
Abstract
Objective:
We examined the relative contribution of parental bipolar disorder (BPD) and psychiatric comorbidities (disruptive behavior disorders [DBD] and anxiety disorders) in predicting psychiatric symptoms and disorders in 2-5-year-old offspring.
Methods:
Participants were 60 families with a parent with BPD and 78 offspring and 70 comparison families in which neither parent had a mood disorder and 91 offspring. Parent and offspring diagnoses and symptoms were assessed using standardized diagnostic interviews and measures, with offspring assessors masked to parental diagnoses.
Results:
Offspring of parents with BPD had significant elevations in behavioral, mood and anxiety disorders and symptoms. Both parental BPD and DBD contributed to elevations in child disruptive behavioral symptoms, whereas child anxiety symptoms were more strongly predicted by comorbid parental anxiety. Parental BPD was a stronger predictor than comorbid DBD of child DBDs.
Conclusion:
Some of the elevated risk for disorders in preschoolers is accounted for by parental comorbidity.
Bipolar Disorder (BPD) in parents confers elevated risk for psychopathology in children, including ADHD, disruptive behavior disorders (DBD), depression, anxiety, BPD, and social and academic dysfunction (Chang et al., 2003; DelBello & Geller, 2001; Henin et al., 2005; Lau et al., 2018; Pavuluri et al., 2005). However, with few exceptions (e.g., Birmaher et al., 2010, 2021), studies of offspring of parents with BPD (BPDO) have focused on children in late childhood and adolescence. The youngest children tend to be overlooked, despite research demonstrating that toddlers and preschoolers may also present with identifiable and impairing psychiatric disorders including anxiety and mood disorders and that early symptoms may be harbingers of future disorder and impairment (Egger, 2009; Mian et al., 2012; Whalen et al., 2017; Wilens et al., 2003). Understanding the early indicators of emotional or behavioral dysregulation among very young children at risk for BPD has critical public health importance because it might help identify developmental precursors to bipolar illness. Better recognition of these symptoms could ultimately facilitate preventative and early intervention efforts among children already at high risk by virtue of having an affected parent.
BPDO are at risk for a broad range of psychiatric disorders. Children and adolescents ages 6 to 18 years old of parents with BPD are known to be at risk for depression, irritability, and labile mood (Birmaher et al., 2009; DelBello & Geller, 2001; Duffy et al., 2007, 2014; Henin et al., 2005; Hirshfeld-Becker, Biederman, Henin, Faraone, Dowd, et al., 2006; Reichart et al., 2004) and to display higher rates (Duffy et al., 2019; Hirshfeld-Becker, Biederman, Henin, Faraone, Cayton, & Rosenbaum, 2006) and earlier onset of anxiety disorders (Duffy et al., 2019; Henin et al., 2005) than offspring of healthy controls. Behavioral symptoms, including hyperactivity and aggression, are also more common among older children and adolescent offspring of parents with versus without BPD (Giles et al., 2007; Maoz et al., 2014), with up to 20% of BPDO diagnosed with ADHD (Lau et al., 2018). A recent meta-analysis of 17 studies of children at risk found that, compared to control offspring, BPDO were nine times more likely to have a bipolar spectrum disorder and two times more likely to have an anxiety disorder (Lau et al., 2018). These offspring also had significantly increased risk for multiple other psychiatric disorders including ADHD, behavioral disorders (i.e., oppositional defiant disorder [ODD], conduct disorder [CD]), and substance use disorders. Importantly, this same meta-analysis found a negative association between risk for mood disorder and age among BPD offspring, indicating that mood symptoms emerged earlier among BPDO.
All of the above studies have been conducted among BPDO age 6 years and older. The very few studies of preschool or early school-aged offspring of parents with versus without BPD show similar patterns. These studies suggest that young children of parents with BPD demonstrate higher disruptive behaviors, hyperactivity, and aggression (Birmaher et al., 2010, 2021; Hirshfeld-Becker, Biederman, Henin, Faraone, Dowd, et al., 2006). Birmaher et al. (2010) found that preschool-age BPDO had an eightfold risk of an ADHD diagnosis and a sixfold risk of having least two psychiatric disorders compared to offspring of parents without BPD, even after controlling for parental psychopathology other than BPD. Another study found that preschool-age BPDO had higher externalizing problems, sleep problems, and aggressive behaviors compared to control children and that these findings held true even after removing children with ADHD and ODD from the sample (Maoz et al., 2014). Hirshfeld-Becker, Biederman, Henin, Faraone, Dowd, et al. (2006) found that young BPDO (mean age of 6.8 years) had significantly higher rates of ADHD and anxiety disorder than offspring of psychiatric and healthy controls. Moreover, laboratory-observed behavioral disinhibition, the temperamental tendency to show talkativeness, exuberance, and approach behaviors with novel situations/people, was significantly more common among preschool-age BPDO compared to offspring of parents without BPD (53%vs. 35%, respectively) (Hirshfeld-Becker, Biederman, Henin, Faraone, Cayton, & Rosenbaum, 2006). More research with young BPDO is needed to confirm findings of elevated symptoms and disorders.
To fully understand the risk for psychopathology conferred by parental BPD, it is important to consider the impact of parental comorbidities. Up to 75% of adults with BPD present with at least one comorbid disorder, including substance abuse, ADHD, and anxiety disorders (Weber et al., 2011). Adults with BPD also report significantly higher childhood histories of ADHD, ODD, CD, and childhood anxiety disorders than those without BPD (Henin et al., 2007). Although many studies of BPDO control for parental comorbidity, the relative contribution of parental BPD versus comorbid psychiatric disorders to young children’s symptoms and disorders remains unclear. For example, parental anxiety disorders are known to elevate risk for anxiety in offspring (Lawrence et al., 2019; Micco et al., 2009), therefore the elevated rates of anxiety reported among BPDO could be accounted for by comorbid anxiety disorders in parents with BPD. In support of this hypothesis, Freed et al. (2015) found that parents with early onset BPD had a significantly greater probability of having an anxiety disorder and that their offspring had higher rates of anxiety disorder than those of parents with later onset BPD.
