
Abstract
Objective:
To determine whether girls and boys with ADHD show distinct impairments in components of cognitive control across multiple tasks (go/no-go, stop signal, and flanker) and performance metrics (response speed, variability, and errors).
Method:
A total of 300 children, ages 8 to 12 years with ADHD (n = 210, 58 girls) or typically developing (TD; n = 99, 37 girls), completed all tasks. Traditional response measures (e.g., mean and standard deviation of reaction time, inhibition errors, and stop signal reaction time) and ex-Gaussian modeling of reaction times (mu, sigma, and tau) were analyzed.
Results:
Girls showed intact response inhibition in the context of slower response speed, while boys made more inhibition errors and did not slow their response speed. Both girls and boys with ADHD showed higher response variability and poorer interference control than TD children.
Conclusion:
Girls and boys with ADHD show distinct impairments in cognitive control that may be important for understanding the pathophysiology of ADHD.
Introduction
ADHD is one of the most common neurodevelopmental disorders, affecting an estimated 6% of children globally (Faraone et al., 2021), characterized by developmentally inappropriate symptoms of inattention, hyperactivity, and impulsivity that impact daily functioning (American Psychiatric Association, 2013). These behavioral symptoms are thought to be related to impaired cognitive control, defined as the ability to direct and coordinate one’s mental processes (Lavie et al., 2004). This includes specific deficits in the domains of inhibitory control, interference control, and attention regulation, reflected in higher intrasubject variability (ISV) of reaction times (Kofler et al., 2013; Nikolas & Nigg, 2013; Willcutt et al., 2005). Furthermore, there is emerging evidence of distinct cognitive deficits in girls versus boys with ADHD, with boys showing less impairment than girls in tasks measuring response inhibition, interference control, and cognitive flexibility (Loyer Carbonneau et al., 2021). However, girls with ADHD are often underrepresented in research given the disproportionate prevalence of ADHD in boys versus girls (2:1; Ramtekkar et al., 2010). This limits our understanding of ADHD-related sex differences in cognitive functioning. Recent studies have shown that girls and boys with ADHD show distinct impairments in response inhibition in childhood (Seymour et al., 2016) and differing trajectories into adolescence (DeRonda et al., 2021). Therefore, it’s important for us to gain a better understanding of the nature of these deficits and their implications for sex differences in clinical presentation, emerging comorbidities, and long-term functional outcomes (Gordon & Hinshaw, 2020; Karalunas et al., 2017).
Inhibitory control, or the ability to suppress a prepotent response or action in order to achieve a goal, is impaired in 40% to 50% of children with ADHD (Nigg, 2005; Sonuga-Barke, 2002; Willcutt et al., 2005) and emphasized in etiological models (Barkley, 1997). ADHD is associated with lower inhibition accuracy (i.e., ability to withhold a response) on go/no-go (GNG) tasks (Manoli et al., 2021; Metin et al., 2012; Wright et al., 2014) and speed of inhibition on stop signal tasks (Huizenga et al., 2009; Lijffijt et al., 2005; Lipszyc & Schachar, 2010). There is inconsistent evidence of ADHD-related sex differences in inhibition accuracy during a GNG task, with some studies reporting higher commission error rates in boys, but not girls, with ADHD (O’Brien et al., 2010; Seymour et al., 2016), whereas others have reported no ADHD-related sex difference in commission errors relative to same-sex typically developing (TD) children (Bezdjian et al., 2009; Sjöwall et al., 2013). Regarding speed of inhibition during the SST, one study reported that girls with ADHD-Inattentive type showed slower stop signal reaction time (SSRT) than boys with ADHD-Inattentive type, who performed as well as control boys (Nigg et al., 2002), whereas most others showed similar deficits in SSRT in girls and boys with ADHD (Kuntsi et al., 2001; Nigg, 1999). Importantly, most studies focus on SSRT, but SSRT estimates are impacted by other task components (e.g., go response speed, adjusting onset of stop signal delay, and response inhibition accuracy). These components may differ among girls and boys with ADHD, but are less often examined.
Interference control, or the ability to direct attention to a specific stimulus while ignoring surrounding/distracting stimuli, is a related but distinct construct to inhibitory control, typically assessed with the flanker task (Eriksen & Eriksen, 1974; Nigg, 2000). The flanker task is designed to test for congruency effects, such that more errors and slower RT occur when a target stimulus is surrounded or “flanked” by incongruent (different) stimuli rather than congruent (same) stimuli (Lewis et al., 2016). Some studies show children with ADHD experience a greater congruency effect than TD children for both RT and accuracy (Crone et al., 2003; Konrad et al., 2006; Tsal et al., 2005), while others report no diagnostic group differences, as reported in a meta-analysis of the flanker task (Mullane et al., 2009). These inconsistent results may be due to small sample sizes, ADHD subtype, comorbidities, or varying task parameters. Furthermore, the few studies comparing flanker task performance for boys and girls with and without ADHD did not find evidence of ADHD-related sex differences (Adamo et al., 2014; Assari, 2021).
One of the most consistent findings in studies of cognitive control in ADHD is higher ISV of RT (Epstein et al., 2011; Klein et al., 2006; Kofler et al., 2013), thought to be related to impairments in attentional processing, temporal processing, state regulation, or higher order cognitive processing (Leth-Steensen et al., 2000; Rapport et al., 2008; Sergeant, 2005; Sonuga-Barke & Halperin, 2010). Traditional measures of ISV included standard deviation (SD) of RT or coefficient of variation (mean/SD of RT), although these metrics are often highly correlated with mean RT and heavily influenced by outlying values (i.e., infrequent, very slow RTs) that occur more often in children with ADHD (Castellanos et al., 2006; Epstein et al., 2011). Alternatively, ex-Gaussian modeling separates the RT distribution into the normal (Gaussian) component with a mean (mu) and standard deviation (sigma), and the exponential component of the RT distribution (tau). This model may be more advantageous than traditional measures of response speed and variability (mean and SD of RT) for examination of ISV in ADHD as it separates response speed and variability (Hervey et al., 2006; Leth-Steensen et al., 2000). Studies that have examined these ex-Gaussian parameters show that children with ADHD displayed higher tau across cognitive control tasks (i.e., SST, GNG, and flanker) but did not differ from TD controls for mu or sigma (Epstein et al., 2011; Hwang-Gu et al., 2019; Salunkhe et al., 2021). Although there is limited research comparing ISV in boys and girls with ADHD, the few studies that have examined ADHD-related sex differences report similar impairments in RT variability among girls and boys with ADHD (Seymour et al., 2016; Sjöwall et al., 2013).
