
Abstract
Objective:
Previous research suggests a potential link between unsaturated fatty acids (UFAs) and ADHD, but the causal relationship remains uncertain. This study aims to investigate the causal association between ADHD and UFAs using Mendelian randomization (MR) analysis.
Methods:
Summary data from genome-wide association studies were used to estimate the concentration of circulating UFAs, including Monounsaturated Fatty Acids (MUFAs), Polyunsaturated Fatty Acids (PUFAs), Omega-3 PUFAs, Omega-6 PUFAs, Linoleic Acid (LA), and Docosahexaenoic Acid (DHA). Data from the Psychiatric Genomics Consortium, including both childhood and adult ADHD, were respectively used to examine the relationship between genetically predicted UFAs levels and ADHD. Various MR methods, including Inverse-variance weighted (IVW), MR Pleiotropy RESidual Sum and Outlier, MR-Egger, weighted median, and weighted mode, were employed to assess heterogeneity and pleiotropy.
Results:
The IVW revealed only nominal evidence suggesting a potential causal relationship between genetically predicted PUFAs (OR = 0.92, 95% CI [0.85, 0.99], p = .031), Omega-6 PUFAs (OR = 0.90, 95% CI [0.83, 0.98], p = .020), and LA levels (OR = 0.90, 95% CI [0.82, 0.98], p = .021) with childhood ADHD risk. However, after false discovery rate correction, the p-values for PUFAs, Omega-6 PUFAs, and LA levels all exceeded the threshold for significance. For adult ADHD, we did not find any significant associations between the six circulating UFA levels and adult ADHD.
Conclusion:
Our findings do not support a causal relationship between UFAs levels and ADHD. This suggests that UFAs supplements may not be effective in improving ADHD symptoms and importantly, it appears that UFAs levels may not have a long-term effect on ADHD.
Introduction
ADHD is a prevalent neurodevelopmental condition characterized by persistent and impairing symptoms of inattention and/or hyperactivity/impulsivity (Thapar & Cooper, 2016). It affects approximately 5% to 7% of children and often persists into adulthood (Polanczyk et al., 2007), resulting in extensive behaviors that impair daily functioning (Du Rietz et al., 2017). ADHD is also associated with adverse outcomes such as accidents (Z. Chang et al., 2014), injuries (Dalsgaard et al., 2015), substance use disorders (Capusan et al., 2019), and significant societal costs (Libutzki et al., 2019). Despite the symptomatic relief provided by medications such as psychostimulants in the short term (Chen et al., 2022; Cortese et al., 2018), the underlying causes of ADHD remain largely elusive.
Unsaturated fatty acids (UFAs), a major dietary nutrient, have connections to neurodevelopment, brain function, behavior, and mental health (Bonvicini et al., 2016; Macaron et al., 2021; Makrides et al., 2009; Yap et al., 2023). UFAs can be categorized into two main types: Monounsaturated fatty acids (MUFAs) and Polyunsaturated fatty acids (PUFAs), with the number of double bonds differentiating them. Furthermore, Polyunsaturated fatty acids can be divided into Omega-3 series and Omega-6 series. Linoleic acid (LA) is included in the Omega-6 series, and Docosahexaenoic acid (DHA) is part of the Omega-3 series. During early life, it is essential for the fetus to receive an adequate amount of DHA from the mother, as it is crucial for proper myelin formation and appropriate neurodevelopment (Makrides et al., 2009). Additionally, the brain tissue contains high levels of Omega-3 PUFAs and Omega-6 PUFAs, which play significant roles in various biological processes such as metabolism, neurotransmission, synaptogenesis, and inflammation (Bonvicini et al., 2016; Macaron et al., 2021). Some studies suggest that ADHD is linked to changes in the levels and functionality of UFAs in the brain (Gao et al., 2022; Sengottuvel et al., 2023).
Several crucial questions still persist. First, does the concentration of circulating UFAs have a causal impact on the risk of ADHD? Clinical observational studies have found decreased UFAs in patients with ADHD (J. P. Chang et al., 2018). Many clinical intervention studies have also supplemented UFAs as a method for treating ADHD, but the results obtained are inconsistent (J. P. Chang et al., 2018; Gillies et al., 2023; Händel et al., 2021). Another question is, which specific concentration of circulating UFAs indicators are associated with the risk of ADHD? Previous research has primarily focused on the concentration of circulating PUFAs or its subtypes, such as omega-3 and DHA (Bonvicini et al., 2016; J. P. Chang et al., 2018). However, there has been limited emphasis on other indicators of UFAs, such as MUFAs, omega-6 PUFAs, and LA (Milte et al., 2015; L. J. Wang et al., 2019).
