
Abstract
Background:
Sleep problems are common in adults with ADHD and may be bidirectionally associated with ADHD severity and other psychiatric symptoms. We investigated the prevalence of positive screenings for various sleep disorders, and their association with psychiatric comorbidities in a large sample of adults with ADHD from a specialized outpatient clinic.
Methods:
We included data of 3,691 adult patients diagnosed with ADHD, who had filled out a screener for sleep disorders (Holland Sleep Disorders Questionnaire (HSDQ)) as part of routine diagnostic assessment. The HSDQ screens for the sleep disorders insomnia, parasomnia, hypersomnia, circadian rhythm sleep disorders (CRSD), restless legs syndrome (RLS)/periodic limb movement disorder (PLMD), and sleep-related breathing disorders (SBD). As delayed sleep phase syndrome (DSPS) is very frequent in ADHD, we additionally screened for DSPS. Psychiatric comorbidities were diagnosed through clinical assessment and the Mini International Neuropsychiatric Interview (M.I.N.I.) Plus, which assesses 26 psychiatric disorders following the classification of the DSM-5. All data were retrieved from the electronic patient files.
Results:
Mean age was 35.4 and 49.4% of the patients were female. About 60% of the adults with ADHD screened positive for any sleep disorder. Highest prevalences were found for symptoms of DSPS (36%), insomnia (30%), and RLS/PLMD (29%). Sleep problems in adults with ADHD were associated with comorbid depression, anxiety, substance use disorder, personality disorder, and post-traumatic stress disorder.
Conclusion:
Adults with ADHD often report sleep problems, which are associated with specific psychiatric comorbidities. Systematic screening for sleep disorders in adult patients with ADHD can contribute to a better understanding of their complaints and may aid improved and integrated treatment for the sleep and psychiatric problems.
Introduction
ADHD is one of the most common psychiatric disorders in both children and adults (Ayano, Demelash, et al., 2023; Ayano, Tsegay, et al., 2023). Sleep problems and disorders are highly prevalent in children and adults with ADHD (Cortese et al., 2022; Freeman et al., 2020; Valsecchi et al., 2022). Most studies on this topic have been conducted in children, showing a high occurrence of both subjective and objective sleep disturbances such as sleep onset difficulties, night awakenings and sleep disordered breathing (Cortese et al., 2009). Polysomnographic studies showed that children with ADHD spend more time in stage 1 NREM sleep compared to controls, leading to lighter sleep (Diaz-Roman et al., 2016), and less time in REM sleep, with a longer REM sleep latency (O’Brien et al., 2003). Additionally, children with ADHD more often show symptoms of restless legs syndrome (RLS; Cortese et al., 2005). An intervention study showed that sleep treatment in children with ADHD significantly improved sleep, psychological functioning, emotional, and social wellbeing (Keshavarzi et al., 2014). In adolescents, a recent meta-analysis showed suboptimal subjective sleep such as a longer sleep onset latency and lower sleep efficiency in those with ADHD, as compared to typically developing controls (Marten et al., 2023). Van der Heijden et al. (2005) found a delayed dim-light melatonin onset (DLMO) in children with ADHD and chronic sleep onset insomnia (SOI). The DLMO is a biomarker for the start of melatonin production by the pineal gland. Children may have had SOI as a consequence of late DLMO, that is, a delayed circadian sleep-wake rhythm, although any biological causality cannot be concluded from this study (Van der Heijden et al., 2005).
