
Abstract
Notwithstanding the deployment of tools to standardize delivery processes, public–private partnerships (PPPs) have encountered significantly different experiences across a broad spectrum of applications during their long-term contractual phase—including those in Ontario Canada, one of the world’s most active PPP markets. This article conducts an in-depth case study of the PPP for the new Bridgepoint Active Health care Hospital, an award-winning 464-bed hospital and administration facility delivered using a design–build–finance–maintenance PPP. This article reveals the role of personalities, relationships, and strong leadership in bringing a successful project to fruition in the face of complex, intersecting challenges. In this context, the PPP is only one variable in explaining the overall success of this complex and highly visible social infrastructure project.
What explains the success—and high-profile failure—of public–private partnerships (PPPs) used to deliver social infrastructure? In mature PPP jurisdictions, tools derived from financial, legal, and economic theories have been used to structure public and private relationships to deliver social infrastructure incentives (Tribilcock & Daniels, 1996). Notwithstanding the deployment of such tools to standardize delivery processes, PPPs have encountered significantly different experiences (Hodge et al., 2010). These variations have prompted the growth of frameworks grounded in governance to better understand PPP outcomes (Kiljn & Koppenjan, 2015). This article contributes empirical research to evaluate how dimensions of nuanced governance is, or is not, influencing project success and failure through a comprehensive case study of a large social infrastructure PPP delivered in Ontario, Canada.
As one of the world’s most active PPP jurisdictions, Ontario has delivered over C$45 billion in infrastructure through an arm’s length government procurement agency, Infrastructure Ontario (I/O), (I/O, 2018). I/O has sought to refine, standardize, and promote PPP processes to deliver infrastructure on time and on budget, particularly as it pertains to social infrastructure. One notable PPP is the new Bridgepoint Active Healthcare hospital facility, a 464-bed hospital and administration facility delivered through a design–build–finance–maintenance (DBFM) PPP.
Bridgepoint Active Healthcare (Bridgepoint) opened a new facility in 2013 using I/O’s (2009c) standardized PPP process. However, the success of this social infrastructure PPP extends well beyond procurement and delivery processes. In addition to achieving on time and on budget completion (Hanscomb, 2015), the facility was instrumental in stimulating community-level revival and health care transformation, while also assisting in Bridgepoint’s strategic positioning and serving as a template for future social infrastructure.
This article undertakes a comprehensive case study of Bridgepoint to identify variables contributing to the outcomes of this social infrastructure PPP. This reveals that the experience of Bridgepoint involves a complex narrative that extends beyond the PPP process, ranging from a government closure notice, challenging capital markets environment, and tensions to defy standard PPP processes. In addition to Bridgepoint’s subsequent merger with a larger health care network just 3 years after the opening of the new facility, these findings offer insight into the success of complex social infrastructure PPPs. This case study reveals the importance of analyzing personalities, relationships, and leadership in bringing a complex project to fruition. PPPs are only one part of an overall strategy to achieve public sector goals.
This article will present these findings as follows. The section “Governance as a Framework for Understanding PPP Outcomes” will summarize governance literature contributing to boarder discussions about the factors that influence PPP outcomes. The section “Delivering Social Infrastructure in Ontario Using PPPs” will introduce the context for delivering social infrastructure in Ontario using PPPs. The Ontario health care experience will be introduced in the section “The Health care Experience in Ontario” followed by this article’s methodology in the “Method” section. The section “The New Hospital as a PPP” will analyze the Bridgepoint experience. The section “Bridgepoint as a Case Study on Infrastructure Governance” will conclude with a discussion on the lessons that can be learned in promoting successful social infrastructure PPPs.
Governance as a Framework for Understanding PPP Outcomes
PPPs continue to gain attraction globally as governments attempt to address growing infrastructure needs (Breadley et al., 1996). The use of PPPs is premised on the theory that arrangements between the public and private sectors can mitigate certain risks in the design, construction, maintenance, and operation of infrastructure on a more cost-effective basis when compared with government-led forms of procurement (Grimsey & Lewis, 2007). PPPs are often used when governments seek to transfer risks that they acknowledge they cannot manage efficiently, wish to retain the expertise of the private sector in areas in which they admit they are deficient, or want to link capital and operating cost, so-called “life cycle” costing, through a long-term contractual arrangement (Boardman & Vining, 2012; Yescombe, 2014).
Despite the final “P” in its acronym, PPPs are not partnerships in a business sense, rather they are a complex set of legal agreements that bind key participants to the process over a specified period of time (Siemiatycki, 2015b). It is the complexity of contractual relationships between a public entity and one or more private entities, as well as the performance of these contractual relationships over long time periods, that make PPPs distinctive from government-led approaches to the delivering public infrastructure (Hussain & Siemiatycki, 2018).
