
Abstract
The current study investigated the parent–child relationship by examining associations between parent stress, parental discipline strategies, child disruptive behavior problems, and level of autism spectrum disorder (ASD) symptoms. A sample of 130 parents of children with ASD ages 3 to 11 years participated. Parents reported high levels of parent stress and high levels of child disruptive behavior problems. A series of mediation analyses via bootstrapping were used to examine the development of child disruptive behavior. Use of harsh and punitive parental discipline strategies mediated the link between parent stress and child disruptive behavior problems. These findings suggest that parental discipline strategies should be a central target in prevention and treatment interventions for children with ASD to reduce the emergence of child disruptive behavior problems. Reducing challenging behavior in children with ASD may improve the rate of skill acquisition and improve the parent–child relationship. Future directions for research along with clinical implications for families are discussed.
Autism spectrum disorder (ASD) is estimated to occur in 1 in 68 births (Centers for Disease Control and Prevention [CDC], 2014). Individuals with ASD display impaired social reciprocity, deficits in communication skills, and have rigid and repetitive behaviors (American Psychiatric Association [APA], 2013). Approximately 70% of individuals with ASD present with at least one additional psychological condition and approximately 40% present with two or more (APA, 2013; Simonoff et al., 2008). Prevalence estimates of comorbid oppositional defiant disorder have been reported as high as 37% in children with ASD (Kaat & Lecavalier, 2013). Midouhas, Yogaratnam, Flouri, and Charman (2013) demonstrated that rates of comorbid psychopathology increase with age among children with ASD. The presence of additional psychopathology is pervasive and chronic, persisting through adolescence without treatment (Simonoff et al., 2013). Emotional and behavioral symptoms associated with additional psychopathology produce adverse effects that transcend the core symptoms of ASD (Mannion & Leader, 2013; Storch et al., 2012).
Emotional and behavioral symptoms have often been labeled as challenging behavior (e.g., disruptive behavior problems, problem behaviors, or aberrant behaviors) in children with ASD. Emerson (1995) defines the term challenging behavior as
cultural abnormal behavior(s) of such intensity, frequency or duration that the physical safety of the person or others is likely to be placed in serious jeopardy, or behavior which is likely to seriously limit use of, or result in the person being denied access to, ordinary community facilities. (p. 4)
Many individuals with ASD exhibit challenging behavior (Lecavalier, 2006; Matson & Nebel-Schwalm, 2007). The debilitating symptoms likely affect all areas of child development. Individuals with ASD are at increased risk for developing challenging behavior compared with those with intellectual disability alone (Holden & Gitlesen, 2006).
Noncompliance, oppositional behavior, and aggression are among the most prevalent challenging behavior problems reported by parents of children with ASD (Baker & Feinfield, 2003). Challenging behaviors commonly occur in those with ASD across the life span (Matson & Nebel-Schwalm, 2007; Smith & Matson, 2010). Parents and teachers often consider challenging behaviors of equal or greater importance to the core symptoms of ASD due to the debilitating nature that the symptoms may have on health, safety, learning, and social relationships (Pearson et al., 2006).
Challenging behavior affects educational intervention, residential placement, social-emotional development, family well-being, and use of antipsychotic medication for those with ASD (Brereton, Tonge, & Einfeld, 2006; Hartley, Sikora, & McCoy, 2008; Lauderdale-Littin, Howell, & Blacher, 2013; Lecavalier, 2006; McGill & Poynter, 2012; Storch et al., 2012). Thus, challenging behavior may result in suboptimal long-term outcomes for children with ASD.
There is overwhelming evidence that parents of a child with ASD are more stressed compared with caregivers with typically developing children and children with other medical and developmental delays (see Hayes & Watson, 2013 for meta-analytic review). Experts in the field have conceptualized parent stress as “the aversive psychological reaction to the demands of being a parent” (Deater-Deckard, 1998, p. 315). Adverse effects of chronic stress have been well documented. For example, Seltzer et al. (2010) found that mothers of children with ASD and a history of clinic-level behavior problems showed reduced cortisol activity. This reduced cortisol activity was similar to the reduced cortisol activity found in those experiencing chronic stressors (e.g., combat veterans and families of children with chronic illnesses).