The current study examines ADHD-related sex differences across multiple cognitive control tasks and performance metrics (e.g., response speed, variability, and inhibition errors) to characterize cognitive control among girls and boys with and without ADHD. We hypothesize that: (1) Boys, but not girls, with ADHD will make more inhibition errors on the GNG task relative to same-sex TD children, as previously shown (Seymour et al., 2016), and show slower inhibition speed (SSRT on the SST); we will also examine RT for go stimuli and other performance metrics to better understand how girls and boys with ADHD approach inhibition tasks; (2) In contrast, boys and girls with ADHD will show similar impairments in interference control during the flanker task (i.e., more errors and slower RT for incongruent vs. congruent trials) relative to same-sex TD children; and (3) Girls and boys with ADHD will show similarly elevated ISV of RT across tasks, relative to same-sex TD children, suggesting a common impairment in ISV in ADHD regardless of sex and task demands.
Methods
Participants
The current sample included 300 children ages 8 to 12 years with either a diagnosis of ADHD (n = 201, 58 girls) TD controls (n = 99, 37 girls; demographic and clinical characteristics are provided in Table 1). Participants were recruited from local schools, pediatricians (office flyers and electronically via MyChart), community centers using flyers and word-of-mouth, and local outpatient clinics. All parents completed an initial telephone screening to determine eligibility. Children with a history of intellectual disability, seizures, traumatic brain injury, neurological illnesses, prematurity, prenatal exposure to teratogens (based on parent-report of maternal substance use and pre/postnatal complications), genetic disorders, or other neurodevelopmental disorders (e.g., autism spectrum disorder), or IQ below 80 were excluded from participation. Participants taking stimulant medication were asked to withhold medication on the day prior to and day of the study visit. Children taking psychotropic medications other than stimulant medication (ADHD non-stimulant medication n = 5; SSRI n = 16; Other psychotropic n = 3) did not discontinue their medication for study visits.
Diagnosis × Sex Group Comparisons of Demographic and Clinical Characteristics.
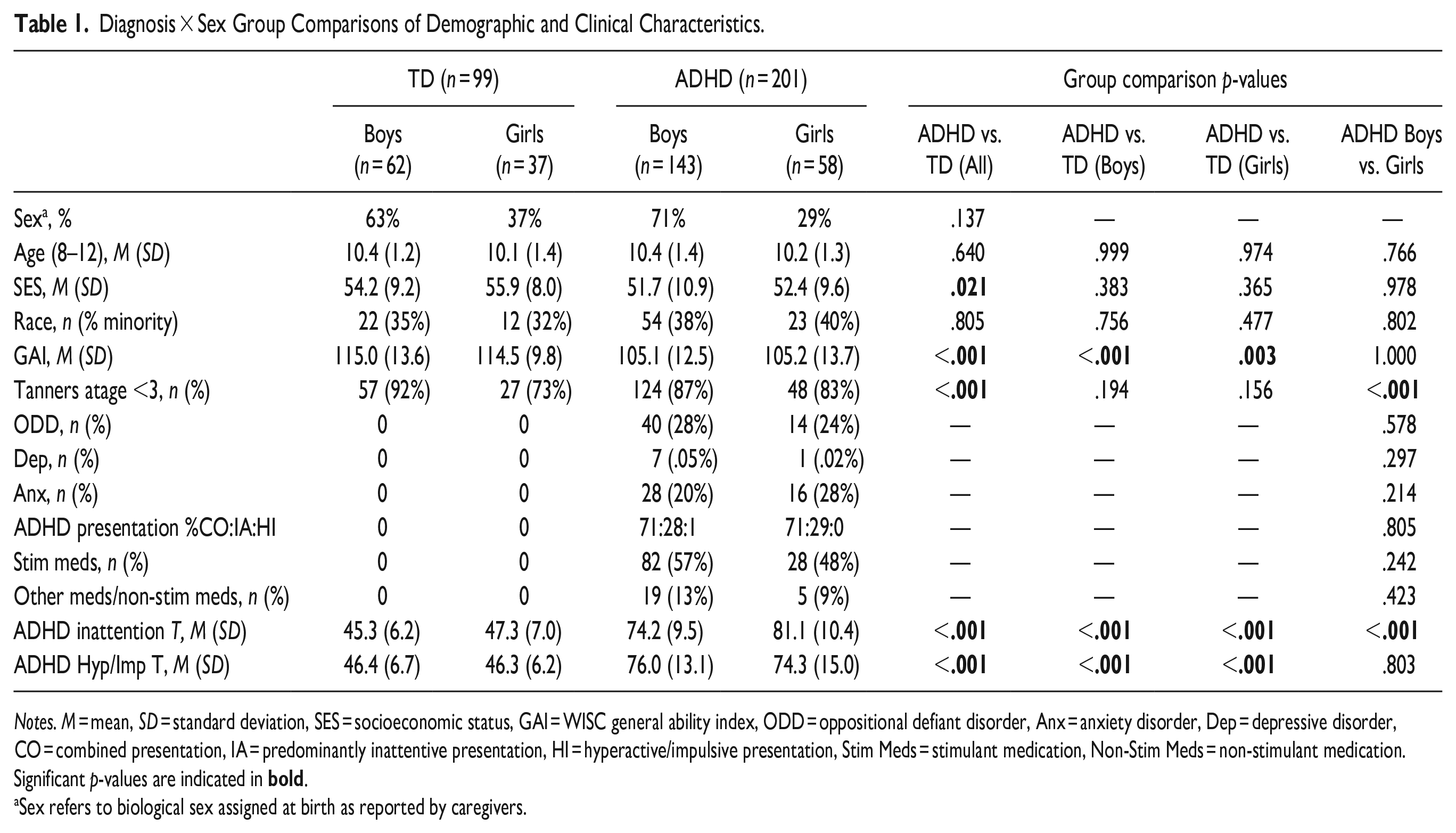
Notes. M = mean, SD = standard deviation, SES = socioeconomic status, GAI = WISC general ability index, ODD = oppositional defiant disorder, Anx = anxiety disorder, Dep = depressive disorder, CO = combined presentation, IA = predominantly inattentive presentation, HI = hyperactive/impulsive presentation, Stim Meds = stimulant medication, Non-Stim Meds = non-stimulant medication. Significant p-values are indicated in
Sex refers to biological sex assigned at birth as reported by caregivers.