In adults, there is a limited number of studies on the relationship between sleep problems and ADHD. A meta-analysis of 13 studies in 2018 showed significantly worse subjective sleep parameters, a longer sleep onset latency and decreased sleep efficiency in adults with ADHD compared to those without ADHD (Diaz-Roman et al., 2018). Wynchank et al. (2017) found a wide prevalence of insomnia in adults with ADHD ranging from 43% to 80% (Wynchank et al., 2017), and a recent meta-analysis of 29 studies showed a prevalence of RLS symptoms of 20% to 33% in adults with ADHD (Migueis et al., 2023). Periodic limb movement disorder (PLMD) symptoms were also reported to occur more often in adults with ADHD compared to healthy controls (Philipsen et al., 2005), and symptoms of sleep apnea may be related to ADHD symptoms (Vogel et al., 2017). In a literature review, diagnosed obstructive sleep apnea (OSA), a sleep-related breathing disorder (SBD) was prevalent in 20% to 30% of adults with ADHD (Youssef et al., 2011). Most convincing evidence on sleep disturbances in adults with ADHD has been on the increased prevalence of a delayed sleep-wake rhythm. In 2010, a study conducted by our group showed a 78% prevalence of SOI, related to a delayed DLMO, that is, a delayed sleep/wake cycle, in a consecutive sample of adults with ADHD (Van Veen et al., 2010). Actigraphy and salivary melatonin measurements showed that on average, the DLMO was delayed by 1.5 hours, compared to healthy controls. This delay of 1.5 hours was confirmed by two other studies (Bijlenga, Van Someren, et al., 2013; van Andel et al., 2021). A delayed DLMO is an indication for the delayed sleep phase syndrome (DSPS): a circadian rhythm sleep disorder (CRSD) characterized by a chronic pattern of late sleep and late rise, leading to significant burden in daily life (American Psychiatric Association, 2013). Studies using subjective instruments to measure DSPS, found a lower prevalence of 26% to 33% in adults with ADHD (Bijlenga, van der Heijden, et al., 2013; Spera et al., 2020). It has to be stated that besides biological mechanisms, also cognitive-emotional or behavioral mechanisms may be involved in the delay of melatonin secretion in ADHD. A study showed that, in a general population of adolescents and young adults, bedtime procrastination is associated with worse sleep outcomes such as social jetlag and daytime sleepiness (Li et al., 2020). However, this has not been studied in relation to ADHD and melatonin production.
The clinical presentation of sleep problems and that of ADHD can be similar and may share a common neurobiological etiology (Bijlenga et al., 2019; Owens, 2005). For example, due to their fragmented sleep, children with OSA may experience behavioral problems such as impulsivity, decreased attention span and hyperactivity. These symptoms overlap with the characteristics of ADHD, adding risk to a misinterpretation of their symptoms as ADHD, thereby overlooking the possibility of OSA in these children (Tsai & Huang, 2010). The result is inadequate treatment, persistence of symptoms, and aggravation of the patient’s symptoms (Spera et al., 2020). This is also seen in the study by Fidan and Fidan (2008), which found that tonsillectomy in children with SBD and ADHD resulted in a decrease of ADHD-related symptoms.
Not only ADHD, but also other psychiatric disorders are associated with sleep problems. As 65% to 89% of adults with ADHD has at least one psychiatric comorbid disorder, these comorbidities should be taken into account when describing sleep problems in adults with ADHD (J. J. Kooij et al., 2012; Sobanski, 2006). Several literature reviews showed particularly high prevalences of substance use disorder, mood disorders, anxiety disorder, and personality disorder in adults with ADHD (Choi et al., 2022; Sobanski, 2006), most of which being individually associated with sleep problems (Freeman et al., 2020). For instance, persons with depression or an anxiety disorder often suffer from insomnia (Morin, 1996). In these associations, insomnia is both a predictor for and a core symptom of depression and anxiety (Baglioni et al., 2011; Johnson et al., 2006). Also, relative circadian phase delay (i.e., an evening chronotype) was found to be common in patients with bipolar spectrum disorders, in particular in the depressive episode (Alloy et al., 2017). While most research on sleep in psychiatric disorders is focused primarily on insomnia, less is known about the occurrence of other sleep disorders, such as DSPS, RLS/PLMD, and SBD across psychiatric disorders. In a recent study in The Netherlands, the Holland Sleep Disorders Questionnaire (HSDQ) was assessed in large groups of various adult populations with psychiatric disorders (Mijnster et al., 2023). They found associations between specific sleep problems across the various psychiatric diagnoses (Mijnster et al., 2023). As adults with ADHD have very high psychiatric comorbidity rates (J. J. Kooij et al., 2012), we hypothesize that any psychiatric comorbidity in ADHD is associated with an increased prevalence of specific sleep problems.
The association of sleep problems in children and adults with ADHD is significant: sleep problems are associated with more severe ADHD symptoms and more daytime impairments (Wajszilber et al., 2018). In adults, ADHD symptoms are more severe in those with OSA, RLS, PLMD, and insomnia symptoms, as well as those with an more delayed circadian sleep-wake rhythm (Gamble et al., 2013; Vogel et al., 2017). Moreover, adults with ADHD who suffer from OSA have a lower self-reported quality of life, and more symptoms of depression and anxiety (Oguzturk et al., 2013).