Similarly, a history of DBDs (ADHD, ODD, or CD) in parents with BPD may confer risk for these disorders in offspring. Young offspring of parents with ADHD are known to have elevated rates of ADHD (Uchida et al., 2021) and a study of parents with unipolar depression found a similar pattern (Hirshfeld-Becker et al., 2008). In this study, both parental depression and parental history of DBDs conferred risk for DBDs in the offspring, with parental DBDs conferring independent risk for ADHD and CD and parental depression conferring independent risk for ODD. These findings underscore the importance of considering comorbid parental DBDs when examining risks for DBDs in offspring, especially younger offspring who might exhibit disruptive behavior symptoms early in development, long before the onset of mood disorders. They also highlight the complex and nuanced interactions among parental BPD and associated disorders and child outcomes.
Therefore, in the current study, we evaluated whether preschool-age BPDO, compared to offspring of parents without personal or family history of mood disorders, had increased likelihood of clinically elevated symptoms and psychiatric disorders, and we examined the relative impacts of parental psychiatric comorbidities. We focused on the youngest children (under age 6), an age group that is understudied despite the recognized importance of identifying risk factors and early symptoms proximally to onset so as to intervene before these symptoms solidify and worsen. We hypothesized that preschool-age BPDO would be more likely to present with elevated behavioral (inattention, hyperactivity, aggression) and emotional (mood, anxiety) symptoms and disorders compared to offspring of non-BPD parents. We also hypothesized that behavioral and emotional dysregulation symptoms and behavioral disorders among BPDO would be predicted by parental BPD rather than comorbid DBD. In contrast, we hypothesized that anxiety symptoms and disorders among BPDO would be predicted by comorbid parental anxiety disorders rather than parental BPD. We did not test parental anxiety disorders as predictors of child DBDs or parental DBDs as predictors of child anxiety disorders because prior research by our group and others has provided evidence that parental anxiety disorders confer risk for child anxiety disorders but not DBDs (Hirshfeld-Becker et al., 2012; Micco et al., 2009; Uher et al., 2023) and that parental DBDs confer risk for child DBDs but not anxiety disorders (Hirshfeld-Becker et al., 2008) with the magnitude of transdiagnostic risk generally smaller than that for diagnostic specific risk (Uher et al., 2023). We evaluated both symptoms and diagnoses for all disorders, given that subthreshold symptoms may be more common than full disorders in this younger age range.
Methods
Procedures and Participants
We recruited two groups of families with at least one child aged 2 to 5 years: families with one or more biological parents with Bipolar I Disorder and a control group in which both biological parents had no lifetime history of mood disorders (depression, BPD I or II, dysthymia) and had no known first-degree relatives with BPD I or II or recurrent major depression resulting in psychopharmacological treatment or hospitalization. Data were collected between 2008 and 2013 and therefore utilized DSM-IV diagnostic criteria.
We used a four-stage ascertainment procedure for recruiting parents with BPD. First, we advertised for patients who had been treated for BPD and who had children in the appropriate age range. Advertisements included letters to clinicians in local outpatient, specialty, and research clinics; handouts given by front desk staff to patients in these clinics; letters to patients in a research registry; and advertisements in a free parenting paper widely available in pediatric practices and libraries. Second, we screened potential participants by telephone with the depression and mania modules of a structured diagnostic interview (SCID-IV) to assess whether they or the child’s other parent had ever met criteria for depression and mania. Third, all parents were administered complete structured psychiatric interviews to determine whether they met diagnostic criteria for BPD. Fourth, all cases of BPD I identified in these interviews were reviewed for “caseness” by licensed psychologists and psychiatrists with expertise in diagnosing adult BPD (DHB, AH, and Dr. Joseph Biederman). To be considered a case, a parent had to have met full criteria for mania (at least one episode), had to have either recurrent (>1 mood episode) or chronic (longer than 6 months) illness, and had to have a severity rating of moderate or severe. Parents were not excluded based upon any comorbid diagnoses or diagnoses in their child’s other biological parent. Comparison parents were recruited from advertisements to hospital personnel (emails to over 11,000 employees) and from print ads and posters systematically placed in publications or venues relevant to parents of young children (e.g., local no-cost parent magazines, pediatricians’ offices). They were screened in the second two stages noted above to rule out BPD or major depression in both parents, in telephone screens and complete diagnostic interviews.
We selected our control group on the basis of not having the disorder used to select cases (i.e., BPD). As individuals with unipolar depression or with first degree relatives with BPD or recurrent major depression may have latent bipolar disorder, we excluded from the control group parents who had had any lifetime mood disorders (history of BPD, MDD, or dysthymia) or whose first degree relatives had had BPD or recurrent major depression. Parents with other mental health disorders were not excluded so as not to create a “super-normal” control group, as doing so would make it impossible to distinguish whether differences between offspring groups are attributable to an increased risk conferred by parental BPD or to a decreased and less-than-typical risk in the control group. Our experience with prior studies suggests that this method is effective; controls in each of these studies have had rates of non-selected disorders consistent with population rates (Biederman et al., 1999, 2004). Note that the present study includes data from all children in each family who were between the ages of 2 and 5 years at baseline. All research procedures were approved by our hospital’s institutional review board, and written informed consent was obtained from parents for their own and their child’s participation.