Diagnostic and Intellectual Assessments
Prior to the initial laboratory session, a diagnosis of ADHD was determined using a diagnostic parent interview administered either via the phone or video conference over the Zoom platform. Participants were administered either the Diagnostic Interview for Children and Adolescents (DICA-IV; n = 111; Reich, 2000) or the Kiddie Schedule for Affective Disorders and Schizophrenia (KSADS; n = 189; Kaufman et al., 2013; Townsend et al., 2020), as we transitioned to the KSADS over the course of the study. Master’s level clinicians conducted all diagnostic interviews and integrated information from rating scales to inform diagnoses under the supervision of licensed doctoral level clinical psychologists. Parents and teachers (when available) also completed the ADHD Rating Scale (ADHD-RS; DuPaul et al., 2015) and the Conners 1 Parent Rating Scale-Revised (n = 44) or Version 3 (n = 243; Conners, 1997, 2008) which were used to inform diagnostic decision-making and to provide dimensional measures of ADHD symptom severity and emotional lability. Parents were instructed on both the diagnostic interview and questionnaires to make ratings based on their children’s symptoms off of their regularly prescribed medication when possible. At the initial laboratory session, participants were administered either the Wechsler Abbreviated Scale of Intelligence, Second Edition (n = 7) or the Wechlser Intelligence Scale for Children Fourth Edition (n = 119) or Fifth Edition (n = 172; Wechsler, 1999, 2003, 2014) and were excluded for a full-scale intellectual quotient (FSIQ) score below 80. 2 The General Ability Index (GAI), an estimate of intellectual reasoning ability without processing speed or working memory subtests, was also calculated and considered as a covariate.
Participants were included in the ADHD group if they: (1) met criteria for an ADHD diagnosis either on the DICA-IV or KSADS and (2) received a T-score of 60 or higher on the DSM Inattentive or DSM Hyperactive-Impulsive scales on the Conners Parent or Teacher (when available) rating scales, or a score of 2 or 3 (i.e., symptoms rated as occurring “often” or “very often”) on at least 6/9 items on the Inattentive or Hyperactivity/Impulsivity scales of the ADHD-RS Home or School (when available) Version. Children with ADHD were allowed to meet criteria for comorbid psychiatric diagnoses on the DICA-IV or K-SADS including oppositional defiant disorder (ODD; n = 54), anxiety disorders (n = 44), and depressive disorders (n = 8). Girls and boys with ADHD did not differ in comorbid diagnoses of ODD (p = .578), anxiety (p = .214), or depression (p = .297).
Participants were included in the control group if they: (1) did not meet criteria for any psychiatric disorders on the DICA-IV or K-SADS, (2) scored below clinically significant cut-offs (T < 60) on the Conners Parent and Teacher rating scales, and ADHD-RS Home and School Versions, and (3) did not have an immediate family member with ADHD given the heritability of cognitive functioning (Crosbie et al., 2013) and evidence that unaffected individuals with a familial history of ADHD often show similar deficits in cognitive control (Arnett et al., 2022; van Lieshout et al., 2019).
Ethical Considerations
Study protocols were reviewed and approved by the Johns Hopkins University Institutional Review Board and parents provided written consent with child participants providing assent.
Cognitive Control (CC) Tasks
Go/No-Go (GNG)
The task stimuli consisted of green spaceships for “Go” trials (80% of trials) and red spaceships for “No-Go” trials (20% of trials), presented one at a time (Mostofsky et al., 2003). Participants were instructed to push the spacebar with their index finger as quickly as possible in response to green spaceships only. The use of familiar stimulus-response associations (green for “go”; red for “no-go”) minimized the perceptual and cognitive demands of the tests. Presentation cues were weighted toward green spaceships at a ratio of 4:1, intensifying the need to inhibit a habituated motor response. Go and no-go trials appeared in pseudorandom order with the restrictions that there were never fewer than three go trials before a no-go cue and never more than two no-go trials in a row. There were 11 practice trials (8 go cues; 3 no-go cues) followed by 217 experimental trials (173 go cues; 44 no-go cues). Stimuli were present on-screen for 300 ms with an interstimulus interval of 2,000 ms (trial length = 2,300 ms) during which a fixation cross was present on-screen. Responses and reaction times (RT) were recorded for the entire trial duration. Responses faster than 200 ms were excluded from all RT analyses.
Commission error rate was defined as the proportion of no-go trials on which the participant responded. Mean RT was also calculated as an index of response speed for go trials to allow for comparison with other tasks. However, mean RT is influenced by the skewed RT distribution. Therefore, mu, sigma, and tau were also derived using ex-Gaussian analysis of correct go trial RTs. Mu represents the mean of the normal component of the RT distribution and sigma represents the variation of the normal distribution. Tau, which was the primary measure of ISV, represents the mean and standard deviation of the exponential component of the distribution. Ex-Gaussian RT estimates and a goodness-of-fit value, with lower values indicating better fit to the ex-Gaussian model, were computed in Matlab (Andreou et al., 2007) using the DISTRIB toolbox (Lacouture & Cousineau, 2008), during which data converged for all participants. Dependent variables (DVs) analyzed for the GNG task were commission error rate (ComRate), mean RT, mu, sigma, and tau.
Stop Signal Task (SST)
The SST was used as a measure of inhibitory control (Rosch et al., 2016). The task stimuli included a 2 × 2 cm arrow pointing either left or right presented on a computer screen. Participants were instructed to indicate the direction of the stimuli by pressing either the left arrow key or right arrow key using a response pad (Psychology Software Tools, Pittsburgh, PA), but to inhibit responding when presented with an auditory stop signal (25% of trials). The stop signal was a 1000 Hz tone presented for 100 ms. Participants first completed 32 practice trials without the stop signal, followed by 32 practice trials including the stop signal, and then 4 blocks of 64 trials. On the first stop trial, the tone onset was 350 ms, then adjusted based on participants’ response. If participants correctly inhibited, the latency between the stimuli and stop signal increased by 50 ms (i.e., became more difficult) but decreased by 50 ms if participants failed to inhibit (i.e., became easier). DVs analyzed for the SST were: (1) Mean of Go RT (MRT); (2) ComRate (responding on a stop trial); (3) Stop Signal Delay (SSD), the time between presentation of the stimuli and stop signal tone, (4) SSRT (MRT – SSD), (5) ex-Gaussian parameters (mu, sigma, and tau) for Go responses.
Flanker Task
This is an adaptation of the Eriksen Flanker task (Eriksen & Eriksen, 1974) designed to measure interference control. In this version, the task stimuli consisted of five arrows pointed to the left or right presented in a single row. Participants were instructed to indicate the direction of the center arrow (target stimuli) by pressing either a left arrow key or right arrow key using a response pad (Psychology Software Tools, Pittsburgh, PA). Incongruent trials (50%) consisted of two arrows on both sides of the center arrow facing the opposite direction of the target stimuli, whereas surrounding arrows were in the same direction as the target stimuli for congruent trials. The task consisted of two blocks of 180 trials; the stimuli were present on the screen for 1,000 ms. Response and reaction time were recorded for each trial. Dependent variables for the flanker task included: congruency effect on error rate and MRT calculated as the incongruent-congruent error rate and MRT with higher scores reflecting a greater flanker interference effect, or increased errors/slowing with incongruent flankers, as well as mu, sigma and tau, calculated regardless of trial type.
