
Abstract
Italy, as many other countries, adopted the design–build–finance–maintain (DBFMO) Anglo-Saxon model to build new hospitals. This model proved to be rigid, nontransparent, nonvalue for money, and unaffordable. The aim of this article is to analyze the main drawbacks of the traditional DBFMO public–private partnerships (PPP) contract applied to the health care sector, by referring to the Italian experience, and to discuss the evolutions, conceived through an inductive/deductive approach, conducted in a context of deep collaboration between academia, health care authorities, and market players to make PPP contracts more value for money, flexible, and affordable. The article provides also an example of the role of academia in closing the rigor–practice gap by supporting and facilitating an institutional change.
Introduction
The first public–private partnership (hereafter PPP) contract was introduced almost 30 years ago in Australia to build/expand hospitals and manage clinical and nonclinical services. The partnership model was then applied in the United Kingdom, within the so-called private finance initiative (PFI), which allowed the National Health Service (NHS) to replace many old hospitals. PPP was subsequently also later adopted in Canada and in southern European countries, such as France, Italy, Spain, and Portugal (PWC, 2017; Roehrich et al., 2014). In Canada, Italy, and in France, the model chosen was consistent with the PFI model, with some variations to adapt it to specific context. Spain and Portugal, and more recently other emerging countries, decided to also include the clinical service. This article focuses its attention on the dominant PFI model (also called accommodation model; see Barlow et al., 2013), which is based on long-term, privately financed contracts (so-called DBFMO) to design (D), build (B), finance (F), maintain (M), and operate (O) social infrastructure, such as hospitals and schools. Under the DBFMO contracts, the procuring public authority pays a unitary charge, built on a combination of availability charges and service fees, to a special purpose vehicle (SPV) to get the infrastructure built and maintained across the length of the contract, in addition to the delivery of a range of noncore services, such as catering, cleaning, laundry, and the provision of a porter service. The model has been adopted in countries based on a national health care system and/or where it is a prerogative to keep clinical governance and delivery within public hospital authorities. This model can also be adopted in emerging countries where the goal is to prevent the “brain drain” of doctors from public hospital service.
PPP contracts in the health care sector have been analyzed by many, such as development banks and consultancy firms, as well as the world of academia. The former have mainly described the positive aspects of public–private collaboration, whereas the latter have mainly scrutinized critical aspects, such as performance, value for money, and affordability (Hodge & Greve, 2017). Governments, so far, have widely relied on consultancy and legal firms to define, structure, and implement the PPP pipeline. This has generated a depoliticization of not only PPP (Willems & Van Dooren, 2016) but also situations presenting high conflict of interest, as documented by Shaoul et al. (2007). Contrary to other countries, in Italy, which is the focus of this article, the role of big consultancy firms and PPP task forces has been negligible, with academia playing a salient role.
By creating a bridge between research and practice (i.e., through an inductive/deductive research approach), academia has stimulated the generation of some innovation, potentially capable of generating more value for money in PPP. These innovations are (a) the so-called “light model” (Amatucci et al., 2010; Vecchi, 2011; Vecchi & Cusumano, 2012), according to which the PPP contract only includes those noncore services that are consistent with the underpinning investment, and (b) the notion of economic and financial equilibrium (Vecchi & Leone, 2016).
Although the first innovation mainly refers to the health care sector, where, following the U.K. PFI model, many noncore services were included in the contractual perimeter, the second one has general validity and applicability across all sectors in which a PPP contract is applied.
Academia has also engaged the main stakeholders in training and dissemination activities to develop the necessary skills to apply these innovations and to spread a culture of higher sustainability in the use of PPP. Training and dissemination activities have made possible a diffusion and legitimation of these changes, resulting in their institutionalization (Lawrence et al., 2001).