Because a complete description of the prevalence and further characteristics of various types of sleep problems is lacking in literature, this explorative study aimed to examine the prevalence of sleep problems, and their associations with psychiatric comorbidity, in a large group of adults with ADHD from specialized outpatient clinics in The Netherlands. Based on the results of previous literature, we hypothesized that sleep problems are common in adults with ADHD, especially those with psychiatric comorbidity. Because there are sex differences in sleep disorder prevalences in the general population, we also analyzed sex differences in sleep problems in our ADHD population. Insight into these associations can help to improve diagnostics and to contribute to the development of combined treatment possibilities for patients with ADHD, sleep problems, and psychiatric comorbidities.
Methods
Participants
For this cross-sectional retrospective study, routine clinical data were extracted from electronic patient files of patients attending one of 46 locations of the specialized outpatient clinics of the mental health institute Parnassia Groep in The Netherlands, between October 2018 and March 2020. Parnassia Groep is the largest mental health care institute in The Netherlands. All patients had been referred by a general practitioner or mental health care professional for diagnosis and treatment of ADHD and any psychiatric comorbidity, as per standard procedure in The Netherlands. As part of the routine diagnostic assessment, patients filled out the online Holland Sleep Disorder Questionnaire (HSDQ), which screens for the most common sleep disorders. We used data of patients who were 18 years of age or older, had an ADHD diagnosis, and had completed the HSDQ. Data of 4,848 patients were available, of which N = 3,691 fit the inclusion criteria. Data were collected in accordance with the requirements of applicable privacy legislations (GDPR).
Measures
Sleep Problems
The HSDQ is a validated screening tool for the most common sleep disorders: insomnia, circadian rhythm sleep disorder (CRSD), hypersomnia, parasomnia, restless legs syndrome (RLS)/periodic limb movement disorder (PLMD), and sleep-related breathing disorders (SBD; Kerkhof et al., 2013). The questionnaire consists of 32 statements concerning sleep quality and quantity. An individual is asked to answer on a 5-point Likert scale how true the statement is for them, ranging from (1) “not at all” to (5) “completely.” The average total score indicates whether clinically relevant sleep problems (general sleep disorder) are present. Specific sleep disorders are indicated by the average of subscales scores. Subscale cut-off points were 3.68 for insomnia (based on eight items), 2.42 for parasomnia (based on six items), 3.41 for CRSD (based on six items), 2.90 for hypersomnia (based on five items), 2.70 for RLS/PLMD (based on five items), and 2.87 for SBD (based on four items).
Kerkhof et al. (2013) showed that the HSDQ has a high internal consistency (Cronbach’s alpha of .9 for the total score), and a good test-retest reliability (r = .79). It has a high diagnostic accuracy (AUC = 0.95; sensitivity 91%; specificity 86%) and it accurately differentiates between sleep disorders in 84.5% of cases (AUC ranging from 0.69 for insomnia to 0.95 for parasomnia). The subscale for CRSD encompasses multiple disorders related to disturbances in the circadian rhythm, including DSPS, but also others, such as advanced sleep-phase syndrome and shift work sleep disorder. In our clinic, an additional subscale is used to specifically screen for DSPS, as this is the most frequent comorbid sleep disorder in AD(H)D. This subscale is based on two HSDQ items: item 13 “I have difficulty falling asleep at night” and item 26 “I sleep poorly because I don’t manage to fall asleep at a normal hour and wake up at a normal hour in the morning”, with a cut-off value of 3.5 for a positive screening for DSPS. It is important to note that the HSDQ is a screening instrument, not a diagnostic tool. In this article, we therefore use the term “sleep problems” to describe a positive screening on the HSDQ.
Demographic Data, ADHD, and Psychiatric Comorbidity
Demographic data on sex and age were collected through electronic patient files. Our standard diagnostic procedure for ADHD consisted of the semi-structured Diagnostic Interview for ADHD in Adults (DIVA-5), which is based on the diagnostic criteria of the DSM-5 (J. J. S. Kooij, 2021). The DIVA-5 was assessed by a specialized mental health professional. Psychiatric comorbidities were diagnosed by the mental health professional through clinical assessment in combination with the Mini International Neuropsychiatric Interview (M.I.N.I.) Plus version 5.0.0 (Sheehan et al., 1998; van Vliet & de Beurs, 2007). The MINI-Plus is a short structured diagnostic interview that assesses 26 psychiatric disorders following the classification of the DSM-5 (American Psychiatric Association, 2013). For the purposes of this study, we categorized the psychiatric diagnoses into 14 categories; for example, a panic disorder was categorized together with anxiety disorder. The psychiatric categories are: depression, substance abuse, anxiety disorder, phobia, personality disorder, learning disorder, posttraumatic stress disorder (PTSD), eating disorder, autism, obsessive compulsive disorder (OCD), sexual disorder, conduct disorder, psychotic disorder, tic/Tourette’s disorder. All data was collected retrospectively from electronic patient files.
