
Abstract
Objective:
To use a family genetic study to evaluate familial risk of obsessive compulsive disorder (OCD) and common comorbid illnesses in first-degree relatives of pediatric-onset probands with primary OCD.
Method:
One hundred and thirty youth with OCD and their 133 siblings and 241 parents and 49 pediatric controls were directly evaluated along multiple domains including psychopathology using structured diagnostic interviews and clinical corroboration.
Results:
Rates of anxiety, mood, disruptive behavior, and tic disorders were markedly elevated in the probands while rates in siblings were elevated at rates between the probands and controls. Twenty six percent of first-degree relatives had clinical OCD, 9% had chronic tics or Tourette’s disorder, and 21% met criteria for ADHD.
Conclusion:
Rates of familial transmission of OCD and common comorbid illnesses were significantly higher in our pediatric-onset probands than rates reported in the literature in relatives of those with adult-onset OCD.
Keywords
Obsessive Compulsive Disorder (OCD) affects 1% to 3% of children and adolescents (Douglass et al., 1995; Flament et al., 1988; Valleni-Basile et al., 1994; van Grootheest et al., 2005; Zohar et al., 1992) and is considered 1 of the 10 most disabling of all medical conditions, according to the World Health Organization (Murray & Lopez, 1996). Despite advances into genetics, phenomenology, diagnosis, and treatment of OCD, less is known about the patterns of familial aggregation of the disorder and its common comorbidities in pediatric-onset cases and whether this differs from patterns observed in adult-onset cases. Studies of familial risk of adult-onset OCD may not fully inform risk of relatives of affected children. Some researchers have found that OCD which begins in youth may represent a pediatric subtype of the disorder with unique clinical correlates (Conceicao do Rosario-Campos et al., 2001; D. Geller et al., 1998). It follows that genetic loading and familial aggregation of the pediatric subtype may differ from that seen in later-onset adult cases. In a systematic evaluation of the effects of age upon the clinical expression of OCD we found that pediatric OCD is associated with a unique peak of age at onset indicating a bimodal incidence of the disorder, male preponderance (D. Geller et al., 1998) and evidence of heterogeneity in that specific correlates were associated with the disorder in different age groups, supporting a hypothesis of developmental discontinuity between pediatric and adult OCD. We also reported that comorbid disorders in youth with OCD were frequent, but importantly, showed that chronological age and age at onset predicted different patterns of comorbidity and dysfunction in children and adolescents with OCD and, equally important, differed from comorbid illness patterns in adult-onset cases (Pallanti et al., 2011). Irrespective of current age, an earlier age at onset predicted increased risk for Attention Deficit Hyperactivity Disorder (ADHD), and multiple anxiety disorders. In contrast, mood and psychotic disorders were associated with chronological age, but not age at onset, and were more prevalent in older subjects. Tourette’s Disorder showed associations with both chronological age and age at onset, being more prevalent in children but remitting in adolescence. Of relevance, there is accumulating evidence that at least some comorbid disorders carry adverse consequences for greater severity of OCD, treatment resistance to standard therapies and poorer long-term outcome (D. Geller et al., 2001; D. A. Geller et al., 2003). Several investigators (D. A. Geller et al., 2003; McDougle et al., 1993) have found reduced response to standard pharmacological treatment in youth with OCD and comorbid tic or disruptive behavior disorders (Wewetzer et al., 2001) or mood disorders and positive family history of OCD (Leonard et al., 1993).
