
Abstract
Objective:
Several studies have shown that Adult ADHD presents differently in younger and older adults. We sought to assess the difference in care between these two groups using previously identified quality measures (QMs).
Methods:
Using electronic health record data, we matched a younger group of ADHD patients to an older group. We then assessed the achievement of the QMs using probit models with and without interaction terms.
Results:
The majority of QMs shown an increase in achievement for both groups over time. However, significant differences in quality of care between younger and older adult ADHD patients persisted. By the end of the study period, with the exception of three QMs, younger patients achieved the QMs more.
Conclusion:
While, in general, the quality of care for adult ADHD increased from 2010 to 2020, there were still differences in care between younger and older adult ADHD patients.
Introduction
Adult ADHD has an estimated epidemiological prevalence of 2.5% to 2.8% (Faraone et al., 2006; Fayyad et al., 2017; Simon et al., 2009) as compared to ADHD in youths with an estimated epidemiological prevalence of 5.9% (Willcutt, 2012). The administrative prevalence of adult ADHD has continued to steadily climb in recent years with clinicians becoming more comfortable with the diagnostic criteria and more recognitive of the disorder (Chung et al., 2019; Dobson-Patterson et al., 2016; London & Landes, 2021). While there are clinical differences between childhood ADHD and adults ADHD (Kasparek et al., 2015; Kessler et al., 2010; Martel et al., 2012; Moffitt et al., 2015), several studies have shown differences in adult ADHD in younger adults and in older adults (Durell et al., 2010; Lensing et al., 2015; Manor et al., 2011; Michielsen et al., 2015; Sasaki et al., 2022; Semeijn et al., 2016; Sibley, 2021a; Surman & Goodman, 2017; Thorell et al., 2019). Recent studies are also showing that it may be necessary to have different criteria for younger adults and older adults when diagnosing and treating ADHD (Surman & Goodman, 2017). ADHD manifestations could change with age (Callahan & Plamondon, 2019; Manor et al., 2011; Semeijn et al., 2016; Surman & Goodman, 2017; Thorell et al., 2019); co-existing diagnoses (e.g., cognition/dementia,(Callahan & Plamondon, 2019; L et al., 2022; Sasaki et al., 2022; Sprafkin et al., 2007; Surman & Goodman, 2017); differences in support structure (Michielsen et al., 2015; Surman & Goodman, 2017); and quality of life (Lensing et al., 2015; Thorell et al., 2019). Adults with ADHD, particularly older adults, also tend to have problems with unemployment (L et al., 2022; Young & Goodman, 2016), financial issues (Michielsen et al., 2015; Young & Goodman, 2016), and personal/social relationships (Michielsen et al., 2015; Young & Goodman, 2016).
One study indicated that the DSM diagnostic criteria between younger and older adults should be relatively similar, but that the threshold for meeting an ADHD diagnosis should be lower for older adults (Surman & Goodman, 2017), while another study called for age-appropriate criteria based on screening from the Conners Adult ADHD Rating Scale (Callahan & Plamondon, 2019). However, a third study indicated diagnostic criteria can be the same for younger and older adults based on a longitudinal aging study (Semeijn et al., 2016). Additional literature have also called for dual diagnosis treatment criteria (e.g., ADHD and substance use disorder or ADHD and Autism Spectrum Disorder; (Matthys et al., 2014; Posserud et al., 2021)) and additional monitoring of older adults for potential comorbid factors (e.g., cardiovascular issues; (Michielsen et al., 2021)).
In this paper, we discuss results from a secondary data analysis of Electronic Health Record (EHR) data of adult ADHD patients. We focus on differences in age, while matched on other demographic variables, in ten quality measures (QMs) previously identified in Faraone et al. (Faraone et al., 2019). These ten QMs focus on necessary components of care for adults with ADHD and we looked for differences in how clinicians instituted these ten QMs into clinical practice from 2010 to 2020.