Analyses
Descriptive statistics were applied to describe demographic characteristics of the study population, and the number and frequencies of the HSDQ screenings and psychiatric comorbidities. Differences in prevalence of positive HSDQ screenings between groups (men/women and comorbidity yes/no) were examined using Pearson chi-squared tests. A variable was created to add up the number of sleep disorders patients had screened positive for. As DSPS is a specific subcategory of CRSD, and certain combinations of CRSD’s cannot occur in the same patient (e.g., a delayed and advanced sleep phase) positive screenings for both DSPS and CRSD were counted as one sleep disorder instead of two separate disorders. Mantel-Haenszel tests for trend were used to analyze differences between men and women and between patients with and without psychiatric comorbidity in the number of sleep disorders that the patients screened positive for (range 0–6). Multiple logistic regression models were applied to assess the associations between specific comorbid disorders (as independent variables) and each of the HSDQ sleep disorders yes/no (as dependent variable), taking age and sex into account as possible confounders. As only a small proportion (<1%) of the data was missing, these data were not imputed. Analyses were conducted using IBM SPSS Statistics version 27 (Armonk, NY). Statistical significance was indicated using an α-value of ≤.05.
Results
Patient Characteristics
Data of 3,691 adults with ADHD were used, of whom 1,825 (49.4%) were female, and mean age was 35.4 years (SD = 11.0; Table 1). In total, 60.1% screened positive for any of the sleep disorders, and 36.4% screened positive for multiple (≥2) sleep disorders. Patients most often screened positive for DSPS (35.8%), followed by insomnia (30.6%) and RLS/PLMD (28.8%). Almost half (48.7%) of the patients had any comorbid psychiatric disorder besides a sleep disorder; 26.8% were diagnosed with depression, 11.4% with substance use disorder and 9.9% with anxiety disorder. Of all ADHD patients in our sample, 618 (16.7%) had been diagnosed with a sleep disorder prior to the start of treatment. Of those 16.7%, 82.7% had a diagnosis of CRSD and 82.2% a DSPS diagnosis, followed by 13.4% insomnia, while the proportion of patients with a diagnosis for parasomnia, hypersomnia, RLS and SBD were all below 2%.