In view of the prevalence, chronicity, morbidity, impairment, and familial transmission risk associated with OCD in children (Flament et al., 1988; Piacentini et al., 2003) a better understanding of familial patterns and risk of OCD, and its frequent comorbid illnesses, in first-degree family members of affected youth will be helpful to both families and clinicians, as well as researchers who design and assess early intervention studies. Heritability estimates for OCD have varied from as low as 27% in one twin population study (Jonnal et al., 2000) to 45% to 58% in another twin pair study (Hudziak et al., 2004) while most studies are in the range of 30% to 40% (Hettema et al., 2001). In addition it has been reported that pediatric OCD is associated with greater familial and genetic risk such that it represents a more highly familial subgroup than cases of adult-onset OCD (Davis et al., 2013; Hanna et al., 2005; Nestadt et al., 2000; D. Pauls et al., 1995; Taylor, 2011; van Grootheest et al., 2005). These heritability estimates of less than 50% indicate the important contribution to the variance of OCD of non-genetic or epigenetic factors.
The aims of the original K08 study were to (1) determine if the pattern of familial aggregation differed between pediatric- and adult-onset OCD; and (2) determine if clinical correlates differed between pediatric- and adult-onset OCD. In this manuscript, we report on the first aim, using pediatric-onset data collected in this study and comparing it with published reports of adult-onset OCD. Since OCD and its most common comorbid conditions are all familial conditions (denoting a measure of genetic and shared environmental risk), (Biederman et al., 1992, 1995, 1996; Davis et al., 2013; D. L. Pauls et al., 2002) assessing the aggregation of these conditions in first-degree relatives can provide useful information about heritability and models of transmission of psychiatric disorders that are frequently comorbid in youth (D. L. Pauls et al., 1993); (Biederman et al., 1992; Faraone et al., 1998). We hypothesized that pediatric- and adult-onset OCD are the same disorder, but that the former emerges earlier due to a higher “dose” of familial and etiologic factors. This hypothesis assumes that familial causes of OCD are multifactorial and that as the number of etiologic factors in families increase, so does the risk for an earlier onset of OCD. We predicted that, compared with literature reports of relatives of adult-onset probands, relatives of pediatric-onset probands will have higher rates of both OCD and common comorbid conditions.
Methods
This family genetic study reports on a sample collected during the first author’s K08 Mentored Clinical Scientist Career Development Award (NIMH K08 MH01481) executed under the mentorship of Joseph Biederman MD. There were several aims of this study, including careful cross sectional clinical characterization of psychopathology (D. Geller et al., 2001), neuropsychological profiles (Abramovitch et al., 2021), family and psychosocial functioning, perinatal risk factors (D. Geller et al., 2008), and familial risk (D. A. Geller et al., 2007). The sample consisted of 130 children and adolescents and their 374 first-degree relatives (including 133 siblings and 241 parents). The original K08 sample was recruited primarily from the senior author’s clinical outpatient program over the course of 3 years from cases referred for assessment and care. In addition, there were recruitment efforts using advertisements in local papers, on the metro T and using flyers (all IRB-approved) specifically targeting African American and other minority participants. As Figure 1 indicates, the number recruited this way was relatively small. Our methodology has been described in detail elsewhere (D. Geller et al., 2007). In brief, pediatric probands and their pediatric siblings were evaluated using direct structured interviews with the Kiddie-SADS-E (Orvaschel & Puig-Antich, 1987) given to both child and parent independently. Findings were corroborated by both clinical assessment by the first author, who administered the CY-BOCS where appropriate (Goodman et al., 1986; Riddle et al., 1993), and a review panel to consider any discrepant diagnostic interview reports using Best Estimate procedures (Leckman et al., 1982). Psychiatric diagnoses were rated as past and/or current using full DSM IV(American Psychiatric Association, 2000) threshold criteria and severity assessed as mild, moderate, or severe. Where indicated, the fist author also administered the Yale Global Tic Severity Scale (YGTSS; Leckman et al., 1989) to quantify and corroborate any tic diagnoses. Parents and adult age siblings were interviewed with the Structured Clinical Interview for DSM-IV (SCID; Spitzer et al., 1992) with additional modules from the KSADS-E to assess childhood diagnoses not included in the SCID. No ethnic or racial group was excluded from this study and efforts were made to over-sample minorities. The study was approved by the MGH/McLean IRB. Age at onset was determined by careful clinical history from parents regarding age at which symptoms first appeared and, for diagnostic purposes, age at which symptoms were first deemed clinical impairing using the DSM criteria of (1) time occupied ≥1 hour, (2) subjective distress, and (3) functional difficulties in at least one important domain of life functioning.
