
Abstract
This preliminary investigation examined the relationship between poverty level and parental awareness of evidence-based interventions in urban African American parents of children with autism spectrum disorder (ASD). Based on responses to a survey, more parents above the Federal Poverty Level (FPL) reported awareness of the interventions than parents who were below the FPL. Similarly, poverty level was related to parental awareness of the educational and therapeutic services their child received.
Keywords
According to a recent national report (Addy, Englehardt, & Skinner, 2013), approximately 16 million children in the United States live in poverty, a 23% increase from 2006 through 2011, the years for which the most recent data are available. Poverty has a significant impact on many aspects of family life—health, physical environment, emotional well-being, and interpersonal interactions (Aber, Jones, & Cohen, 2000; National Scientific Council on the Developing Child, 2010; Park, Turnbull, & Turnbull, 2002). For example, poverty impacts the health of the child because of its association with more frequent incidence of illnesses and concomitant increased rates of hospitalization (Aber et al., 2000). Poverty also impacts the home environment through overcrowding, inadequate heating, and lead exposure, resulting in impoverished learning environments. Consequently, those living in poverty may have poor educational outcomes resulting from these health and environmental factors.
Poverty in childhood is more common among children with disabilities than among children without disabilities. Fujijura and Yamaki (2000) reported that 28% of U.S. children with disabilities lived below the Federal Poverty Level (FPL), as contrasted with 16% of children without disabilities. Using data from a national survey to examine one particular disability, Kogan and colleagues (2008) found that children with autism spectrum disorder (ASD) that have special health care needs were more likely to live in families that report financial problems, need additional income for their child’s medical care, and reduce or stop work to care for their child. Parents who have fewer resources may be less informed and knowledgeable about their child’s disability, which could affect the timely identification and subsequent treatment of ASD.
There is a growing body of literature to indicate that there are disparities in the age of diagnosis of ASD in children from traditionally underserved populations, which includes those who are poor and from racial/ethnic minorities. Early identification of ASD is presumed to be associated with higher socioeconomic status (SES) because greater parental education and wealth provides the family with resources that increase the likelihood that their child will receive an early, accurate diagnosis. This in turn optimizes the chance of an earlier onset of intervention (Liptak et al., 2008). Studies have shown that earlier identification of children with ASD is related to maternal education (Magaña, Lopez, Aguinaga, & Morton, 2013), income (Durkin et al., 2010; Goin-Kochel, Mackintosh, & Myers, 2006; Liptak et al., 2008; Mandell, Novak, & Zubritsky, 2005), race (Mandell, Listerud, Levy, & Pinto-Martin, 2002; Mandell et al., 2009; Rosenberg, Landa, Law, Stuart, & Law, 2011; Sansosti, Lavik, & Sansosti, 2012), and ethnicity (Liptak et al., 2008; Magaña et al., 2013; Rosenberg et al., 2011). The literature also indicates that despite similar ages of parental concern, professionals identify children with ASD from two traditionally underserved populations, African Americans (Mandell et al., 2002; Mandell et al., 2009; Rosenberg et al., 2011; Sansosti et al., 2012) and Latinos (Magaña et al., 2013), later than Caucasian children.
In addition to differences in age of diagnosis, recent emerging evidence suggests that disparities also exist in the awareness, knowledge, and receipt of services in traditionally underserved populations. Factors related to these disparities, like those related to ASD identification, are socioeconomic and racial/ethnic variables. For example, Magaña and colleagues (2013) found that Latino children were less likely than non-Latino White children to receive varied services, including early intervention, respite, and a Medicaid-funded intensive autism treatment. In an investigation involving a national sample of children, being “Black, Latino, or poor” was associated with decreased access to heath care services such as having a personal physician or obtaining needed advice (Liptak et al., 2008, p. 152). Harstad, Huntington, Bacic, and Barbaresi (2013) found that disparities in the receipt of special education services through an Individualized Education Plan (IEP) in school-age children with ASD were related to maternal education, an indicator of SES, and race/ethnicity. Thus, in addition to being “undercounted,” children with ASD from lower SES might also be “underserved relative to those with high SES” (Durkin et al., 2010, p. 7).