Measures
Parent Disorders
Parent Axis I disorders were assessed using the Structured Clinical Interview for DSM-IV (SCID-IV; First et al., 1997). We assessed both past and current diagnoses, number of episodes, length of longest episode, and ages at onset and offset. To assess childhood diagnoses in adults, we administered an addendum derived from the K-SADS-E (Orvaschel, 1994), adapted for DSM-IV, including ADHD, conduct disorder, oppositional defiant disorder, and separation anxiety disorder. Our previous work has shown that we can make these retrospective diagnoses in a reliable and valid manner (Biederman et al., 1999, 2004). Parents were also interviewed about mood disorders in their first-degree relatives using the Family Interview for Genetic Studies (FIGS) (Maxwell, 1992). Whenever possible, we interviewed both parents in each family. When both parents were not available, we interviewed the available parent about the second parent (proxy interview).
For purposes of analyses, a child was considered the offspring of a parent with BPD if either parent met criteria for this disorder at any point in their lifetime. In addition, we also classified each child on the basis of risk for two other categories of parental diagnosis: Parental DBD was considered present if either the mother or the father met criteria (at any point in their lifetime) for ODD, CD, or ADHD. Parental anxiety disorder was considered present if either the mother or the father met criteria (at any point in their lifetime) for two or more DSM-IV anxiety disorders (i.e., panic disorder, agoraphobia, social phobia, separation anxiety, generalized anxiety disorder, specific phobia, OCD and post-traumatic stress disorder, not necessarily concurrent). We used this stringent criterion to ensure that the parent had significant anxiety, as we have done in prior studies (Biederman et al., 2004; Hirshfeld-Becker, Biederman, Henin, Faraone, Cayton, & Rosenbaum, 2006).
Child Disorders
To assess the presence of child psychiatric disorders, we administered the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Epidemiological 4th Edition (KSADS-E; Orvaschel, 1994) to mothers of all children. This is a widely used, semi-structured, psychiatric diagnostic interview with established psychometric properties. For ODD and CD modules, we used modifications to questions as developed by Keenan and Wakschlag (2002, 2004). Children were evaluated by assessors who were masked to parent diagnoses (see below for information on training and reliability). We have experience successfully evaluating children ages 2 to 5 years with the KSADS-E administered to mothers (e.g., Biederman et al., 1991, 2001) and this measure both in its epidemiologic (Henin et al., 2005; Wilens et al., 2003) and present-lifetime versions (Birmaher et al., 2009, 2010) has been found to be useful and reliable for establishing psychiatric diagnoses in preschoolers. For purposes of analyses, a DBD was considered present if the child met criteria for ADHD (inattentive type, hyperactive type, or combined), ODD, or CD. An anxiety disorder was present if the child met criteria for generalized anxiety, social anxiety disorder (meeting criteria for either DSM-IV social phobia or DSM-IIR avoidant disorder), or separation anxiety. A mood disorder was considered present if the child met criteria for MDD or BPD.
Diagnostic interviews about both parents and children were completed by raters with undergraduate degrees in psychology who were trained to high levels of reliability and supervised by a committee of board-certified psychiatrists and licensed psychologists who reviewed all diagnoses and resolved diagnostic uncertainties. All interviewers and diagnostic reviewers were masked to ascertainment status, and parent and child interviews for each family were completed by different raters. Kappa values for agreement between diagnostic reviewers (based on 20 interview modules for each diagnosis) ranged from 0.73 (for OCD) to 1.0 (for MDD), with a median of 0.87. Training of interviewers was overseen by AH.
Child Psychiatric Symptoms
Child externalizing and internalizing symptoms were assessed using the parent-report Child Behavior Checklist for ages 1½ − 5 (CBCL 1½ − 5; Achenbach & Rescorla, 2000). Along with general scores for internalizing and externalizing symptoms, the CBCL provides DSM-oriented scales (Anxiety Problems, Autism Spectrum Problems, Attention Deficit/Hyperactivity Problems, Oppositional Defiant Problems) (Achenbach et al., 2003) as well as seven subscales (Emotionally Reactive, Anxious/Depressed, Somatic Complaints, Withdrawn, Sleep Problems, Attention Problems and Aggressive Behavior). For the subscales, T-scores ≥ 70 are considered clinically elevated and T-scores between 65 and 69 are in the subclinical range. For the internalizing and externalizing scales, T-scores ≥ 64 are considered clinically elevated and T-scores between 60 and 63 are considered subclinical. We combined scores from the Attention Problems, Aggression, and Anxious/Depressed scales and calculated the CBCL- Bipolar Disorder (CBCL-BD) scale for each child, which consists of the sum of the T-scores on the Attention Problems, Aggressive Behavior, and Anxious/Depressed. Elevations on these subscales (Mick et al., 2003) and this profile (DiSalvo et al., 2023) has been found in meta-analytic studies in older children to be associated with concurrent pediatric bipolar disorder and to be predictive of future onset pediatric bipolar disorder (Biederman et al., 2009). Where applicable, we also collected the Caregiver/Teacher Report Form (CRF) (Achenbach & Rescorla, 2000) from preschool or daycare teachers. This report covers all symptom scales except Sleep Problems.
Child Emotion Dysregulation
Children’s emotion dysregulation and lability were assessed using the Emotion Regulation Checklist (ERC; Shields & Cicchetti, 1997), a 24-item parent-report questionnaire. Items cluster into two subscales for Emotional Lability/Negativity and Emotion Regulation. The Emotional Lability/Negativity subscale is derived of 15 items with scores between 15 and 60, with higher scores indicating greater emotion dysregulation or emotional lability. The Emotion Regulation subscale is derived of 8 items with scores ranging from 8 to 32, with higher scores indicating greater emotion regulation. The ERC has demonstrated strong psychometric properties, including high validity and reliability (Shields & Cicchetti, 1997). In the current study, internal consistency for the Emotion Lability/Negativity subscale was fair with Cronbach’s alpha of .75. However, the internal consistency for Emotional Regulation subscale was poor with Cronbach’s alpha of .49.
