
Abstract
Objective:
We analyzed adult ADHD symptoms in a cross-cultural context, including investigating the occurrence and potential correlates of adult ADHD and psychometric examination of the Adult ADHD Self-Report Scale (ASRS) Screener.
Method:
Our analysis is based on a large-scale research project involving 42 countries (International Sex Survey, N=72,627, 57% women, Mage=32.84; SDage=12.57).
Results:
The ASRS Screener demonstrated good reliability and validity, along with partial invariance across different languages, countries, and genders. The occurrence of being at risk for adult ADHD was relatively high (21.4% for women, 18.1% for men). The highest scores were obtained in the US, Canada, and other English-speaking Western countries, with significantly lower scores among East Asian and non-English-speaking European countries. Moreover, ADHD symptom severity and occurrence were especially high among gender-diverse individuals. Significant associations between adult ADHD symptoms and age, mental and sexual health, and socioeconomic status were observed.
Conclusions:
Present results show significant cross-cultural variability in adult ADHD occurrence as well as highlight important factors related to adult ADHD. Moreover, the importance of further research on adult ADHD in previously understudied populations (non-Western countries) and minority groups (gender-diverse individuals) is stressed. Lastly, the present analysis is consistent with previous evidence showing low specificity of adult ADHD screening instruments and contributes to the current discussion on accurate adult ADHD screening and diagnosis.
Introduction
Attention deficit/hyperactivity disorder (ADHD) is one of the most common childhood psychiatric disorders (e.g., Polanczyk & Jensen, 2008), where symptoms have traditionally been considered to diminish or cease in late adolescence or early adulthood (Hill & Schoener, 1996). Although it is now known that impairing levels of symptoms often persist into adulthood (Caye et al., 2016; Kooij et al., 2010), screening, diagnosis, and treatment of ADHD in adults lag behind those in children and require further exploration.
Two central features of ADHD include inattentiveness and impulsiveness/hyperactivity which are inconsistent with the child’s developmental level (American Psychiatric Association [APA], 2013). The abovementioned factors have been found to be consistent across cultures for children (e.g., Bauermeister et al., 2010), suggesting common genetic and neurobiological underpinnings of the disorder, which are at least to some degree, not dependent on cultural factors (Meyer, 2005). At the same time, the basic character of adult ADHD across cultures did not undergo similar scrutiny, and previous analysis suggests significant cultural variability in its prevalence, rate of diagnosis, and treatment (Fayyad et al., 2017; Gómez-Benito et al., 2019; Timimi & Taylor, 2004). The present study focuses on the subject of adult ADHD screening in a cross-cultural context, employing and psychometrically evaluating one of the most established measures for adult ADHD assessment, the Adult ADHD Self-Report Scale (ASRS) Screener (Kessler et al., 2005, 2007).
The ASRS Screener and Adult ADHD Assessment
The extended version of the ASRS Screener and its direct predecessor, the ASRS, were developed by the World Health Organization (WHO) World Mental Health Initiative as previously existing measures of adult ADHD failed to address all 18 Diagnostic and Statistical Manual of Mental Disorders (DSM) IV symptoms (Kessler et al., 2005, 2007). Further analysis showed that the same, or even higher, diagnostic precision of the full 18-item ASRS can be achieved with 6 items, creating a unidimensional, shortened version of the full scale (i.e., the ASRS Screener). This version of the screener offered the best psychometric properties and was characterized by a sensitivity of 68.7% and specificity of 99.5%, with a total classification accuracy of 97.9% and high internal consistency (Kessler et al., 2005, 2007). Moreover, the ASRS Screener has demonstrated good test-retest reliability (Matza et al., 2011) as well as high sensitivity to identify ADHD in clinical samples (e.g., for people seeking treatment for substance use disorders; Van De Glind et al., 2013). Recently, the ASRS Screener has been updated to better fit DSM-5 diagnostic criteria for adult ADHD (APA, 2013), although its 6-item length remained unchanged (Ustun et al., 2017). In the current cross-cultural analysis, we are using the original DSM-IV version. Initial work on a clinical sample showed that DSM-IV and DSM-5 versions achieve almost identical psychometric characteristics in terms of sensitivity, specificity, and positive and negative predictive value (Bastiaens & Galus, 2018).
It is worth noting that adult ADHD screening—including the ASRS Screener—is limited by several challenges. First, positive adult ADHD diagnosis currently requires symptoms to be present during childhood, that is, knowledge about recent level of symptoms is not sufficient for a diagnosis. Secondly, symptoms of ADHD are non-specific and can appear in the course of a wide variety of conditions, including anxiety, mood, and substance use disorders (e.g., National Collaborating Centre for Mental Health UK [NCCMH UK], 2009). Lastly, self-report measures are also prone to multiple biases and may be manipulated by respondents (Lovett & Harrison, 2021). Therefore, clinicians should not rely on self-report alone for ADHD assessment, as multiple factors may result in high false-positive rates in self-report screening measures.
Available reports show that the rate of clinical diagnosis of ADHD in the US and some other Western countries has undergone a several-fold increase in the 21st century (e.g., McCarthy et al., 2012; Olfson et al., 2013), which is possibly facilitated by the limitations of screening tools to assess ADHD accurately. However, exaggeration of symptoms by individuals to obtain prescription medications (i.e., stimulants to enhance cognitive performance or for recreational purposes) or disability accommodations have been linked to ADHD overdiagnosis (e.g., Lovett & Harrison, 2021). Given these factors, a surge of ADHD diagnoses in the US has been termed as an epidemic problem (Paris et al., 2015). On the other hand, adults with ADHD often describe experiencing significant concerns in multiple domains that may not be adequately appreciated or identified by clinicians (Ginapp et al., 2022, 2023). This indicates that further work is needed to better understand the disorder and its repercussions.
