants were White, heterosexual, and female. However, considering that women are typically more positive about issues related to mental illness (Holzinger et al., 2011), the fact that reactions reflecting ADHD stigma were noted and were as strong as they were in this study is telling. Future research would benefit from a larger, more balanced sample that could document possible gender and racial/ethnic differences in the perception of ADHD in others, such that replicated findings could be more broadly generalized.
Perhaps relatedly, this study employed videos of a young, White-appearing actress to depict ADHD behaviors, including stimulant use. The same actress was used across video types to ensure that gender or race was not a confounding variable. This study specifically builds on a slim body of prior research that has examined the general social outcomes of girls and women with ADHD and found them to be problematic. Different stigmatic judgments might be made by research participants if the observed individual was a man, or a person who is non-gender conforming or of minoritized ethnicity; as noted above, similar demographic differences amongst the observers (i.e., participants) could also engender different perceptions and opinions, as could the interaction between observer and target characteristics. Future research would do well to explore these possibilities with a broader range of video vignettes and a larger sample.
The current study attempted to depict a wide range of potential ADHD symptoms by presenting the actor as having ADHD of the Combined presentation type. While the results illustrate the presence of stigma relating to general ADHD symptoms, it is worth investigating how different clusters of symptoms may have an impact on perception. Future research in this area could thereby investigate the differences in perception between actors that have the predominantly IA and HI presentations of ADHD, as well as the Combined presentation. Finally, the current study examined whether certain observer (i.e., participant) characteristics might be related to their opinion of someone with apparent ADHD and/or PMSU, such as prior general knowledge of aspects of ADHD. Untested, however, is whether knowledge of certain aspects of ADHD (e.g., efficacy of treatment, degree of impairment) might influence such perceptions, and this is also worthy of empirical examination.
Supplemental Material
sj-docx-1-jad-10.1177_10870547231211358 – Supplemental material for Stigma Related to Observable Symptoms, But Not Stimulant Medication Use, in Young Women With ADHD
Supplemental material, sj-docx-1-jad-10.1177_10870547231211358 for Stigma Related to Observable Symptoms, But Not Stimulant Medication Use, in Young Women With ADHD by Will H. Canu, M. Jamie Cave and Jennifer M. Nelson in Journal of Attention Disorders
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.