Data Analysis
Data analysis was conducted with Jamovi Version 2.319 (Jamovi, 2022). Performance for each DV on the GNG, SST, and Flanker tasks was examined with 2 Diagnosis (ADHD vs. TD) × 2 Sex (male vs. female) analysis of covariance (ANCOVA) with age as a covariate. Post-hoc analyses were stratified by sex to test for effects of diagnosis among males and females separately given the difference in sample size (M:F ratio of 2:1) and our sex-specific hypotheses, and to be consistent with published guidelines (Heidari et al., 2016). Cohen’s d is reported as a measure of effect size to allow for comparison of the magnitude of effects given the difference in sample size by sex, with small, medium, and large effect sizes as Cohen’s d = 0.3 to 0.5, 0.5 to 0.8, and ≥0.8, respectively (Cohen, 1988). We also conducted sensitivity analyses with additional covariates to examine the potential impact of non-stimulant medication, pubertal status, GAI, and SES 3 (see Supplemental Table 1) and noted any meaningful change in results where relevant. Additionally, all analyses were also conducted excluding children with comorbid anxiety/depression (n = 48) and any meaningful differences are noted (see Supplemental Table 2). Finally, outliers were defined as values that were ±3 SDs away from the overall group mean specific to a task metric. Analyses were conducted with and without outliers for individual task metrics with similar results obtained and any meaningful changes reported in a footnote.
Results
Demographic and Clinical Characteristics
Descriptive statistics and results of one-way ANOVAs comparing demographic and clinical characteristics between diagnostic groups across and within sex are provided in Table 1. Diagnostic groups did not differ in age (p = .640), sex (p = .137), or race (p = .805), whereas SES was significantly lower for the ADHD group (p = .021) and GAI was significantly lower for boys with ADHD compared to TD boys (p ≤ .001) as well as girls with ADHD compared to TD girls (p = .003). Regarding ADHD-related sex differences in symptom presentation, inattention T-scores were greater among girls compared to boys with ADHD (p < .001).
GNG Performance
Results of 2 Diagnosis × 2 Sex ANCOVAs for the GNG task are reported in Table 2. Consistent with previously published findings (Seymour et al., 2016), ComRate was higher in boys with ADHD than TD boys (p = .008, d = 0.041), whereas girls with ADHD did not differ from TD girls (p = .938, d = 0.02). Thus, there was no main effect of diagnosis, F(1, 295) = 2.64, p = .105, and the Diagnosis × Sex interaction was not significant, F(1, 295) = 2.25, p = .135 (Figure 1a). A main effect of diagnosis was observed for GoMRT, F(1, 295) = 17.0, p < .001, with slower responses in children with ADHD than TD controls. Within sex comparisons revealed that this diagnostic effect was similar in boys (p = .008, d = 0.041) and girls (p = .002, d = 0.66), with no Diagnosis × Sex interaction, F(1, 295) = 0.99, p = .321. A Diagnosis × Sex interaction emerged 4 for mu, F(1, 295) = 5.85, p = .016, and sigma, F(1, 295) = 5.93, p = .015, such that girls with ADHD displayed higher mu (p = .061, d = 0.40) and sigma (p = .003, d = 0.64) than TD girls, whereas boys with ADHD did not differ from TD boys for mu (p = .128, d = −0.23) or sigma (p = .974, d = 0.01; Figure 1b and c). Furthermore, there was a main effect of diagnosis on tau, F(1, 295) = 15.7, p < .001, such that children with ADHD, regardless of sex, showed greater tau than TD children (p < .001) with similar magnitude effects of diagnosis for girls (d = 0.46) and boys (d = 0.57; Figure 1d).
Results of ANCOVAs for Each Task Dependent Variable and Comparison of Diagnosis-by-Sex Subgroups.
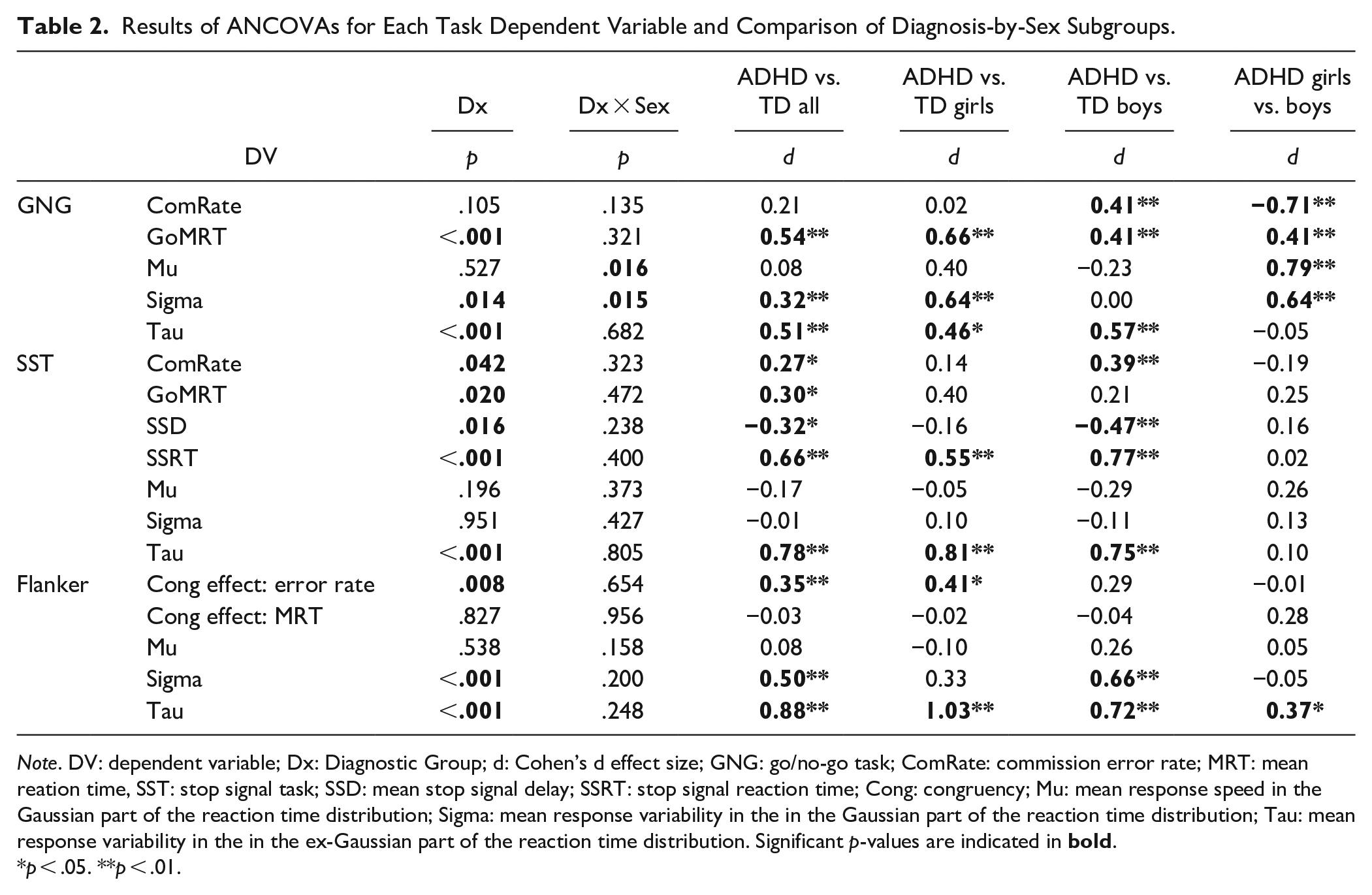
Note. DV: dependent variable; Dx: Diagnostic Group; d: Cohen’s d effect size; GNG: go/no-go task; ComRate: commission error rate; MRT: mean reation time, SST: stop signal task; SSD: mean stop signal delay; SSRT: stop signal reaction time; Cong: congruency; Mu: mean response speed in the Gaussian part of the reaction time distribution; Sigma: mean response variability in the in the Gaussian part of the reaction time distribution; Tau: mean response variability in the in the ex-Gaussian part of the reaction time distribution. Significant p-values are indicated in
p < .05. **p < .01.