Using a descriptive case study research methodology (Yin, 2006), the aim of this article is to analyze the main drawbacks of the traditional DBFMO PPP contract, adopted within the accommodation model, by referring to the Italian experience, and to discuss the evolution conducted in a context of deep collaboration between academia, health care authorities, and market players, to deliver more value for money, flexibility, and affordable PPP contracts.
This article only focuses on the discussion of reasons beyond the validity of the “light model” in addition to the drawbacks to the standard model that it can solve, that is, overrigidity (Blanken & Dewulf, 2010), nontransparency, lack of value for money, and unaffordability (Vecchi & Hellowell, 2018b). As a matter of fact, the notion of economic and financial equilibrium in PPP has been the subject of other articles (Hellowell & Vecchi, 2012; Vecchi & Hellowell, 2013; Vecchi et al., 2013). 1
Despite being context-dependent, the Italian case could also be of great interest in countries based on a common law system or with different institutional features, given that the “light model” addresses issues that are common across jurisdictions. In reality, the concept of the “light model” can be seen to be one of the founding elements of Private Finance 2 (PF2) in the United Kingdom (HM Treasury, 2012), and was also chosen by one of the leading hospitals in Europe, the Karolinska in Sweden, whose contract was signed in 2010.
This case is an interesting example of closing an academic–practice gap (also known as “rigour-practice” gap) in a field in which academic research has always underlined the need for more competence and empowerment in the public sector (Bloomfield, 2006; Jooste et al., 2011; Jooste & Scott, 2011; Opara et al., 2017; Soecipto & Verhoest, 2018; Vecchi & Hellowell, 2018a). This is also an example of institutional change and institutionalization of new models within a field (e.g., Dacin et al., 2002; DiMaggio, 1988; Greenwood & Hinings, 1993; Oliver, 1991), where academia plays a key role in processes of adaptation, amendment, and improvement of existing practices (Pettigrew & Starkey, 2016).
The article is structured as follows: The section “The First Generation of PPP Contracts in Italy” presents the features of the first wave of PPP contracts in the Italian health care sector; the section “The Research–Training Approach to Support the Innovation of Italian PPP Model for Health Care Investments” discusses the role played by academia through research, training and dissemination to support the institutional change in the PPP field; the section “The Emergence of the PPP Light Model to Overcome the Weaknesses of the DBFMO Contract” discusses the drawbacks of the DBFMO model that can be overcome by the “light model”; and the section “Concluding Discussion” draws a concluding discussion.
The First Generation of PPP Contracts in Italy
Italy has imported the U.K. model (Hellowell & Vecchi, 2015) in which the private operator (an SPV) designs, finances, and builds hospitals, as well as manages a wide array of noncore services (e.g., hard facilities and medical equipment maintenance, energy management, cleaning, catering, laundry, and IT management). The adoption of the PPP model for building new hospitals was initiated at the end of the 1990s, with the revision of the Law on Public Procurement (the so-called Merloni ter). Since then, 20 new hospitals (where “new” stands for newly built, completely renovated, or enlarged) have been realized under PPP contracts up to 2010.
The main driver beyond the introduction of this first generation of PPPs was the shortage of public capital available to renew the network of public hospitals, many of them built at the beginning of the 20th century. In contrast to the United Kingdom, which stood as a reference model for Italy when the PPP was introduced (some of the first contracts were awarded to a British company and British speakers were an unavoidable presence at the first conferences on the topic), PPP was actually used to match public funds available with private capital; a large proportion (often more than 50%) of the upfront capital expenditure was provided by the public sector, both through the so-called “extraordinary program of public investments in health,” or “article 20 program,” 2 and capital contributions from regional governments (Hellowell & Vecchi, 2015).
For those projects that benefited from a large public grant, private capital invested was remunerated through the margins generated by the management of noncore services. For those that received a lower public contribution, the investment was also remunerated through a residual availability charge.
Table 1 reports the main data of the 20 projects of the first generation of PPPs. All but three are completed projects, with these three still being in the final stages of construction. An amount of €2.34 billion was invested with a total of 12,000 hospital beds realized. Investment values are all net of VAT and they include the cost of design, build, and furnishing.