Much of debate on the efficacy of PPPs revolves around the cost of private capital and whether the cost of using private capital is commensurate with the public savings when risks are transferred to the private sector. Academic research has focused on the value for money (VfM) proposition, an a priori calculation of potential public savings that is predicated on various assumptions used to compare the proposed PPP with what is called the Public Sector Comparator, a comparison based on a government-led procurement approach (Siemiatycki & Farooqi, 2012).
In the absence of consensus on the postproject VfM methodology (Hodge & Boardman, 2010), literature has emerged exploring the processes, relationships, and structures that develop in the process of delivering and managing infrastructure (Organisation for Economic Co-Operation and Development, 2015). This is paralleled by academic theories that seek to identify the role of interorganizational and cross-sectoral relationships in the formation of infrastructure governance systems (Kiljn & Koppenjan, 2015). Social infrastructure development involves complex decision-making processes among a wide variety of stakeholders (Flyvbjerg, 1998). Due to this complexity, unexpected outcomes may arise, as well as intense conflicts that are not easily resolved, especially with legal tools (Flyvbjerg, 1998). Rather, the interdependencies of stakeholder networks based in patterns of social relations can offer a framework for analyzing how actors coordinate to form policy, implement solutions, and deliver services. Known as networked governance, this body of literature has emerged to adapt public governance frameworks to understand the nuances of infrastructure projects (Kiljn & Koppenjan, 2015).
PPPs offer a unique opportunity to examine whether the outcomes of large-scale public expenditures can be explained using governance literature alongside traditional frameworks from law and economics. This article seeks to contribute empirical research in this area by examining whether these concepts can explain the outcomes of social infrastructure PPPs in Ontario.
Delivering Social Infrastructure in Ontario Using PPPs
Canadian PPPs borrowed heavily from lessons learned in both Australia and the United Kingdom and applied internal PPP experiences across Canadian provincial governments (Murphy, 2008). Provincial governments are the most active PPP originators in Canada. These governments are generally conscious of widespread political aversion to “privatization” of public assets or the delivery of public services (Hodge & Greve, 2007). Early in the PPP adoption cycle, many politicians avoided use of the term public–private partnership and some created their own acronyms to disguise what was still a PPP (Loxley & Loxley, 2010). Ontario PPPs are driven by the need to transfer certain risks that governments are not adept at mitigating; they are not seen as a model to replace public funding with private capital (Cory, 2016). Within this frame, PPPs have consistently received political support from Ontario governments (Siemiatycki, 2015).
The success of Canadian PPPs can be attributed to several factors (Table 1):
Success in Canadian PPPs.

Note. PPP = public–private partnership.
These factors offer insight into how the Canadian market has emerged as one of the world’s most stable and consistently productive infrastructure markets. Ontario has led the way with a strong pipeline of PPP projects. Much of this has expertise that has been developed from delivering social infrastructure PPPs, specifically new health care facilities across the province through its special purpose procurement body, namely, I/O.
The Health Care Experience in Ontario
Ontario relies exclusively on a publicly funded health care system whereby the province funds the delivery of health care services from its general treasury (Vader & Deber, 1984). Ontario hospitals are governed and mostly funded by the province while doctors remain as private entities who rely on government for payment of patient fees. Hospitals are generally quasiprovincially owned, regulated, and funded. While publicly funded, hospitals are run by independent boards of directors (the Board), charged with overseeing the quality of patient care, to undertake complex building programs, control capital costs and delivery times, and keep abreast of new trends and technologies (Canadian Medical Association [CMA], 2010). Hospital Boards hire a CEO and all personnel, and grant hospital privileges to doctors (Vader & Daber, 1984).
This model emerged to balance the tension of the province, seeking to exert control over hospitals, while respecting hospital independence. Over the decades, this model has became focused on the objectives of controlling the ever-expanding cost of delivering health care services, rationalizing scarce resources, avoiding duplication of services, standardizing delivery systems, and addressing patient needs across regions (CMA, 2010). During this time, the province was increasingly wary of the capability of hospital boards to undertake complex building programs, control capital costs (which were often well over budget) and delivery times, and keep abreast of new trends and technologies (CMA, 2010). This became evident in the early 1990s, prompting drastic action to restructure the hospital sector. A significant part of any strategy was hospital closures, consolidation of smaller hospitals, building new state-of-the-art facilities, and standardization of key functional elements, as well as the incorporation of new technologies (CMA, 2010). This initiative paralleled a similar review across all asset classes owned and managed by governments, including jails, courthouse, schools, and specialized facilities such as laboratories (Loxley & Loxley, 2010).
To implement these changes, the province sought to explore the use of PPPs to manage the delivery and management of hospital infrastructure. A sensitive issue was structuring the PPP in a way that did not appear to “privatize” the delivery of health care, nor undermine the autonomy of hospital boards, doctors, and unionized hospital staff. Approaching new hospital construction with the PPP model met strong initial resistance from hospital boards who saw this as direct provincial intervention into their affairs (Cohn, 2008).