Patient Characteristics: Age, Sex, HSDQ Screenings for Sleep Disorders, and Psychiatric Comorbidity.
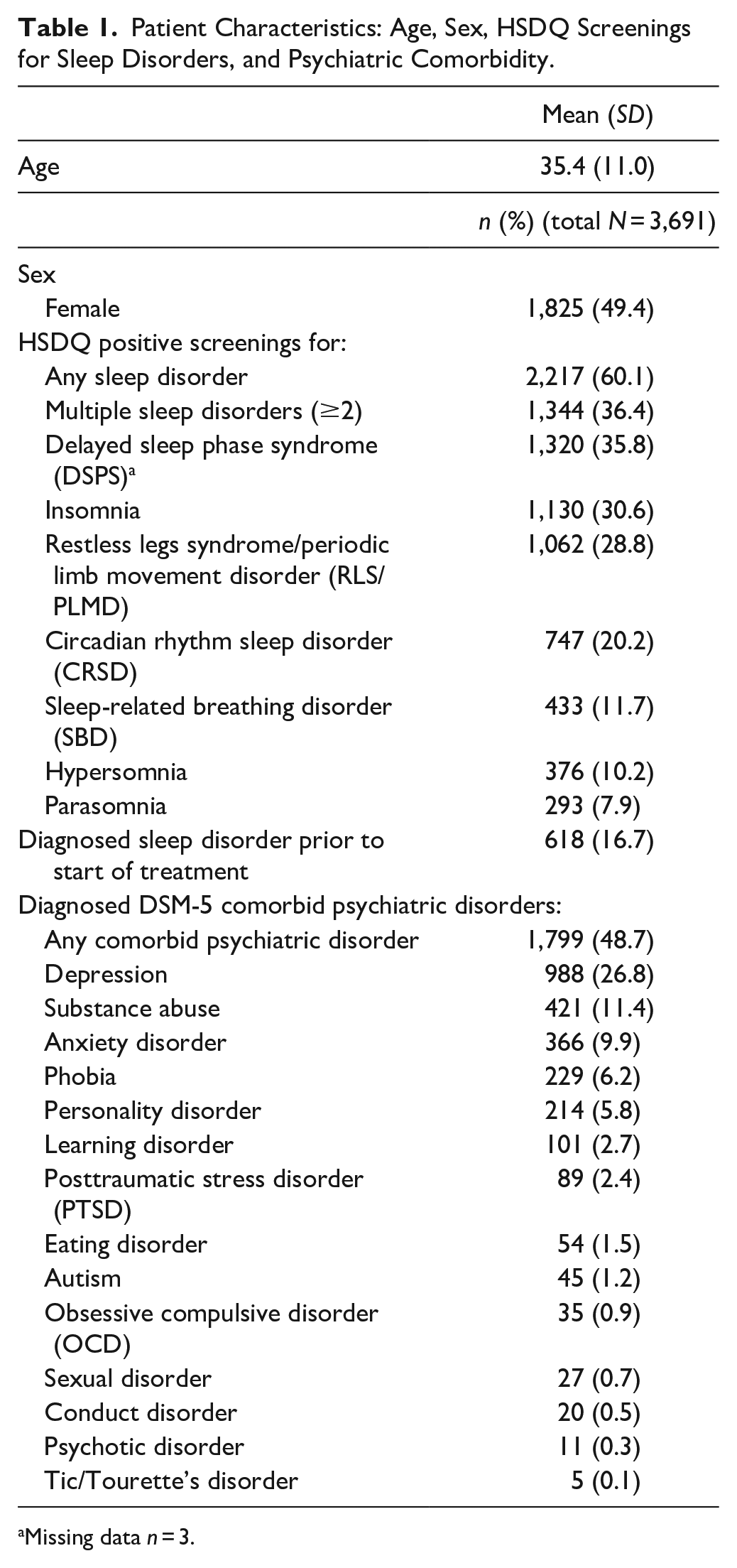
Missing data n = 3.
The frequencies of sleep problems as screened with the HSDQ are shown in Table 2, for the total group, for males and females separately, and per psychiatric comorbidity. Women significantly more often screened positive for any sleep disorder than men (61.8% vs. 58.4%, p = .038). The prevalences of some of the specific sleep problems were significantly higher in women than in men (insomnia: 34.4% vs. 26.9%, p < .001; hypersomnia: 12.1% vs. 8.3%, p < .001; parasomnia 8.9% vs.7.0%, p = .027). However, the prevalence of SBD was higher in men (15.0%) compared to women (8.4%; p < .001). Exploratory post-hoc stratified analyses (Appendix 1) showed that in patients with psychiatric comorbidity, females more often reported symptoms of insomnia and hypersomnia than males. In patients without psychiatric comorbidity, females more often reported general sleep problems, insomnia, hypersomnia, parasomnia, and RLS than males. Males, with and without psychiatric comorbidity, more often reported more symptoms of SBD than females.
Distribution of Sleep Problems per Sex (Male/Female), Psychiatric Comorbidity (Yes/No), With Chi-squared Test Results.

Note. Percentages calculated per column.
Missing data n = 3.
Patients with psychiatric comorbidity significantly more often screened positive for any sleep disorder compared to those without psychiatric comorbidity (67.5% vs. 53.0%, p < .001). Prevalences of all specific types of sleep problems were higher in the group with any comorbid psychiatric disorder (all p < .001). Exploratory post-hoc stratified analyses (Appendix 2) showed that the associations between psychiatric comorbidity and all of the sleep problems were present in both males and females.
Mantel-Haenszel tests for trend showed a significantly higher number of positive HSDQ screenings (sleep problem types) in patients with psychiatric comorbidity, compared to patients without comorbidity (χ2 = 116.273, df = 1, p < .001). Moreover, women significantly more often had a higher number of positive screenings compared to men (χ2 = 4.392, df = 1, p = .036).