The First Generation of PPPs in the Italian Health Care.
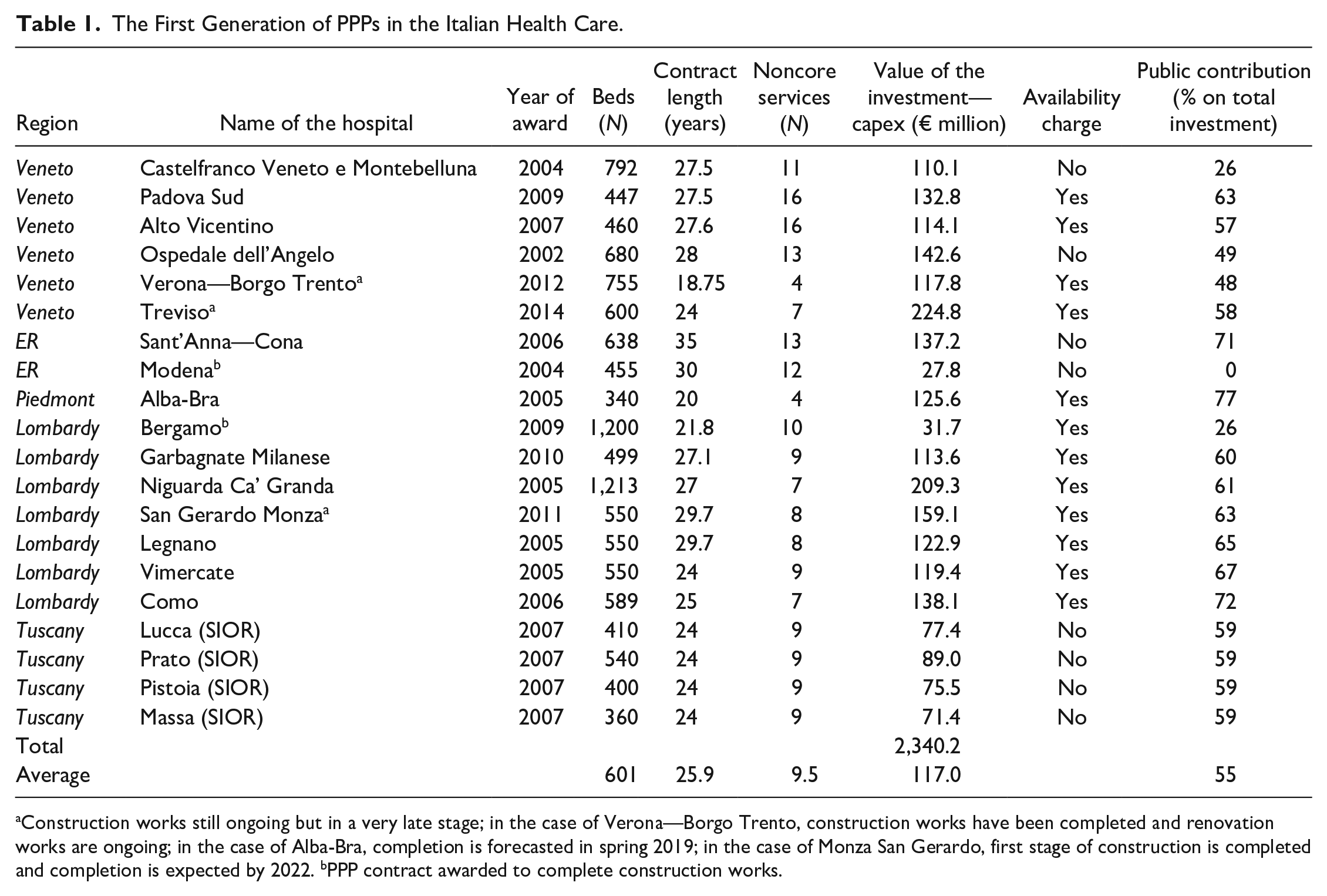
Construction works still ongoing but in a very late stage; in the case of Verona—Borgo Trento, construction works have been completed and renovation works are ongoing; in the case of Alba-Bra, completion is forecasted in spring 2019; in the case of Monza San Gerardo, first stage of construction is completed and completion is expected by 2022. bPPP contract awarded to complete construction works.