PPPs prevailed, as there were few options available to address the significant cost overruns that plagued new hospital construction. In 1999, the province launched Superbuild Corporation, and this was the first reference to PPPs in Ontario (Ministry of Finance, 2000). To quote the minister at the time, The SuperBuild Corporation represents a new and fresh approach to government capital planning . . . It is an approach anchored firmly in the belief that public-private partnerships can help build public infrastructure in the province in the most cost-effective and productive manner possible.
In 2003, the Ministry of Public Infrastructure Renewal was created into which SuperBuild was folded. The new ministry went through several transformations and, in 2005, I/O was formed as a government agency with a primary role in procuring infrastructure, including engaging in traditional public sector forms of procurement and PPPs. I/O remains Ontario’s procurement authority for health care projects employing the PPP framework (Canadian Construction Monitor, 2019).
Table 2 summarizes health care PPPs delivered by I/O that achieved Commercial Close between 2006 and Q1 2017, and representing various degrees of risk transfer to private concessionaires based on the model applied (Hussain & Siemiatycki, 2018). It is within the context of PPPs in the hospital sector in Ontario that the following case study is examined.
Ontario Health Care Infrastructure PPPs, 2006 to Q1 2017.
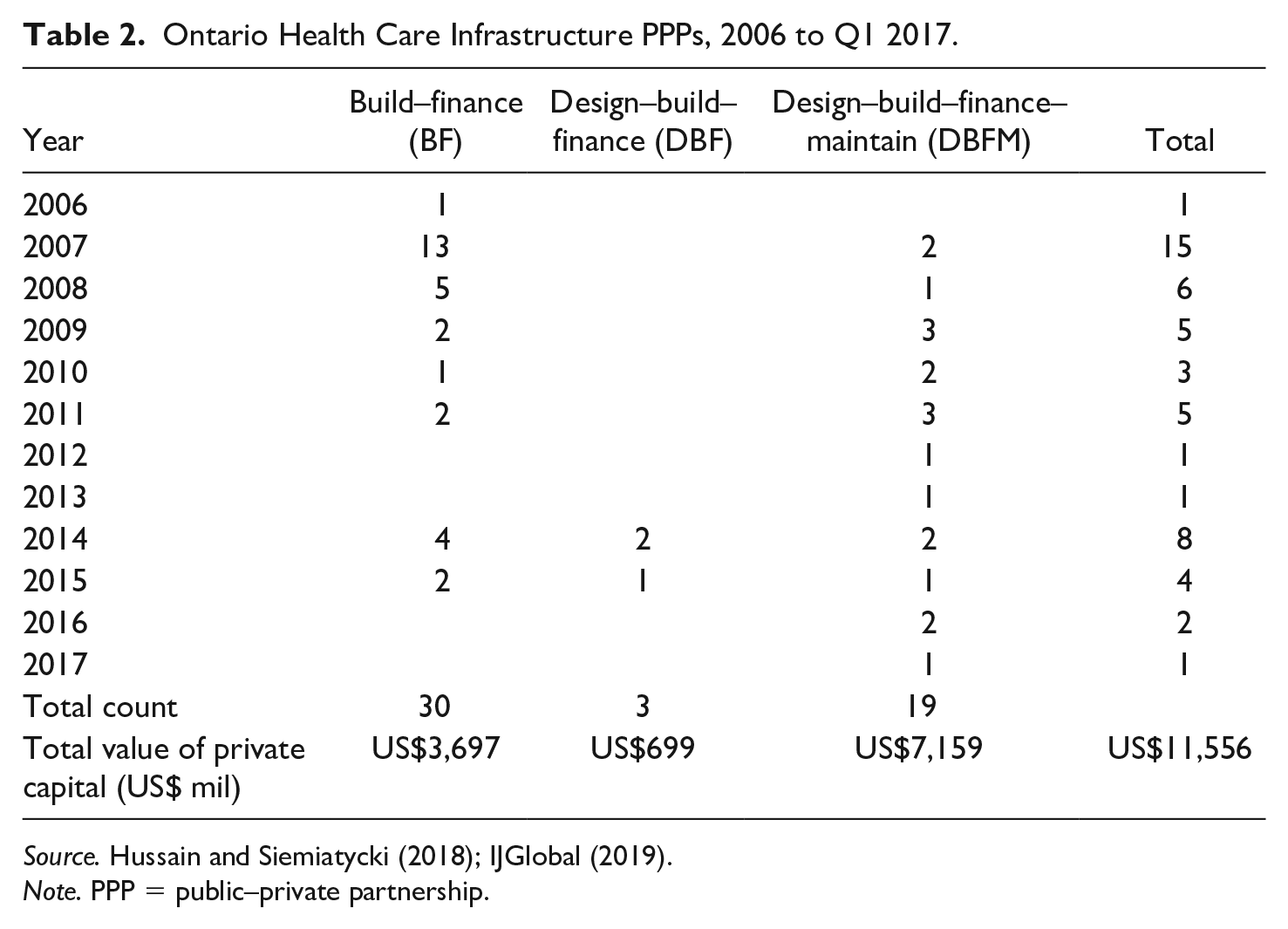
Note. PPP = public–private partnership.