An important research avenue in adult ADHD research lies outside of the so-called “WEIRD” populations (i.e., Western, Educated, Industrialized, Rich, and Democratic populations) involving groups underrepresented in research (e.g., Fayyad et al., 2017; Gómez-Benito et al., 2019). Much prior research on adult ADHD has been based on student samples (Lovett & Harrison, 2021), which calls for research efforts targeting populations including older individuals.
Adult ADHD Prevalence and Cultural Context
The prevalence estimates of adult ADHD assessed with the ASRS, as well as other screening tools, differ largely across studies depending on the sample’s characteristics, grading criteria, and cut-off values (e.g., Song et al., 2021). As direct cross-cultural comparisons have been rare in previous studies, it is challenging to determine whether differences in estimates may derive from methodological, sample-related, cultural, or other types of differences (Polanczyk et al., 2007). One notable multi-country initiative that allowed for direct-cross cultural comparisons of the prevalence of ADHD in adults is the WHO World Mental Health Surveys (Fayyad et al., 2017). The study was based on standardized interviews administered face-to-face in respondents’ homes, assessing a range of DSM-IV disorders. The study involved participants from 20 countries and showed that ADHD occurrence was estimated to be the highest in Western high-income countries like France (7.3%), Northern Ireland (6.0%), and the USA (5.2%)—and lower in middle/low-income countries, for instance Iraq and Romania (both 0.6%; Fayyad et al., 2017).
Occurrence estimates based on self-report surveys employing large-scale national samples range from 2.1 to 11.4% (Adler et al., 2019, N = 22,397, 2.1%, US sample; Kessler et al., 2006, N = 3,199, 4.4%, US sample; Polanczyk et al., 2010, N = 3,007, 5.8%, representative Brazilian sample; Vňuková et al., 2021, N = 1,518, 7.8%, Czech sample; Weissenberger et al., 2018, N = 1,012, 11.4%, Czech sample). In rare cases, reported adult ADHD occurrence in general population convenience samples has been higher (20.2%; Panagiotidi et al., 2019, N = 344; mostly British sample). In clinical psychiatric populations, adult ADHD rates typically exceed 20% (e.g., Syed et al., 2010, N = 243). Moreover, early conceptualizations suggested that ADHD was more prevalent in males (APA, 2013). Currently, however, some researchers claim this disproportion results from the underestimation of female cases arising from bias in sampling, differences in symptomatology or presentation or other factors (Simon et al., 2009).
Although cross-cultural comparative research on ADHD is scarce, findings suggest the existence of cultural differences regarding perceptions of ADHD and ADHD-like symptoms (e.g., Fayyad et al., 2017; Song et al., 2021). As degrees of support versus discouragement towards hyperactive or impulsive behavior may differ between cultures, perceptions of what behavior is considered problematic or disordered may also differ (e.g., Gómez-Benito et al., 2019; Timimi & Taylor, 2004). Thus, quantitative research of ADHD occurrence and treatment-seeking individuals may partially reflect cultural expectations and the influence of cultural environment on behavior (Kooij et al., 2010).
Present Study Goals and Adult ADHD Related Factors
The goal of the present study was to investigate cross-cultural variability in adult ADHD symptoms, by analyzing symptom severity, occurrence of scoring at risk for adult ADHD, and cross-cultural measurement invariance, reliability, and validity of the ASRS Screener across analyzed country samples. Attention was given to non-Western countries, in which ADHD diagnosis is not as established, and to minority samples (e.g., gender-diverse individuals). Investigating cross-cultural measurement invariance is essential, as it shows whether the analyzed underlying construct and employed instrument have the same structure, are interpreted in similar ways, and have comparable applicability in different languages, countries, or subgroups like gender-based ones (e.g., Davidov et al., 2014).
Next, several factors potentially relevant to adult ADHD were analyzed, including age, gender, socioeconomic status, and mental, physical, and sexual health. Previous analysis showed that ADHD symptoms may decline with age (e.g., Faraone & Biederman, 2005), be more severe in gender minority individuals (Bretherton et al., 2021; Dawson et al., 2017), people affected by socioeconomic disadvantage (Russell et al., 2014), and be associated with increased odds of various psychiatric disorders (NCCMH UK, 2009).
Method
Procedure
The International Sex Survey (ISS) is a large, cross-sectional, multi-national study, conducted online in 42 countries. 1 The study design was preregistered (https://osf.io/uyfra).
Translation
The original (English) version of test battery was translated into 25 other languages, according to guidelines of a pre-established translation procedure for cross-cultural studies (Beaton et al., 2000). The translation procedure is also described in more detail in the previously published study protocol (Bőthe et al., 2021).
Data Collection
Data for the ISS were collected between October 2021 and May 2022 in all collaborating countries. Participants who responded to the study advertisements completed an anonymous survey on the Qualtrics Research Suite, which took approximately 25 to 45 minutes. Detailed information regarding data collection was described previously (Bőthe et al., 2021).
To ensure transparency of data use, all published manuscripts and conference presentations which employ data gathered as part of the ISS project are available using the following links: publications, https://osf.io/jb6ey; conference presentations, https://osf.io/c695n.
Ethics
The study was conducted in accordance with the Declaration of Helsinki. The study procedures were approved by appropriate ethics review boards for collaborating countries or, in some cases, the appropriate ethics review boards considered the study exempt from additional approval as it had already been approved by the ethics review boards of the principal investigators’ institutions (https://osf.io/n3k2c). All participants were informed about the study and provided informed consent.
Participants
On the data preprocessing stage, participants who (a) failed more than one out of three attention questions and/or (b) produced response patterns suggesting inattentiveness (e.g., contradictory answers to several questions, see https://osf.io/uyfra for a detailed description). Next, after excluding all participants with missing values in the variables of interest, data collected from 72,627 participants (Mage = 32.84, SD = 12.57) were included in the analyses. Of all participants, 41,360 identified as women (57.0% of the total sample), 28,877 as men (39.8%), and 2,390 (3.3%) as gender-diverse individuals. Detailed sociodemographic distribution is presented in Table 1.
Participants’ Sociodemographic Characteristics.