Mendelian randomization (MR) is a powerful approach in genetic research that leverages genetic variants as instrumental variables (IVs) to investigate causal associations between risk factors and diseases, mitigating the inherent biases caused by confounding factors in observational studies (Z. Wang et al., 2024; Wei et al., 2023). However, it relies on the assumption that the genetic instruments are valid across the two datasets and that there is no horizontal pleiotropy (where genetic variants affect the outcome through pathways other than the exposure of interest). Through MR methods, Gao et al. discovered genetic correlations between metabolic syndrome and ADHD (Gao et al., 2024). Another MR study suggested that liability to atopic dermatitis is associated with an increased risk of ADHD (Cao et al., 2024). Additionally, a recent drug-target MR study indicated that lipid metabolism is also linked to the risk of ADHD (Guo et al., 2024). However, the causal link between different levels of UFAs and ADHD remains unestablished.
Our two-sample MR study utilized publicly accessible genome-wide association studies (GWASs) datasets from large populations, without directly analyzing participant-level datasets, to examine the impact of the concentration of circulating various UFAs on ADHD. Based on the literature review, our research hypothesis posits that a decrease in the concentration of circulating UFAs will increase the risk of ADHD, as analyzed through MR.
Method
Study Design
In order to explore the potential causal links between the concentration of circulating UFAs and the risk of ADHD, we designed a two-sample MR study. This MR design has to meet three conditions: (1) genetic instruments should predict the exposure of interest with a p-value of less than 5 × 10−8; (2) genetic instruments must be independent of any potential confounders; and (3) genetic instruments must affect the outcome only through the risk factors. The study design is outlined in Figure 1.
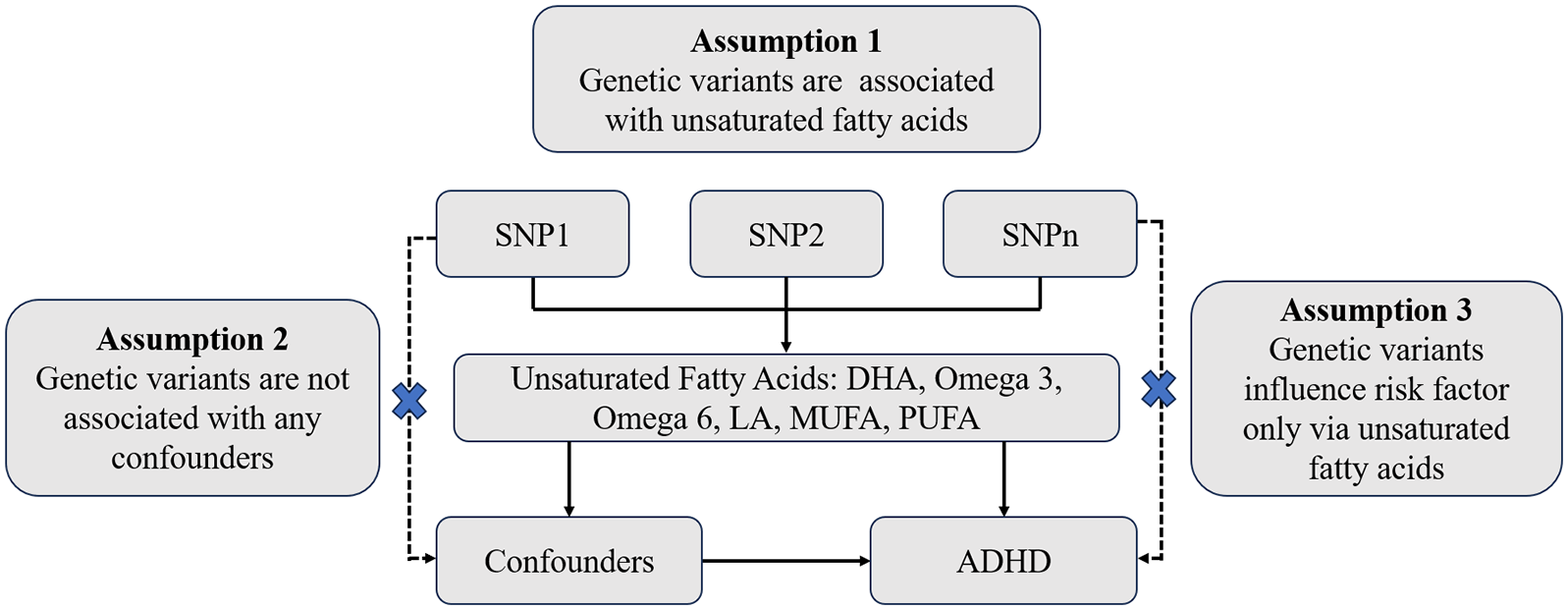
MR Model. Two-sample MR study to examine the potential causal links between the concentration of circulating unsaturated fatty acids and the risk of ADHD. The MR method relies on the following assumptions: (1) the selected SNPs were reliably associated with unsaturated fatty acids; (2) SNPs must be independent of confounding factors; and (3) SNPs were associated with the risk of ADHD only via circulating unsaturated fatty acids levels. The dotted line and the “ × ” represent the variables are invalid if they are associated with the outcome or potential confounders.