Method
To understand Bridgepoint’s PPP experience, a comprehensive case study was undertaken. This critical case was selected because it can offer a glimpse into a successful social infrastructure PPP that faced numerous complexities (Flyvbjerg, 1998). At the time, the Bridgepoint PPP, which was Ontario’s largest DBFM, experienced the effect of global financial crisis (GFC) when seeking to obtain private capital and was to be developed in an existing built area (as a brownfield PPP). The Bridgepoint PPP has been used as a template for subsequent DBFM projects in Ontario and abroad. However, the success of this PPP cannot be understood without examining the context for the conception, development, and management of the new hospital.
The case study was completed by conducting a literature and archival review of key policy submissions, project documents, private sector agreements, and financial disclosures spanning back to late 1990s. It is supplemented by over 40 semistructured interviews conducted from 2013 to 2019 with government officials, hospital board members and senior management, private contractors, advisors, politicians, and stakeholders involved in the Bridgepoint PPP. Several interviews were repeated years into the PPP’s operation to triangulate findings.
The New Hospital as a PPP
Founded in 1860, Bridgepoint is an integrated health care organization offering specialized care for people living with the effects of stroke, dementia, brain injuries, neuro-generative diseases, diabetes/dialysis, HIV/AIDS, fracture/trauma, and major postoperative complications (Bridgepoint Active Healthcare, 2019). The new PPP hospital and administrative facility opened in June 2013 at a cost of C$1.2 billion 1 for the brownfield redevelopment, which at the time was one of Canada’s largest urban brownfield projects and social infrastructure PPPs (I/O, 2009). The 472 bed, 680,000 sq ft, state-of-the-art facility was delivered under a 35.5-year DBFM contract with a private sector consortium.
Pre-PPP Development
In 1997, Marian Walsh, Bridgepoint’s then president and CEO, faced a formidable challenge, namely, how to save Bridgepoint’s health care facilities, given that the Ontario government directed the closure of Bridgepoint’s existing hospital and transfer of patients to other long-term care facilities. Bridgepoint did not fit into the government’s strategy to reallocate hospital beds through the closure and consolidation across Ontario. Bridgepoint held few options: it occupied a functionally obsolete hospital, sat upon leased land from the City of Toronto, was stigmatized by being adjacent to one of the most notorious jails in Canada (the Don and Toronto Jail), and had insufficient funds for a new facility.
Bridgepoint’s then CEO, with the backing of the board, sought to reverse the Ontario government’s decision to close the existing hospital. Following an intensive public education campaign launched by Bridgepoint, focused on the unique specialized needs of complex patients, the Ontario government reversed its closure order in 2001 and directed that Bridgepoint proceed with a “modest redevelopment plan.” The struggle to succeed from 2001 onward can be grouped into five categories: land assembly, the planning and approvals process, building the hospital with PPPs, historic preservation, and community engagement. According to Walsh, the common thread was to “earn a social license” from the many stakeholders likely to be involved to provide health care through a new hospital facility (Interview, 2017).
Land Assembly
For Bridgepoint to build a new hospital facility, it would have to control adjacent lands that were owned by different levels of government. The City of Toronto (City) owned the land upon which the former hospital stood, an adjacent land parcel dedicated to a lawn bowling club; and another parcel through the Toronto Community Housing Corporation (a City-owned social housing provider) which contained 15 units of affordable housing. The City also owned the existing streets and Riverdale Park immediately north of the site.
The province owned the Don Jail lands, which included the original historic jail and a more recent addition called the Toronto Jail, plus two houses associated with the Jail that were also historically listed properties. All historic structures, with the exception of the lawn bowling clubhouse, were largely vacant and in very poor condition with limited prospects for adaptive reuse (City of Toronto, 2002). The Toronto Jail was still in use and prisoners could not be relocated until a new facility was completed in another part of town (I/O, 2009b).
Although the key planning document, the Master Plan, for the site was not available at the time, Bridgepoint decided it would be in its best interests to purchase the Don Jail lands from the Ontario government and lands from Toronto Community Housing to have some control over the site and its potential use, while also having some flexibility from a planning and site density perspective (Toronto Community Housing, 2011). Ultimately, Bridgepoint entered into a complex land exchange agreement with the City and provincial governments that enabled the realization of a new Master Plan (Appendix A). This Plan included the footprint for a new hospital building, new city roads, a new city park, and renovated heritage buildings, with most of the land now owned fee simple by the hospital.
Notwithstanding provincial jurisdiction over health care, Bridgepoint had to manage municipal bodies to approve its planned redevelopment of the site. Whether or not the existing hospital building should be preserved became a contentious issue that was appealed to a planning adjudication tribunal. Overlaying the necessary land arrangements was a complex regulatory process that required Toronto City Council to approve the land deal, heritage easements agreements, a comprehensive Master Plan, Official Plan Amendment, Rezoning Application, Plan of Subdivision, and a Development Agreement, all of which required extensive public consultation (Urban Strategies, 2005).