Measures
The complete set of measures collected, including item questions and available responses in all languages, can be found following the link: https://osf.io/jcz96. Outlined below are measures focal to the current analyses.
Adult ADHD symptom severity was assessed using the ASRS Screener (Kessler et al., 2007). This questionnaire is a 6-item screening measure for adult ADHD symptoms and is an abbreviated version of the 18-item ASRS, developed by the World Health Organization (Kessler et al., 2005). It measures the frequency of relevant behaviors (on a scale from 0 [Never] to 4 [Very often]).
For the ASRS Screener validity analyses, we included additional measures. With three separate questions, we gathered information about participants’ self-reported (1) mental, (2) physical, and (3) sexual conditions. Response options were 0 (indicating that a participant is not suffering from mental, physical, or sexual condition) and 1 (indicating that a participant is suffering from mental, physical, or sexual condition). As an indicator of relative socioeconomic status, respondents were also asked to rate their life circumstances in comparison to the others. Response options ranged from 1 (among the worst) to 7 (among the best).
Data Analysis
All analytical procedures were performed in the R computational environment (R Core Team, 2019). Preregistered analysis plan can be found using the link https://osf.io/dk78r. R code used for the statistical analysis can be found following the link https://osf.io/w6dvh/?view_only=ce8cc37f36d34240b687b548385a89a0.
Descriptive Analysis
First, descriptive statistics were calculated for all ASRS Screener items. We rejected the hypothesis that the data were missing non-randomly, based on Little’s missing completely at random test, χ2(105) = 106.21, p = .449). On this basis, all observations with missing values in any of the ASRS Screener items were removed.
Dimensionality
The dimensionality of the ASRS Screener was assessed using CFA. Evaluation of model fit was based on established goodness-of-fit metrics (Marsh et al., 2005; Schermelleh-Engel et al., 2003): Comparative Fit Index (CFI; ≥.90 adequate; ≥.95 good), Tucker-Lewis Index (TLI; ≥.90 adequate; ≥.95 good), and Root-Mean-Square Error of Approximation with its 90% confidence interval (RMSEA; ≤.10: acceptable, ≤.08: adequate, and ≤.05: good; Kenny et al., 2015; Schermelleh-Engel et al., 2003). The diagonally weighted least square estimator was used for fitting the CFA and measurement invariance models (Finney & DiStefano, 2013).
Measurement Invariance
To minimize measurement bias and maximize inter-group comparisons validity, tests of measurement invariance were performed with language, country, and gender of participants as grouping variables (Millsap, 2011; Vandenberg & Lance, 2000). Six levels of invariance were tested with increasingly constrained parameters: configural (i.e., same structure across groups), metric (i.e., same factor loadings across groups), scalar (i.e., same item intercepts across groups), and residual (i.e., same residual covariance across groups), as well as latent variance-covariance, and means invariance (Milfont & Fischer, 2010; Vandenberg & Lance, 2000).
Significant changes in RMSEA (ΔRMSEA ≤ .015) and CFI (ΔCFI ≤ .01) suggested which level of measurement invariance was achieved (Chen, 2007; G. W. Cheung & Rensvold, 2002). We also reported additional goodness-of-fit metrics (TLI) to account for model parsimony in model comparisons (Marsh et al., 2005, 2013). In cases where full invariance was not achieved, partial invariance tests were performed by progressively releasing equality constraints (i.e., factor loading, intercept, and residual covariance parameters for a given item) in the order according to the expected χ2 difference until assumed cut-off values for the changes in RMSEA and CFI were met (Milfont & Fischer, 2010) or the number of modification indices was exhausted.
For measure invariance tests, based on an a priori Monte Carlo simulation (see details in https://osf.io/dk78r), only groups consisting of a minimum of 460 participants were retained. Accordingly, in the language-based measurement invariance tests, 20 of 26 groups met the minimum group size criterion, 32 out of 42 groups for country-based tests and all three gender groups (i.e., men, women, gender-diverse individuals) meeting the size criterion for gender-based tests.
Reliability, Validity, and Screening Threshold
ASRS Screener reliability was assessed using Cronbach’s alpha and McDonald’s omega (McDonald, 1970; McNeish, 2018; Nunnally, 1978). Validity was assessed by calculating ASRS Screener general score correlations with theoretically relevant characteristics and testing for differences in total ASRS Screener scores between participants who identified themselves as men, women, or gender-diverse individuals (one-way analysis of variance; η2 is provided as effect size as well as Cohen’s d for pairwise comparisons).
Results
Descriptive Statistics and Confirmatory Factor Analysis of the Full Sample
A one-factor measurement model was fit to the data with acceptable goodness-of-fit (RMSEA = 0.093, 95% CI [0.091, 0.095]; CFI = 0.945; TLI = 0.909). Although the obtained RMSEA was slightly higher than the recommended target value of <0.08, given that other indicators achieved acceptable scores, the tested model was unidimensional and based on only 6 items (which should be considered when evaluating RMSEA; Kenny et al., 2015), we proceeded with this model with no additional adjustments. Summary statistics for ASRS total score, items, and standardized factor loadings are presented in Table 2.
Descriptive Statistics, Standardized Factor Loadings in the Confirmatory Factor Analysis, and Reliability Metrics of the ASRS Screener.