Data Sources
The UK Biobank provided genetic instrument exposure associations from a GWAS for the concentration of circulating UFAs traits (MUFAs, PUFAs, Omega-3 PUFAs, Omega-6 PUFAs, LA, and DHA) among individuals of European ancestry, which involved 114,999 participants and 12,321,875 measured SNPs (Borges et al., 2022). Since the samples for UFAs are all from adults, we aimed to maximize the generalizability of our study by analyzing ADHD as an outcome in both adults and childhood separately. The associations between childhood and adult ADHD and genetic instrument for variants derived from GWAS of ADHD from the Psychiatric Genomics Consortium (PGC) among individuals of European ancestry. Summary statistics for childhood ADHD obtained from a recent GWAS meta-analysis including 38,691 individuals with ADHD and 186,843 controls (Demontis et al., 2023) and for adult ADHD including 6,961 late-diagnosed ADHD and 38,303 controls (Rajagopal et al., 2022). In a recent umbrella review, Kim et al.’s (2020) umbrella review provided a comprehensive investigation into environmental risk factors, protective factors, and peripheral biomarkers for ADHD. This review meticulously cataloged all risk factors associated with ADHD and categorized the evidence of association. To explore the underlying mechanisms genetically connecting the concentration of circulating UFAs and ADHD, we selected risk factors identified as having convincing evidence, including maternal pre-pregnancy obesity, childhood eczema, hypertensive disorders during pregnancy, pre-eclampsia, and maternal acetaminophen exposure during pregnancy (Kim et al., 2020). To explore the underlying mechanisms genetically linking the concentration of circulating UFAs with ADHD, we further investigated these potential confounders for analysis. Genetic effects on hypertensive disorders during pregnancy and pre-eclampsia were derived from the FinnGen database which released in May 2023 (https://www.finngen.fi/en/access_results). The database included samples of 14,727 cases and 196,143 controls for hypertensive disorders during pregnancy, as well as 6,663 cases and 194,266 controls for pre-eclampsia, all of European ancestry. However, the analysis of the other three risk factors, maternal pre-pregnancy obesity, childhood eczema, and maternal acetaminophen exposure during pregnancy, could not be achieved as their phenotypes were not found. Details of all GWASs included in our study were described in Table 1.
Details of the GWASs Included in the Mendelian Randomization.
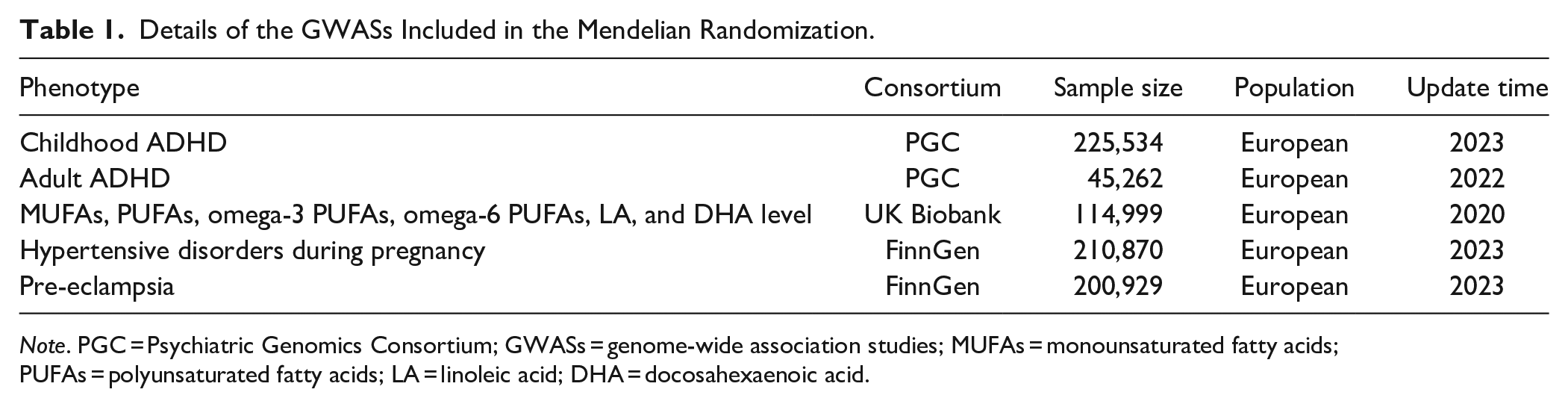
Note. PGC = Psychiatric Genomics Consortium; GWASs = genome-wide association studies; MUFAs = monounsaturated fatty acids; PUFAs = polyunsaturated fatty acids; LA = linoleic acid; DHA = docosahexaenoic acid.
Selection of Genetic Instruments and Steigering Filtering
All relevant SNPs selected as genetic instruments met the widely accepted threshold of 5 × 10−8 (Sadik et al., 2022; Wong et al., 2023). Linkage disequilibrium (LD) clumping was performed on the candidate instrumental SNPs to identify independent ones (r2 < .001 within 10,000 kb). Subsequently, the exposure and outcome datasets were harmonized to determine the genetic instrument effects on the concentration of circulating UFAs and remove SNPs not available in both the exposure and outcome. The strength of instruments for exposures was assessed by the proportion of variance (R2) explained by the SNPs and the F statistic with SNPs having an F statistic >10 generally considered as sufficiently strong instruments for MR analysis (Pierce et al., 2011). Next, to safeguard against potential distortion of causation due to reverse causation, we applied the Steiger filtering method, where a significance level of p < .05 signifies that the causal effect direction is from the exposure to the outcome (Hemani et al., 2017).