The various agreements and approvals collectively resulted in a new pattern of land ownership, a complex sequencing of development, adaptive reuse of the designed historic structures as administration facilities, the eventual demolition of the existing hospital building and the Toronto Jail, construction of new streets and pedestrian walkways, and a new public park (Appendix B).
In addition to managing the planning process, Bridgepoint had to secure approval for a new hospital facility. The fate of the Don Jail and timing for removal of the Toronto Jail rested with the province, which also had full control over building a new facility. The province was clear that a new hospital would only be built through the use of the PPP model, and only then if positive VfM could be demonstrated (Infrastructure Ontario, 2007). 2 In 2006, the Ontario Ministry of Health and Long-Term Care (MOHLTC) approved Bridgepoint’s Master Plan Business Case, recommending it be delivered as one of the province’s first complete DBFM with the procurement support of I/O. What made Bridgepoint different from other PPPs was that it was a brownfield situation, whereas most of Ontario’s PPPs for social infrastructure were “greenfield,” on stand-alone developments. This distinction created new opportunities but made the process more complex and time-consuming.
Brownfield Redevelopment
The business case guiding the redevelopment of this brownfield site had to offer something for all stakeholders to gain approval. First, a new use had to be found for the Don Jail, Correctional Services had to initiate plans and build a new remand center before they could move existing prisoners (a project that also used the PPP model). Second, the local community wanted improved parks, roads, and bike paths (see City of Toronto, 2010a, City of Toronto 2010b). Third, a new facility had to be designed and built. Fourth, Bridgepoint had to oversee the removal of the existing facility, which involved opposition from some local groups and architectural interests. All of this was overlaid by approval processes that extended from the MOHLTC and the Ministry of Infrastructure to various City departments, compounded by an ever-changing political landscape at the City and provincial levels. At each stage, Bridgepoint had to align itself with each stakeholder group, secure its support, and attempt to deliver the value that each would expect in return for its support (Table 3). Where support was lacking, Bridgepoint had to consider its next best move.
Bridgepoint Stakeholder Matrix (Pre-PPP).

Note. PPP = public–private partnership; MOHLTC = Ministry of Health and Long-Term Care; I/O = Infrastructure Ontario.
Bridgepoint’s board understood that implementation was a combination of strategy and tactics, relying upon strong leadership, good team players, keen judgment, and a long-term commitment to serve the broad public interest. The board realized that it “could not satisfy everyone and at the same time achieve its vision; it would have to draw the line somewhere when two issues became potential ‘deal breakers’” (Interview-Planning Consultant, 2013). For example, the City’s heritage planner required all bars on the windows of the historic Don Jail be retained when repurposing it into an administrative building. Bridgepoint’s Board felt that this was incompatible with adaptive reuse for hospital staff. The matter was eventually decided by City Council. Bridgepoint prevailed with an agreement to preserve the bars on the ground floor. This battle consumed more than 6 months in the development timeline.
Design and Stakeholder Negotiation
To garner support from community groups, medical professionals, patients, and hospital staff, Bridgepoint’s board and the City agreed that exceptional architecture was critical. At an early design stage, the Minister of Infrastructure commented that the new building “looked too good” and would be seen as wasteful of taxpayer money (Interview-Government Official, 2013). He requested a modified design. Then there was a surprising decision by the minister to cancel the entire project in response to cost concerns. Bridgepoint’s then CEO responded in a matter of weeks with significant design changes and a revised cost estimate that prompted the minister to reverse his decision. A final threat was the collapse of global capital markets that jeopardized the future of the PPP model (below).
Subsequent discussions with MOHLTC officials, City Planning staff, and the surrounding community resulted in a request that Bridgepoint come forward with a comprehensive proposal that would include a new hospital that would integrate the historic Don Jail, now owned by Bridgepoint. Bridgepoint retained consultants to facilitate the development of “A Master Plan for Bridgepoint Health—Don Jail Site” that was submitted to MOHLTC in July 2004. In parallel, submissions were made to City Planning officials. A comprehensive approach to redevelopment was supported by the City Council in December 2005 (City of Toronto, 2005). Following an appeal that consumed over a year, the City and Bridgepoint agreed that that the irregular land parcel could be planned by Bridgepoint (OPA & Rezoning Application and Subdivision, 2006). It was within this Master Plan that a PPP would be construed to demolish the existing hospital, reconfigure the Don Jail, and build a new hospital facility and surrounding parks/roads/bike lanes.