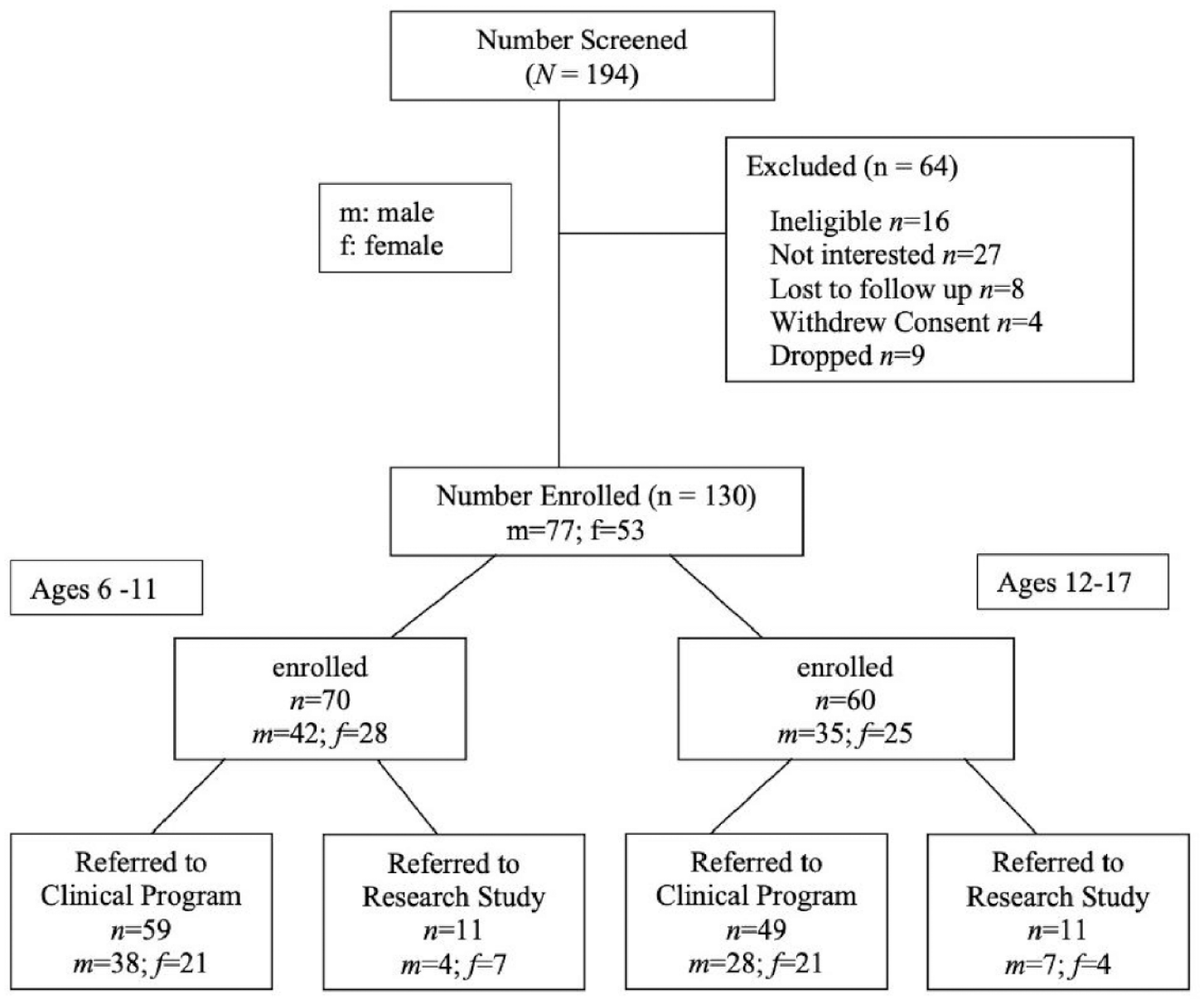
Enrollment chart. Clinical program participants were recruited from the last author’s outpatient clinic, “research” referrals refers to those recruited from disseminated advertising efforts.