Parents’ familiarity with different evidence-based interventions would support their ability to make informed decisions about their child’s therapy and ultimately enable them to more fully participate as partners in the therapeutic process. The establishment of parent−professional partnerships, which involve mutual participation, collaboration, and support, is considered a best practice for all children with disabilities including those with ASD (Taber-Doughty & Bouck, 2012). Furthermore, educational law mandates that parents be decision makers and advocates for their child through active collaboration with professionals (Individual With Disabilities Education Improvement Act [IDEIA], 2004), a best practice, which applies to all children including those from underserved populations.
Based on the literature review, no published studies have examined the relationship between poverty and parental awareness of evidence-based interventions for children with ASD. Awareness of evidence-based interventions for children with ASD would help parents in the decision-making process and enable them to be more active partners in their child’s services as mandated by IDEIA (2004). One study (Sansosti et al., 2012) that examined parental knowledge of different interventions for ASD used a sample of 16 families, 4 who were African American and 2 of mixed racial background. The majority of these families were middle income. These families had adequate knowledge of the majority of contemporary interventions such as Applied Behavior Analysis (ABA), the Picture Exchange Communi-cation System™ (PECS), Developmental Individualized Relationship–based® (DIR)/Floortime™, and Social Stories™. However, studies involving parent reports of autism interventions (e.g., Goin-Kochel, Myers, & Mackintosh, 2007; Green, 2007; Green et al., 2006; Mackintosh, Goin-Kochel, & Myers, 2012) have not focused exclusively on African American parents nor have they analyzed parents’ awareness of the interventions in relation to poverty. Although there are no studies addressing parents’ awareness of evidence-based interventions in relation to poverty, it is clear that being a member of a racial ethnic minority and living in poverty are both documented risk factors associated with poor educational outcomes (Shonkoff, 2012).
The purpose of this pilot investigation was to provide preliminary data on the relationship between poverty level and awareness of different evidence-based interventions in urban African American parents of children with ASD. African American parents living in urban areas were asked to self-report their awareness of eight different evidence-based interventions used with children with ASD. All treatments selected for inclusion in the study have some degree of empirical support. The interventions included both broad-based models such as the TEACCH (Treatment and Education of Autistic and Related Communication for Handicapped Children) program, SCERTS® (Social Communication Emotional Regulation Transactional Supports) model, and DIR®/Floortime™, and skill-based treatments such as PECS™, Social Stories™, peer-mediated strategies, and Augmentative Alternative Communication (AAC). The therapies surveyed in the study represent a continuum of approaches (Prizant & Wetherby, 1998) from the behavioral such as ABA to the developmental social-pragmatic such as DIR®/Floortime™. Five of the treatments were registered or trademarked. Biomedical treatments such as drugs, special diets, and physiological treatments such as sensory integration were excluded. All of the treatments could be delivered by an educator or a therapist. In addition, the investigators examined the relationship between poverty level and parental awareness of the services their child received. The following research questions were asked:
Method
The Institutional Review Board at Brooklyn College of the City University of New York approved this pilot study.
Participants
Forty-nine African American parents of children with ASD who resided in neighborhoods of Brooklyn, located in New York City, completed a survey designed for families of children with ASD. According to the most recent data available from the U.S. Census Bureau (2010), these areas include a disproportionately high number of low income and African American families. The percentage of all families with related children under 18 years whose income in the past 12 months was below the poverty level ranged from 13% to 37%. The percentage of African Americans living in the target neighborhoods ranged from 55% to 91%. The participants were volunteers who were recruited at support group meetings at a community-based agency selected because of its location in one of the target neighborhoods. This family support agency serves African American parents whose children were previously identified with ASD. Parents attending the agency’s monthly support group meetings were invited to complete a survey for families of children with ASD.