There is strong evidence of a bi-directional link between parenting stress and child disruptive behavior problems in non-ASD families (Anthony et al., 2005; Blader, 2006). Theoretical models (i.e., Deater-Deckard, 1998; Hastings, 2002) have suggested complex links between parent stress and child disruptive behavior problems. However, few studies have examined these models within an ASD population, and results of these studies are inconsistent. Two studies found a bi-directional effect between child behavior and parent stress. Lecavalier, Leone, and Wiltz (2006) reported a bi-directional link between parent stress and child behavior problems in 293 children and adolescents with ASD across a 1-year period. The authors found that parent stress and behavior problems exacerbated each other during that time period. Zaidman-Zait et al. (2014) examined parent stress over a 4-year period. They found evidence of both bi-directional and unidirectional effects. A bi-directional effect was found between parenting stress (i.e., stress directly related to the parenting role) and child externalizing behavior. A unidirectional effect, however, was found for general parent distress (e.g., depression, isolation) predicting child externalizing behavior. Similarly, Totsika et al. (2013) found that general parent distress, physical health limitations, and lower life satisfaction are risk factors for the development of child behavior problems. However, early child behavior problems were not necessarily associated with later maternal stress. Therefore, certain parenting characteristics that stem from the stress of feeling alone and isolated may lead children to exhibit more problem behaviors over time. However, stress specifically within the parenting role likely results in bi-directional associations with child behavior problems.
Researchers have expanded upon the associations between parent stress and child behavior to include other variables (i.e., parenting strategies) that have been proposed in theoretical models (i.e., Deater-Deckard, 1998; Hastings, 2002). To date, limited research has examined these associations in combination within families affected by ASD. Osborne and Reed (2010) found a bi-directional link between parent stress and parent strategies among 138 families with a child with ASD. Osborne, McHugh, Saunders, and Reed (2008) found that the parent behavior of limit-setting, a form of parental discipline strategy, mediated the link between parent stress and subsequent child disruptive behavior problems. Their findings suggest that there may be certain parenting strategies that may elicit child disruptive behavior problems. Furthermore, Midouhas et al. (2013) found that low maternal warmth and chaotic household environments are risk factors for child externalizing behavior.
To date, only one study has simultaneously demonstrated the link between parent stress, parenting behavior, and child disruptive behavior problems within a sample of children with ASD (i.e., Osborne et al., 2008). Further research is needed to test multiple parent–child relationship variables simultaneously, especially multiple discipline strategies other than limit-setting. This research is especially needed with younger samples of children with ASD.
Examining how parent stress affects child disruptive behavior problems is warranted. Identifying potential mediating variables, such as parenting strategies, is important because these mediators may provide targets for intervention. This is timely as different treatments are being developed that target parent stress and child disruptive behavior problems. Practical and theoretical understanding the process by which these variables interact would best inform directions for treatment. Some treatments have identified that parental mindfulness may reduce child disruptive behavior problems (Singh et al., 2006; Singh et al., 2014). However, a plethora of research is underway examining behavioral parent training designed to decrease child disruptive behavior problems through modifying the parent–child relationship (e.g., Aman et al., 2009; Bearss, Johnson, Handen, Smith, & Scahill, 2013; Durand, Hieneman, Clarke, Wang, & Rinaldi, 2013). Practical and clinical considerations rely on identification of treatment targets that have the potential to affect most families. In the current study, we chose to examine parental discipline strategies as it has the potential to reduce child disruptive behavior, which should theoretically simultaneously decrease parent stress.