Data Analysis
Independent-samples chi square and t-tests were conducted to examine differences between BPD and comparison groups on parent and offspring demographic characteristics. Where demographic variables were associated significantly with both predictor and outcome variables, we co-varied them in all subsequent analyses. Mixed effects models were utilized to determine the association between parental BPD and child symptoms (CBCL) as well as child emotion regulation and lability (ERC). Multiple members of one family (i.e., groups of siblings) cannot be considered independent because they share genetic and environmental factors. Therefore, family level random effects were used to account for correlations within the family. T-scores from the CBCL and raw scores from the ERC were utilized in the analyses. To test whether CBCL and ERC measures were more strongly predicted by parental BPD or comorbid disorders, we conducted mixed effect models covarying parental comorbidities. Specifically, (1) parental BPD status and parental DBD status were entered simultaneously as predictors for CBCL Oppositional Defiant Problems, Attention Deficit Hyperactivity Problems, Aggressive Behavior and Externalizing Problems, and ERC Lability, and (2) parental BPD status and parental anxiety disorder status were entered simultaneously as predictors for CBCL Anxious/Depressed, Anxiety Problems, and Internalizing Problems and ERC Lability. We examined parental DBD and parental anxiety in separate analyses because we had strong pre-existing hypotheses regarding the risk conferred by each.
To test the associations between parental BPD and child diagnoses, we conducted logistic regressions. For these analyses, we used clustered standard errors (Rogers, 1993) to account for non-independence of siblings. This method calculates Huber-White standard errors that are robust to within cluster (i.e., family) correlation (White, 1980). We also used logistic regression with clustered standard errors to test the associations between comorbid parental disorders and child disorders: (1) we entered parental BPD and DBD as predictors of any child DBD, and (2) we entered parental > 1 anxiety disorders as predictors of any child anxiety. For strata in which no subjects reported a positive response, violating assumptions of logistic regression, we ran Fisher’s Exact analyses and could not derive odds ratios. All tests were two-tailed with alpha set at 0.05.
Results
Sample Size and Characteristics
The sample included a total of 169 offspring from 130 families: 60 families where one or both parents had BPD (and their 78 offspring) and 70 families where neither parent had a mood disorder or a first-degree relative with a major mood disorder (and their 91 offspring). In the BPDO group, 15 families had two offspring and one family had three offspring included in the analyses. In the comparison group 17 families had two offspring and two families had three offspring included in the analyses. We were able to collect CBCLs for parents of 162 offspring (72 BPDO and 90 comparison). Teacher forms (CRF) were available for 83 offspring.
Among the BPDO, 38 (62%) had an affected mother, 19 (27%) had an affected father and 3 (12%) had both parents affected. Based on case review by senior clinicians as described above, we were confident that we recruited families of parents with BPD I. The average number of manic symptoms endorsed in the most severe episode was 6.05 (SD 1.08) (from a total of seven possible symptoms). Fourteen participants (22%) characterized their BPD symptoms as moderately impairing, while 46 (73%) characterized symptoms as severely impairing. Twenty-five (40%) had been previously hospitalized due to BPD symptoms, and an additional 23 (37%) had been treated as outpatients with both therapy and medication. Three (5%) had received psychotherapy only, 1 (1%) received medication only, and 11 (17%) never had treatment. Among parents with BPD, 48.1% had comorbid anxiety disorders (two or more) and 59% had comorbid DBDs.
In analyses examining contributions of parental comorbid disorders to children’s outcomes, 89% of parents with DBDs also had BPD, and 84% of parents with anxiety disorders also had BPD. Thus these parental disorders were largely accounted for by comorbid disorders in the parents with BPD themselves (rather than in their spouses).
Children were between the ages of 2 and 5 years (M = 3.56, SD = 1.08). Descriptive demographic data for the BPD and comparison groups are presented in Table 1. Groups did not differ on offspring age, gender, race, or ethnicity, or parent age, ethnicity, race, or psychiatric diagnoses. However, significantly more BPDO came from families where parents were not living together (encompassing separated, divorced, or never living together; χ² = 7.49, p < .01). Therefore, because it was also associated with child symptoms and disorders, we covaried family status in all analyses.
Demographic Characteristics of BPD and Comparison Parents and Offspring.