A contemporaneous family case-control study of DSM-III-R ADHD that employed identical evaluation methods provided controls (Biederman et al., 1996). Siblings of controls from that study, who had neither ADHD nor OCD were randomly selected as gender and age matched controls for this study.
We addressed several issues relevant to the analysis of family and outcome studies of psychiatric illness: (1) the appropriate statistical model, (2) the non-independence of observations within families due to cultural and/or genetic factors, (3) statistically controlling for the effects of potentially confounding variables, and (4) the potential for referral biases to produce spurious evidence for comorbidity. Our hypotheses were framed within the context of a general linear model using hypothesized predictor variables to predict specific outcomes. We modeled binary data with logistic regression and ordinal data with ordinal logistic regression. Data collected from subjects in the same family is not statistically independent for cultural or genetic reasons. The problem of nonindependence was handled within the general linear model framework by applying Huber’s (1967) formula as implemented in STATA (Stata Corporation, 1992) to produce robust statistical tests for clustered data. We used regression for all analyses, where group status was the dependent variable, and the diagnosis outcome measure was the independent variable. In two instances group comparisons contained cells with 100% and the logistic regression would not converge. Here we used chi-squared tests. All tests were two-tailed and statistical significance was set at a probability of .05. All pediatric subjects (probands and siblings) provided assent while parents provided consent for all youth. The study was approved by the McLean hospital IRB.
Results
One hundred and thirty children and adolescents were enrolled after screening 194 youth (Figure 1).
We also evaluated 133 of 165 total siblings and 241 parents. A breakdown of the proband sample by age and gender is shown in Figure 2 (range 6–17 years) and baseline characteristics are shown in Table 1. In the K08 sample there were one Asian and two mixed Asian/White subjects and three Hispanic families.
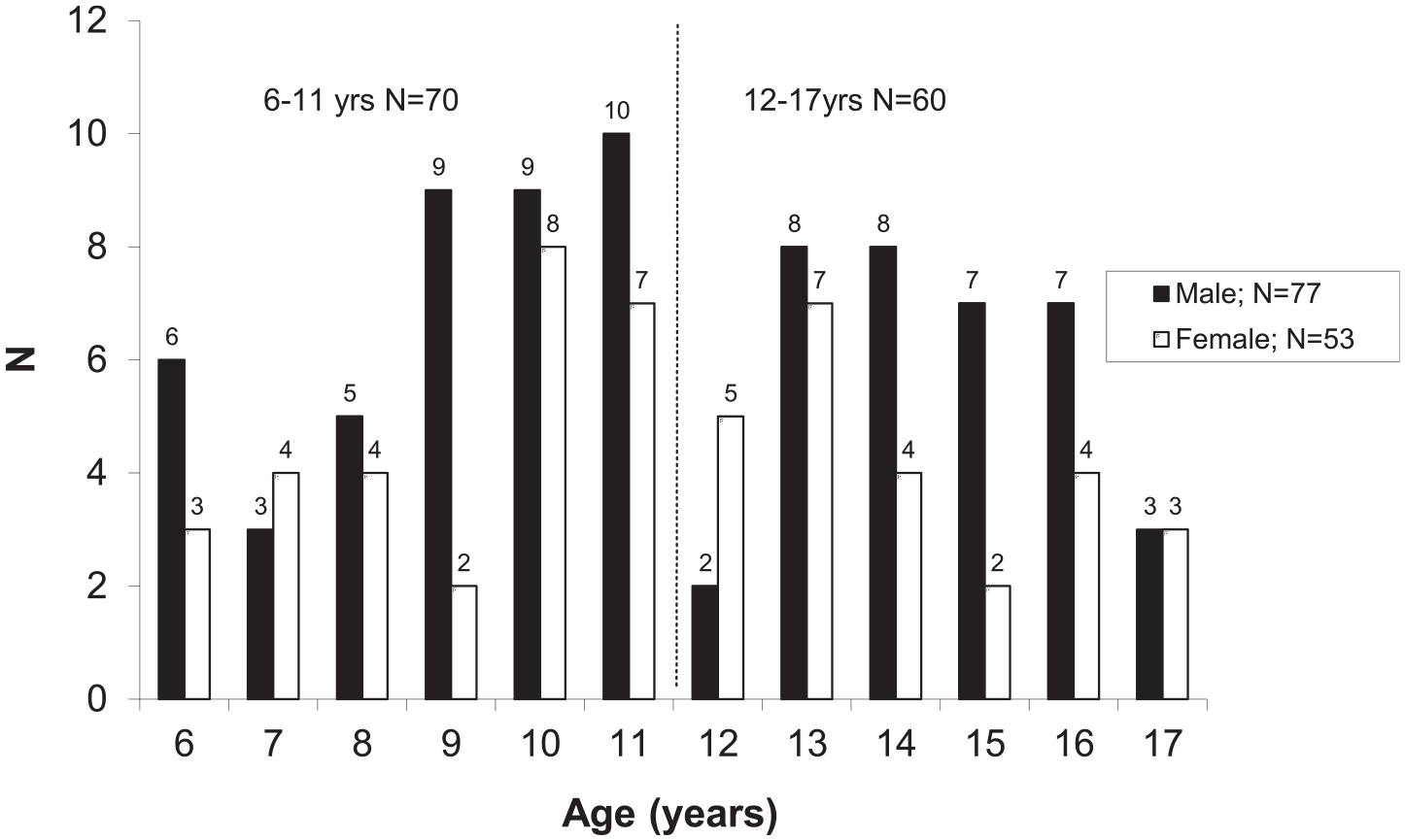
Age and gender of OCD probands.
Pediatric OCD Cohort, All Proband, Sibling, and Matched Control Characteristics at Baseline.
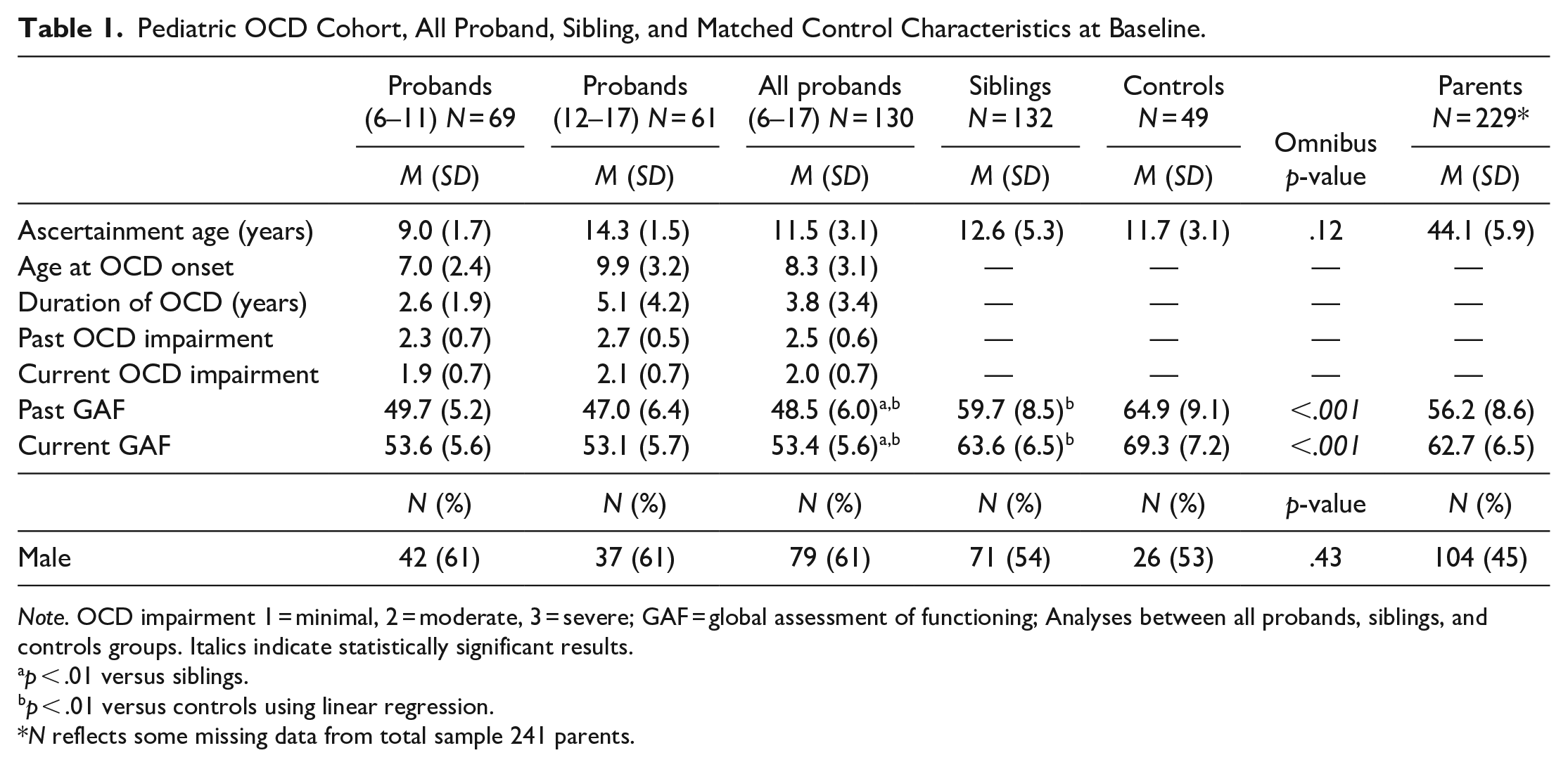
Note. OCD impairment 1 = minimal, 2 = moderate, 3 = severe; GAF = global assessment of functioning; Analyses between all probands, siblings, and controls groups. Italics indicate statistically significant results.
p < .01 versus siblings.
p < .01 versus controls using linear regression.
N reflects some missing data from total sample 241 parents.
Comorbid disorders were highly prevalent. Table 2 shows frequency in probands, siblings, controls, and parents while regression analyses compare the pediatric groups only without parents. Overall, 98% of our sample had at least one comorbid diagnosis, 80% met criteria for at least one other anxiety disorder, 42% had DSM IV ADHD, 39% had chronic tics or Tourette’s syndrome, and 51% had major depressive disorder. Many had multiple disorders. There were highly significant differences between the probands, their siblings, and controls in rates of psychiatric disorders, especially anxiety, disruptive behavior, chronic tic, and mood disorders. In general siblings’ rates were elevated and intermediate between probands and controls. Despite having ASD diagnosis as an exclusion criterion at screening, 7% still met criteria for this at structured diagnostic interview when corroborated clinically by the first author. With the exception of major depression, comorbidity was not associated with the total or sub-scores on the CY-BOCS scale (p = .57) or OCD-specific impairment (p = .96) but was associated with a lower GAF (p = .02). However, comorbid major depression was associated with greater OCD-specific impairment (p = .02), higher CY-BOCS scores (p = .05), more frequent psychiatric hospitalization (p < .001), and lower GAF scores (p < .001).