Methods
Dataset Overview and Creation
Data used in this analysis were obtained from DARTNet Institute’s Practice Performance Registry (PPR). The PPR has been standardized to the Observational Medical Outcomes Partnership Common Data Model v6 (OMOP CDM v6; (Barton Pai et al., 2020; Ratigan et al., 2021)). The data contained four million de-identified patient records from across the United States and covered demographics, diagnosis codes, procedure codes, measurements, observations, and medications for all patients and covered all patients’ historical data (up to 15 years back) through December 2020. Dates of services were masked ±30 days with the spacing between dates preserved.
For dataset creation of the analysis files, three authors (EC, TC, and JA) worked with an external consultant (small number of meetings), SF (definition refinement), and DARTNet Institute (clarification of variables) to refine definitions used for dataset creation. After refinement, EC, JA, and TC finalized all necessary definitions and generated a list of codes needed to create the definitions from the Electronic Health Record (EHR) data. The definitions were expressed using 498 created value sets with almost 700,000 codes and had repeated data quality checks performed against them. These value sets were pulled from the PPR data and combined to create the QM definitions needed for analysis. Finally, each patient needed to be assigned to a home clinic. For the purposes of this analysis, a patient’s “home clinic” was the last primary care clinic they were seen in within the dataset. The datasets were created using SAS 9.4 (Cary, NC). Full definitions for all QMs are located in Callen et al. (2023).
Matching
We defined older and younger patients as: 1930s to 1960s (older; 50+ years old) and 1970s to 2000s (younger; Lensing et al., 2015; Sibley, 2021a; Surman & Goodman, 2017). We used 1:1 matching using genetic matching with exact matching turned on and without replacement (Ho et al., 2007, 2011). We matched based on gender, race, ethnicity, practice type, and organization ownership. Genetic matching uses propensity scores calculated with Mahalanobis distance with nearest neighbor (Ho et al., 2011). The genetic matching was completed using R 4.2.0 (Vigorous Calisthenics) with the MatchIt package (v042.8.1; (Ho et al., 2007)).
Statistical Analyses
The analyses documented here were completed only on the matched data. Descriptive statistics were calculated for demographic variables and for the graphics (counts and percentages). A series of probit models determined the effect of age on the achievement of the QMs (with the Wald statistic reported), after accounting for exact genetic matching. All probit models covered the years 2010 through 2020. Interaction terms (year × age) were included in probit models when significant. A two-sided alpha of 0.05 was used. The analyses were completed using SPSS 27 (Armonk, NY, USA).
Results
After matching, the sample had 17,887 patients diagnosed with ADHD in both groups (1930s–1960s [older]; 1970s–2000s [younger]). The sample was majority white (74.9%), not Hispanic or Latinx (71.2%), female (62.4%), and from a primary care office (70.0%; Table 1). When comparing the two groups in the number of QMs met in each year of analysis (2010–2020), younger patients achieved more QMs than older patients (χ2(1) = 992.897; p < .001). As an example, in 2020, the dark blue area of the stacked bar chart (Figure 1) is smaller in the younger group than in the older group indicating that fewer younger patients met no QMs than the older patients. The following QMs are the nine measures and results for each by age group. The first QM is not included due to issues with finding the necessary information in the EHR (Callen et al., 2023).
Demographics.