Materials and Procedures
A speech-language pathologist with expertise in ASD, a special educator with expertise in ASD, a representative of the agency, and a university administrator with skill in survey question design developed a 38-question traditional pencil-and-paper survey designed to assist the administration of the agency to collect information on the profiles of African American families of children with ASD who attended their support groups. The survey included 12 questions regarding demographic information that included household income, in US$10,000 increments that ranged from “less than US$10,000” to “US$50,000 and above,” neighborhood of residence, marital status, and the number children residing in the household. In addition to demographics, the survey covered the topics of social-emotional well-being (n = 8 questions), support groups (n = 3 questions), health care (n = 3 questions), resources (n = 5), services (n = 3), and evidence-based interventions (n = 4 questions). For the purpose of this preliminary study, the investigators retrospectively analyzed the responses to seven questions, five regarding demographic information, one regarding evidence-based interventions, and one regarding services, all of which were directly related to the two research questions. The questions about social-emotional well-being, health care, support groups, and other resources were not analyzed because they were not germane to the research questions. The appendix contains the seven survey questions that were used in the retrospective analysis.
A representative of the non-profit family support agency, which collaborated in this study, distributed, administered, and collected the surveys from 49 parents who volunteered to complete them after a support group meeting. Confidentiality of the surveys was maintained by requesting that the respondents not write any identifying information on them. Only one member of each household was permitted to complete the survey. The parents were given 45 min to complete the survey, but additional time was allotted if a respondent requested it. Most respondents completed the questions in approximately 30 min. The data were collected over a 3-month period at the monthly support group meeting in which new members attended. At the close of the data collection period, the representative of the family support agency who distributed and collected the surveys hand-delivered them to the first author who numbered, coded, and analyzed them using SPSS® (IBM Corp., 2011).