Frequency of Comorbid Disorders in Probands, Siblings, Controls, and Parents With Regression Analyses Comparing Pediatric Groups Only Without Parents.

p < .05 versus siblings.
p < .01 versus siblings.
p < .05 versus controls.
p < .01 versus controls.
p-values derived from logistic regression; If sample included zero, Fisher’s exact test was used. Italics indicate statistically significant values.
Only 10% of the adolescents had not received any treatment at enrollment compared with 27% of children and 46% of siblings. Half the children and most of the adolescents had received SSRIs but far fewer had received CBT as their only treatment and less than half had received combined SSRI and CBT treatment considered the most effective intervention clinically (March, 2003). A substantial number had received treatment with multiple medications; one third of children and two thirds of adolescents. Twenty percent of adolescents and 9% of children had been hospitalized by the time of ascertainment despite their young age. Findings from neuropsychological assessments have been published elsewhere (Abramovitch et al., 2021; D. A. Geller et al., 2018).
Nineteen (8%) parents and 29 (22%) siblings had a full DSM IV diagnosis of OCD representing first-degree relatives of 39 (30%) probands. A further 9 siblings and 22 parents had subthreshold OCD symptoms (definitely present but not meeting threshold criteria for full diagnosis, based upon time occupied, distress, and impairment). Four families had more than one affected sibling, two families had both an affected parent and sibling while one family had two affected parents. Rates of comorbid illness in first-degree relative are shown in Table 3.
Age Corrected Risk for OCD, TS, Chronic Tics, and ADHD in First-degree Relatives of Pediatric OCD Probands.
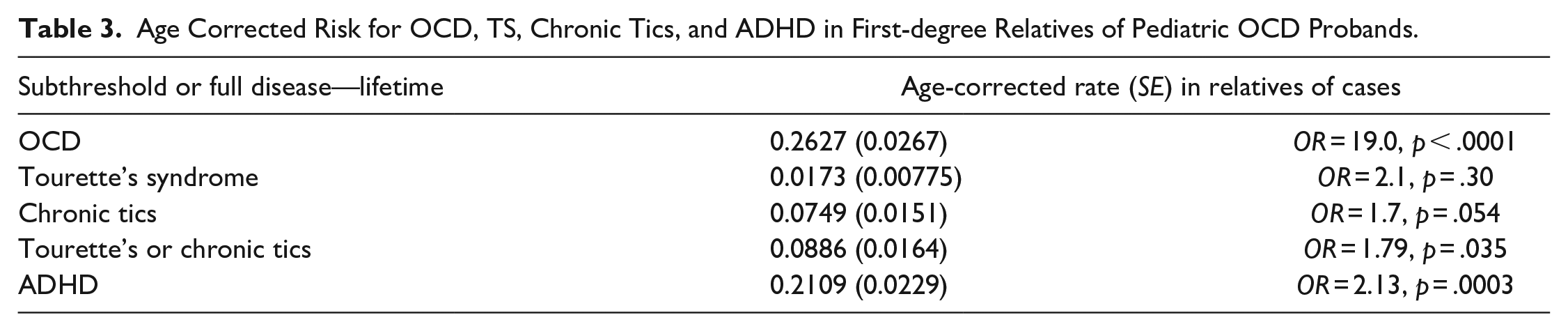
Age-corrected morbid risk for comorbid illnesses in relatives is seen in Table 3 with odds ratios expressing relative risk compared to expected population prevalence. Notably, 26% of relatives had a clinical diagnosis of OCD, a rate twice as high as that reported in familial samples of adult cases (Mattheisen et al., 2015), confirming the increased transmission risk from early-onset illness. A further 1.7% of first-degree relatives met criteria for Tourette’s syndrome and 7.5% for chronic tic disorders, considered phenotypically and genetically similar (Claudio-Campos et al., 2021) with a combined risk of 9%. Fully 21% of relatives met diagnostic criteria for ADHD, a rate greatly elevated above the expected population prevalence (Polanczyk et al., 2014).