Configuration of the PPP
Bridgepoint was beholden to the PPP process that was prescribed and controlled by I/O through to the point of occupancy. This forced Bridgepoint staff, executive team, and board to keep abreast of a fast moving and complex process that they were experiencing for the first time. At the time, Bridgepoint was one of the first hospital boards in Ontario to be involved in a complex risk sharing arrangement using PPPs. The PPP involved a series of activities to be completed by Bridgepoint (and not I/O), the first of which was the preparation of the new hospital’s Function Program, adhering to guidelines issued by I/O and MOHLTC. This program was completed in 2006 and, once approved by MOHLTC, set the stage for a new facility in terms of scope, cost, and performance. Bridgepoint also selected initial project consultants; provided project management; managed contracts during construction, transition, and operation phases; and processed all approvals and payments, all under the guidance of I/O.
The learning curve for staff was challenging, risky, technically complex, and highly controlled (Interview-I/O Staff, 2014). Although much of the construction risk is transferred to the private sector within the PPP model, Bridgepoint was obligated to share certain risks with the ongoing facility management (FM) of the site through a 35.5-year PPP contract. There was the additional challenge of understanding a complex financial structure that was in transition. One hospital senior staff member referred to the process as “the RFP Olympics, requiring training, stamina, focus, and determination to win” (Interview-Bridgepoint Staff, 2014).
PPP Award
Plenary Health Bridgepoint LP (Plenary Health) was awarded the contract to design, build, finance, and maintain the new hospital and repurpose the Don Jail under the PPP. The PPP contract comprised of approximately 51 months of construction and a 30-year facility maintenance agreement (Table 4). The total expenditure was estimated at C$1.27 billion over the 30 years, equivalent to approximately C$622 million in 2009 dollars (I/O, 2009).
Composition of Private Sector Counterparty.

Source. Infrastructure Ontario (2009).
Under the terms of the PPP contract, Plenary Health agreed to
Design and build the facilities in compliance with Project Specific Output Specifications (PSOSs);
Finance the construction and capital costs of the facilities over the term;
Obtain a third-party independent certification that the facilities are built in compliance with the contract;
Provide FM and life cycle maintenance for the facilities for the 30-year service period under established performance standards; and
Ensure that, at the end of the contract term, the building meets the conditions specified in the contract (I/O, 2009).
Capital Markets and Project Delivery
The PPP contract was executed in two parts. At the time of Commercial Close, all legal documents are executed and signed, with the exception of the financial documents. At Financial Close, the cost of financing is confirmed and private capital flows to Plenary Health (I/O, 2009). The time between Commercial Close and Financial Close was intended to be a matter of days. Unfortunately, for Bridgepoint, the GFC occurred during that period and jeopardized the PPP process.
Prior to the GFC, a large portion of private financing for Canadian PPPs was provided by European banks (IJGlobal, 2019). European banks were willing to lend for the long term, whereas Canadian banks were averse to the perceived risks of long-term lending. When the GFC occurred, long-term credit was not available from these sources and the interest rate differential between government lending and private financing widened by as much as 30 bps on Canadian infrastructure deals (Hussain & Siemiatycki, 2018). For Ontario PPPs seeking Financial Close, long-term debt providers were abandoning their commitment to reach financial close, including the Bridgepoint PPP. 3
In response to the absence of private capital to reach financial close, I/O and Bridgepoint were required to explore different approaches to identify capital for this and subsequent DBFM projects (Table 5). A solution emerged from the collaboration among the infrastructure developers, banks, and other financial institutions, driven in large part by the Ontario government’s unwavering support for PPPs. The solution applied to the Bridgepoint PPP involved a combination of bank debt from several Canadian banks, in what was called a “club deal,” and bonds privately placed with Canadian institutional investors sought to introduce temporary liquidity into the Canadian PPP market (I/O, 2015). 4
Bridgepoint Stakeholder Matrix (During GFC).

Note. GFC = global financial crisis.
To achieve Financial Close on the Bridgepoint PPP, changes were introduced to the PPP payment mechanism to offer a large payment to Plenary Health following construction to discharge private construction lending (Hussain & Siemiatycki, 2018; Table 6). In parallel, I/O changed its procurement processes to reduce the time between commercial and financial close such that it can now occur in a matter of hours (Cory, 2016). As well, the province’s step actively attracted institutional private capital that is willing to lend over long time periods through infrastructure bonds provided that the transfer of risks to private consortiums were well understood and strictly managed (Interview-Private Sector Participant, 2016). The latter also saw the emergence of construction companies providing their own capital into projects on the basis that they have a better understanding of construction risks (Hussain & Siemiatycki, 2018).
Break down of Financing Sources.

Source. Standard and Poor’s (2009).
Note. SPV = special purpose vehicle.