Mendelian Randomization Analyses
Four distinct approaches of MR (namely: random-effect inverse-variance weighted (IVW), MR Egger, weighted mode, and weighted median) were performed to investigate the causality between the concentration of circulating UFAs and ADHD. IVW was the primary outcome, allowing for the calculation of the magnitude of causal effects without individual-level data (Burgess et al., 2015). To ensure the consistency of the effect and reduce the impact of overlapping SNPs, one should compare the assessed causal effect acquired by IVW approach with the results procured by MR Egger, weighted mode, and weighted median. MR-Egger permits any genetic variant to have a pleiotropic effect, however, this effect must be not influenced by the variant-exposure association (Bowden et al., 2015). The weighted median analysis enables the utilization of potentially unreliable instruments, assuming that at least half of the instruments employed in the study are reliable, thus providing a causal effect estimate without bias by taking the median of the weighted ratio estimates (Bowden et al., 2016). The weighted mode method identifies less pronounced causal effects compared to IVW, but exhibits reduced bias and lower rates of type-I errors (Hartwig et al., 2017). If fewer than 3 instrument variants were extracted, the Wald ratio was employed to gauge the resultant connection (Bowden et al., 2015).
Sensitivity Analyses
Sensitivity analysis has been essential in MR research to uncover pleiotropy and the disparity of MR estimates can be drastically undermined. Firstly, we employed Cochran’s Q tests to explore heterogeneity within the IVW approach, where a significance level of p < .05 indicated the presence of heterogeneity. Additionally, we utilized the MR-Egger intercept and the MR-Pleiotropy Residual Sum and Outlier (MR-PRESSO) methods to test and address potential horizontal pleiotropy among the selected instrumental variables (Bowden et al., 2015; Verbanck et al., 2018). The MR-Egger method helped evaluate underlying directional pleiotropy, with a statistically significant intercept suggesting violations of the instrumental variable suppositions (Bowden et al., 2015). MR-PRESSO encompassed three components: detecting horizontal pleiotropy, correcting for horizontal pleiotropy by removing outliers, and examining significant differences in resultant evaluations before and after outlier correction (Verbanck et al., 2018). Furthermore, we performed leave-one-out analyses to investigate the impact of individual genetic variants on the results (Burgess & Thompson, 2017).
Risk Factors
To explore the underlying mechanisms genetically connecting the level of UFAs and ADHD, we analyzed potential mediators including hypertensive disorders during pregnancy and pre-eclampsia, based on the results of prior study (Kim et al., 2020). The concentration of circulating UFAs were used as exposure and potential risk factors were taken as outcomes to conduct MR analyses. The main results were estimates of IVW, and a significance level of p < .05 was set.
Statistics
To account for multiple tests, the Benjamini–Hochberg method was employed for false discovery rate (FDR) correction (Q-value) to adjust the p values. The threshold of FDR-adjusted p < .05 was considered as showing evidence of a causal effect. The MR estimates were displayed as odds ratios (OR) with 95% confidence intervals (CI). All calculations were completed by the TwoSampleMR (version 0.5.7), MendelianRandomization (version 0.6.0), and MRPRESSO (version 1.0) packages in R (version 4.3.0).
Results
Initially, we identified 66 SNPs associated with circulating MUFAs level, 66 SNPs associated with circulating PUFAs level, 52 SNPs associated with circulating Omega-3 PUFAs level, 63 SNPs associated with circulating Omega-6 PUFAs level, 48 SNPs associated with circulating DHA level, and 57 SNPs associated with circulating LA level (Supplemental Tables 1–6). Subsequently, we conducted an intersection analysis and harmonized the SNPs with childhood and adult ADHD, resulting in 49 SNPs for circulating MUFAs level, 52 SNPs for circulating PUFAs level, 39 SNPs for circulating Omega-3 PUFAs level, 46 SNPs for circulating Omega-6 PUFAs level, 36 SNPs for circulating DHA level, and 40 SNPs for circulating LA level in childhood ADHD (Supplemental Tables 7–12) and 40 SNPs for circulating MUFAs level, 41 SNPs for circulating PUFAs level, 33 SNPs for circulating Omega-3 PUFAs level, 35 SNPs for circulating Omega-6 PUFAs level, 30 SNPs for circulating DHA level, and 29 SNPs for circulating LA level in adult ADHD (Supplemental Table 13–18). Finally, as shown in Supplemental Table 7–18, the F statistics for these genetic instruments exceeded the commonly selected threshold of 10, indicating the presence of robust instruments (Pierce et al., 2011). Steiger filtering analysis confirmed the correct direction of causal associations. Additionally, we have listed the overlapping SNPs among the six UFAs in both sets of analyses in Supplemental Figures 5a and 5b.