In this study, we systematically investigated parent stress, parental discipline strategies, child disruptive behavior problems, and ASD symptomatology. Previous studies have often combined common externalizing behavior problems with other symptoms associated with ASD. Examining common disruptive behavior problems such as noncompliance and aggression is warranted as these behaviors often occur in parent–child interactions. Common disruptive behavior problems are often exhibited in response to a parental demand (e.g., parental instruction to turn off the television results in a child protest) and are likely followed by a parental discipline strategy. Therefore, analysis of these behaviors should incorporate both parent and child variables. Parental discipline strategies can vary greatly from a lax response (e.g., lack of follow through on the original instruction or completing the task for the child), harsh or overreactive response (e.g., yelling, threatening), or an effective strategy such as restating the instruction and following through until the child has complied.
In the current study, disruptive behavior problems do not include direct symptoms of ASD (e.g., stereotypy; inattention) or other behavioral abnormalities such as drooling, Pica, or Bruxism. Although the specific symptoms of ASD and behavior abnormalities deserve attention and can be challenging for families, they were not addressed in this study.
Studies simultaneously examining parent stress, parenting behavior, child disruptive behavior problems, and ASD symptomatology are lacking. Most previous research has focused on child variables only or on one area of parenting (e.g., teaching skills to child, parent stress). The simultaneous investigation of these variables is important in further developing a comprehensive, family-based approach to treating children affected by ASD and disruptive behavior problems.
Method
Participants
A sample of 130 parents of children with a confirmed diagnosis of ASD was recruited through the Interactive Autism Network (IAN) Research Center at the Kennedy Krieger Institute and Johns Hopkins Medicine–Baltimore, sponsored by the Autism Speaks Foundation. The IAN (principal investigator [PI]: Dr. Paul A. Law; Johns Hopkins Medicine Institutional Review Board NA_00002750) is a national online autism registry that has enrolled more than 40,000 individuals with ASD and their family members. The diagnosis of ASD in the IAN database has been clinically validated as well as verified by a review of parent- and professional-provided medical records (Daniels, Rosenberg, Anderson, Law, Marvin, & Law, 2012; Lee et al., 2010). Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994, 2001) criteria were used for diagnosis, and resulted in a sample of 74 children diagnosed with autistic disorder, 32 with Asperger disorder, and 24 with pervasive developmental disorder–not otherwise specified (NOS). Parents from 36 states in the United States participated in the study. The data were collected from April to July 2012.
The children ranged in age from 3 to 11 years (M = 8.57, SD = 2.36). Of the 130 children, 116 (89.2%) were male and 14 (10.8%) were female. The parents ranged in age from 24 to 58 years (M = 39.81, SD = 6.56). Of the participants, 115 (88.5%) were biological mothers, 11 (8.5%) were biological fathers, and 4 (3%) were adopted mothers. Although participants were recruited from many states representing diverse geographical areas, there was extremely limited heterogeneity in terms of the ethnicity of the parents. The majority of the sample was Caucasian (90.8%) and married (77.7%). Education of parents varied: high school (5.4%), some college (30.8%), bachelor’s degree (37.7%), and advanced degree (26.1%). Household income ranged from less than US$15,000 to more than US$150,000.
Materials
Demographic survey
Parents completed a demographic/background form designed specifically for the study. The form included the participant’s age, child’s age, child’s diagnoses, relationship to the child (i.e., biological parent, step-parent, or adopted parent), race/ethnicity, yearly household income, years of education completed, and marital status.
Parent Stress Index–Short Form (PSI-SF)
The PSI-SF (Abidin, 1995) Total Stress scores were used as a comprehensive assessment of stress in all areas of the parenting role. The PSI-SF, Parental Distress (PD) subscale scores were used as a measure of parent stress that is not confounded by measures of child characteristics (e.g., disruptive behavior). The PSI-SF is a 36-item parent self-report questionnaire that yields a Total Stress score that is derived from three subscales: PD, Parent–Child Dysfunctional Interaction (P-CDI), and Difficult Child (DC). The PSI-SF is a widely used measure and yields strong psychometric properties (see Abidin, 1995, for a review). For instance, the PSI-SF has demonstrated concurrent validity (r = .94) with the long form version (Abidin, 1995) and has been used extensively within the ASD literature (Dunn, Burbine, Bowers, & Tantleff-Dunn, 2001; Robbins, Dunlap, & Plienis, 1991; Quinn, Carr, Carroll, & O’Sullivan, 2007). Parents who obtain a Total Stress raw score above 90 are considered to be experiencing clinically significant parenting stress. For the current study, Cronbach’s alphas for Total Stress, PD, P-CDI, and DC were .91, .85, .84, and .87, respectively.