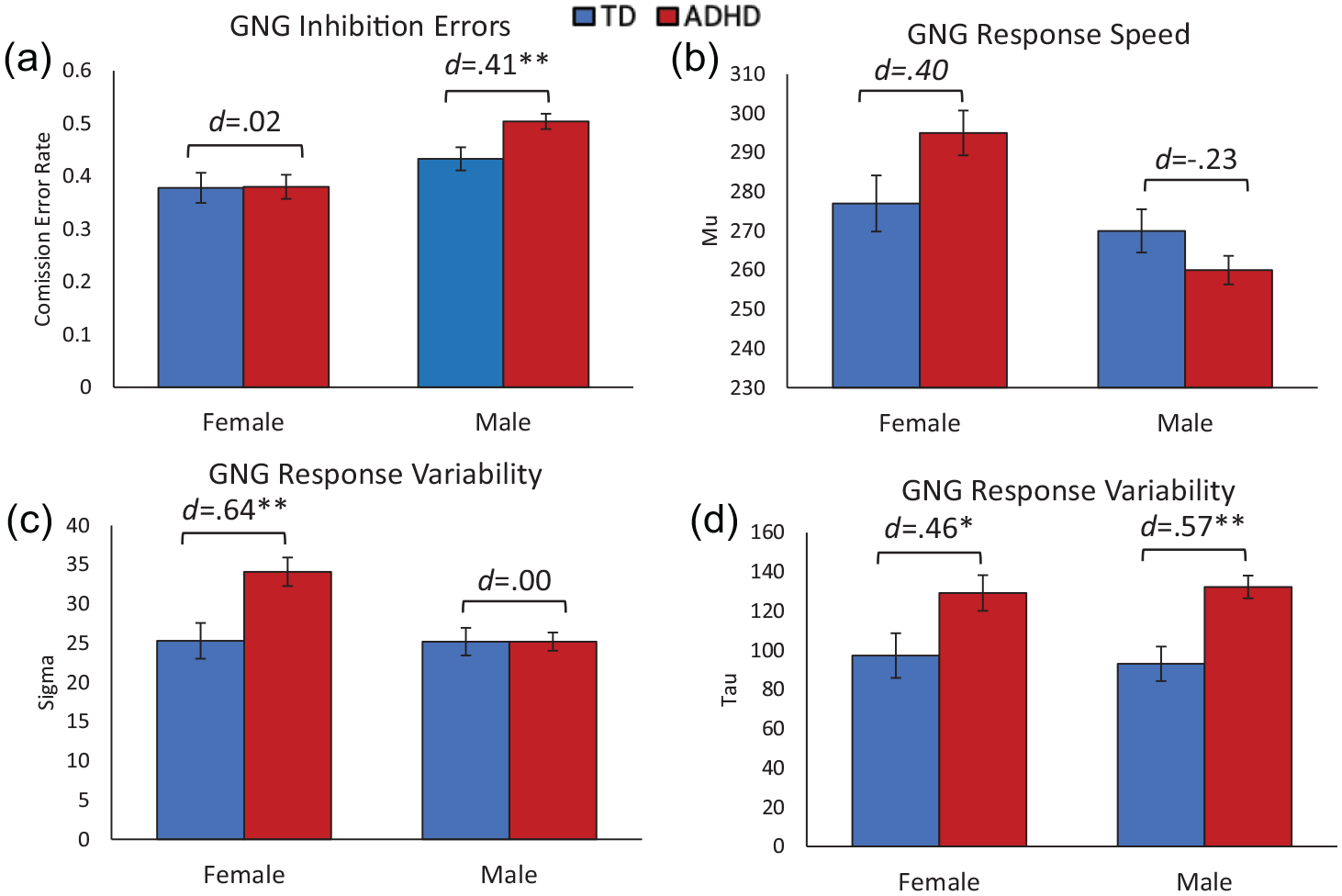
Go/no-go task performance among diagnosis by sex subgroups: (a) commission error rate: proportion of no-go trials with a failed inhibition, (b) Mu: mean response speed in the Gaussian part of the reaction time distribution for go trials, (c) Sigma: mean response variability in the in the Gaussian part of the reaction time distribution for go trials, and (d) Tau: mean response variability in the in the ex-Gaussian part of the reaction time distribution for go trials.