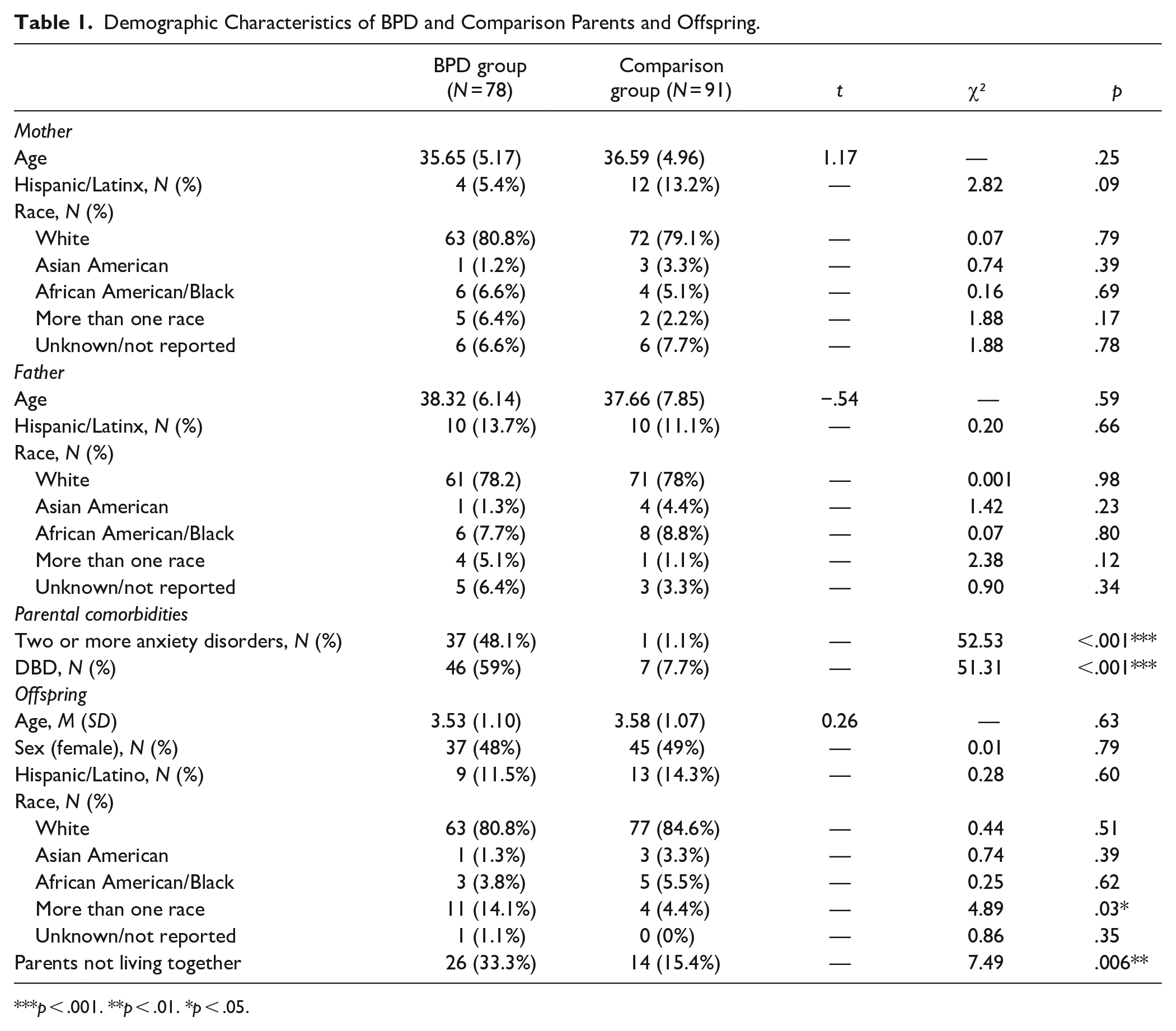
p < .001. **p < .01. *p < .05.
Emotional and Behavioral Symptoms in Offspring
CBCL T-scores for the two groups are shown in Table 2. Compared to offspring of comparison parents, BPDO had significantly greater mean scores on the Externalizing Problems Scale and on all subscales except the Withdrawn subscale, even when controlling for parental separation. They also had significantly higher means on the CBCL-BD profile. On the ERC, compared to offspring of comparison parents, BPDO had significantly greater mean scores on the ERC Lability scale but not the ERC Regulation scale. CRF scores (teacher or caregiver reports) were available for only 49% of the sample and showed no significant differences between groups for any scales. However, CBCL and CRF (parent and teacher) scores showed significant positive correlations with one another for all subscales except withdrawn and depressive symptoms.
Mean Emotional and Behavioral Symptoms and Emotion Regulation in BPDO and Comparison Offspring with Family Level Clustering.

Note. **p < .001. *p < .01; all analyses control for parent marital status (together vs. separated) and are nested within family.
To further explore clinical-level symptoms on the CBCL, we examined rates of children who had elevations above the clinical cutoffs for the overall scales (Internalizing, Externalizing, and CBCL-BD). Although the number of children in clinical range on the Internalizing scale was higher in the BPDO group, it did not reach significance (8/72 [11.1%] vs. 2/90 [2.2%]; Odds Ratio with 95% confidence interval 3.82 [0.74, 19.62], z = 1.61). However, the number of children in clinical range on the Externalizing scale was significantly higher in the BPDO group (12/72 [16.7%] vs. 2/90 [2.2%]; OR = 6.66 [1.37, 32.35], z = 2.35, p < .05). Further examination revealed that this was accounted for by higher rates of clinical elevation on the Aggressive Behavior (8/72 [11.1%] vs. 0/90 [0%]; p = .001 by Fisher’s Exact Test) and Oppositional Defiant Problems subscales (9/72 [12.5%] vs. 2/90 [2.2%]; OR = 4.86 [1.05, 22.52], z = 2.03, p < .05). When using the strict cutoff on the CBCL-BD of 210, only 3/72 (4.2%) of BPDO were elevated compared with 0/90 (0%) of comparison children (p = .086 by Fisher’s Exact Test). However, when we used the cutoff of 180 used in some other studies (Kim et al., 2012; Meyer et al., 2009; Wilens et al., 2013) that has been referred to as indexing “deficits in emotion self-regulation” (Wilens et al., 2013), we found significant elevations among BPDO (14/72 [19.44%] vs. 1/90 [1.11%]; OR = 16.65 [2.03, 136.33], z = 2.62, p < .01).
Psychiatric Disorders in Offspring
As shown in Table 3, relative to offspring of comparison parents, BPDO demonstrated significantly greater lifetime prevalence of any DBD, accounted for by higher rates of ADHD, CD, and ODD; of any mood disorder, accounted for by higher rates of mania; and of any anxiety disorder, accounted for by a higher rate of separation anxiety disorder. These analyses controlled for whether or not parents were living separately; family status did not contribute significant variance to any of these child disorders when parental BPD was in the equation.
Psychiatric Disorders in BPDO and Comparison Offspring with Family Level Clustering.

p < .001. **p < .01. *p < .05; where there were 0 cells, we used Fisher’s Exact Tests and reported p values only. All analyses controlled for parental separation.