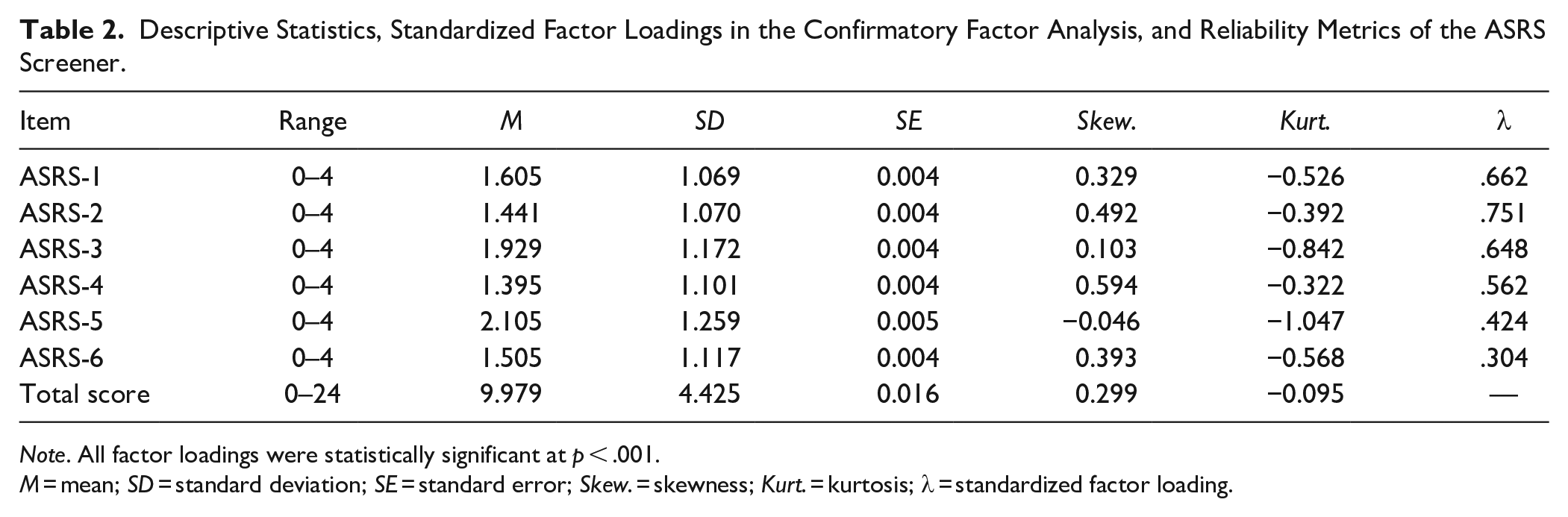
Note. All factor loadings were statistically significant at p < .001.
M = mean; SD = standard deviation; SE = standard error; Skew. = skewness; Kurt. = kurtosis; λ = standardized factor loading.
Measurement Invariance Across Language, Country, and Gender Groups
First, measurement invariance was assessed across language groups. Descriptive statistics for countries included in measurement invariance tests are given in Supplemental Materials in Table S1. Table S1 contains both unadjusted means for the ASRS Screener in respective country-based subsamples, as well as means adjusted for age and gender as those basic characteristics differed between country subsamples and may have relevance for the presentation of ADHD symptoms. Additionally, both empirical (unadjusted) and adjusted means are depicted in Figure 1. Next, mean comparisons for the countries included in measurement invariance tests are depicted in Tables S2 (unadjusted means) and S3 (means adjusted for age and gender). Since changes in RMSEA and CFI values in the measurement invariance tests did not meet the assumed cut-offs, subsets of constraints were relaxed, resulting in acceptable changes in goodness-of-fit metrics up to the level of residual invariance. Second, measurement invariance across country groups was assessed. Like in the language-based tests, partial invariance was tested by relaxing select constraints. Again, this method resulted in adequate changes in goodness-of-fit metrics up to residual invariance. Third, measurement invariance across genders was also tested. The same method was used as described above, resulting in partial invariance, this time up to a variance-covariance level.
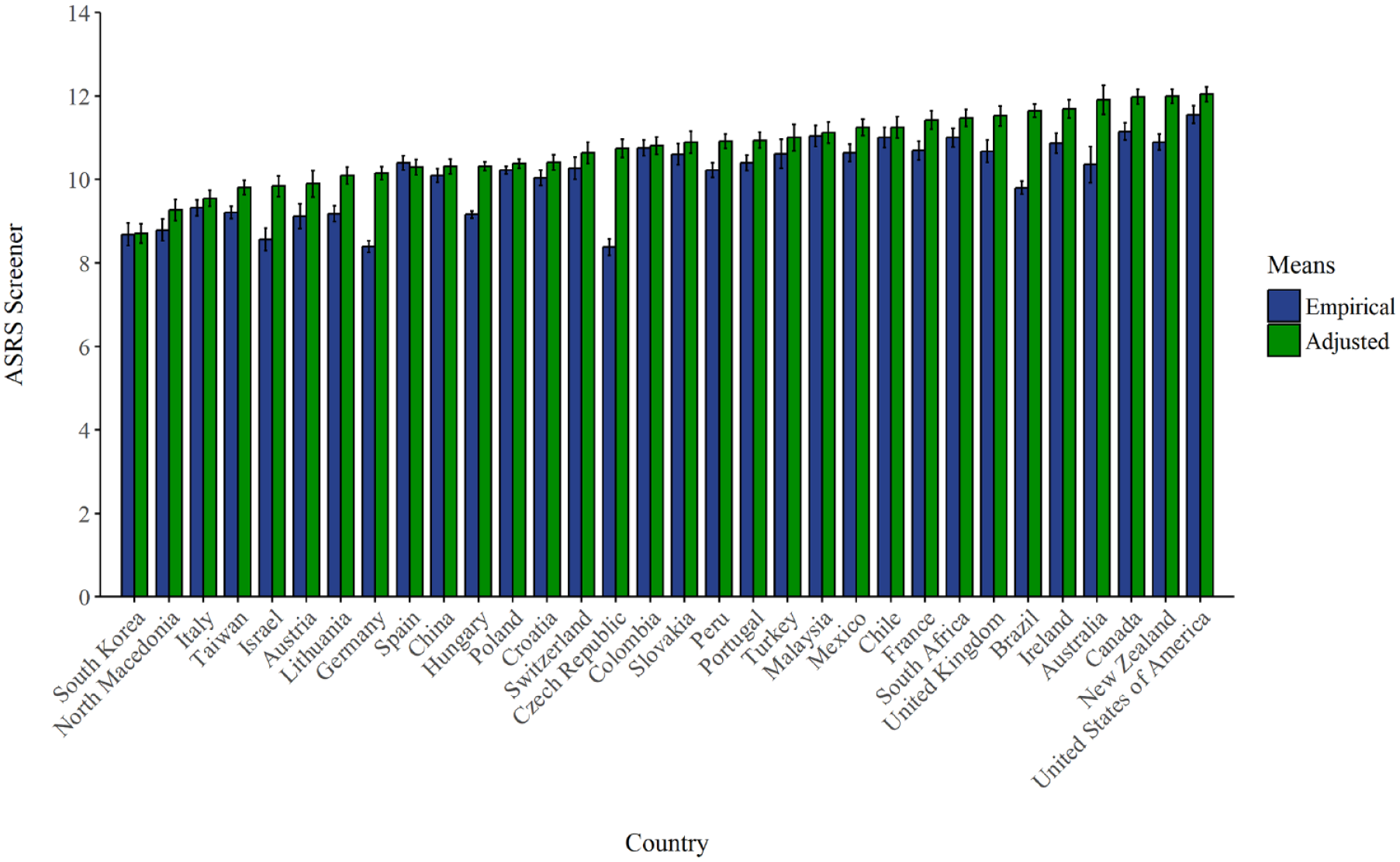
ASRS screener mean scores in respective countries included in measurement invariance tests: empirical (unadjusted) and adjusted for age and gender.