The participants were assigned to two groups based on FPL (Federal Register, 2011) which was determined from the participants’ self-reported income level and household size using the Health and Human Services Poverty Guidelines (U.S. Department of Health & Human Services, 2009). Household size was estimated on the basis of marital status and number of children residing in the home. For example, if the participant was single and had two children below 18, household size was estimated at three.
Although families were encouraged to answer all of the questions, some respondents who handed them in opted not to respond to some of them. Surveys were excluded from the analysis if respondents did not answer the demographic questions regarding income level, marital status, and the number of children in the household because that information was needed to determine if the participant was above or below the FPL. Surveys were also excluded if the respondents did not answer the questions regarding evidence-based interventions and services, which were the focus of this preliminary investigation. Using these guidelines, 15 of the 49 surveys were eliminated because they were incomplete. Of the 34 remaining respondents who comprised the participant base in the preliminary investigation, 16 of the participants were below the FPL and 18 were above the FPL using the criteria previously described. The characteristics of the 34 participants in the two groups in terms of income range, marital status, and number of children residing in the household are listed in Table 1.
Demographic Characteristics of the Participants Below and Above the FPL.
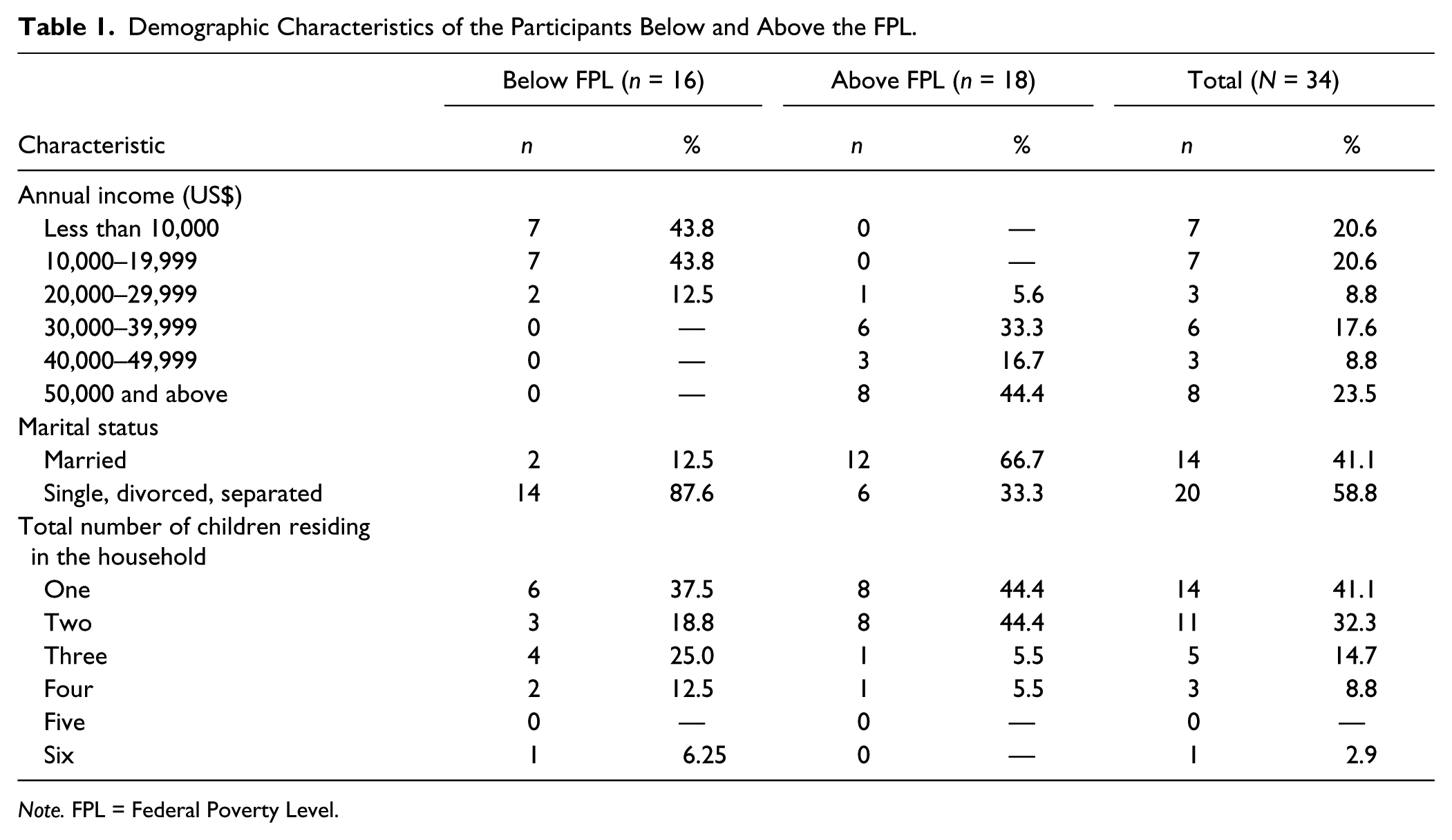
Note. FPL = Federal Poverty Level.
The variable of poverty level was dichotomized into the groups below and above the FPL. Within the two research questions, the subcomponents were dichotomized into the aware/not aware categories. The first research question concerned eight evidence-based interventions, which are listed with a brief description in Table 2. The subcomponents of the second research question were the dichotomous categories aware/not aware of the services their child received. The research questions were analyzed using a cross-tabulation procedure. Fisher’s (1954) exact test, a chi-square statistic, was used for all analyses.
The Name and Description of the Eight Evidence-Based Interventions Used in the Survey.