The prevalence of positive HSDQ screenings per comorbid psychiatric disorder are shown in Table 3. Overall, those with any psychiatric comorbidity had an OR of 1.84 (95% CI [1.61, 2.10], p < .001) for any positive screening for a sleep disorder compared to those without psychiatric comorbidity. The highest odds for a positive HSDQ screening were observed in patients with PTSD, who had an OR of 3.21, compared to those without PTSD (95% CI [1.76, 5.86], p < .001). Odds for a positive HSDQ screening were also significantly higher for ADHD patients with depression (OR = 1.73, 95% CI [1.47, 2.03]), substance use disorder (OR = 1.76, 95% CI [1.40, 2.21]), anxiety disorder (OR = 1.51, 95% CI [1.18, 1.92]), and personality disorder (OR = 1.54, 95% CI [1.12, 2.11]) compared to the ADHD patients without these comorbid disorders.
Prevalences of Psychiatric Comorbidity in ADHD Patients Without Any Positive HSDQ Screening Versus Those With a Positive HSDQ Screening, With Odds Ratio (OR) and 95% CI or Fisher’s Exact Test, N = 3,691.
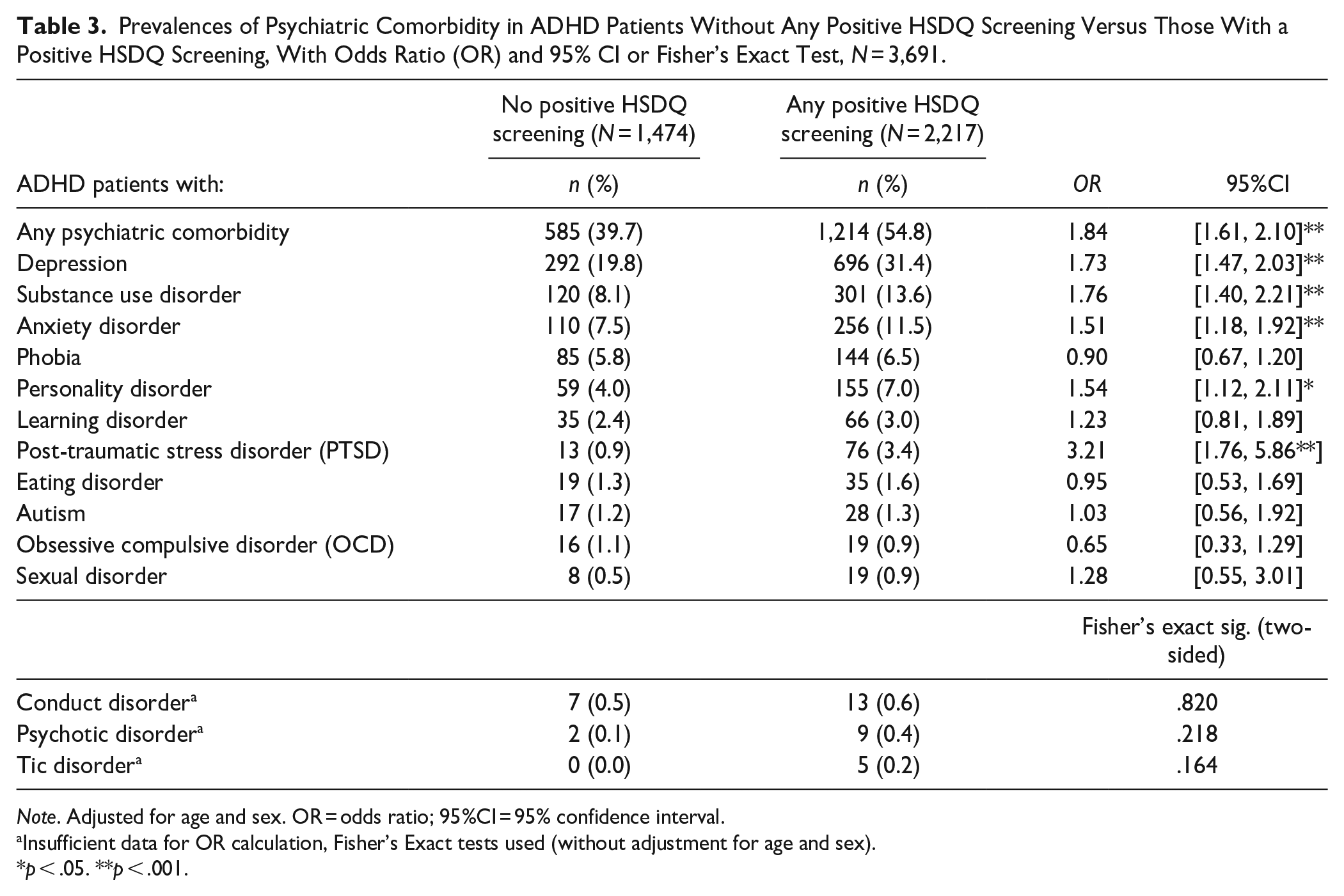
Note. Adjusted for age and sex. OR = odds ratio; 95%CI = 95% confidence interval.