SST Performance
Results of 2 Diagnosis × 2 Sex ANCOVAs for the SST are reported in Table 2. There was a main effect of diagnosis for ComRate, F(1, 295) = 4.19, p = .042. 5 Although the Diagnosis × Sex interaction was not significant, F(1,295) = 0.98, p = .323, within sex comparisons suggests the effect of diagnosis was driven by boys with ADHD who made significantly more commission errors than TD boys (p = .010, d = 0.39), with no effect in girls (p = .515, d = 0.14; Figure 2a). There was also a main effect of diagnosis on SSRT, F(1, 295) = 26.1, p < .001. This did not significantly vary by sex, Diagnosis × Sex: F(1, 295) = 0.70, p = .402, with similar effects of diagnosis for girls (p = .009, d = 0.55) and boys (p < .001, d = 0.77; Figure 2b). Interestingly, there was some evidence of ADHD-related sex differences in Go Mean RT and SSD, which contribute to SSRT. Specifically, there was a main effect of diagnosis for Go MRT, F(1, 295) = 5.48, p = .020, and for SSD, F(1, 295) = 5.87, p = .016, 6 with no significant Diagnosis × Sex interaction (ps = .472 and .238, respectively). However, within-sex comparisons revealed that girls with ADHD tended to respond more slowly than TD girls (p = .060, d = 0.40), than did boys with ADHD compared to TD boys (p = .167, d = 0.21; Figure 2c). In contrast, for SSD, girls with ADHD did not differ from TD girls (p = .445, d = −0.16) whereas SSD was lower (making it easier to inhibit) in boys with ADHD compared to TD boys (p = .002, d = −0.47; Figure 2d). Finally, there was also a main effect of diagnosis on tau, F(1, 295) = 34.1, p < .001, with similar magnitude effects of diagnosis for girls (p < .001, d = 0.81), and boys (p < .001, d = 0.75), whereas there were no effects of diagnosis on mu (p = .196) or sigma (p = .951).
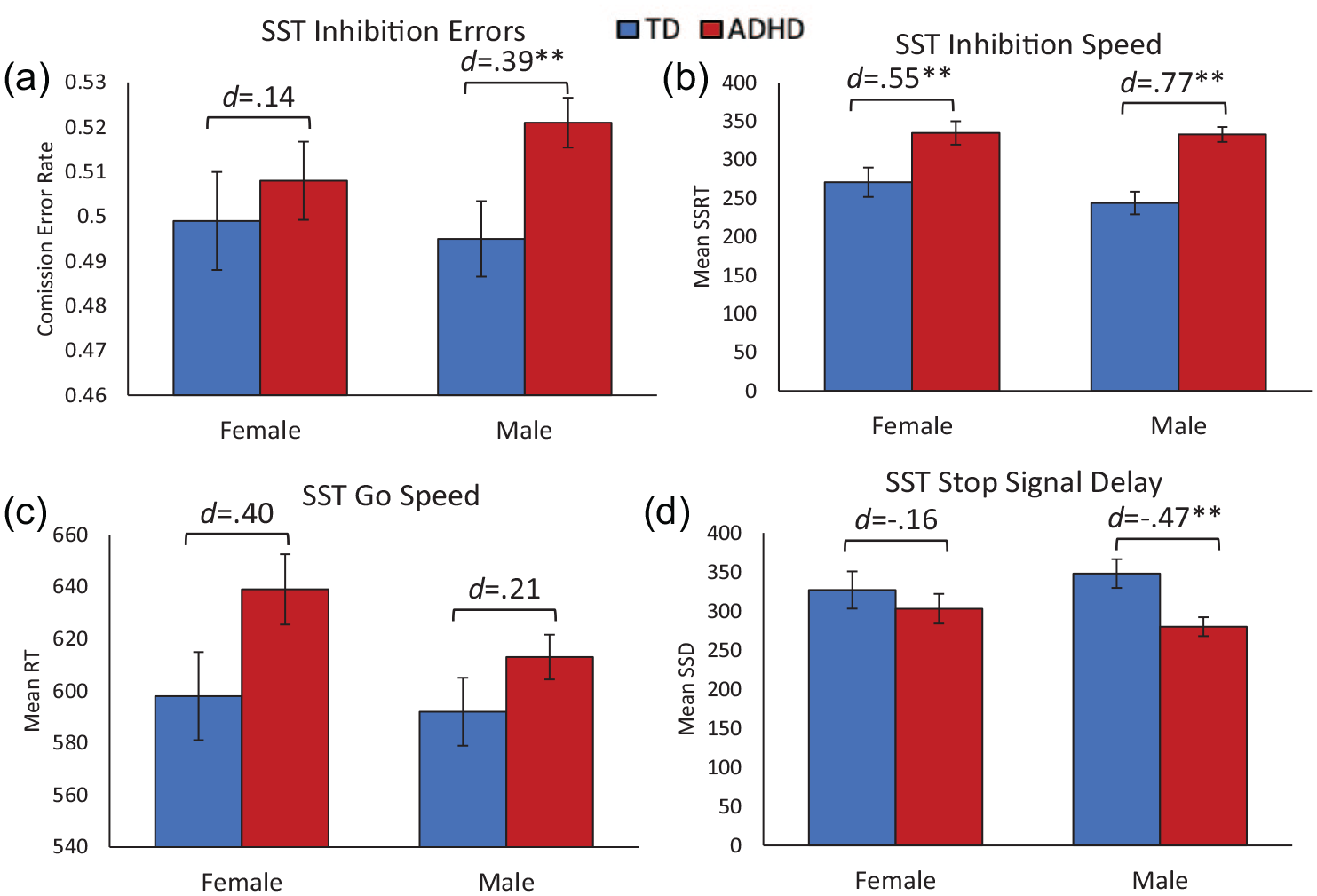
Stop signal task performance among diagnosis by sex subgroups: (a) commission error rate: proportion of stop trials with a failed inhibition, (b) stop signal reaction time (SSRT): speed of inhibition calculated as the difference between the mean RT for go trials and the mean stop signal delay, (c) mean RT: mean response speed for go trials, and (d) mean stop signal delay (SSD): mean onset of the stop signal relative to the onset of the go stimulus.
Flanker Performance
Select results of 2 Diagnosis × 2 Sex ANCOVAs for the Flanker are reported in Table 2. There was a main effect of diagnosis for the congruency effect on error rate, F(1, 295) = 7.2, p = .008, such that children with ADHD showed a larger increase in errors for incongruent versus congruent stimuli, with similar magnitude effects of diagnosis for girls (d = 0.41) and boys (d = 0.29; Figure 3a). In contrast, diagnostic groups did not differ in the congruency effect on mean RT, F(1, 295) = 0.05, p = .827, regardless of sex (girls d = −0.02; boys d = −0.04; Figure 3b). There were also main effects of diagnosis, regardless of congruency, on sigma, F(1, 295) = 14.7, p < .001, and tau, F(1, 295) = 45.7, p < .001, that did not vary by sex (sigma: girls d = 0.33, boys d = 0.66; tau: girls d = 1.03, boys d = 0.72). Children with ADHD showed greater response variability in the normal and exponential parts of the RT distribution than TD children, whereas mu did not differ across diagnostic groups, F(1, 295) = 0.38, p = .538.