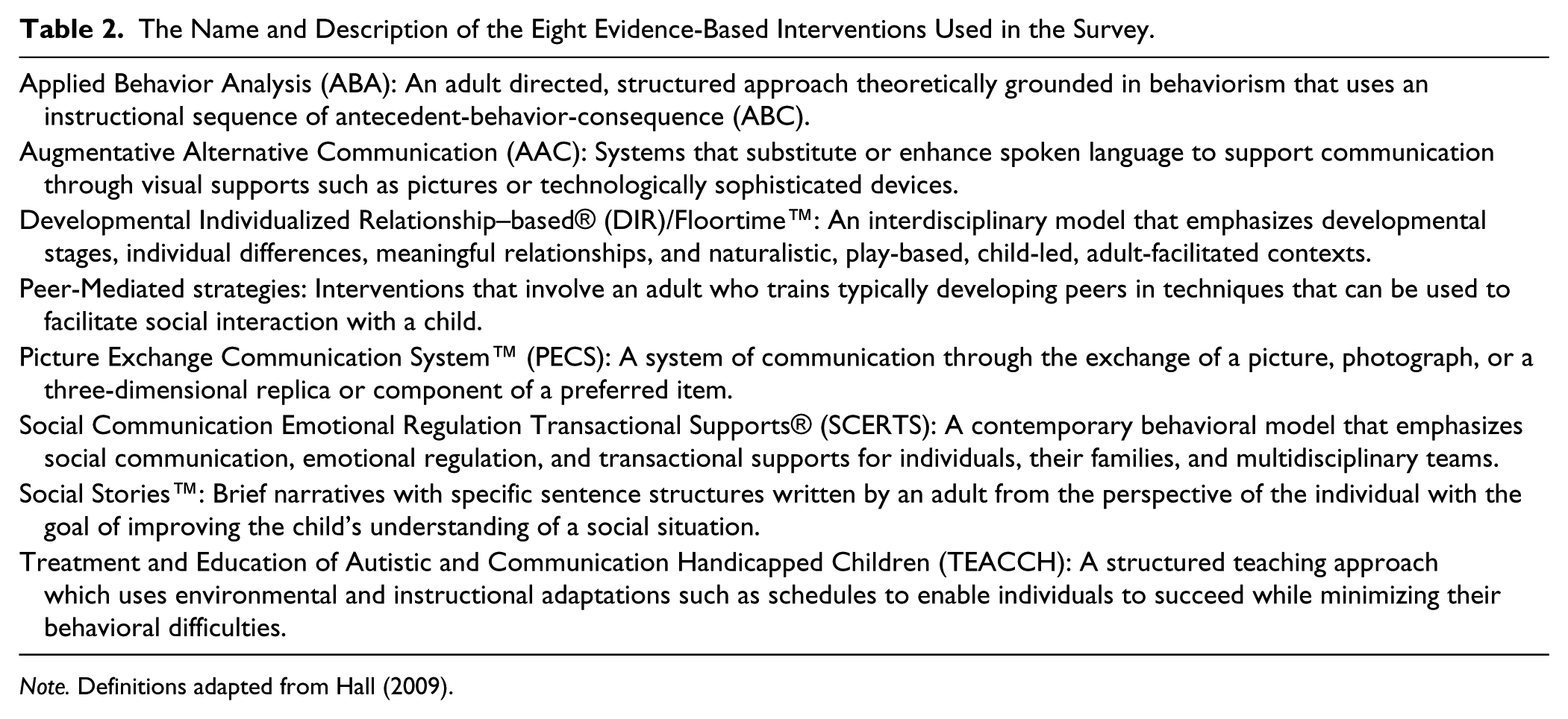
Note. Definitions adapted from Hall (2009).
Reliability of data entry was established by having a trained research assistant check the accuracy of the data entry for 30% of the survey questions relevant to this preliminary report selected at random. Reliability was calculated by dividing the number of agreements by the number of agreements + disagreements × 100. Reliability of data entry using this procedure was 100%.
Results
The results of this preliminary report focus on those survey questions that addressed parental awareness of evidence-based interventions and services received. The first research question concerned parental awareness of eight different evidence-based interventions for children with ASD. For six of the treatments surveyed, more parents above the FPL were aware of the treatments surveyed than were parents below the FPL. The two exceptions were the SCERTS® model and peer-mediated strategies that resulted in proportionately slightly higher awareness of the interventions by those below the FPL than above. For the SCERTS® model, 25% of the parents below the FPL and 5.6% of those above reported awareness of the approach. The proportion of parents who reported awareness of peer-mediated strategies was 12.5% for those below the FPL and 11.1% for those above.
ABA was the treatment approach most familiar to the parents who completed the survey, with self-reported awareness by 94.4% of the respondents above the FPL and 68.8% of those below the FPL. The TEACCH program was the second most familiar program in both groups, with self-reported awareness by 55.6% of those above the FPL and 31.2% of those below the FPL. A similar pattern of awareness was observed for PECS™, the third most familiar approach, with self-reported awareness by 55.6% of the parents above the FPL and 12.5% of those below the FPL, a difference that was significant on Fisher’s (1954) exact test (*p < .05). Three treatments, the SCERTS® model, DIR®/Floortime™, and Social Stories™, were ranked fourth with reported awareness by 14.7% of the parents in both groups. AAC and peer-mediated strategies ranked fifth, with reported awareness by 11.8% of the parents in both groups. Table 3 lists the parents’ reported awareness of the evidence-based interventions for the two poverty-level groups and the rank order of parental awareness for the total participants.