Association Between Parental Psychiatric Disorders and Offspring Emotional and Behavioral Symptoms
Table 4 examines relative contributions of parental BPD and comorbid disorders in accounting for mean elevations in CBCL T-scores. For child Externalizing symptoms, both parental BPD status and parental DBD contributed significantly to the variance. On the one hand, BPD explained a significant portion of the variance in Oppositional Defiant Problems and Aggressive Behaviors while parental DBD did not. On the other hand, parental DBD explained a significant portion of the variance in ADHD problems, while parental BPD did not. For child Internalizing problems, parental anxiety disorders predicted a significant portion of variance whereas parental BPD did not. This pattern was maintained as well for the Anxiety Problems subscale.
Mixed Effects Linear Models with Family Level Clustering Predicting Child Symptoms.
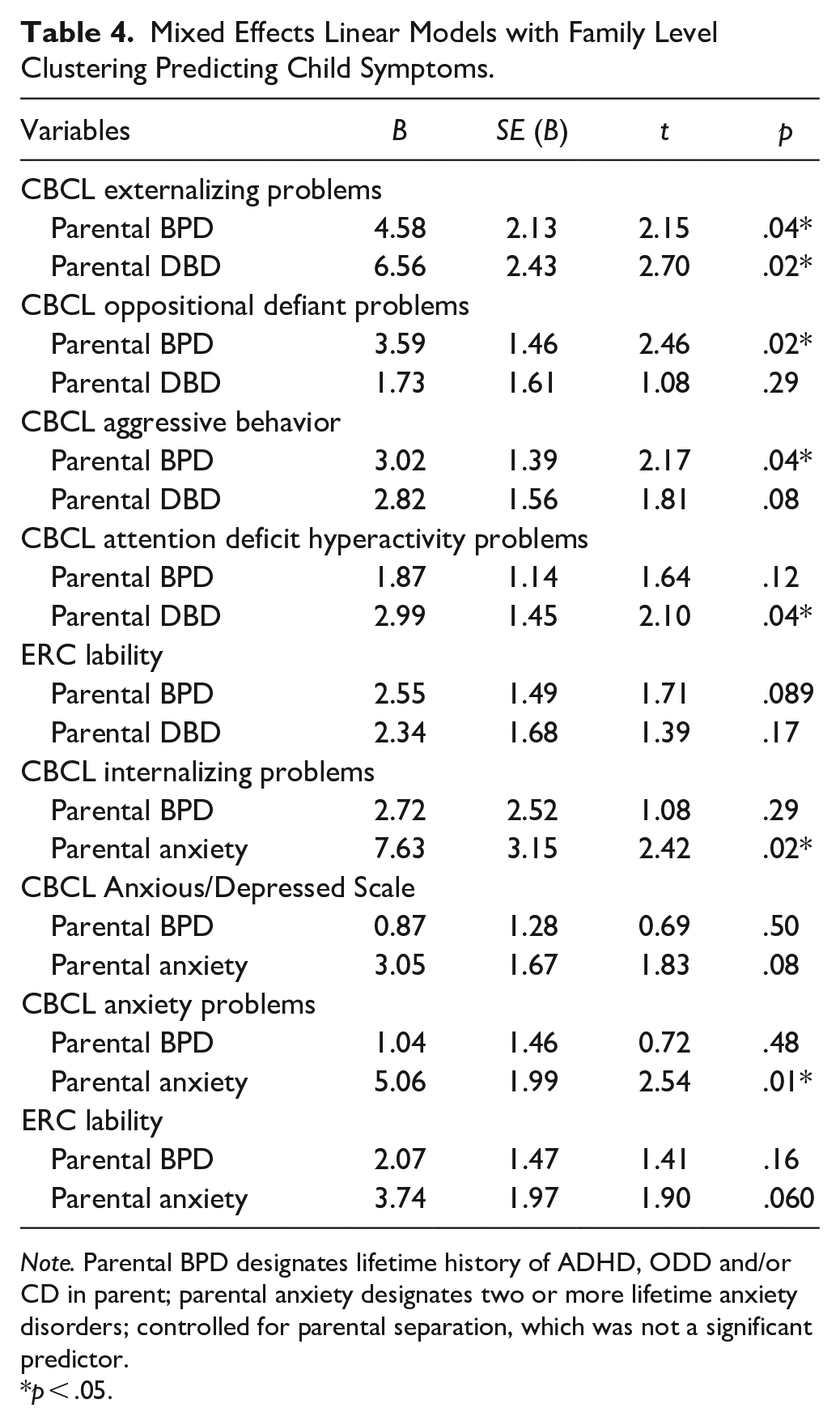
Note. Parental BPD designates lifetime history of ADHD, ODD and/or CD in parent; parental anxiety designates two or more lifetime anxiety disorders; controlled for parental separation, which was not a significant predictor.
p < .05.
Association Between Parental Psychiatric Disorders and Offspring Psychiatric Disorders
Table 5 examines relative contributions of parental BPD and comorbid disorders in accounting for child psychiatric disorders. When parent BPD and DBD were simultaneously entered as predictors, only parent BPD predicted increased likelihood of the child having a disruptive behavioral disorder, with a 5.6-fold increase in risk. When parental BPD and parental anxiety disorder were simultaneously entered as predictors, parental anxiety disorders significantly predicted increased likelihood anxiety disorder in offspring. Parental BPD was at trend significance (p = .05). Parental anxiety disorders increased the likelihood of an anxiety disorder in the child about 3-fold.
Logistic Regressions Testing Parent Diagnosis as Predictors of Child Diagnosis With Family Level Clustering.

p < .01; *p < .05.
Any behavioral disorder = child received diagnosis of ADHD, ODD, and/or CD; bAny anxiety disorder = child received diagnosis of GAD, social/avoidant anxiety, and/or separation anxiety; controlled for parental separation, which was not a significant predictor.