Commissioning and Operation
During the summer of 2013, Bridgepoint moved its patients into the new state-of-the-art hospital. In the months that followed, construction commenced of new streets, bicycle and pedestrian ways, a large public park and an adjoining palliative care center, and demolition of the last vestiges of the jail. In addition, the conversion of parts of the jail into administrative offices and demolition of the existing hospital occurred. The site also incorporated four new development sites to accommodate up to four private mixed-use buildings “to weave the project back into the fabric of the community” (Interview-Site Plan Consultant, 2013) and offer a source of revenue should Bridgepoint choose to sell them in the future (Interview-Bridgepoint Staff, 2018). The vision began to materialize: to create a new hospital site that rejuvenated the community by welcoming community members to utilize the new hospital building as the anchor and catalyst for local change (Alvaro & Kostovski, 2014).
Under the contract, Bridgepoint is obligated to make monthly payments to Plenary Health, based on performance requirements. Bridgepoint was not required to advance any funds until the new hospital building reached substantial completion (Infrastructure Ontario and Bridgepoint Hospoital, 2009). Monthly service payments then commenced (more than 30 years) to cover the balance of construction, maintenance, operations, and lifecycle replacement costs.
Johnson Controls LP (JCLP), as the service provider for specific FM services, provides a help desk, plant and utilities management services, security, running parking services, and some minor services for the new facility’s retail.
Table 7 illustrates that, of the typical C$4.88 million in annual service payments relating to FM services, JLCP receives the larger share. The average operations and maintenance (O&M) annual payment is called the monthly base payment (MBP). Deductions can be made to the MBP, up to a maximum in any one month, as a result of performance failures. These deductions are categorized into availability failure deductions, service failure deductions, and quality failure deductions (I/O, 2009). Each deduction results in the allocation of failure points, the accumulation of which can lead to warning notices, the exercising of remedial rights, subcontractor replacement, and ultimately Plenary Health’s default under the PPP contract (Standard & Poor’s, 2009; Infrastructure Ontario and Bridgepoint Hospital, 2009).
Plenary Health Bridgepoint LP—Service Payments and Operating Costs.

Source. Standard and Poor’s (2009).
Note. FM = facility management; CPI = consumer price index; JCLP = Johnson Controls LP; SPV = special purpose vehicle.
During the commissioning phase, the Bridgepoint board was vocal that it wanted continuity of its project teams. Following several personnel turnover from Plenary Health during the PPP’s construction phase, the Bridgepoint board refused to accept any further changes to the private sector’s project management team (Interview-Private Sector Participant, 2016). This team was required to work with the team formed with Bridgepoint personnel, and that team could not be modified until the new hospital was complete (Interview-Bridgepoint Management, 2017). Following commissioning, effort was undertaken by both Plenary Health and Bridgepoint to retain personnel or have an FM project team formed using individuals who shadowed members of the construction project teams (Interview-Bridgepoint Management, 2017). In addition, both undertook to establish ongoing relationships to manage issues that arose during building operation. Bridgepoint’s then CEO was vocal that these relations “were formed at the most senior levels and the lowest contract management levels so everyone would work together to find solutions” (Interview-Hospital Staff, 2019). This proved true when the facility’s electrical and elevator systems failed. The ability to begin conversations and engage in negotiations prevented the use of payment mechanism deductions specified in the PPP contract.
The use of relationships and communication channels, differing from what is specified in the PPP contract, problematize statements by I/O about the benefits of the structured risk transfer mechanisms the PPP process offers. Despite positive VfM calculations, skepticism remains among the many critics of PPPs that taxpayers benefit from PPPs. In December 2014, a year after occupancy in the new hospital facility, the Auditor General of Ontario issued a report suggesting that ‘traditional’ procurement would be superior to ‘Public Private Partnerships’ if projects were simply ‘managed better’ by government (Auditor General of Ontario, 2014). An assessment by such an esteemed body as the Auditor General of Ontario, which reports directly to the Ontario legislator, underscores the dilemma with PPPs and the extent to which the public sector has come to rely on such a narrow assessment of PPPs.
Project Outcome and Bridgepoint Today
I/O lists Bridgepoint as a successful PPP as the redevelopment was completed on time and on budget. However, it was Bridgepoint’s intent to provide the best in health care for people living with complex illnesses and disabilities, enhance the quality of life for patient, improve operational efficiencies, and enhance access to rehab programs (Alvaro & Kostovski, 2014). In addition, the new facilities sought to address current site deficiencies, improve vehicular and pedestrian access, integrate the site with the community, remove the stigma of the jail, and provide opportunities for expansion (Alvaro & Kostovski, 2014). The City gained “an outstanding piece of public architecture and restoration of one of its most important historic structures” (Interview-Architecture Consultant, 2015).
By implementing the new Master Plan, Bridgepoint made more effective use of public open space and supported the ongoing revitalization of the adjacent community. The new hospital building ensured the retention of more than 1,100 high-quality health jobs in the adjacent community, expanded the taxable assessment base, generates C$880,000 to C$970,000 per year in new tax revenue for the City, and is estimated to generate C$2.5 to C$2.7 million in development charge revenue for the City when the four development sites are disposed of (City of Toronto, 2008). A postoccupancy evaluation found that staff, patients, and medical professionals felt the new facility improves wellness, and ratings of user satisfaction are much higher compared with the former hospital (Alvaro & Kostovski, 2014).