Insufficient data for OR calculation, Fisher’s Exact tests used (without adjustment for age and sex).
p < .05. **p < .001.
Discussion
This cross-sectional study aimed to examine the prevalence of sleep problems, and their associations with psychiatric comorbidity in adults with ADHD. The study showed that in adults with ADHD, the prevalence of self-reported sleep problems is very high, especially in those with comorbid psychiatric disorders. Specifically, comorbid PTSD, depression, anxiety, substance use disorder, and personality disorder were associated with an increased prevalence of sleep problems. Additionally, female ADHD patients and those with comorbid psychiatric disorders report more types of sleep problems than men or patients without any psychiatric comorbidity.
More than half (60.1%) of the ADHD patients in our sample screened positive for a sleep disorder, in particular DSPS (35.8%), insomnia (30.6%), and RLS/PLMD (28.8%). These numbers are substantially higher compared to those in the general population of The Netherlands: 0.13% to 3.1% for DSPS, 8.2% for insomnia, and 12.5% for RLS/PLMD (Kerkhof, 2017; J. J. Kooij & Bijlenga, 2013). Our results are largely in line with those of previous research on the prevalence of sleep disorders in ADHD. However, we found a lower prevalence of positive screenings for insomnia in ADHD compared to other studies. For instance, Wynchank et al. (2017) found a prevalence of 43 - 80% in their literature review (Wynchank et al., 2017). A possible explanation might be that the accuracy of the HSDQ is limited when distinguishing insomnia symptoms from the symptoms of other sleep disorders, as indicated by a lower AUC of 0.69 for the insomnia subscale (Kerkhof et al., 2013). Another discrepancy with previous literature is the low prevalence of positive screenings for SBD. For instance, Mijnster et al found an SBD prevalence of 22.6% SBD in patients with ADHD, in comparison to our 11.7% (Mijnster et al., 2023). However, these discrepancies may be due to differences in sample size and population characteristics.
In our sample, the male-female ratio was almost 1:1. Although in childhood, ADHD is more commonly diagnosed in men, studies show that these differences between men and women decrease in adulthood to a ratio similar to the one we found in our study (Cortese et al., 2016; da Silva et al., 2020). Women, compared to men, significantly more often screened positive for a higher number of sleep disorders, and specifically more often for insomnia, hypersomnia and parasomnia. Men more often screened positive for SBD. These results are in line with previous results in general and psychiatric populations (Ahlberg et al., 2023; Arnulf et al., 2019; Bollu et al., 2018; Fuller-Thomson et al., 2016; Lin et al., 2008; Nevsimalova et al., 2021). Contrary to results of previous studies in the general population, we found no significant sex differences in the prevalence of RLS and PLMD symptoms. An explanation may be found in the similarities between symptoms: ADHD patients often have the urge to move their legs, which is one of the core symptoms of ADHD; as a result, their scores may have been higher on the RLS/PLMD subscale, in both men and women. Also, low serum ferritin levels are known to be related to RLS, and may be related to ADHD, suggesting that iron-deficiency, may be the bridge between the overall high prevalence of self-reported RLS symptoms in ADHD (Cortese et al., 2008; Xiao et al., 2024).
Comorbid psychiatric disorders, specifically PTSD, depression, anxiety, substance use disorder, and personality disorder, were associated with all sleep problems, and with having multiple types of sleep problems. These results add new insights to previous findings on associations between ADHD and psychiatric comorbidity and between sleep disorders and psychiatric disorders other than ADHD (Choi et al., 2022; Freeman et al., 2020).