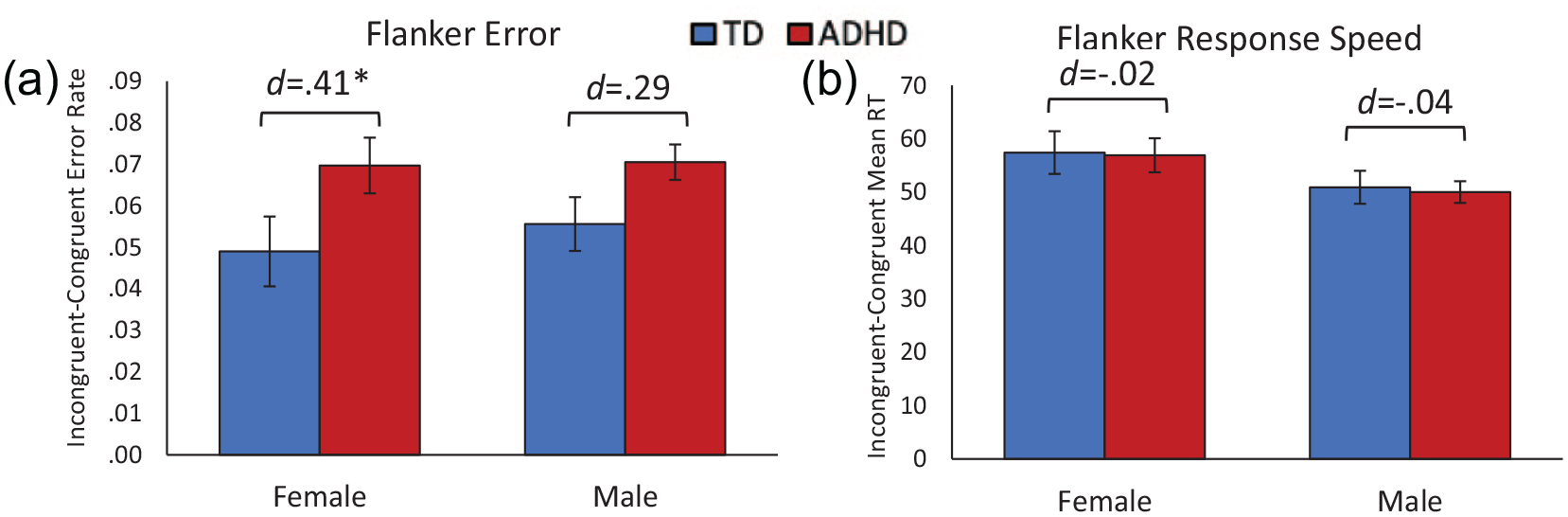
Flanker task performance among diagnosis by sex subgroups: (a) error rate: difference in proportion of errors for incongruent versus congruent trials (higher values reflect a greater flanker interference effect) and (b) mean reaction time (RT): difference in RT for incongruent versus congruent trials (higher values reflect a greater flanker interference effect).
Discussion
The current findings add to our understanding of ADHD-related sex differences in cognitive control through replication and extension of prior findings to assess multiple performance indicators across different cognitive control tasks. Our results suggest distinct profiles of cognitive control impairments in girls and boys with ADHD, relative to same-sex TD children, that vary across tasks and performance metrics. Boys with ADHD show impaired response inhibition accuracy across GNG and SST tasks, whereas girls with ADHD show intact response inhibition accuracy, but at the cost of slower response speed to the go stimuli. Speed of response inhibition, assessed with the SSRT, is similarly affected in girls and boys with ADHD, but for different reasons, with slower go response speed in girls with ADHD and shorter stop signal delay (related to lower inhibition accuracy) in boys with ADHD. There was no evidence of ADHD-related sex differences in interference control, assessed with the flanker task. Finally, children with ADHD, regardless of sex, displayed higher response variability (as reflected in tau) across all tasks. Understanding shared and distinct deficits in cognitive control in girls and boys with ADHD across performance metrics and cognitive control tasks is important for advancing the ADHD cognitive literature and the nature of sex differences in youth with ADHD.
Regarding performance on inhibition tasks (GNG and SST), we were able to replicate GNG findings from Seymour et al. (2016), showing intact response inhibition in girls with ADHD relative to TD girls, whereas boys with ADHD made more commission errors than TD boys. Similarly, for the SST, inhibition accuracy was also lower in boys, but not girls, with ADHD relative to TD children. Building on these findings to better understand how girls with ADHD are able to inhibit as well as TD girls, we examined indicators of response speed (mean RT and mu). Results suggest that although boys and girls with ADHD had a slower response speed to go stimuli than TD counterparts, this effect is more pronounced in girls with ADHD and particularly for mu, indexing the mean response speed separate from variability. Our results indicate that girls with ADHD are slower to respond to go stimuli, thereby improving their ability to inhibit on no-go/stop stimuli. Thus, girls with ADHD may engage in more compensatory behavior (i.e., slowing down) in order to inhibit as well as TD girls. On the other hand, boys with ADHD are responding as fast as TD boys but are making significantly more errors, which may be reflective of impulsivity.
Considering both response speed and inhibition accuracy suggests that girls and boys with ADHD may adopt a different approach to inhibition tasks, with boys responding as quickly as possible but failing to inhibit and girls slowing down to inhibit. This interpretation is consistent with a previous study (Newcorn et al., 2001) showing that girls with ADHD and anxiety made fewer commission errors, but this effect was not observed in boys with ADHD regardless of comorbid anxiety. Thus, it may be that co-occurring internalizing symptoms may facilitate error monitoring and compensatory behavior in girls with ADHD, but not boys, prompting them to slow down to successfully inhibit. As boys and girls with ADHD in our sample did not differ significantly in diagnoses of depression or anxiety, these ADHD-related sex differences are not due to higher rates of anxiety in girls with ADHD, but perhaps subthreshold anxiety serves an adaptive function in girls with ADHD.