These results suggest that, while differences in group means may be present, no significant measurement biases exist across the examined variables. The results of all measurement invariance test sets, along with a detailed description of relaxed constraints, are available in Supplemental Materials (Tables S4–S6).
Reliability and Validity
The ASRS demonstrated adequate reliability, as evidenced by acceptable values of the Cronbach’s alpha (α = .73) and McDonald’s omega (ω = .82). There were also differences in ASRS scores with respect to gender, F(2; 72,624) = 855.57, p < .001, η2 = .02, with gender-diverse individuals scoring higher (M = 13.20, SD = 4.89) than women (M = 10.14, SD = 4.36; t(72,624) = 33.25, p < .001, Cohen’s d = 0.66), who in turn, scored higher than men (M = 9.49, SD = 4.35, t(72,624) = 19.35, p < .001, Cohen’s d = 0.15).
In addition, the ASRS Screener score had weak to moderate associations with theoretically relevant variables (Figure 2), including age (r = −0.28, p < .001), socioeconomic status (r = −0.11, p < .001), self-reported experiences with mental illness (r = 0.32, p < .001), and sexual problems (r = 0.09, p < .001), but not physical illness (r = < 0.01, p = .218).
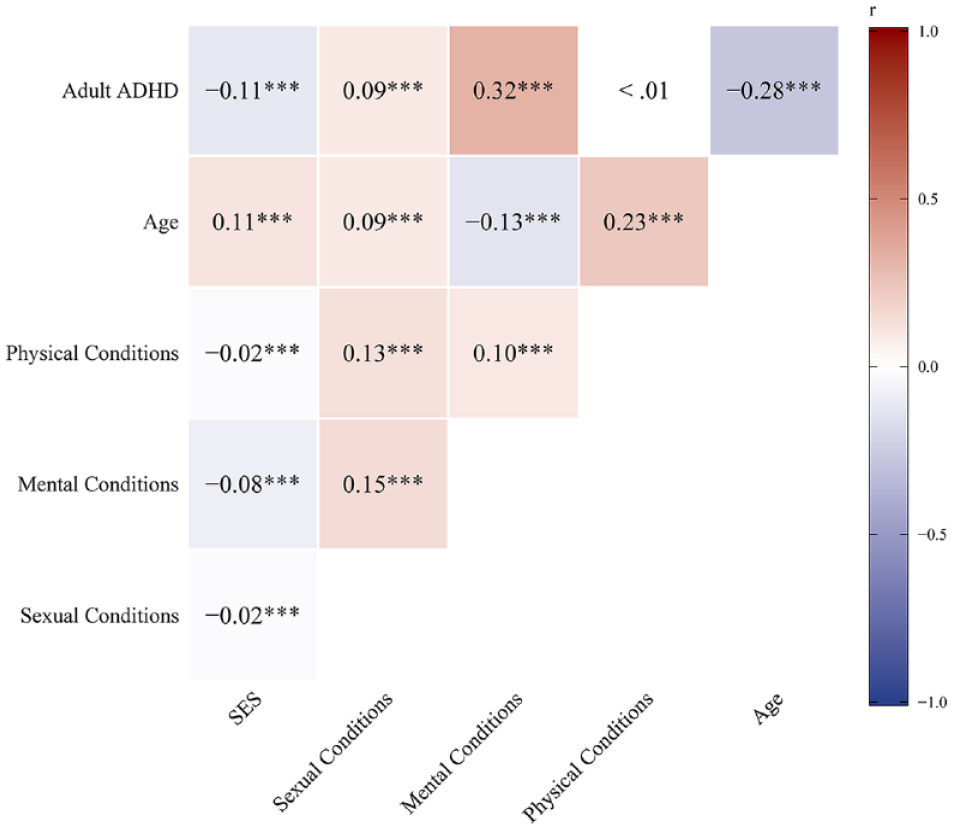
Associations between adult ADHD symptoms and selected factors (Pearson’s r).
Applicability of the ASRS Cut-Off Score
Applicability of the diagnostic cut-off score for the ASRS Screener was assessed by calculating the proportion of individuals who screened positive using the established threshold of 14 points or more (Kessler et al., 2007). 20.9% of participants (15,201 out of N = 72,627 participants) scored above the screening threshold, indicating higher risk of adult ADHD. Comparisons of participants who scored lower or higher on the ASRS Screener in their respective countries are presented in Table 3. In terms of gender, 21.4% of women (8,838), 18.1% of men (5,213), and 48.1% of gender-diverse individuals (1,150) scored above the threshold.
Percentages of Participants Who Scored Lower or Higher Than the Pre-Established Cut-off Value for the ASRS Screener.