For childhood ADHD, in the MR analysis of six circulating UFAs levels, the IVW analysis indicated a protective causal relationship between PUFAs level (OR = 0.92, 95% CI [0.85, 0.99], p = .031), Omega-6 PUFAs level (OR = 0.90, 95% CI [0.83, 0.98], p = .020), LA level (OR = 0.90, 95% CI [0.82, 0.98], p = .021), and ADHD. Meanwhile, results from other MR approaches indicated a consistent but nonsignifcant direction. However, following FDR correction, the p-value for circulating PUFAs level was all greater than 0.05, none of them reached significance after adjustment. This suggests that the protective effects of these three concentration of circulating UFAs indicators on childhood ADHD are not significant. Additionally, for the circulating MUFAs level (OR = 0.97, 95% CI [0.87, 1.07], p = .512), Omega-3 circulating PUFAs level (OR = 0.95, 95% CI [0.88, 1.02], p = .175), and circulating DHA level (OR = 0.94, 95% CI [0.86, 1.03], p = .172), the IVW analysis did not reveal a significant causal relationship with ADHD. All of the MR analysis outcomes are presented in Figure 2a and Supplemental Table 19.
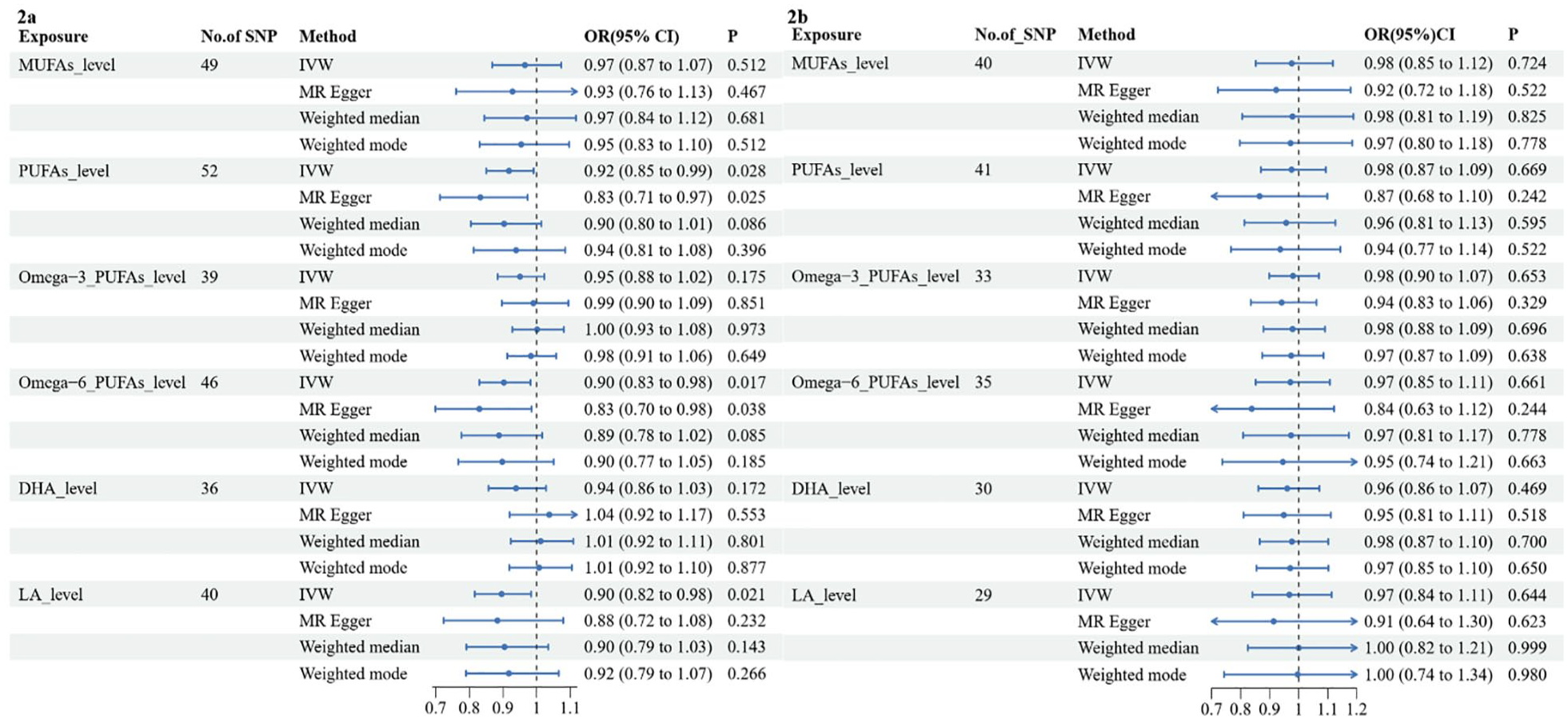
Causal effects for circulating unsaturated fatty acids levels on childhood (a) and adult (b) ADHD.