Discussion
To our knowledge, this study represents the largest sample of pediatric OCD probands assessed in a cross-sectional study using thorough and well-validated methodology, including direct evaluations employing structured diagnostic interviews and corroborating clinical assessments of all subjects. Studies such as this, here including 130 probands, 133 siblings, and 241 parents, are rare, and have laid the foundation for much of what is accepted as core knowledge of pediatric OCD. In addition to careful characterization of these affected youth, direct assessment of first-degree relatives enabled careful documentation of familial risk of OCD and comorbid illnesses with a high degree of confidence.
The great majority of our probands had a prepubertal onset of OCD, were male, and had at least moderate functional impairment. They displayed high rates of non-OCD anxiety, mood, disruptive behavior, and tic disorders at highly statistically significant rates, well beyond the expected population prevalence and rates seen in control group. Age-corrected risk, taking into account periods of peak risk for onset of OCD and comorbid illnesses, showed markedly elevated risk in both parents and siblings for OCD. The risk for siblings to develop OCD is about 1 in 4 or 25%, a rate more than twice as high as published risk data for family members of those with OCD that onsets in adult years (Nestadt et al., 2000).
Some unexpected findings emerged regarding comorbidity in affected relatives for conditions more commonly seen in children and adolescents, that is, chronic tic disorders, Tourette’s disorder, and ADHD. Chronic tics and Tourette’s are often considered phenomenologically similar (Claudio-Campos et al., 2021) and although chronic tics and Tourette’s disorder typically remit in the second decade of life, our siblings and parents had a combined rate of almost 9% with a significantly elevated odds ratio over the expected population prevalence. Even more compelling was our finding of markedly elevated rates of ADHD in both siblings and parents. At the time of this study, ADHD remained an under-recognized and under diagnosed condition in adults.
Familial risk analysis methodology permitted examination of the relationship between ADHD and OCD in comorbidly affected children since it might be assumed that ADHD-like symptoms are merely an artefact of intrusive anxiety-provoking thoughts in youth with OCD. By comparing the actual aggregation of ADHD and OCD in relatives to patterns predicted by different models of transmission (D. L. Pauls et al., 1986), we elucidated the relationship between these conditions. Our results on familial risk for ADHD in an OCD proband sample yielded results consistent with co-segregation as reported in Geller et al. 2007 (D. Geller et al., 2007; D. A. Geller et al., 2007).
One limitation is that most of the sample was clinically referred, and since it might be assumed that patients seeking care in a specialized clinical setting are likely to have more than one diagnosis (Berkson’s bias; Berkson, 1946), we do not know whether our findings generalize to non-referred samples. However, we have previously shown that they do resemble other clinical samples (D. Geller et al., 2000). Another limitation is that, despite efforts to recruit minority participants, our sample was almost entirely white and non-Hispanic. In summary, the familial risk in first-degree relatives of youth with OCD is higher than that seen in adult-onset cases and brings added risk for commonly observed comorbid illnesses typically seen in the pediatric years but not in adults. Family genetic study methodology enables investigators to disentangle the confounds of complex comorbid psychopathology in affected probands and document familial transmission risks with a high degree of confidence.
Footnotes
Acknowledgements
Joe Biederman changed the world. When I met him in 1992, I had never written or published a manuscript. For a decade we would meet early every Monday morning to develop and write papers and grants. As a consequence, Sunday evenings were miserable as I prepared for these meetings. Joe would generally delete most of what I had written, even (what I thought were) well-crafted sentences. He taught me to think and write like a clinical scientist. Unfailingly brilliant, kind, and generous with his time, he propelled a whole generation of clinical researchers. We are ever grateful.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: financial support for the research used in this article from Dr. Daniel Geller’s KO8 grant (1K08MH01481-01A) from the National Institute of Mental Health.