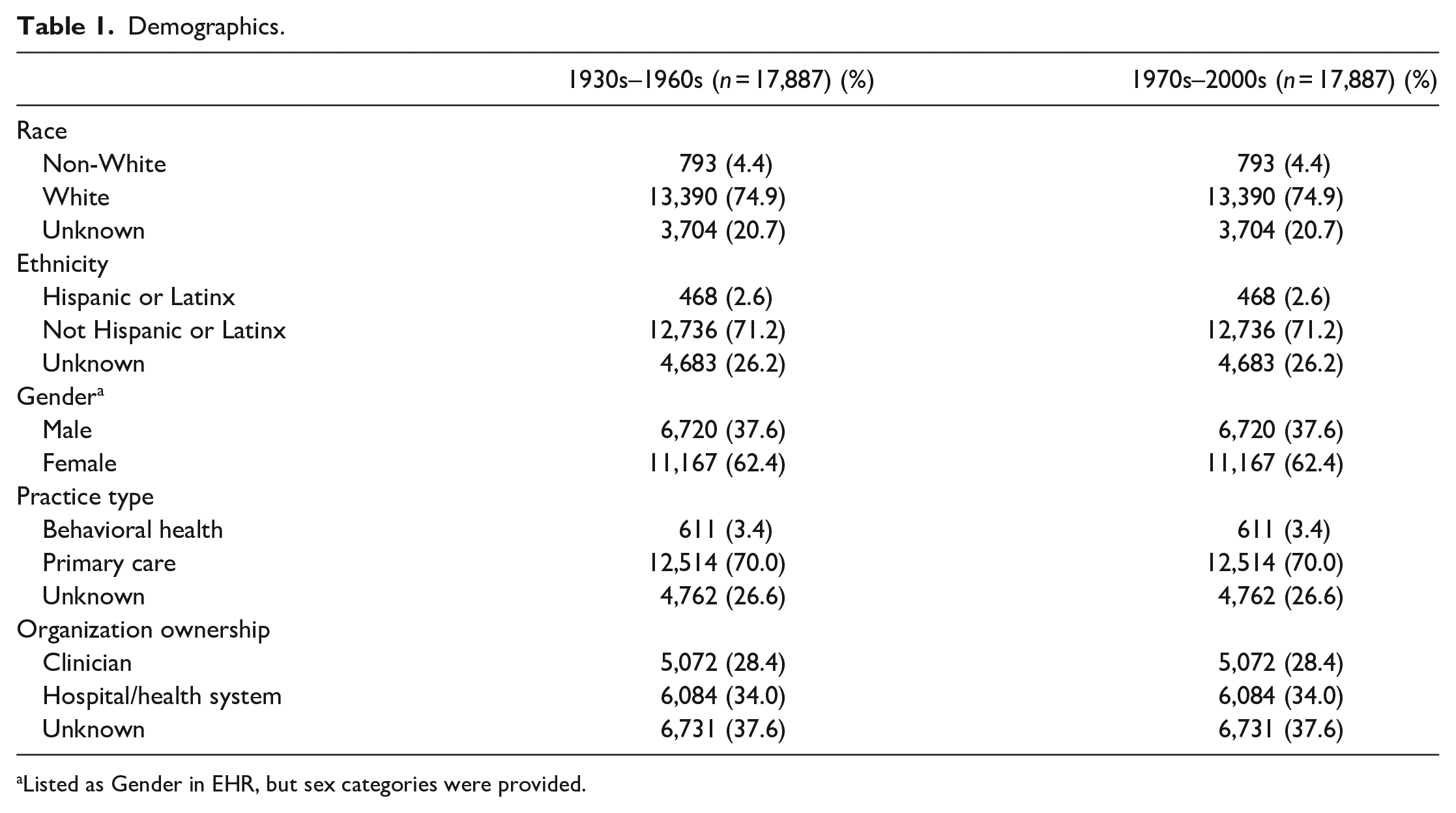
Listed as Gender in EHR, but sex categories were provided.