Eyberg Child Behavior Inventory (ECBI)
The ECBI (Eyberg & Pincus, 1999; Eyberg & Ross, 1978) was used in this study to measure child disruptive behavior problems (e.g., noncompliance, oppositional behavior, aggression). The ECBI is a 36-item parent-report assessment for children between the ages of 2 and 16 years, which yields an intensity score reflecting the frequency of these behaviors. The clinical cutoff score is 131 for the intensity score (Eyberg & Pincus, 1999). The ECBI is a commonly used measure to assess clinically referred children for externalizing behavior disorders, including children with ASD (Brookman-Frazee, Taylor, & Garland, 2010). The ECBI has high internal consistency (α = .95) and good test–retest reliability (r = .86), and reliably discriminates between problem and nonproblem children (Robinson, Eyberg, & Ross, 1980). Several studies have shown the ECBI to be a reliable and valid measure in assessing common problem behavior, and to be sensitive to behavior change in response to treatment (e.g., Boggs, Eyberg, & Reynolds, 1990). For the current study, Cronbach’s alpha was .93.
Gilliam Autism Rating Scale–Second Edition (GARS-2)
The GARS-2 (Gilliam, 1995) was used as an estimate of the presence and frequency of ASD symptoms to later covary this dimension and examine it separately from common child disruptive behavior problems. The GARS-2 is a 42-item parent-report questionnaire that has been widely used in schools and research for children between the ages of 3 and 22 years (Gilliam, 1995; South et al., 2002). The GARS-2 is composed of the following three subscales: Stereotyped Behaviors (e.g., flaps hands, rocks back and forth, spins items not designed for spinning), Communication (e.g., repeats words, uses pronouns inappropriately), and Social Interaction (e.g., avoids eye contact, becomes upset when routines are changed). Gilliam (1995) reported excellent psychometric properties. Studies reveal internal consistency of .84 for Stereotyped Behaviors, .86 for Communication, .88 for Social Interaction, and .94 for the Autism Index. For the current study, Cronbach’s alphas were .82, .87, .82, and .92, respectively.
Parenting Scale (PS)
The PS (Arnold, O’Leary, Wolfe, & Acker, 1993) is comprised of 30 items and measures dysfunctional parental discipline techniques using a 7-point rating scale. It yields a Total Score and three factor scores: Laxness, a parenting technique associated with permissive discipline (e.g., giving in to a tantrum, failing to enforce rules); Overreactivity (e.g., displays of parental anger and irritability); and Verbosity (e.g., reasoning and verbalization in response to misbehavior). Lower scores indicate more effective strategies. The Verbosity score was not included in the current analysis as it has not emerged consistently in factor analytic studies with older children (Arnold et al., 1993; Irvine, Biglan, Smolkowski, & Ary, 1999). Arnold and colleagues (1993) reported test–retest reliability coefficients of .83 for Laxness, .82 for Overreactivity, and .84 for the Total Score. The current study yielded Cronbach’s alphas of .84 for Overreactivity, .81 for Laxness, and .86 for the Total Score. The Total Score as well as the Overreactivity and Laxness factor scores were used as measures of parenting discipline strategies.