Discussion
Our results replicate findings by other investigators (Birmaher et al., 2010; Maoz et al., 2014) demonstrating that like older children, 2-5-year-old offspring of parents with BPD have significantly higher rates of clinically elevated symptoms and disorders across multiple psychiatric outcomes. They had significantly higher rates of clinically elevated Externalizing symptoms, Aggressive Behavior, and Oppositional Defiant Problems. When looking at continuous symptoms, although mean T-scores still fell within the normal range, BPDO had higher mean scores than comparison offspring on almost all CBCL subscales, including internalizing symptoms; syndrome subscales measuring emotional reactivity, anxious/depressed symptoms, and somatic complaints; externalizing symptoms; and syndrome scales measuring attention problems and aggressive behaviors. BPDO also had higher scores on sleep problems and on DSM-oriented scales including depressive problems, anxiety, ADHD problems, and oppositional defiant problems. On the ERC, a measure of emotional dysregulation, BPDO had higher ratings of emotional lability.
Moreover, preschool-age BPDO already exhibited significantly higher rates of ADHD, CD, ODD, anxiety disorders (specifically separation anxiety disorder), and mood disorders. Overall, a total of 55% of BPDO had at least one psychiatric disorder, compared to only 14% of control non-BPD offspring. Almost 40% of the BPDO met criteria for a disruptive behavior disorder, over 30% met criteria for one of the three major anxiety disorders assessed, and 10% already met criteria for mood disorder. The early onset of BPD in some of these young children accords with retrospective reports in clinically referred older pre-pubertal children, where the mean age of onset of BPD in two cohorts were 3.9 and 4.4 years (Biederman et al., 2004).
Of note, the mean Bipolar Disorder profile on the CBCL (CBCL-BD) was significantly higher among BPDO than among control offspring. The CBCL-BD is calculated by summing T-scores on the Attention Problems, Aggressive Behavior and Anxious/Depressed scales. Previous studies have shown that it has at least moderate accuracy in identifying concurrent pediatric BPD (Diler et al., 2009; Faraone et al., 2005; Kahana et al., 2003; Uchida et al., 2014) and that high scores capture severe psychopathology and dysfunction (Biederman et al., 2012). The profile has been found to run in families, that is, to correlate positively among siblings (Biederman et al., 2018) and to predict subsequent BPD. Biederman et al. (2009) found that elevated scores on the CBCL Dysregulation Profile in children ages 6 to 18 years predicted subsequent BPD diagnosis a mean of 7.4 years later. Others have found that the profile measured in childhood predicts BPD and other severe psychopathology in adulthood (Althoff et al., 2010; Meyer et al., 2009). As described by Maoz et al. (2014), our study also found that very young children at risk for BPD exhibit elevations on this profile. When using the 180 cutoff for the scale, which is thought to indicate deficient emotional self regulation (Kim et al., 2012; Meyer et al., 2009), over 19% of BPDO showed elevation on this subscale.
Interesting findings emerged when we looked at the relative contribution of parental comorbid disorders to childhood symptoms and disorders. Analyses of CBCL scores revealed that child externalizing symptoms were predicted both by parental BPD and by parental history of DBDs. Parental BPD, but not parental DBD, accounted for the variance in Oppositional Defiant Problems and Aggressive Behaviors. Similarly, when examining diagnostic outcomes, we found that parental BPD, and not parental DBD, predicted diagnosis with a disruptive behavior disorder. This finding highlights that disruptive behaviors in general, and oppositional and aggressive problems in particular, may reflect emotional dysregulation as it presents in early childhood. ODD, when associated with tantrums and reactive rather than proactive aggression, has been recognized as involving poor affective modulation and risk for later mood disorder comorbidity (Greene & Doyle, 1999).
The picture with regards to ADHD was less straightforward. On the one hand, child ADHD symptoms on the CBCL were more highly related to parental history of DBD than to parental BPD. This finding is consistent with the high heritability of ADHD (Faraone & Larsson, 2019) and with studies finding associations between child and parental ADHD (Uchida et al., 2021). It also accords with cross-sectional studies demonstrating higher rates of behavioral disinhibition and impulsivity in preschool-age BPDO compared to offspring of parents without BPD (e.g., Hirshfeld-Becker, Biederman, Henin, Faraone, Cayton, & Rosenbaum, 2006; Luby & Belden, 2006). On the other hand, parental BPD was more strongly associated with child DBD diagnoses (including ADHD) than parental DBD. One possible interpretation of these seemingly conflicting results draws on a family risk analysis suggesting that ADHD comorbid with pediatric BPD represents a distinct subtype that breeds true in families, with the two disorders co-segregating among relatives (Biederman et al., 2012). Since ADHD is known to have an earlier onset than pediatric mania and to be found at high rates in children with BPD (Biederman et al., 2004; Wozniak et al., 1995), it is possible that some of the young BPDO diagnosed with ADHD in our sample will go on to onset with comorbid BPD, accounting for the stronger association with parental BPD. For example, in a longitudinal study of BPDO, ADHD diagnosed in the child before age 6 predicted later onset of BPD in the child (Birmaher et al., 2021). Further research is needed to better evaluate the familial association between parental BPD and ADHD in preschoolers.
Our finding that child anxiety symptoms on the CBCL and anxiety disorder diagnoses were predicted by parental anxiety disorders more strongly than by BPD is consistent with the extensive literature documenting that parental anxiety disorders confer risk for child anxiety (e.g., Hirshfeld-Becker et al., 2012; Micco et al., 2009). Our study confirms findings by others that preschool-age BPDO are at risk for higher levels of anxiety symptoms compared to non-BPD offspring (Birmaher et al., 2002; Hirshfeld-Becker, Biederman, Henin, Faraone, Cayton, & Rosenbaum, 2006; Masi et al., 2004), but suggest that this risk may be driven by parental anxiety disorder rather than BPD itself.