On average, 9.6 different noncore services were included. All projects include hard facility management services (i.e., building maintenance and energy management) plus several soft facility management services, such as catering, cleaning, and linen and laundry service.
As we can notice from Table 1, the number of services included in PPP contracts has tended to diminish in more recent projects and varies across regions.
The Research–Training Approach to Support the Innovation of Italian PPP Model for Health Care Investments
As stated in the introduction, PPP across the world has been the result of the work by consultancies and legal firms (Shaoul et al., 2007; Willems & Van Dooren, 2016). However, to be successful, PPP needs a conducive local institutional environment (Jooste et al., 2011; Jooste & Scott, 2011; Opara et al., 2017; Soecipto & Verhoest, 2018) that helps to legitimate the model, establishing trust between key stakeholders and providing the system with adequate competencies for handling projects and contracts (Verhoest et al., 2015). These outcomes are the result of the interplay of a supportive political environment and clear policies, appropriate legal and regulative frameworks, competence units, and systems for learning and knowledge diffusion (Verhoest et al., 2015). During the first generation of PPPs, Italy largely lacked such elements. PPP was not adopted on the basis of an explicit policy or political commitment, but mainly for short-term financing needs (Vecchi et al., 2019). This was also reflected in the regulatory framework, which used the expression “project financing” as a proxy of PPP to describe the procedure to select the concessionaire. A national PPP unit was established but it has played a rather limited and diminishing role over the years.
In this context, in 2006, the authors started inductive/deductive research, typical of the management and economics of business literature (e.g., Masini, 1970) and public administration studies (e.g., Jensen & Rodgers, 2001). Over 12 years, between 2006 and 2018, this group met and engaged more than 1,000 Italian public and private managers involved in planning, evaluation, design, execution, monitoring, and renegotiating of PPP contracts to collect and analyze cases, which, when compared with the literature, have been the basis of a deep understanding of the drawbacks of the traditional model adopted in Italy, as well as to elaborate some possible evolutions (notably, the “light model” and the notion of economic and financial equilibrium). These evolutions were discussed, revised, and disseminated after 2010. This research approach also paved the way for the involvement of authors in action-research (i.e., on-field assignment aimed at the monitoring, evaluation, and renegotiation of contracts), which has proven to be fundamental in improving the understanding of the criticalities of PPP and the dissemination of the research results. To disseminate the knowledge of these research efforts, scientific and educational materials have been produced and training and dissemination activities organized, as reported in Table 2.
Dissemination and Training Activities Carried Out in the 2010–2018 Period.