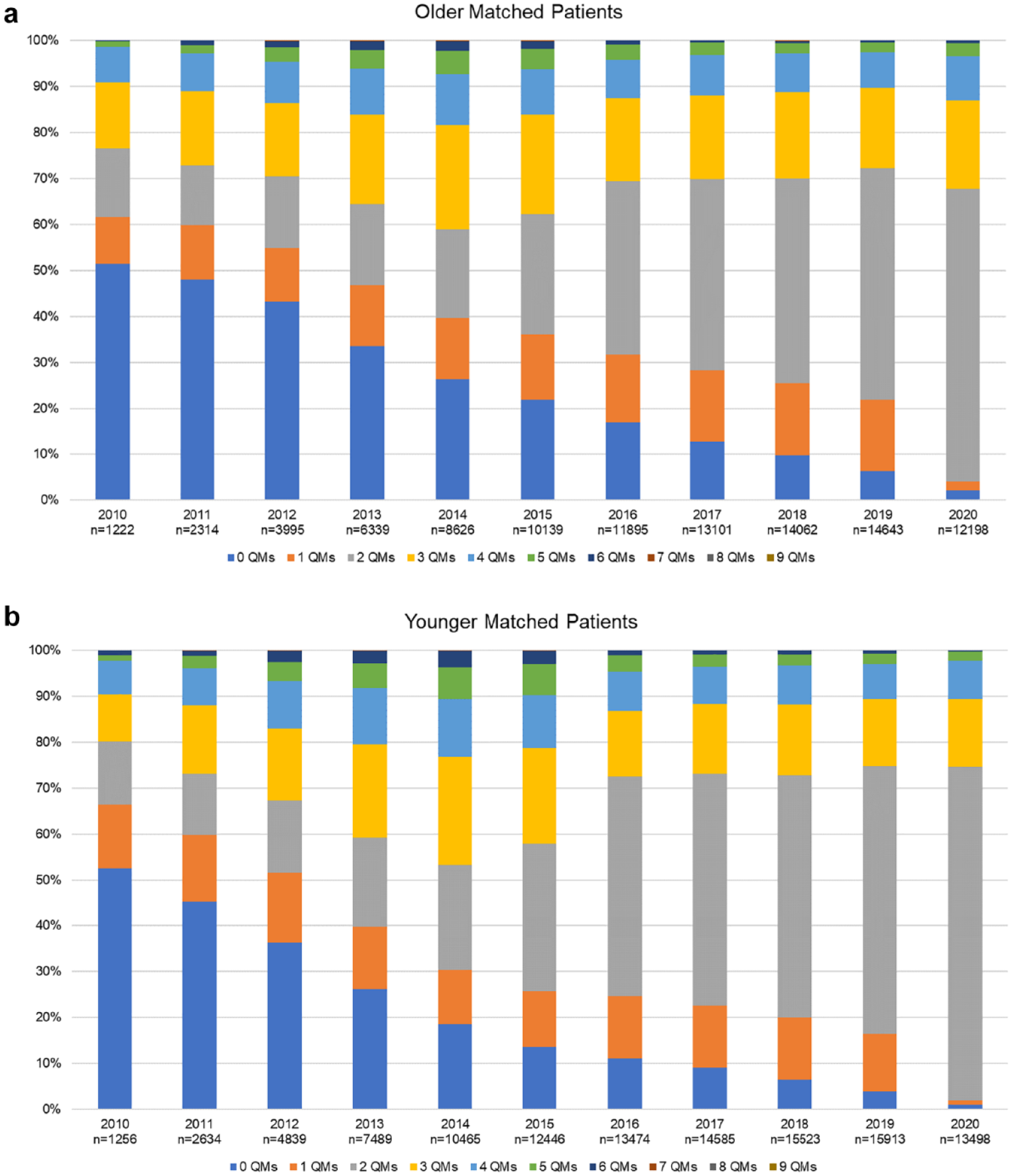
Achievement of adult ADHD quality measures from 2010 through 2020: (a) patients born in 1930s to 1960s (older matched patients) and (b) patients born in 1970s to 2000s (younger matched patients).
QM2: Percent Patients Treated for ADHD Having Documented DSM-5 Diagnosis of ADHD
The general trend for both age groups between 2010 and 2020 was upward with almost all patients meeting this QM by 2020. While the older group had, generally, lower achievement rates of this QM than the younger group, by 2020, the difference had almost disappeared (Figure 2a). This interaction of year with age was statistically significant (W(1) = 16.5; p < .001). The odds of achieving the QM increased each year (1.2 times greater each year; W(1) = 1,290.5; p < .001) and the younger group had higher odds (1.6) of achieving the QM than the older group, but the difference in achievement between the two groups is small by 2020.

Trends of individual adult ADHD quality measures from 2010 through 2020 (blue: matched patients born in 1930s–1960s; orange: matched patients born in 1970s–2000s). (a) percent patients treated for ADHD having documented DSM-5 diagnosis of ADHD, (b) percent patients with ADHD with review of other psychiatric disorders, (c) percent patients with ADHD with documentation of impairment, (d) percent patients receiving ADHD medications for whom treatment alternatives, benefits, and risks have been discussed, (e) percent patients with ADHD assessed for vitals prior to medication treatment, and (f) percent patients with ADHD for whom warnings and contraindications for medication were reviewed.