Procedures
The IAN Research Project was the primary means of recruitment for the present study. IAN, a web project of Kennedy Krieger Institute, Baltimore, Maryland, is designed to accelerate the pace of ASD research by linking families of children with ASD and researchers. IAN sent emails to their registry consisting of families of children with a diagnosis of ASD between the ages of 3 and 11 years. The email included a link and a password to a secure website that interested participants followed to access the study materials. To help ensure participation, IAN sent reminder emails approximately 2 weeks and 3 weeks after the initial email. Following participation of the online portion, parents were sent a packet via mail that included the GARS-2, instructions to complete the GARS-2, a ticket for a raffle for US$150, a US$10 gift card to a national chain store, and a postage-paid return envelope. Survey Gizmo was used for the online questionnaires. All of the information collected was stored in a secure database that was transferred to a secondary secure database on a university server. The participation and response rate is unknown, as recruitment was restricted to the first 130 participants who responded to the survey. It is likely that some families attempted to reach the survey after the recruitment process had been closed. All mailed packets were sent within a week of online participation and returned within 2 months of online participation.
Outliers and excluded data
Each of the independent and dependent variables was screened for univariate outliers, defined as scores greater than 3 standard deviations above or below the group mean. This procedure revealed no outliers. Two participants had two or more items missing within the same subscale on the PSI-SF, and their PSI-SF scores were excluded from analyses. Two participants missed four or more items on the ECBI; their scores were considered invalid and excluded from analyses. Participants who did not return the GARS-2 (n = 17) were not included in analyses that used this score. This resulted in a final sample size of 110 families for the mediation analyses.
Results
Descriptive data for the sample on measures with clinical cutoffs are presented in Table 1. These data clearly document clinically significant levels of parent stress and comorbid child disruptive behavior problems for a large percentage of families. To establish justification of a possible indirect effect, a series of simple associations were conducted (see Table 2). Significant simple associations suggest that it is plausible to test for indirect effects.
Descriptive Data on Measures With Clinical Cutoff Scores.
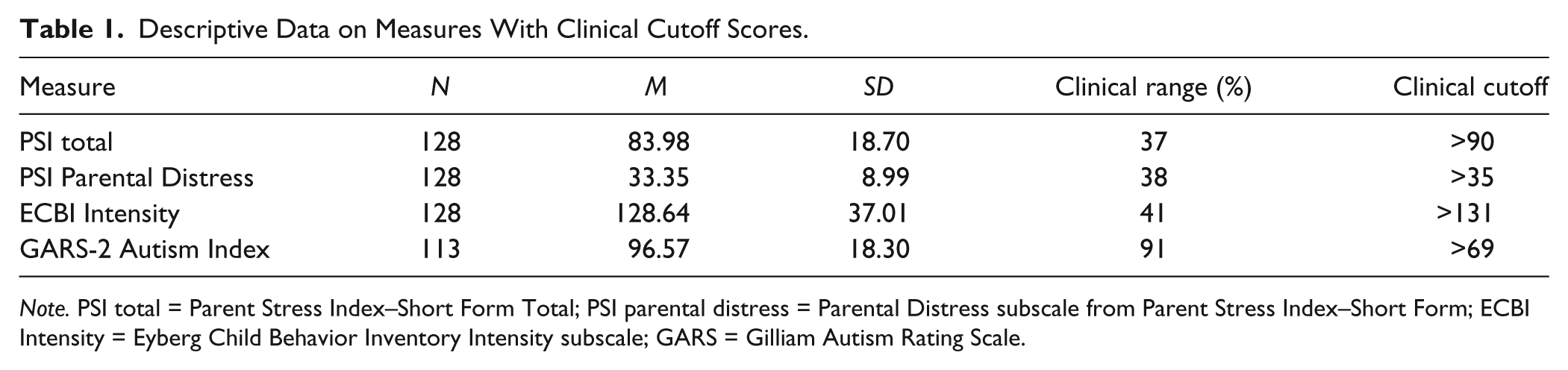
Note. PSI total = Parent Stress Index–Short Form Total; PSI parental distress = Parental Distress subscale from Parent Stress Index–Short Form; ECBI Intensity = Eyberg Child Behavior Inventory Intensity subscale; GARS = Gilliam Autism Rating Scale.
Dimension of Parenting and Child Symptoms Within Families.