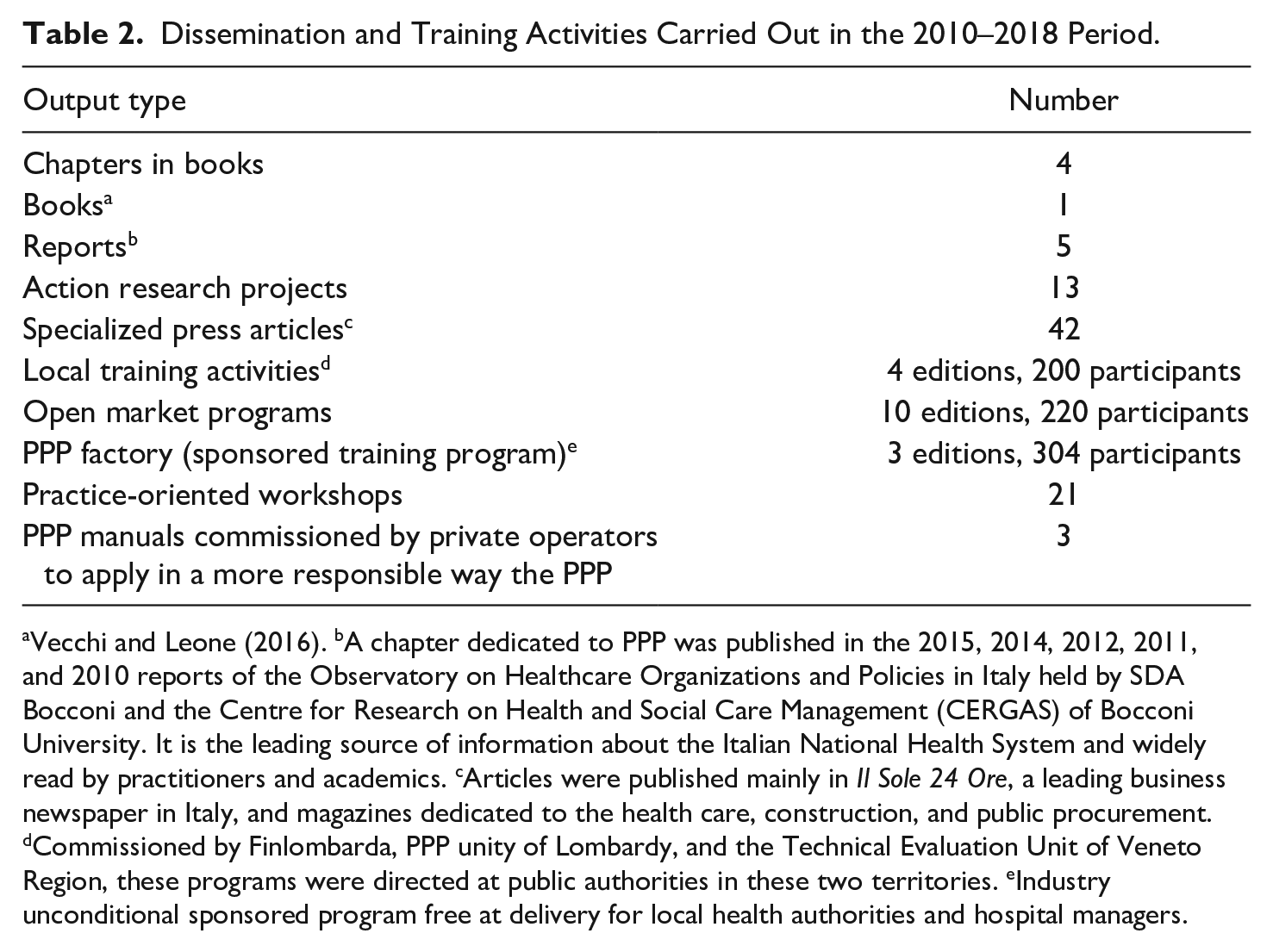
Vecchi and Leone (2016). bA chapter dedicated to PPP was published in the 2015, 2014, 2012, 2011, and 2010 reports of the Observatory on Healthcare Organizations and Policies in Italy held by SDA Bocconi and the Centre for Research on Health and Social Care Management (CERGAS) of Bocconi University. It is the leading source of information about the Italian National Health System and widely read by practitioners and academics. cArticles were published mainly in Il Sole 24 Ore, a leading business newspaper in Italy, and magazines dedicated to the health care, construction, and public procurement. dCommissioned by Finlombarda, PPP unity of Lombardy, and the Technical Evaluation Unit of Veneto Region, these programs were directed at public authorities in these two territories. eIndustry unconditional sponsored program free at delivery for local health authorities and hospital managers.