QM3: Percent Patients With ADHD With Review of Other Psychiatric Disorders
Starting in 2013, both age groups achieved this QM at very similar rates and the trend plateaus at almost 100% of patients achieving the QM. Before 2014, the older group achieved this QM at a higher rate than the younger group with an upward trend for both groups (Figure 2b). This interaction of year with age was statistically significant (W(1) = 255.9; p < .001). The odds of achieving the QM increased each year (1.1 times greater each year; W(1) = 2,919.7; p < .001) and the younger group had higher odds (1.1) of achieving the QM than the older group (W(1) = 90.7; p < .001)
QM4: Percent Patients With ADHD With Documentation of Impairment
Over the 11-year period, both groups saw an increase in QM achievement from less than 50% to almost 100%. At the start, the older group had higher achievement in the QM, but in 2012 the groups had similar achievements. This interaction of year with age was statistically significant (W(1) = 131.6; p < .001). After 2012, the younger group had higher achievement in the QM than the older group (Figure 2c). The odds of achieving the QM increased each year (1.2 times greater each year; W(1) = 19,829.3; p < .001) and the younger group had higher odds (1.2) of achieving the QM than the older group (W(1) = 634.2; p < 0.001).
QM5: Percent Patients Receiving ADHD Medications for Whom Treatment Alternatives, Benefits, and Risks Have Been Discussed
From 2010 through 2014, the QM achievement had an upward trend with after 2014 the trend plateaued. The two age groups had very similar QM achievements throughout the 11-year period, but these small differences were statistically significant (Figure 2d; W(1) = 8.3; p = .004). The odds of achieving the QM increased each year (1.2 times greater each year; W(1) = 228.7; p < .001) and there was no difference in the achievement of the QM between groups.
QM6: Percent Patients With ADHD Assessed for Vitals Prior to Medication Treatment
The achievement of this QM was generally low with no year greater than 50% of patients achieving this QM for either group (Figure 2e). The odds of achieving the QM increased each year (1.1 times greater each year; W(1) = 9.4; p = .002) and the younger group had higher odds (1.1; W(1) = 35.9; p < .001) of achieving the QM than the older group. The trajectory of QM achievements over the 11-year period did not differ between groups (W(1) = 1.1; p = .298).
QM7: Percent Patients With ADHD for Whom Warnings and Contraindications for Medication Were Reviewed
There is trend for either age group for this QM with achievements fluctuating widely from year to year (Figure 2f). The main effect of group was not significant (W(1) = 0.0; p = .954) and there were no significant changes over time The main effect of group was not significant (W(1) = 2.7; p = .102) or differences between groups (W(1) = 2.1; p = .150). The interaction between age and year was not statistically significant (W(1) = 0.2; p = .653).
QM8: Percent Patients With ADHD Where Validated Measure of Symptom Change Used to Assess Treatment Efficacy at Least Annually
For both groups, this QM had very high levels of achievement through the 11-year period. While there was a slight downward term over time, by 2020, both age groups still had a greater than 85% achievement for this QM (Figure 2g). The odds of achieving the QM decreased each year (1.1 times less each year; W(1) = 1,070.8; p < .001) and the older group had higher odds (1.1; W(1) = 28.1; p < .001) of achieving the QM than the younger group. The interaction between age and year was statistically significant (W(1) = 4.8; p = .029).
QM9: Percent Patients Stabilized on an ADHD Medication Seen at Least Once per Year
There is an upward trend in QM achievement for both age groups until 2015, at which point the QM achievement drops off, rises slightly again, and the plateaus. These small differences in trajectories were, however, statistically significant (W(1) = 11.3; p < .001). Both age groups are similar through the entire 11-year period following the same rises and dips (Figure 2h). The odds of achieving the QM increased each year (1.1 times greater each year; W(1) = 261.6; p < .001) and the younger group had higher odds (1.1) of achieving the QM than the older group (W(1) = 12.1; p < .001).