Further research is needed to determine whether early or preventive interventions can specifically reduce or mitigate rates of onset of BPD in these youth, and the degree to which they affect later functioning. Additionally, since almost half of the BPDO did not have a psychiatric diagnosis, future studies should examine genetic and psychosocial risk and protective factors contributing to differences in offspring’s adaptive function. Additional research identifying biomarkers of risk for mood disorders is needed to further understand the risk conferred from parent to child.
Findings from this study suggest that preschool-age children of parents with BPD should be carefully monitored for onset of psychiatric symptoms and disorders and provided with appropriate clinical intervention and support. Half of the BPDO in our sample already met diagnostic criteria for psychiatric diagnoses and were likely in need of early intervention to mitigate impact on social and academic development. Disorders such as anxiety in young children are often misperceived as being transient and un-impairing despite evidence that they are often associated with persistent distress and impairment (Egger & Angold, 2006). Clinical studies suggest that children with pediatric BPD (Marchand et al., 2006) and anxiety disorders (Hammerness et al., 2008) may wait an average of 5 years or longer from the time of onset of disorder to the time of first treatment. During this long wait, these children may undergo significant symptomatic worsening, functional deterioration, and adverse impact on learning, self-image, friendships and family relationships.
In addition, our results highlight that externalizing symptoms and emotional dysregulation in preschoolers, particularly those at risk for BPD, may reflect early symptoms of mood disorder and should be monitored and appropriately recognized as such. In clinical practice, older children may be treated pharmacologically with repeated stimulant trials for “severe ADHD” when the associated dysregulation, reactive aggression and oppositional behavior may reflect an underlying mood disorder. As Spencer et al. (2001) have pointed out, recognizing mood disorders in children with DBDs enables disorders previously thought of as refractory ADHD, ODD or CD to be treated with mood stabilization.
Our findings may also inform the types of preventive CBT interventions that might be utilized in early childhood to promote better affective regulation. For example, young offspring of parents with BPD who exhibit behavioral symptoms could be referred for parent-child interventions including positive parenting, collaborative problem solving (Greene et al., 2004), or parent child interaction therapy (Thomas et al., 2017). Supporting parents in finding ways to prevent and de-escalate these child behaviors in ways that promote adaptive function and problem solving is very important, as research has shown that these behaviors may elicit more negative parenting styles, with parents of dysregulated children engaging in more punitive and controlling parenting styles, or alternatively, increased permissiveness (Kim et al., 2012).
Young BPDO and comorbid anxiety disorders might be referred for parent-implemented CBT, a treatment with established efficacy for reducing anxiety in young children (e.g., Comer et al., 2019; Hirshfeld-Becker et al., 2010), that has also been shown to reduce onset of depression in adolescent girls (Rapee, 2013). Although anxiety disorders may be distinct from the BPD itself, because of the impairment and avoidance they entail, treating them early might improve functional outcomes even in the event of a comorbid mood disorder. In addition, interventions that address parents’ own symptoms and dysregulation, if present, would also be expected to benefit the children. Parental BPD may also be associated with other psychosocial stressors that may confer risk for child disorders; policies and interventions designed to ameliorate early life stressors associated with parental mental illness may also be particularly impactful on youth outcomes. In the present study, BPDO were less likely to live with both parents in the same household, and this factor was itself associated with child symptoms and disorders. Familial transmission of mood disorders reflects a complex interplay of biological and psychosocial factors; preventative interventions must be sufficiently broad to capture the range of known risk factors while being individualized and targeted to the needs of any given child and family (Duffy et al., 2023).
Our findings should be viewed in light of methodological limitations. First, we used a community sample recruited through advertisements. However, our careful recruitment and diagnostic strategies ensured that the parents we recruited with BPD met criteria for clinical caseness. Nonetheless, future studies utilizing clinical and epidemiologic samples are needed to confirm results. Second, we relied on parent-reports of child symptoms. Data from teachers/caregivers were limited because many children in this age range were not in day care or preschool, and it is likely that children who were more symptomatic were less likely to be attending daycare or preschool. Nonetheless, among the offspring who did have teacher/caregiver-report data, parent and teacher reports of symptoms were generally positively and significantly correlated. Third, although our sample was representative of the broader population of the counties served by our clinical center, White, non-Hispanic participants were overrepresented compared to national rates. The impact of parental psychopathology on child mental health may vary depending on a range of environmental and individual level factors including demographic factors and exposure to life stressors. The expansion of this research in samples with greater socioeconomic, racial, and ethnic diversity is a critical next step in order to generalize findings from this study.
Despite these limitations, our findings confirm that very young children with BPD parents, like their older child and adolescent counterparts, are at risk for a broad array of clinically elevated mental health symptoms and disorders, particularly ADHD, behavioral disorders, and anxiety disorders. Most significantly, our findings highlight the relative contribution of parental BPD compared to other common co-occurring disorders in predicting young child symptoms and disorders. Specifically, parent BPD predicted DBD in young children above and beyond effects of parental DBD, whereas anxiety disorders in parents accounted for significantly more variance than BPD in predicting child anxiety symptoms and disorders. These findings underscore the importance of identifying children at highest risk for early psychiatric symptoms and may guide the selection and implementation of specific preventive or early interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Henin receives book royalties from Oxford University Press. The other authors have no relevant financial or non-financial interests to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by R01 MH076923 (PI: Hirshfeld-Becker)
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional review board at Massachusetts General Hospital/ Mass General Brigham and conducted in accordance with the ethical standards of the American Psychological Association.
Informed Consent
Informed consent was obtained from all individual participants included in the study.