In May 2014, Mount Sinai Hospital (Mount Sinai) and Bridgepoint announced a “voluntary amalgamation,” a step they say will allow for better integrated patient car e (Bridgepoint Active Healthcare, 2015). Mount Sinai is a notable acute care center and university teaching hospital located in Toronto’s downtown medical complex. The amalgamation is a mutually beneficial arrangement that “strengthens the long-term viability of both institutions” (Interview-Mount Sinai Senior Executive, 2015). According to Bridgepoint’s then CEO, the PPP enabled the hospital to procure a new building that attracted attention from other hospital groups seeking to expand into complex medical care (Interview, 2017). Bridgepoint, lacking research capabilities, required a larger network to ensure its long-term viability as a provider of medical excellence. Through strong project management, design excellence, and positive community engagement, Bridgepoint was in a stronger position to negotiate favorable terms with potential hospital partners through the delivery of the new hospital facility (Interview-Bridgepoint Senior Management, 2016). The new hospital group is currently undertaking a complete renovation and upgrading of their downtown facility using a PPP and under the direction of the same staff who managed Bridgepoint’s PPP.
Bridgepoint as a Case Study on Infrastructure Governance
The Bridgepoint experience reveals the broader values related to a PPP exercise that would not be reflected in the VfM exercise; attempts were necessary to identify some of these values and how they were created, by whom, and why. The case involves a piece of social infrastructure where the PPP was a necessary but not sufficient condition to deliver what the public bodies and affected stakeholders expected in terms of value. Understanding and managing preexisting networks of social relations, patterns of behavior, and conflicting incentives were paramount for the leadership of Bridgepoint to build the new hospital. The PPP process pushed these networks into nuanced areas, continuing the objective of realizing broader social value.
There are four ingredients that contributed to the success of this project and leveraged the use of a PPP to deliver a new hospital building and redevelopment of a brownfield site. These ingredients collectively shaped a value proposition that went far beyond building a facility:
A social license to operate. A social license exists when a project has the ongoing approval within the local community and other stakeholders, ongoing approval or broad social acceptance, and ongoing acceptance (Moffat et al., 2016). The result is that community members become advocates of the project as they consider themselves to be co-owners and emotionally vested in the future of the project; such is the strength of self-identification (Interview-Bridgepoint Staff, 2016).
Strong leadership. The importance of this leadership from Bridgepoint’s then CEO cannot be underestimated. Her leadership was embodied in clarity of purpose, tenacity, interpersonal skills, effective communication skills, management of governing bodies, and a vision. Her strong leadership was respected by many stakeholders and became the glue among the project components that transcended legal agreements (Interview-Mount Sinai Senior Executive, 2015).
A clear vision. The vision was driven by two things: first, a commitment to a hospital environment that directly addressed the special needs of various stakeholders, and, second, a commitment to a surrounding community in need of economic and social renewal.
An architectural statement that embodies the vision. This new facility served an important symbolic as well as functional role, extending beyond the physical buildings.
This case also offers a different basis for assessing the success of this social infrastructure PPP. What is missing from the VfM is an assessment of value to the public in delivering services on behalf of taxpayers, whether the ability to deliver these services was enhanced by virtue of this new infrastructure, whether there were additional benefits to those who require these services, and whether there was significant community benefit. If broader benefits exist, they can they be attributed to the credibility and competence of a government agency; the competences of the concessionaire; the contributions of certain organizations, groups, or individuals in key roles; strong leadership or the personalities involved in decision-making roles; or even a strong shared vision among all stakeholders.
The value proposition for Bridgepoint was the investment of its own limited resources, in addition to that of the province, plus a commitment of significant talent and time. It is difficult to quantify the value added in circumstances such as this; however, several features distinguish this project and reinforce the concept of value creation. They include a clear vision aligned with the interests of the various stakeholders, realization that Bridgepoint was not a stand-alone project as are the majority of PPPs in Canada, broad interpretation of Bridgepoint’s health mandate and delivery of value to the community, and recognition that innovation drives the value proposition. Bridgepoint’s leaders were open-minded when it came to the master plan; were permissive, not restrictive when it came to ancillary uses on the site; sought private partners through a competitive public process; and demanded design excellence and protected this excellence through the complex procurement process. They managed political risks and leveraged the PPP in a way that optimized its network of relationships.
Conclusion
This article examines a successful social infrastructure PPP that faced multifaceted objectives extending well beyond the measures traditionally captured by PPP evaluation tools. It provides an opportunity to assess the role of personalities, relationships, and strong leadership in bringing a successful project to fruition in the face of complex, intersecting challenges. From the perspective of public management, the new facilities had an “ultimate” purpose of leveraging a PPP as part of an overall strategy to redefine a health care delivery model for complex long-term patient care. In this context, the PPP is only one variable in explaining the overall success of this social infrastructure project.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.