QM10: Percent Patients Prescribed Medication for ADHD Seen Within 1 Month of Initial Prescription
There is an upward trend in QM achievement for both groups until 2015 where the younger group has a higher QM achievement than the older group. Throughout the remainder of the 11-year period, the younger group plateaued while the older group saw a decrease in QM achievement (Figure 2i). These small differences in trajectories were, however, statistically significant (W(1) = 57.4; p < .001). The odds of achieving the QM increased each year (1.1 times greater each year; W(1) = 513.4; p < .001) and the younger group had higher odds (1.2) of achieving the QM than the older group (W(1) = 50.1; p < .001).
Discussion
This study showed that, in general, younger patients achieve more QMs than older patients, potentially indicating better care for their ADHD or a difference in attitudes and beliefs toward ADHD in different age groups. It could also be an indication of the differences potentially needed in treating their ADHD due to changes in manifestation over time as seen in other studies (Callahan & Plamondon, 2019; Lensing et al., 2015; Michielsen et al., 2015; Sasaki et al., 2022; Semeijn et al., 2016; Surman & Goodman, 2017; Thorell et al., 2019) as well as the need for validation of the ADHD diagnosis via structured clinical means in older adults (Goodman et al., 2016; Semeijn et al., 2013; Sharma et al., 2021; Sibley, 2021b; Surman & Goodman, 2017). Younger patients were more likely to be treated after having a documented DSM-5 diagnosis of ADHD, which is consistent with previous findings (Hechtman et al., 2011; Ramtekkar et al., 2010). While prior studies have indicated that all adults with ADHD should be screened for other psychiatric disorders (Anker et al., 2017; Barkley & Brown, 2008; Choi et al., 2022; Holst & Thorell, 2017, 2020; Sobanski, 2006), we found that younger adults were screened at a higher rate than older adults. It is difficult to explain this discrepancy. There are several possible explanations: inadequate clinical education on comorbid psychiatric assessment in older adults (Goodman, 2009; Goodman & Thase, 2009; Weisler & Goodman, 2008), medical illnesses in older adults may consume clinicians’ time not allowing for comprehensive psychiatric assessment (Adelman et al., 2000; Herndon et al., 1997), assumption that the likelihood of undetected mental health disorders is negatively correlated with duration/age (Buitelaar & Ferdinand, 2013; Chen et al., 2018; Soegaard, 2012), and ageism bias dismissing psychiatry symptoms in older adults (Asherson et al., 2012; Officer et al., 2016; Ribeiro-Goncalves et al., 2023; Temple et al., 2021). Previous studies also indicate that impairments related to ADHD (e.g., financial issues, unemployment, and social structure) can change with age (Anker et al., 2017; Brown et al., 2017; Holst & Thorell, 2020; L et al., 2022; Lensing et al., 2015; Michielsen et al., 2015), which could be related to our findings in that younger patients and older patients had different levels of documented impairment related to their ADHD.
The three visit related QMs (percent patients with ADHD assessed for vitals prior to medication treatment; percent patients stabilized on an ADHD medication seen at least once per year; percent patients prescribed medication for ADHD seen within one month of initial prescription) were more achievable for younger patients than for older patients, indicating a difference in the clinical approach to ADHD. Since these QMs also focus on medication treatment, these do not focus on the difference in younger patients and older patients receiving medication but how their medication is managed within their practices. This is somewhat consistent with previous studies in that how older patients’ ADHD are managed is different than for younger patients (Durell et al., 2010; Lensing et al., 2015; Manor et al., 2011; Michielsen et al., 2015; Sasaki et al., 2022; Semeijn et al., 2016; Sibley, 2021a; Surman & Goodman, 2017; Thorell et al., 2019).
One QM was more achievable for older patients than for younger patients—percent patients with ADHD where validated measure of symptom change used to assess treatment efficacy at least annually. This difference could arise in differences in quality of life between the groups or competing diagnoses that require other assessments, due to concerns over the validity of diagnosis in older adults or concerns over the use of medication in older adults, which is consistent with preceding studies (Callahan & Plamondon, 2019; Durell et al., 2010; Lensing et al., 2015; Michielsen et al., 2021; Semeijn et al., 2016; Surman & Goodman, 2017; Thorell et al., 2019).