Discussion
The aim of the article was the cross-cultural examination of adult ADHD symptoms, filling a gap in research on adult ADHD outside of WEIRD populations and among groups underrepresented in research (e.g., gender-diverse individuals). Concurrently, the present study allowed for achieving these aims while investigating the psychometric properties of one of most popular self-report screening measures, the ASRS Screener. First, the unidimensional model of the ASRS Screener was tested and found to fit the data well for the whole sample. This result supports the notion that the ASRS Screener assesses a single underlying construct. The factor loadings of all 6 items were sufficiently high, and the internal consistency achieved for the measure was also high. Overall, this supported the notion that the 6-item ASRS Screener is an internally coherent, unidimensional brief tool for assessing general ADHD symptoms in adults.
The ASRS Screener achieved partial invariance across languages and countries up to the residual invariance level. For gender groups, full metric invariance was achieved, with partial invariance up to the variance-covariance level. This indicates that although some differences in item interpretation and measurement may exist, the basic structure of the adult ADHD symptoms as assessed by the ASRS Screener was similar across the country, language, and gender groups. However, it should be noted that relaxing constraints as part of testing partial invariance on different levels has implications for the interpretability of the results, as well as the generalizability of the questionnaire and inter-group comparisons (Millsap, 2011; Vandenberg & Lance, 2000). Therefore, the present findings should be interpreted cautiously (implications of relaxing equality constraints on each of these levels are further detailed in the Supplemental Materials).
Occurrence of Being at Risk for Adult ADHD Across Countries
The occurrence rates estimated in the current study for different countries varied starkly between 9.1 and 32.3%. For most countries in the study (29 of 42), estimates exceeded 20%, higher than those usually reported in previous studies where estimates of current occurrence reached up to 15% (Adler et al., 2019; Kessler et al., 2006, 2007; Vňuková et al., 2021; Weissenberger et al., 2018). Of the countries which qualified for measurement invariance analysis, the highest percentages of being at-risk for adult ADHD were noted for the US (34.9%) and Canada (31.0%), followed predominantly by other Western countries for which English is the primary language: South Africa (29.6%), Ireland (28.8%), New Zealand (28.5%), and the United Kingdom (28.0%). The lowest occurrence was found in a more diverse group of countries including non-English speaking European countries (predominantly not Western European) as well as East Asian countries: Germany (10.0%), North Macedonia (13.2%), Taiwan (13.8%), Israel (14.4%), Lithuania (14.6%), Hungary (15.5%), and South Korea (17.2%). Similarly, gender- and age-adjusted means (which may offer less biased estimates) of adult ADHD symptom severity were highest in the US, New Zealand, Canada, Australia, and Ireland, while lowest in South Korea, North Macedonia, Italy, Taiwan, and Israel.
When interpreting results, it is important to note that the ASRS was designed as a screener. Hence, false positives will exist. Thus, scoring above the diagnostic threshold for ASRS Screener may not reflect a case and should rather call for further clinical assessment. As discussed earlier, symptoms characteristic of ADHD, including inattentiveness, impulsiveness, and hyperactivity, are non-specific to ADHD and may relate to other disorders and behavioral problems (NCCMH UK, 2009). Similar to other measures of adult ADHD, the ASRS Screener does not provide information about the possible childhood onset of the disorder. While this is currently needed for diagnosis, it should be noted that in some cases, ADHD only presents first in adulthood. This might be especially the case with women and others for whom inattentiveness is the leading symptom. Nonetheless, recent findings suggest a high rate of false-positives using self-report screeners for adult ADHD (Chamberlain et al., 2021). Moreover, in the present study, samples were not representative of the national populations, and reported percentages should not be considered an accurate representation of ADHD prevalence or severity as reported across languages, countries, and genders.
Further possible explanations for being at risk for adult ADHD may be related to increased diagnoses of ADHD in the 21st century (and possible overdiagnosis), especially in Western countries. Evidence supporting this hypothesis shows a six-fold increase in cases in which stimulants were prescribed from 1994 to 2009 in the USA alone (Olfson et al., 2013), and doubling in the UK between 2004 and 2009 (McCarthy et al., 2012). Moreover, the previous analysis provided initial evidence that excessive use of digital media among adolescents, which has also increased recently, has been associated with subsequent, significant increases in self-reported ADHD symptoms (Ra et al., 2018).
Increasing rates of adult ADHD diagnosis in Western countries may also be connected to ADHD-related information being accessible and proliferated in Western countries (especially English-speaking countries, where people can easily access much ADHD-related information). Previous findings (Suhr & Wei, 2017) show that exposure to popular information on ADHD can make people focus on their self-perception of impulsive and inattentive behavior seemingly fitting ADHD symptom descriptions, even when they do not meet the formal criteria for the disorder. Next, in the process of formal diagnosis and/or screening, people may inaccurately (although honestly) report heightened levels of symptoms (Suhr & Wei, 2017). Thus, cultural factors related to ADHD may be partially responsible for differences in adult ADHD symptom severity in the countries analyzed in the current study. Lastly, another possible explanative route in light of which current results can be considered is based on previous, initial evidence showing elevated severity of ADHD symptoms as related to the COVID-19 pandemic (Behrmann et al., 2022). As the present research was conducted during the COVID-19 pandemic, findings should be treated with caution.
Sociodemographic Factors and Other Adult ADHD-Related Variables
Analysis of factors potentially associated with adult ADHD in the current work brought significant evidence of convergent analysis of the ASRS Screener (e.g., negative association with age, positive association with self-reported mental health problems).
Age
Our results point to weak to moderate, negative associations of the ASRS Screener score with age, consistent with research showing an age-related decline of ADHD (e.g., Faraone & Biederman, 2005; Polanczyk et al., 2007).