Currently, Italy is inaugurating its second generation of PPPs in the health care sector. Two small PPP contracts were signed in 2018 for medical equipment provision and management (managed equipment service—PPP-like contract) in the Piedmont Region, and several other large schemes are also in the pipeline: four contracts in Piedmont, for an overall value of about €1 billion; one project in Veneto Region, for €150 million; and five projects in the Abruzzo Region, for an overall value of €400 million. Thanks to the disseminating activities, which reached out to both authorities and economic operators, all these contracts have been framed around the “light model” and encompass the notion of economic and financial equilibrium.
These two contractual innovations are also institutionalized features, as they are included in the PPP standard model of the Italian Treasury, and the latter also in the Guidelines for PPP monitoring of Anticorruption National Authority.
The Emergence of the PPP Light Model to Overcome the Weaknesses of the DBFMO Contract
In this section, we analyze and comment on the relevance of the contractual innovation conceived within the inductive/deductive research approach explained in the section, “The Research–Training Approach to Support the Innovation of Italian PPP Model for Health Care Investments.” Considering its technical complexity, we have used some explanatory cases, exemplar and transparently observable (Eisenhardt, 1989; Flyvbjerg, 2006), selected from Italian PPP contracts. In consideration of the confidentiality of the information, the cases remain anonymous.
In the “light” PPP model (Vecchi & Cusumano, 2012), the SPV designs, finances, and builds the hospital, as well as takes a management only approach to hard facility services, that is, those strictly related to the availability of the newly built facilities. The rationale of the “light model” is that only those services that are strictly related to the core and main investment shall be included in the PPP contract. Therefore, if the hospital needs the renewal of medical equipment (investment component), the management component of the contract should include only those services that are related to the underlying investment, that is, the maintenance and renewal of equipment; when relevant, it is also possible to include the delivery of services through nurses or specialized technicians who work under the clinical governance of the health authority.
When an extensive DBFMO contract is signed, which includes many noncore services, the contract may generate a lot of rigidity in future decisions of the procuring health authority. In reality, prices and delivery modes of noncore services may change significantly during the life of the contract, as well as the needs of the health authority. Dehospitalization trends, for example, lead to the progressive reduction of hospital capacity and length of stay, with related consequences on services. Benchmarking contractual clauses, in principle aimed at renegotiating with the SPV features and price of services, have proven ineffective in providing the necessary flexibility to update contractual conditions, in addition because they have been solely conceived as a way to reduce fees for services.
The benchmark test methodology applied in all contracts is based on the calculation of an average price defined with reference to two average bids collected by the authority, the new bid produced by the SPV, and an official benchmark, such as a standard price released by national or regional authorities. If the average price thus defined falls within a certain band, generally in the range of ±10%, the cost of the service is not rectified. If it falls outside, provided that it is not an anomalous value, the price of the service offered by the SPV is rectified accordingly. This methodology generates moral hazard behaviors both by market players, from whom the authority has to collect bids (with the sole aim of calculating an average price), and by the SPV. Market players only have to provide an offer, but they may not then be involved by the SPV in the delivery of the service, also considering that SPV shareholders are often industrial players (i.e., companies that are involved in the building and operation tasks). Furthermore, they may have the incentive to offer low prices just to try to reduce the margins of the SPV and subsequently of their market competitors. On the contrary, the SPV has the incentive to offer higher prices to keep the average fee of the service within the band and therefore not apply the price revision. The ambiguity of this mechanism can be seen in the case of a PPP contract for which the authors got access to the results of the benchmark test. 3 The SPV offered prices that were, on average, 40% higher than those offered by the market. The consequence of this was that only five out of 13 service fees had been revised. Subsequently, due to the ambiguity of the mechanism, the authority also lost savings for an amount equal to the 14% of the service fee that had to be paid to the SPV.