For adult ADHD, however, we did not find any significant associations between the six circulating UFA levels and adult ADHD. Specifically, the IVW results were as follows: the circulating MUFAs level (OR = 0.98, 95% CI [0.85, 1.12], p = .724), PUFAs level (OR = 0.98, 95% CI [0.87, 1.09], p = .669), Omega-3 circulating PUFAs level (OR = 0.98, 95% CI [0.90, 1.07], p = .653), Omega-6 PUFAs level (OR = 0.97, 95% CI [0.85, 1.11], p = .661), circulating DHA level (OR = 0.96, 95% CI [0.86, 1.07], p = .469), and LA level (OR = 0.97, 95% CI [0.84, 1.11], p = 0.644). The results of all the MR analyses are shown in Figure 2b and detailed in Supplemental Table S20.
For childhood ADHD, to assess the robustness of the aforementioned nominally significant findings, a series of sensitivity analyses was employd, including MR-Egger intercept test, MR-PRESSO global test and Cochran’s Q test (Table 2). Firstly, both the MR-PRESSO test and the MR-Egger intercept test did not reveal any evidence of horizontal pleiotropy (all p > .05), except for circulating DHA level where the MR-Egger intercept test yielded a p-value of .026. The MR regression slopes and individual causal estimates for each SNP are presented in Supplemental Figures 1 and 2. Second, the p-values from the heterogeneity Q test were all greater than .05, except for the DHA level (Q = 51.30, p = .037). However, this did not undermine the MR assessments as the random-effect IVW method employed in the present research, which helps mitigate the aggregated heterogeneity. Thirdly, leave-one-out analyses demonstrated that no single SNP significantly influenced the causal assessments (Supplemental Figure 3). Additionally, the funnel plot exhibited symmetry, suggesting the absence of pleiotropy (Supplemental Figure 4). For adult ADHD, since no significant causal relationships were found, further sensitivity analyses and pleiotropy tests were not conducted.
Sensitivity Analysis of the Causal Association Between the Concentration of Circulating Unsaturated Fat Acids Level and the Risk of Childhood ADHD.
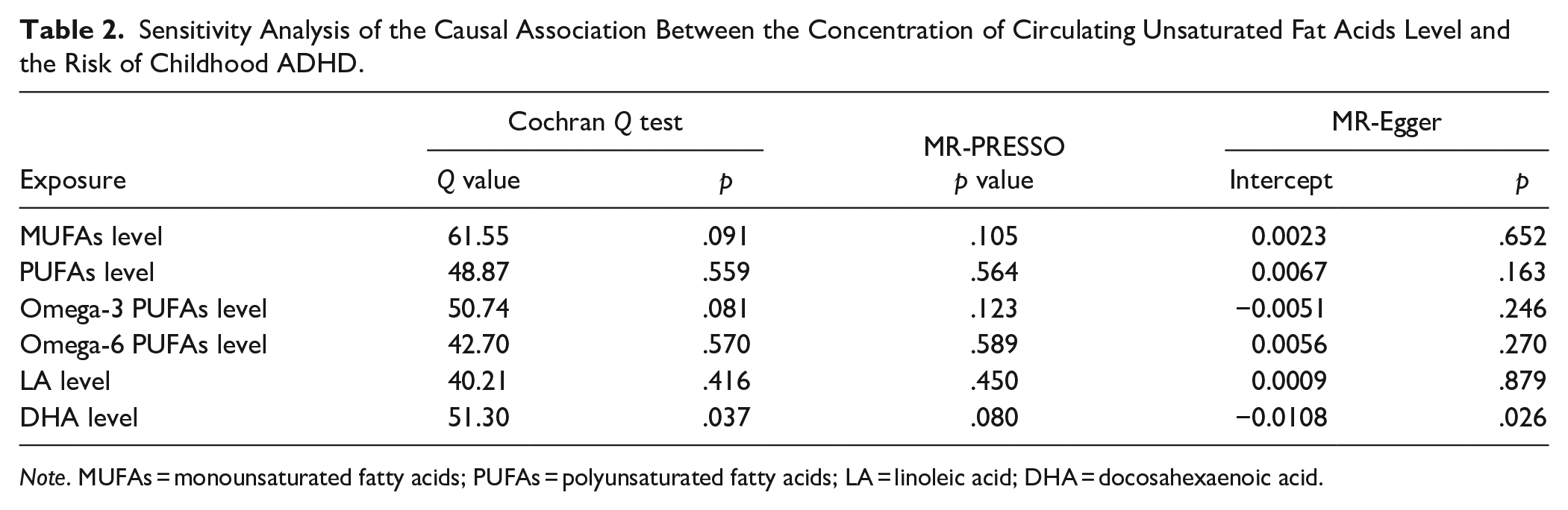
Note. MUFAs = monounsaturated fatty acids; PUFAs = polyunsaturated fatty acids; LA = linoleic acid; DHA = docosahexaenoic acid.
To examine whether the nominally significant estimates were confounded by pleiotropic pathways related to ADHD, we employed the IVW method to assess the causal link between the concentration of circulating PUFAs, Omega-6 PUFAs, LA, and the aforementioned two convincing risk factors for ADHD, namely hypertensive disorders during pregnancy and pre-eclampsia. As presented in Supplemental Table 21, no causal effects were detected between circulating PUFAs, Omega-6 PUFAs, LA levels, and the potential risk factors for childhood ADHD.