Number and Percent of Some Urban African American Parents Below and Above the FPL Who Self-Reported Awareness of Evidence-Based Interventions for Children With ASD With Rank Order of the Treatments by All Parents.

Note. FPL = Federal Poverty Level; ASD = autism spectrum disorder; ABA = Applied Behavior Analysis; TEACCH = Treatment and Education of Autistic and Related Communication for Handicapped Children; PECS = Picture Exchange Communication System; DIR = Developmental Individualized Relationship–based; SCERTS = Social Communication Emotional Regulation Transactional Supports; AAC = Augmentative Alternative Communication.
p < .05 (two-tailed).
The second research question concerned parents’ self-report of awareness of services received. Parents above the FPL indicated that their children received more services than the children of parents below the FPL for all services—educational services as well as speech-language, occupational, and physical therapies. These trends were consistent in the data but the differences between the groups were not statistically significant using Fisher’s (1954) exact test (see Table 4). Based on the parental reports, 66.7% of children from families above the FPL and 43.8% of parents below the FPL indicated that their children received educational services. Speech-language therapy was reportedly received by 77.7% of the children from families above the FPL and 43.75% of the children from families below the FPL. Occupational therapy was reportedly received by 50% of the children from families above the FPL and by 18.75% of the children from families below the FPL. Physical therapy was reportedly received by 22.2% of the children from families above the FPL and 18.75% of the children from families below the FPL.
The Number and Percentage of Urban African American Parent Participants Below and Above the FPL Who Self-Reported Their Child’s Receipt of Educational Services and Speech-Language, Occupational, and Physical Therapies.

Note. FPL = Federal Poverty Level.
Discussion
The results of this pilot study provide preliminary data, which suggest a trend in the relationship between poverty level and awareness of evidence-based interventions for urban African American parents of children with ASD. A greater proportion of parents living above the FPL than below, as measured by reported income, marital status, and the number of children living at home, were aware of more of the evidence-based interventions and services their children received. These findings support the notion that poverty is a risk factor that affects families’ awareness of different interventions and services received.
The data suggested that poverty level was related to the parents’ awareness of evidence-based interventions and their child’s program of service. In terms of the evidence-based interventions sampled, fewer than half of the total parents in both groups were aware of the different treatments available with the exception of ABA. The parents above the FPL were more aware than those below the FPL of six out of the eight of the interventions surveyed. Similarly, parents above the FPL were consistently more aware than parents below the FPL of their child’s educational and therapeutic services. These findings suggest a greater risk of poor outcomes for children living in poverty, a view consistent with the work of Aber and colleagues (2000), Park and associates (2002), and Shonkoff (2012).
Similar to the participants in this study who were above the FPL, the middle-income participants in the study by Sansosti and colleagues (2012) self-reported adequate knowledge of the majority of the evidence-based interventions they surveyed. In terms of parental awareness of the therapies their child received, the majority of the participants in the present study reported that their child received speech-language therapy. Green and associates (2006) found that speech therapy, visual schedules, sensory integration, ABA, Social Stories™, PECS™, TEACCH, DIR®/Floortime™, and AAC were the evidence-based interventions that parents reported were more commonly used. In this study, six of the same treatments were surveyed—ABA, Social Stories™, PECS™, TEACCH, DIR®/Floortime™, and AAC. The study did not include speech therapy because it is generic and can be conducted within the framework of all of the interventions surveyed. Two additional evidence-based interventions, peer-mediated strategies and the SCERTS® model, which were not included in the study by Green and associates (2006), were surveyed here.