In Italy, as described in the section “The First Generation of PPP Contracts in Italy,” the investment is remunerated through the availability charge and service fees. It must be noted that when service fees remunerate the investment, this component is not subject to a benchmark test. To avoid overindexation (Vecchi & Hellowell, 2018b), fees (availability charge and service fees) should only be partially indexed to inflation, on the basis of the incidence of the costs that are affected by inflation. When part of the investment is remunerated through service fees, which are fully indexed to inflation, there is a risk of overindexation that may bring an increase in SPV profitability (Vecchi & Hellowell, 2018b), which can undermine value for money and affordability of the project. This indexation mechanism may also expose the SPV to the risk of underprofitability if the effective inflation rate to be used to update the annual fees to be paid is lower than forecasted in the financial plan. In the latter case, however, the SPV is generally protected as a contract renegotiation can be requested. The mechanism is complex and, in one case, the procuring authority wrongly renegotiated the contract, thus causing an overall extra payment to the SPV of €6 million. Once the mistake was disclosed, the authority had to cancel the contract revision approval act; otherwise, the extra payment would have totaled €87 million.
When multiple noncore services are included and the main SPV shareholders are industrial players, as it happened in Italy and elsewhere, in a context of low competition due to the complexity of PPP transactions, the risk that prices of services are overestimated compared with market dominant prices is high, thus increasing the effective profitability for the SPV (Edwards et al., 2004). This also means that, because, as previously stated, these services often include a margin to remunerate the investment, they are often complex to calculate, especially due to the lack of dedicated skills in the public sector and the relevant information asymmetry that affect complex transactions, such as PPP contracts.
In one project, under the scrutiny of the responsible audit authority, it was found that the annual overall difference between the costs for noncore services in comparable hospitals and the unitary payment due (the sum of the service fees, as the contract does not include the payment of an availability charge) was between €25.3 and €26.5 million. Considering that the production costs are similar between PPP contracts and traditional situations (although, generally, the SPV is able to extract more margins from subcontractors than an health care organization from a contract with a service provider within a traditional procurement), this sum can be considered the extra remuneration for the net investment (of the public grant) and the capital invested (debt and equity). In fact, the examination of the internal rate of return (IRR) derived from the financial model annexed to the final version of the contract shows that the PPP contract provides only a normal return for the private investors involved. The projected IRR is approximately 6.60% and the equity IRR is 8.5%, which are quite low compared with international norms (Vecchi et al., 2013). However, by considering a net margin of €25.3 to €26.5 million for the SPV, the project IRR is between 12.5% and 13%, which is far higher than that derived from the financial model annexed to the contract (6.60%). However, it must be noted that this net margin is not wholly retained by the SPV directly, but is instead mainly passed on to subcontractors, who are also the shareholders of the SPV. This case clearly raises not only an issue of unaffordability and non-value-for-money of the PPP contract but also of transparency, as the extra margins hidden in noncore services may generate returns that are not captured in the official financial plan of the contract (Edwards et al., 2004).
The inclusion of many noncore services also generates another two drawbacks in the standard DBFMO contract. It can damage the market of small and medium enterprises, also social, which are often involved in the delivery of noncore services. In reality, they may not have the necessary equity to become an industrial investor and, as a mere subcontractor of the SPV, they may be forced to reduce their margin to the benefit of industrial and financial investors. These small players generally act as subcontractors of the industrial investor, thus allowing them to extract a higher return than those officially declared in the contract, as explained above. Furthermore, when the perimeter of the project is wide, due to the high number of noncore services, the risk of contract incompleteness increases (Brown et al., 2009, 2016; Kim & Brown, 2012), thus exposing parties to the risk of contract renegotiation, which happens in a situation of monopoly, thus reducing the negotiating power of the authority with the SPV, with negative consequences in terms of affordability and value for money.