Gender
In our study, women displayed slightly more severe symptoms of ADHD than men. Moreover, more women than men scored above the diagnostic threshold. Some research showed results consistent with this pattern: women with ADHD experienced more intense inattention and hyperactivity symptoms than men with ADHD (Fedele et al., 2012). However, the difference between women and men in our analysis has a small effect size, which supports the hypothesis that sex-related differences in ADHD occurrence and symptom severity are less pronounced for adults than for children (Simon et al., 2009). Importantly, we observed a high occurrence of ADHD-like symptoms among gender-diverse individuals. Previous studies have shown that ADHD was more prevalent among transgender adolescents compared to age-matched individuals (A. S. Cheung et al., 2018). Transgender individuals, compared to individuals identifying as cisgender, more frequently reported having ADHD (Bretherton et al., 2021; Dawson et al., 2017). The reported estimates reached values as high as 23% for transmasculine and 26% for non-binary study participants (Leven et al., 2020). A recent systematic review concluded that evidence suggesting a higher occurrence of ADHD in transgender than cisgender individuals exists; however, the evidence is scarce and thus the authors recommended treating it cautiously (Thrower et al., 2020). This analysis, which is based on a sizable sample of gender-diverse individuals (n = 2,390) from diverse cultural backgrounds represents an important step in supplementing previously scarce evidence on this subject.
Socioeconomic Status
The evaluation of life circumstances as slightly worse by participants reporting higher ADHD symptom severity is consistent with previous studies showing that ADHD in childhood or adolescence may predict economic disadvantage and academic, occupational, and social dysfunction in adulthood (Du Rietz et al., 2017; Galéra et al., 2012; Kooij et al., 2005).
Mental Illness, Physical Illness, and Sexual Problems
The positive relationship between ADHD symptoms severity and self-reported mental illness that we observed is supported by previous research (NCCMH UK, 2009) showing adult ADHD to increase the odds of having another mental illness, for example, autism spectrum (Jensen & Steinhausen, 2015), mood, and anxiety disorders (Kessler et al., 2006). In our study, ADHD symptoms were not associated with reporting a physical illness, which is in contrast to the meta-analysis that showed co-occurrence of ADHD with asthma, sleep disorders, and obesity, as well as providing evidence for associations with migraine and celiac disease (Instanes et al., 2018). The authors point, however, to the relatively poor quality of studies and the need for large systematic studies investigating this topic, which our work helps to provide. At the same time, our study only included a single general question about experienced physical problems, and no objective measures or medical records were employed. Additionally, our results point to adult ADHD’s weak positive relation with self-reported sexual problems. This association aligns with a recent systematic review by Soldati and colleagues (2020) showing that individuals with ADHD report less sexual satisfaction and more sexual dysfunctions, but stronger sexual desire.
In summary, we have provided much needed data on adult ADHD in a multi-national context, including non-Western countries which were previously largely understudied (Fayyad et al., 2017; Gómez-Benito et al., 2019). The study had a very wide scope, as 42 countries, representing six continents and a variety of distinct cultural backgrounds, were included in the analysis. As these data had been lacking in the available literature, the current study can provide a foundation for future research in these countries, while also helping to create scientifically informed screening and diagnostic standards for adult ADHD in multiple populations. On a scientific level, the present results can help establish a more comprehensive and accurate picture of interdependencies between ADHD symptoms and various factors across countries with different cultures, which had also been a knowledge gap, especially in terms of comparing WEIRD and non-WEIRD countries (e.g., Fayyad et al., 2017; Gómez-Benito et al., 2019; Song et al., 2021).
As part of the present project, 26 different language versions of the ASRS Screener were prepared, adapted, and psychometrically examined. These versions are openly available for research and clinical use by other researchers (https://osf.io/jcz96). This allows for further scientific contributions and can facilitate assessment and diagnostic processes in clinical domains. Through providing new scientific results from diverse populations as well as making the assessment tools openly available, the current project can help propel further research on culturally-sensitive interventions for adults with ADHD. Although previous data on this subject were scarce (e.g., Thrower et al., 2020), our findings provide evidence that adult ADHD symptom severity is especially high in gender-diverse individuals. Significant attention to this group in clinical domains seems warranted (Bretherton et al., 2021; Dawson et al., 2017; Leven et al., 2020).
Limitations and Future Directions
Despite significant strengths, the limitations of the current study should be noted. General limitations associated with using ISS data (e.g., convenience sample use, cross-sectional design, online data collection) are described here https://osf.io/6kscb. Additionally, the analysis is based on self-report, with no additional assessment by a clinician; therefore, the results should be interpreted with caution. The current results should be supplemented in future research involving (1) clinical samples, (2) expert assessment by a clinician, (3) additional ADHD screening measures and a broader palette of measures for convergent and divergent validity investigation (e.g., screening measures for specific co-occurring disorders), (4) representative samples, and (5) longitudinal designs allowing for investigating test-retest reliability. The current analysis should also be replicated with other adult ADHD screening tools (e.g., Ustun et al., 2017).
Conclusions
The present work involved 42 countries and 72,627 participants to investigate cross-cultural differences in adult ADHD. The findings supported inter-cultural stability of a basic adult ADHD symptom structure, as well as the unidimensionality of the ASRS Screener and its high internal consistency and validity. Despite significant cross-national differences, a substantial number of participants in each of the analyzed countries was identified as being at-risk for adult ADHD. This includes some countries previously underrepresented in research (e.g., South Africa, Malaysia), showing the need for developing quality diagnosis, assessment, and treatment for adult ADHD worldwide, particularly in non-Western countries, for which science, assessment, and diagnosis of adult ADHD may be more underdeveloped. At the same time, we caution against the risk of overestimating adult ADHD based solely on self-report screening tools, which should be supplemented by additional information from clinical evaluations for adequate differential diagnosis and assessment of early ADHD onset. Notably, the increased risk among the minority groups like gender-diverse individuals was suggested, which supports a need for further research on adult ADHD in these individuals. As part of the current project, 26 language versions of the ASRS Screener were prepared and psychometrically examined and are freely and openly available as part of the current project documentation. Altogether, the findings of the current project can contribute to significant advancements in adult ADHD assessment standards, including among groups underrepresented in previous research.