Discussion
To our knowledge, this is the first extensive two-sample MR analysis aimed at comprehensively assessing the causal impact of different circulating UFAs levels on ADHD incidence. However, our findings have not yielded evidence supporting the causal role of genetically predicted circulating PUFAs level, Omega-6 PUFAs level, and LA level in relation to the risk of ADHD.
The relationship between the concentration of circulating UFAs and ADHD remains unclear. However, evidence from studies at the organizational level suggests that Omega-3 polyunsaturated fatty acids (PUFAs) and Omega-6 PUFAs are abundantly present in the brain (Mallick et al., 2021), accounting for approximately 35% of brain lipids (Yehuda et al., 1999). Sufficient levels of brain DHA and LA are crucial for normal cellular processes, such as transmembrane potential, neurotransmission, and ion channel function (Luchtman & Song, 2013). Furthermore, alterations in brain fatty acid composition, metabolism, and the signaling systems derived from fatty acids are closely associated with mental disorders (Bazinet & Layé, 2014; Mallick et al., 2021). Hence, it has been widely believed that supplementing UFAs in fetuses and infants can enhance brain development and function, improve cellular information processing, promote normal brain development, and even prevent or ameliorate mental disorders (Willatts et al., 1998), particularly ADHD, which is closely related to neurodevelopment.
However, more studies have yielded inconsistent findings on this matter (Makrides et al., 2014; Nevins et al., 2021). Limited evidence suggests that plasma levels of DHA and Omega-3 PUFAs are lower in individuals with ADHD compared to those without the condition, but the existing evidence is not convincing (Gao et al., 2022). However, the strength of this evidence is weak, and has low credibility (Gao et al., 2022). A recent study published in the Cochrane Library examined the effects of UFAs supplementation on ADHD symptoms. This comprehensive investigation included 37 trials with over 2374 participants. The findings indicate that there is no significant improvement in ADHD symptoms when comparing PUFAs supplementation to a placebo. While there is some evidence suggesting a potential benefit of PUFAs in improving ADHD symptoms in children and adolescents, the credibility of this evidence is low (Gillies et al., 2023). Therefore, the current evidence from basic research, case-control studies, and randomized controlled trials (RCTs) suggests a complex relationship between UFAs levels and ADHD (Bazinet & Layé, 2014; J. P. Chang et al., 2018; Makrides et al., 2014).
When the genetic impact on exposure shifts over time, the MR estimate doesn’t straightforwardly align with any causal parameter and definitely isn’t a valid estimate of the lifespan effect. Variations in genetic effects throughout lifespan complicate MR analyses. Our two-sample MR study separately examined the relationship between the concentration of circulating UFAs levels and childhood and adult ADHD. Ultimately, no causal relationship between UFAs and ADHD was found in either the childhood or adult ADHD populations. This suggests from a genetic perspective that UFAs may not have a long-term effect on ADHD incidence. However, it is important to note that this conclusion is limited to the specific indicators of circulating UFAs levels we included in our study, namely MUFAs, PUFAs, Omega-3 PUFAs, Omega-6 PUFAs, LA, and DHA.
Meanwhile, our study suggests a nominal causal relationship between the concentration of circulating PUFAs, Omega-6 PUFAs, and LA with ADHD. This may be attributed to the complexity of UFAs composition, particularly evident in PUFAs. PUFAs can be further divided into omega-3 PUFA, commonly found in fish, and omega-6 PUFAs, commonly found in vegetable oils. Omega-3 PUFAs includes alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), and DHA, while Omega-6 PUFAs include LA and arachidonic acid (AA; Gao et al., 2022). Due to limitations in data sources (Borges et al., 2022), our study did not include ALA, EPA, and AA, which are important indicators. Previous research on ADHD has often focused on total omega-3 PUFAs and omega-6 PUFAs (J. P. Chang et al., 2018; Hawkey & Nigg, 2014; Nevins et al., 2021), overlooking the investigation of their subcategory indicators, which could provide important pathways for understanding the potential causal relationship with ADHD. However, in our analysis, we only found a nominal causal relationship with LA, but no causal relationship between DHA and ADHD. Future research should incorporate indicators such as ALA, EPA, and AA to provide a more comprehensive understanding of the potential causal relationship between UFAs and ADHD.
Although our findings suggest no direct causality between the concentration of circulating UFAs and ADHD incidence, it is possible that UFAs may have an effect on the progression of ADHD (Moon et al., 2016). To investigate this, we included previously identified risk factors strongly associated with ADHD, such as pre-eclampsia and pregnancy hypertension (Kim et al., 2020), as confounding factors in our analysis. The results showed that for the nominally significant outcomes of circulating PUFAs level, Omega-6 PUFAs level, and LA level, the IVW analysis revealed no significant relationship with the highest recommended risk factors: pre-eclampsia and pregnancy hypertension. This once again indicates that UFAs not only lack a direct causal relationship with ADHD but also do not exert an indirect influence on ADHD through known risk factors. However, due to a lack of GWAS data on other highly correlated risk factors for ADHD, such as maternal pre-pregnancy obesity and overweight, acetaminophen exposure, and childhood atopic diseases (Kim et al., 2020), the relationship between the concentration of circulating UFAs and these risk factors remains unexplored. Future studies can focus on gathering data in these areas to comprehensively investigate the complex mechanisms between UFAs and ADHD.