Our study provides insight into the prevalence of sleep problems in the adult ADHD population. A strength of this study is its large sample size that is representative of ADHD patients referred for treatment to a mental health institution in The Netherlands. Also, a wide range of psychiatric comorbidities was represented. Therefore, we were able to examine specific associations between psychiatric comorbidity in ADHD and types of sleep problems. However, some limitations must be stated. First, as this was a cross-sectional study, no statements can be made about causality. Also, due to the exploratory nature of this study, it does not provide any information about potential biological and cognitive-emotional processes that could explain the high prevalence of sleep problems in adults with ADHD. Secondly, we used data retrieved from electronic patient files. Some relevant covariates, such as BMI, treatment history and medication, could not be taken into account as they were not systematically recorded in clinical practice. For instance, it would have been interesting to look at BMI as a mediator for SBD, as it is an important factor in the etiology of the disorder (Senaratna et al., 2017). Also, sleep-related symptoms are a part of the diagnostic criteria of several psychiatric disorders (e.g., depression and anxiety). It would have been more accurate to correct for these symptoms in our analyses, to avoid circular reasoning. However, items scores on the MINI-Plus were not available, and could therefore not be corrected for any sleep-related symptoms. Furthermore, our study did not include a control group such as a psychiatric group without ADHD. Therefore, a comparison between the ADHD population and the general population or a population with other primary psychiatric disorders could not be made. Additionally, it should be emphasized that our study population consisted of adults with ADHD who were in care at a specialized mental health clinic. It is possible that these persons experience more severe ADHD symptoms and more psychiatric comorbidity compared to adults with ADHD from the general population or from those seeking general mental health care. Finally, as the HSDQ is a screening tool, measuring self-reported sleep problems, no inferences can be made about actual sleep disorders in our population.
Conclusion
Adults with ADHD have a high prevalence of self-reported sleep problems. Especially women and those with comorbid depression, anxiety disorder, substance use disorder, personality disorder and PTSD are at increased risk of various types of sleep problems. In order to fully understand the pathways of the associations between sleep disorders and ADHD, with or without psychiatric comorbidity, future studies should include objective sleep parameters such as DLMO, actigraphic, and polysomnographic measures. The present study provides a broad first overview of the scope of the problem and underlines the need for more attention to sleep problems in diagnosis and treatment of adults with ADHD. Treatments for specific sleep problems are available, relatively accessible to implement in ADHD patients and can improve ADHD treatment results substantially.
Footnotes
Appendices
Distribution of Sleep Problems for Stratified Groups: Psychiatric Comorbidity (Yes/No), Stratified by Sex (Male/Female), With Chi-squared Test Results.

| Male (n = 1,866) | Female (n = 1,825) | |||||
|---|---|---|---|---|---|---|
| Psychiatric comorbidity | Psychiatric comorbidity | |||||
| HSDQ sleep problem type | Comorbidity n (%) | No comorbidity n (%) | χ2, p | Comorbidity n (%) | No comorbidity n (%) | χ2, p |
| Total | 898 (48.1) | 968 (51.9) | 901 (49.4) | 924 (50.6) | ||
| Any sleep disorder | 608 (67.7_ | 482 (49.8) | <.001 | 606 (67.3) | 521 (56.4) | <.001 |
| Delayed sleep phase syndrome (DSPS) a | 378 (42.1) | 282 (29.1) | <.001 | 376 (41.7) | 284 (30.8) | <.001 |
| Insomnia | 302 (33.6) | 200 (20.7) | <.001 | 370 (41.1) | 258 (27.9) | <.001 |
| Restless legs syndrome (RLS)/periodic limb movement disorder (PLMD) | 299 (33.3) | 221 (22.8) | <.001 | 293 (32.5) | 249 (26.9) | <.001 |
| Circadian rhythm sleep disorder (CRSD) | 241 (26.8) | 138 (14.3) | <.001 | 216 (24.0) | 152 (16.5) | <.001 |
| Sleep-related breathing disorders (SBD) | 152 (16.9) | 128 (13.2) | .025 | 99 (11.0) | 54 (5.8) | <.001 |
| Hypersomnia | 100 (11.1) | 55 (5.7) | <.001 | 131 (14.5) | 90 (9.7) | <.001 |
| Parasomnia | 89 (9.9) | 41 (4.2) | <.001 | 100 (11.1) | 63 (6.8) | <.001 |
Note. Percentages calculated per column. HSDQ = Holland Sleep Disorders Questionnaire.
Missing data n = 3.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.