Overall, for eight of the nine QMs detailed here, the general trend was upward over the 11-year period for both younger and older patients. One QM, percent patients with ADHD where validated measure of symptom changed used to assess treatment efficacy at least annually, did decrease over the time period analyzed. The increase in QM achievement could indicate a better understanding of adult ADHD among the practices included in this dataset.
Finally, while it is encouraging that clinical utilization of QMs increased over the 11 years, the noted differences between younger and older adults with ADHD merits increased attention to improving clinical oversight of older adults with ADHD through enhanced educational efforts for clinicians. Older patients were, in general, monitored less than younger patients, which is contrary to concerns about greater medical illness and comorbidities in the older cohort.
Limitations
EHR data can have several limitations. Since we received a de-identified dataset, we did not receive clinical notes, which could have improved the QM achievement. All the QM achievements are based off what is documented with codes (e.g., ICD-10, ICD-9, and SNOMED) within the EHR. However, the codes were applied consistently over the entire dataset, so if a note was not coded in one practice, it also was not coded in any other practice. The EHR data can also contain gaps due to changes in EHR systems, non-reporting for activities, and the location of the necessary data within the EHR (e.g., vital signs).
Footnotes
Author Note
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Over the past 3 years, Dr. Callen received research support from PCORI, Merck, NIH, AAFP Foundation, Otsuka, Takeda, UnitedHealth Foundation, HRSA, GlaxoSmithKline, SAMHSA, Eli Lilly, CDC, Helmsley Foundation, and VaxCare. Over the past 3 years, Ms. Clay received research support from NIH, Otsuka, Takeda, UnitedHealth Foundation, HRSA, SAMHSA, Eli Lilly, and AAFP Foundation. Over the past 3 years, Ms. Alai received research support from PCORI, Abbott, Eli Lilly, and Otsuka. Over the past 3 years, Dr. Goodman received honoraria, consulting income, potential income, or travel expenses from Tris, Otsuka, Ironshore, Supernus, Sunovion, Noven, Shionogi, Ondosis, Medscape, HCPlive, Clinical Care Solutions, National Football League, WebMD, and the Neuroscience Education Institute. Over the past 3 years Dr. Adler is a consultant for Takeda, Otsuka, Bracket/Signant, Major League Baseball, the National Football League, and the State University of New York; receives grants from Takeda and Otsuka; and royalty payments from New York University School of Medicine for scales and training material for adult attention-deficit/hyperactivity disorders. Over the past 3 years, Mr. Shields received research support from PCORI, Merck, Humana, NIH, and AAFP Foundation. Over the past 3 years, Dr. Faraone received income, potential income, travel expenses continuing education support and/or research support from Aardvark, Aardwolf, AIMH, Tris, Otsuka, Ironshore, Kanjo, Johnson & Johnson/Kenvue, KemPharm/Corium, Akili, Supernus, Atentiv, Noven, Sky Therapeutics, Axsome, Genomind, Shire/Takeda, Arbor, Medice, Ondosis, Rhodes, and Vallon. With his institution, he has US patent US20130217707 A1 for the use of sodium-hydrogen exchange inhibitors in the treatment of ADHD. He also receives royalties from books published by Guilford Press: Straight Talk about Your Child’s Mental Health; Oxford University Press: Schizophrenia: The Facts; and Elsevier: ADHD: Non-Pharmacologic Interventions. He is Program Director of www.ADHDEvidence.org and ![]() . Dr. Faraone is supported by the European Union’s Horizon 2020 research and innovation programme under grant agreement No 965381; NIMH grants U01AR076092-01A1, 1R21MH1264940, R01MH116037; 1R01NS128535—01; Oregon Health and Science University, Otsuka Pharmaceuticals, Noven Pharmaceuticals Incorporated, and Supernus Pharmaceutical Company.
. Dr. Faraone is supported by the European Union’s Horizon 2020 research and innovation programme under grant agreement No 965381; NIMH grants U01AR076092-01A1, 1R21MH1264940, R01MH116037; 1R01NS128535—01; Oregon Health and Science University, Otsuka Pharmaceuticals, Noven Pharmaceuticals Incorporated, and Supernus Pharmaceutical Company.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.