Consistent with prior literature, our results showed that the ADHD group showed slower SSRT than the TD group with ADHD boys and girls not differing in their performance (Kuntsi et al., 2001; Nigg, 1999). However, further probing of the components of SSRT (i.e., go RT and onset of the stop signal delay, which adjusts depending on inhibition accuracy) revealed differences in girls and boys with ADHD. During the SST, the SSD will occur sooner if participants fail to inhibit which in turn makes it easier for them to inhibit and will result in shorter SSD. In addition, the task is designed to approximate 50% inhibition, but this is not necessarily achieved and may be important to consider when interpreting SSRT. Examination of these additional parameters revealed that the ADHD group made significantly more commission errors and had a longer SSD than the TD group; however, this effect was driven by boys with ADHD, as girls with ADHD did not differ from TD girls. On the other hand, the ADHD group was slower to respond than the TD group, but this effect was driven by girls with ADHD as boys with ADHD did not differ from TD boys. Thus, focusing analyses only on differences in SSRT may overlook ADHD-related sex differences, such that girls with ADHD may have slowed to inhibit and boys with ADHD did not apply this strategy. As findings from the SST show similar patterns to the GNG task, this suggests that these tasks assess similar aspects of inhibitory control and demonstrate the importance in examining the metrics that influence SSRT, which provide us with an in depth understanding of the cognitive processes involved in this task and revealed some ADHD-related sex effects.
Prior literature shows that interference control is inconsistently affected in children with ADHD (Crone et al., 2003; Konrad et al., 2006; Mullane et al., 2009; Tsal et al., 2005), with no prior evidence of sex differences (Adamo et al., 2014; Assari, 2021). In our study, during the flanker task, children with ADHD and TD children were both slower to respond during incongruent trials but did not differ from each other in the extent of response slowing, regardless of sex. However, children with ADHD made more errors during incongruent trials compared to TD children with a larger and significant diagnostic effect (i.e., ADHD vs. TD) in girls relative to boys, but there is otherwise not strong evidence of differential impairments in interference control in girls and boys with ADHD. In our sample, although boys and girls with ADHD did not differ on ADHD subtype and hyperactive/impulsive symptom severity, they did differ on inattentive symptom severity. Consistent with ADHD literature, girls with ADHD showed greater inattentive symptoms (Hinshaw et al., 2006; Rucklidge, 2010). Distractibility is one of the nine inattentive symptoms of ADHD and empirical evidence suggests that individuals with ADHD are more distracted by irrelevant information during a cognitive task relative to TD children (Cao et al., 2013). This may be why girls with ADHD had a higher error rate than TD girls during the Flanker task, while boys with ADHD did not differ from TD boys.
These findings also provide evidence that, although interference control and response inhibition are indeed components of cognitive control, they are separate cognitive domains. Intact response inhibition, but deficient interference control, may be explained by factors related to effort, arousal and motivation (Johnstone et al., 2009). This might suggest that cognitive impairments are not the result of deficits in a single domain, but rather dysfunction in the executive functioning system as a whole as modeled by various theoretical frameworks (Sergeant, 2000; Sonuga-Barke, 2002) where some domains may be intact, while others are not.
Similar to flanker task performance, tau is consistently elevated in children with ADHD, regardless of sex, with similar effect sizes for tau between girls and boys with ADHD across the GNG and SST task, and slightly larger effects in girls versus boys with ADHD in the flanker task. This is consistent with prior research showing that individuals with ADHD exhibit higher RT variability across various cognitive domains (Adamo et al., 2014; Castellanos et al., 2006; Epstein et al., 2011). This deficiency is not task-specific and is thought to be mediated by lapses in attention, a core symptom of ADHD (Epstein et al., 2011; Leth-Steensen et al., 2000). Sigma is also a measure of RT variability but reflects the normal distribution (mean of central RT). While tau provides implications for lapses in attention, sigma is thought to reflect motor/response preparation (Gooch et al., 2012; Metin et al., 2016). The findings from each suggest that boys with ADHD did not differ from TD boys in the speed of their average responses (sigma) but had significantly more extremely slow responses (tau) which resulted in a slower MRT. On the other hand, as compared to TD girls, girls with ADHD were more variable in their responding across trials (sigma and tau). Given that girls with ADHD in our sample also show greater inattention symptom severity, and motor planning has been shown to relate to inattention, this might explain the elevated sigma levels in girls with ADHD (Fassbender et al., 2015; Kaiser et al., 2015). Future studies should include more girls with ADHD to allow for diagnostic group comparisons to be made within sex, particularly in childhood and adolescence when girls and boys are developing at different rates (Murray et al., 2019) and ADHD is more common in boys, whereas sex differences in prevalence are no longer observed in adults (Nussbaum, 2012). Future studies should also examine these cognitive control difficulties in relation to clinical presentation and changes to symptoms as an individual ages using multiple performance indicators to understand the overall strategy. The use of traditional RT measures (mean and SD) and ex-Gaussian metrics (mu, sigma, and tau) also elucidates the cognitive processes involved by separating speed and variability of responding.
Limitations
This study is not without limitations. First, our study excluded children with prematurity or prenatal exposure to teratogens (e.g., maternal substance use) to minimize variance in the etiology of ADHD in our sample. Therefore, the current study findings may not generalize to individuals with ADHD due to prenatal complications. Second, we excluded TD participants with an immediate family member with ADHD given the heritability of cognitive functioning (Crosbie et al., 2013) and evidence that unaffected individuals with a familial history of ADHD often show similar deficits in cognitive control (Arnett et al., 2022; van Lieshout et al., 2019). Therefore, these findings may not generalize to studies that include typically developing controls with greater genetic risk for ADHD. Finally, our sample was comprised mostly of ADHD-combined type participants. It will be important to examine cognitive control in a sample that has an equal distribution of ADHD subtype (as in our sample) and symptom severity among girls and boys to fully understand the cognitive domains affected in different clinical presentations of ADHD.
Conclusion
Results of this study indicate that boys and girls with ADHD engage in distinct task-dependent strategies during inhibition tasks whereas they show similar deficits in interference control and elevated RT variability. Further research is needed to understand the neurobiological basis for these cognitive differences and associations with clinical presentation and course, which has been shown to differ among girls and boys with ADHD. Additionally, these findings demonstrate the value in considering multiple aspects of task performance (including ex-Gaussian modeling) to fully understand the cognitive processes that contribute to ADHD-related sex differences.
Supplemental Material
sj-docx-1-jad-10.1177_10870547241237242 – Supplemental material for The Impact of Sex on Cognitive Control in ADHD: Girls Slow to Inhibit, Boys Inhibit Less, and Both Show Higher Response Variability
Supplemental material, sj-docx-1-jad-10.1177_10870547241237242 for The Impact of Sex on Cognitive Control in ADHD: Girls Slow to Inhibit, Boys Inhibit Less, and Both Show Higher Response Variability by Beatrice Ojuri, Alyssa DeRonda, Micah Plotkin, Stewart H. Mostofsky and Keri S. Rosch in Journal of Attention Disorders
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NIH with grants awarded to KSR (K23-MH101322, R03-MH119457), SHM (R01-MH078160 and R01-MH085328), and P50HD103538. These sponsors had no role in the study design, collection of data, analysis of data, or interpretation of data.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.