Supplemental Material
sj-docx-1-jad-10.1177_10870547231215518 – Supplemental material for Cross-Cultural Adult ADHD Assessment in 42 Countries Using the Adult ADHD Self-Report Scale Screener
Supplemental material, sj-docx-1-jad-10.1177_10870547231215518 for Cross-Cultural Adult ADHD Assessment in 42 Countries Using the Adult ADHD Self-Report Scale Screener by Karol Lewczuk, Przemysław Marcowski, Magdalena Wizła, Mateusz Gola, Léna Nagy, Mónika Koós, Shane W. Kraus, Zsolt Demetrovics, Marc N. Potenza, Rafael Ballester-Arnal, Dominik Batthyány, Sophie Bergeron, Joël Billieux, Peer Briken, Julius Burkauskas, Georgina Cárdenas-López, Joana Carvalho, Jesús Castro-Calvo, Lijun Chen, Giacomo Ciocca, Ornella Corazza, Rita I. Csako, David P. Fernandez, Hironobu Fujiwara, Elaine F. Fernandez, Johannes Fuss, Roman Gabrhelík, Ateret Gewirtz-Meydan, Biljana Gjoneska, Joshua B. Grubbs, Hashim T. Hashim, Md. Saiful Islam, Mustafa Ismail, Martha C. Jiménez-Martínez, Tanja Jurin, Ondrej Kalina, Verena Klein, András Költő, Sang-Kyu Lee, Chung-Ying Lin, Yi-Ching Lin, Christine Lochner, Silvia López-Alvarado, Kateřina Lukavská, Percy Mayta-Tristán, Dan J. Miller, Oľga Orosová, Gábor Orosz, Sungkyunkwan University’s research team, Fernando P. Ponce, Gonzalo R. Quintana, Gabriel C. Quintero Garzola, Jano Ramos-Diaz, Kévin Rigaud, Ann Rousseau, Marco De Tubino Scanavino, Marion K. Schulmeyer, Pratap Sharan, Mami Shibata, Sheikh Shoib, Vera Sigre-Leirós, Luke Sniewski, Ognen Spasovski, Vesta Steibliene, Dan J. Stein, Banu C. Ünsal, Marie-Pier Vaillancourt-Morel, Marie Claire Van Hout and Beáta Bőthe in Journal of Attention Disorders
Footnotes
Acknowledgements
The authors would like to thank Anastasia Lucic and Natasha Zippan for their help with project administration and data collection, and Abu Bakkar Siddique, Anne-Marie Menard, Clara Marincowitz, Club Sexu, Critica, Digital Ethics Center (Skaitmeninės etikos centras), Día a Día, Ed Carty, El Siglo, Jakia Akter, Jayma Jannat Juma, Kamrun Nahar Momo, Kevin Zavaleta, Laraine Murray, L’Avenir de l’Artois, La Estrella de Panamá, La Voix du Nord, Le Parisien, Lithuanian National Radio and Television (Lietuvos nacionalinis radijas ir televizija), Mahfuzul Islam, Marjia Khan Trisha, Md. Rabiul Islam, Md. Shahariar Emon, Miriam Goodridge, Most. Mariam Jamila, Nahida Bintee Mostofa, Nargees Akter, Niamh Connolly, Rafael Goyoneche, Raiyaan Tabassum Imita, Raquel Savage, Ricardo Mendoza, Saima Fariha, SOS Orienta and Colegio de Psicólogos del Perú, Stephanie Kewley, Sumaiya Hassan, Susanne Bründl, Tamim Ikram, Telex.hu, Trisha Mallick, Tushar Ahmed Emon, Wéo, and Yasmin Benoit for their help with recruitment and data collection.
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KLe was supported by Sonatina grant awarded by National Science Centre, Poland, grant number: 2020/36/C/HS6/00005. MG was supported by National Science Centre of Poland grant number: 2021/40/Q/HS6/00219. LN was supported by the ÚNKP-22-3 New National Excellence Program of the Ministry for Culture and Innovation from the source of the National Research, Development and Innovation Fund. MK was supported by the ÚNKP-22-3 New National Excellence Program of the Ministry for Culture and Innovation from the source of the National Research, Development and Innovation Fund. SWK was supported by the Kindbridge Research Institute. ZD was supported by the Hungarian National Research, Development, and Innovation Office (Grant number: KKP126835). SB was supported by a Tier 1 Canada Research Chair. LJC was supported by the National Social Science Foundation of China (Grant No. 19BSH117). RC was supported by Auckland University of Technology, 2021 Faculty Research Development Fund. HF was supported by Grant-in-Aid for Transformative Research Areas (A) (Japan Society for The Promotion of Science, JP21H05173), Grant-in-Aid for Scientific Research (B) (Japan Society for The Promotion of Science, 21H02849), and the smoking research foundation. RG was supported by Charles University institutional support program Cooperatio-Health Sciences. JBG was supported by grants from the International Center for Responsible Gaming and the Kindbridge Research Institute. CY-L was supported by the WUN Research Development Fund (RDF) 2021. JBi and ChL received support from the WUN Research Development Fund (RDF) 2021. KLu was supported by Charles University institutional support program Cooperatio-Health Sciences. PMT was supported by Universidad Cientifica del Sur. GO was supported by the ANR grant of the Chaire Professeur Junior of Artois University and by the Strategic Dialogue and Management Scholarship (Phase 1 and 2). SURT was supported by Brain Korea 21 (BK21) program of National Research Foundation of Korea. GQG was supported by the SNI #073–2022 (SENACYT, Rep. of Panama). KR was supported by a funding from the Hauts-de-France region (France) called “Dialogue Stratégique de Gestion 2 (DSG2).” DS was supported by the South African Medical Research Council. MPVM was supported by a Research Chair from the Université du Québec à Trois-Rivières and a career award from the Fonds de recherche du Québec–Santé (FRQ-S).
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.