Our study has several advantages. Firstly, by utilizing the MR design, we can simulate randomized controlled trials in observational settings, which is generally accepted as the most reliable method for determining causality. MR studies can effectively reduce confounding biases by using single-nucleotide polymorphisms (SNPs) randomly assigned at conception, while avoiding the issue of reverse causality that is common in other observational studies. Second, to generate reliable MR estimates, we selected robust genetic instruments (F > 10), excluded SNPs correlated with the outcome, and employed clustering. We also assessed the directionality pleiotropy through MR Egger analysis and conducted leave-one-out analysis to evaluate whether the MR estimates were biased by individual SNPs. Lastly, our findings, along with previous research, could potentially influence health care policies regarding UFAs and ADHD. Stimulant medication, particularly methylphenidate, is often prescribed for ADHD (Hales et al., 2018), but it may have limited efficacy for some patients and is associated with a range of serious adverse events, such as psychosis and arrhythmias (Storebø et al., 2018), as well as nonserious side effects such as decreased appetite, weight loss, insomnia, stomachache, headache, and irritability (Punja et al., 2016; Salazar de Pablo et al., 2023). Thus, families may seek alternative treatments, such as UFAs supplementation. However, our results, which suggest that there is no causal relationship between UFAs levels and ADHD, do not support the supplementation of UFAs as a potential alternative treatment.
This study has some limitations. It is important to note that while genetic variants are indeed fixed, their relationships with phenotypes often vary with age (Labrecque & Swanson, 2019). Although we analyzed the relationships between childhood and adult ADHD with UFAs, the lack of GWAS data for childhood UFAs means that our study cannot completely rule out the influence of age on the results. Future GWAS studies need to consider including populations from different age groups. Additionally, all the participants were Europeans, thus the connection between the concentration of circulating UFAs and ADHD in other population is still unknown. Furthermore, due to the lack of related data, the association between ALA, EPA, and AA levels and ADHD could not be studied (Borges et al., 2022), which is a possible research area in the future. Finally, we must be mindful of the diversity among people with ADHD since UFAs may be causal for a certain type of ADHD (Thapar & Cooper, 2016), Therefore, a comprehensive study with subgroups of ADHD should be considered in the future.
Conclusion
This is the first comprehensive MR study that uncovers relationships between the concentration of circulating UFAs and ADHD. Our study does not support a causal relationship between the concentration of circulating UFAs and ADHD. These findings provide etiological evidence that aligns with previous research, which suggests that supplementing UFAs does not have a significant therapeutic effect on improving ADHD symptoms. Moreover, and perhaps more importantly, UFAs may not exert a long-term impact on ADHD incidence. Lastly, further research is needed to explore the complex genetic mechanisms underlying ADHD.
Supplemental Material
sj-docx-1-jad-10.1177_10870547241264660 – Supplemental material for Absence of Causal Relationship Between Levels of Unsaturated Fatty Acids and ADHD: Evidence From Mendelian Randomization Study
Supplemental material, sj-docx-1-jad-10.1177_10870547241264660 for Absence of Causal Relationship Between Levels of Unsaturated Fatty Acids and ADHD: Evidence From Mendelian Randomization Study by Zuxing Wang, Hongru Zhu, Lili Chen, Chenyu Gan, Wenjiao Min, Jun Xiao, Zhili Zou and Ying He in Journal of Attention Disorders
Supplemental Material
sj-xlsx-2-jad-10.1177_10870547241264660 – Supplemental material for Absence of Causal Relationship Between Levels of Unsaturated Fatty Acids and ADHD: Evidence From Mendelian Randomization Study
Supplemental material, sj-xlsx-2-jad-10.1177_10870547241264660 for Absence of Causal Relationship Between Levels of Unsaturated Fatty Acids and ADHD: Evidence From Mendelian Randomization Study by Zuxing Wang, Hongru Zhu, Lili Chen, Chenyu Gan, Wenjiao Min, Jun Xiao, Zhili Zou and Ying He in Journal of Attention Disorders
Footnotes
Acknowledgements
We wish to acknowledge the participants and investigators of the UK Biobank, the Psychiatric Genomics Consortium (PGC) and the FinnGen database.
Author Contributions
All authors contributed toward the design of the study. ZXW and HRZ collected and transcribed data for analysis. ZXW performed the analysis, with input from CLL, CYG, WJM and JX. ZXW, ZLZ, and YH wrote the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Sichuan Science and Technology Program (2024NSFSC1564 and 2020YJ0457), Science and Technology Department of Sichuan Province (grant number 2021YJC0440), and the Sichuan Provincial People’s Hospital Translational Medicine Fund (2021LY02).
Supplemental Material
Supplemental material for this article is available online.
Data Avilability Statement
All data used in the current study are publicly available GWAS summary data.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.