Concluding Discussion
Among social infrastructure, the health care sector has so far been one of the main fields of application of PPP contracts, with some main variations across jurisdictions. The DBFMO contract, which has been the focus of extensive literature production, is one of the most adopted models, especially across Western countries under national health care systems. Italy is second to the United Kingdom in Europe for the implementation of the DBFMO model, which has been used in 50% of the investments over the past 15 years (Cappellaro et al., 2015).
Thanks to an inductive/deductive research approach applied over the past 18 years, the authors have analyzed the main drawbacks of this model, and conceived, through continuous interaction with main public and private stakeholders, two key innovations: the concept of financial equilibrium and the PPP “light model.” This article focuses on the latter. The two innovations have been institutionalized as they are now part of Italian soft law (Italian Treasury standard PPP contract and Anticorruption National Authority guidelines for PPP contracts monitoring).
The article provides a discussion, rooted in an exemplary and transparently observable case (Eisenhardt, 1989; Flyvbjerg, 2006), of the weaknesses of the traditional DBFMO model when applied to the health care sector, which can be overcome through the adoption of the “light model.”
The application of the “light model” is recommended, especially in mature economies, where authorities potentially have the capacity of coordinating different contracts, namely, the PPP contract for building/refurbishing the facilities and those for the provision of services, which can also be structured as PPP (e.g., in the field of medical equipment). When PPP contracts are applied to emerging countries, the traditional DBFMO contract could be preferred, however, with some improvements with reference to the inclusion of noncore services. One solution could be the inclusion of noncore service operations for a limited number of years (3 or 5 years), to ensure the start-up of the hospital. Later on, authorities can decide to procure these noncore services directly or they can delegate this activity to the SPV under a transparent mechanism.
At the time of writing, some countries have taken a stance of distancing themselves from PPP. In the United Kingdom, it has been announced that the PF2 model will be abandoned and, in March 2019, the Treasury issued a consultation paper to profoundly review the policy to finance infrastructure (HM Treasury, 2019). In Italy, the position of the Five Star Movement, which is currently one of the governing parties, is absolutely against the involvement of private capital in infrastructure and, above all, in the health care sector. Therefore, the pipeline of second wave contracts, briefly described in the “Introduction” section, has not yet been fully implemented. In general, across the world, PPP is under massive discussion, especially for the higher cost of private capital vis-à-vis the cost of public money.
Despite the low cost for many governments, the public sector lacks the administrative capacity to manage a pipeline of investments, as recently witnessed by the press also for countries such as Germany 4 ; therefore, it is difficult to predict a complete abandoning of PPP. The “light model” and the notion of economic and financial equilibrium, in a context of appropriate risk allocation and strong competence in the public sector to structure and monitor contracts, could still represent a viable solution. Furthermore, PPP latu sensu seems to represent the only option to make use of the enormous private liquidity available on the financial markets, including the savings of citizens (also through pension funds and insurance companies), in search of better and more stable returns compared with those offered by traditional asset classes (Gatti & Della Croce, 2015).
This article has also provided insight into the role that academia, and in particular business schools (Grey, 2001; Starkey & Madan, 2001), can play through research, training, and dissemination in the institutional change process (Pettigrew & Starkey, 2016), thus contributing to the closure of the so-called rigor–practice gap (i.e., the gap between academia, public management, and policy), which is evident across the world, as discussed by Cepiku (2011). In particular, the gap can be due to the low relevance of research and its focus more on rigor rather than relevance (Gibbons, 1994). The approach used, which is an example of a mix of M2K—Mode 2 knowledge (Joan E. van Aken, 2004, 2005) and a coproduction approach (Cepiku, 2011; Orr & Bennett, 2008), has allowed academia to understand the relevant issues that need solutions to improve value-for-money to make PPP acceptable and helped (public and private) operators to profoundly understand the dynamics underpinning PPP contracts. This collaborative process is replicable and it could open up further avenues of research to compare the role of academia across different jurisdictions and contexts and to further develop the workstream of research on the academic-relevance gap in the field of PPP, especially for social infrastructure, where the model is currently under deep discussion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.