The result that parents above and below the FPL did not differ significantly in their awareness of seven of the eight interventions was surprising given the suggestion in the literature that populations living in poverty may have less access to information than those who do not (Gourdine, Baffour, & Teasley, 2011; Park et al., 2002; Shonkoff, 2012). Only PECS™ reached statistical significance for the participants above and below the FPL. The reason for this significant difference remains unclear.
The finding that most of the parents surveyed reported that their children received speech-language services was not surprising given that challenges in social interaction and communication-language are core deficits of ASD. Following speech-language therapy, more of the participants reported that their children were enrolled in occupational therapy than in physical therapy, as expected given the preponderance of sensory issues in individuals on the spectrum (Baranek, Parhm, & Bodfish, 2005). In fact, the sensory challenges of individuals on the spectrum have been recognized in the diagnostic criteria of ASD in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013).
Limitations
The primary limitations of this investigation were the small sample size, the fact that the data were derived from parental report, the retrospective use of the survey, the sample composition from one urban area, and the lack of verification of an ASD diagnosis from record review. The small sample size likely precluded reaching statistical significance for most of the variables analyzed.
While this study examined African American parental awareness of evidence-based interventions for ASD, the sample represented that racial/ethnic group from only one geographic location, an urban area of New York City. Generalizations cannot be made to African Americans from other urban regions or to other types of environments such as the rural or suburban. Furthermore, one cannot generalize the results of 34 surveys to the millions of people in poverty who have children with ASD.
Another limitation was that the parents self-reported their incomes and their child’s ASD identification. Further-more, they were not asked to report the specific ASD diagnosis that their child had received such as Asperger syndrome, classic autism, or pervasive developmental disorder–not otherwise specified (PDD-NOS). Although the participant base was too small in this preliminary study to group the children by ASD diagnosis, this could be done in future studies with larger numbers of subjects.
Clinical Implications
The fact that so few of the parents surveyed had heard of the evidence-based interventions and that so few of them knew what services their child received highlights the need for better parent–professional partnerships. For example, Green (2007) reported that only 6 of 19 families indicated that they received information about treatments from their child’s school. Another study (Mackintosh et al., 2012) found that some parents reported problems of autism awareness in their children’s schools. Parents’ familiarity with different treatments could facilitate collaboration with their child’s teacher or service provider regarding their child’s education and therapy. School personnel have the most contact with the child and can provide valuable input to the parents about different interventions. Conversely, parents know their child best and can provide invaluable input to their child’s teacher or service providers. In addition, it is a legal mandate (IDEIA, 2004) and best practice to include parental input in the decision-making process. Taber-Doughty and Bouck (2012) noted, “Parents need the support and training from trained school personnel to make informed decisions for their children” (p. 270). Similarly, the National Scientific Council on the Developing Child (2007) called for the education of parents in areas where they need information. Marcus, Kunce, and Schopler (2005) noted that schools need to work closely with parents who have been inundated with information about ASD from the media and presented with uncertain and unsubstantiated practices.
Future Research
Future studies of parents’ awareness of evidence-based interventions should involve larger, more defined samples of parents and children with comparisons of individuals from different racial ethnic backgrounds using subjects from varied locations that would be more representative of the population at large. A larger sample would also allow an examination of the impact of the child’s age on what parents know about evidence-based interventions. The Internet would be better way to reach participants from varied geographic areas.
Future studies should attempt to verify participants’ income and include additional breakdowns above the US$50,000 level. Studies should also include a mechanism for confirming ASD diagnosis and mandated services. Finally, it would be important to investigate how parents learned about the evidence-based interventions they are aware of. Future research could include more established evidence-based interventions as well as emerging ones that may currently have a smaller research base, such as Relationship-Based Developmental Intervention (Guttstein & Sheely, 2002) and the Early Start Denver Model (Rogers & Dawson, 2010). This work would add to the emerging body of work on the impact of poverty on ASD in the African American community.
Footnotes
Appendix
Acknowledgements
The authors wish to acknowledge Lucina Clarke and Wayne Clarke for their assistance with data collection. The assistance of Michele Emmer, Baila Epstein, Elaine Geller, Sima Gerber, Timothy Gura, Angelo LaGrega, Ciara Leydon, Mariana Regalado, and Howard Spivak is also acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.