Note. PSI total = Parent Stress Index–Short Form Total; PD subscale = Parental Distress subscale from Parent Stress Index–Short Form; ECBI Intensity = Eyberg Child Behavior Inventory Intensity subscale; Autism Index = Gilliam Autism Rating Scale Autism Index; PS total = Parenting Scale total; PS Laxness = Parenting Scale Laxness subscale; PS Overreactivity = Parenting Scale Overreactivity subscale.
p < .05. **p < .01. ***p < .001.
Mediation Models of Parent and Child Interactions
The main purpose of this investigation was to simultaneously assess key factors within the parent–child relationship. Mediation analyses were used to examine these more complex associations between multiple variables as depicted in Figure 1.
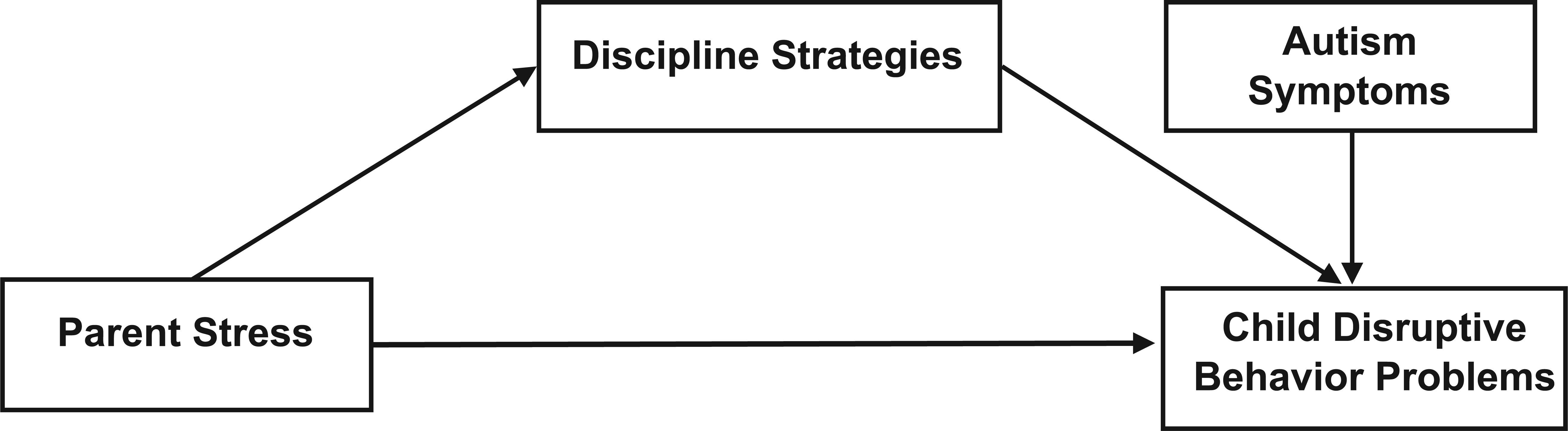
Parent and child mediation model within autism spectrum disorders.
In all subsequent analyses, level of ASD symptoms was used as a covariate, so that the associations between parent stress, parental discipline strategies, and child disruptive behavior could be examined independently. The recommended and preferred method for determining the statistical significance of a potential mediating variable (i.e., the indirect effect) is via the bootstrapping procedure (see Hayes, 2009, 2012; Preacher & Hayes, 2004, 2008). Bootstrapping utilizes resampling of the original distribution “to generate an empirically derived sampling distribution of the indirect effect” (Hayes, 2013, p. 106). A 95% confidence interval (CI) of the derived sampling distribution is constructed for the indirect effect. CIs that do not include 0 are considered statistically significant at the .05 level. A measure of effect size cannot be calculated with the analyses due to the presence of a covariate. Following the recommendations of Hayes (2012), 1,000 samples were derived from the original sample by a process of resampling with replacement. Refer to Table 3 for a summary of the results.
Bootstrap Analyses of Indirect Effects for Mediation Model.
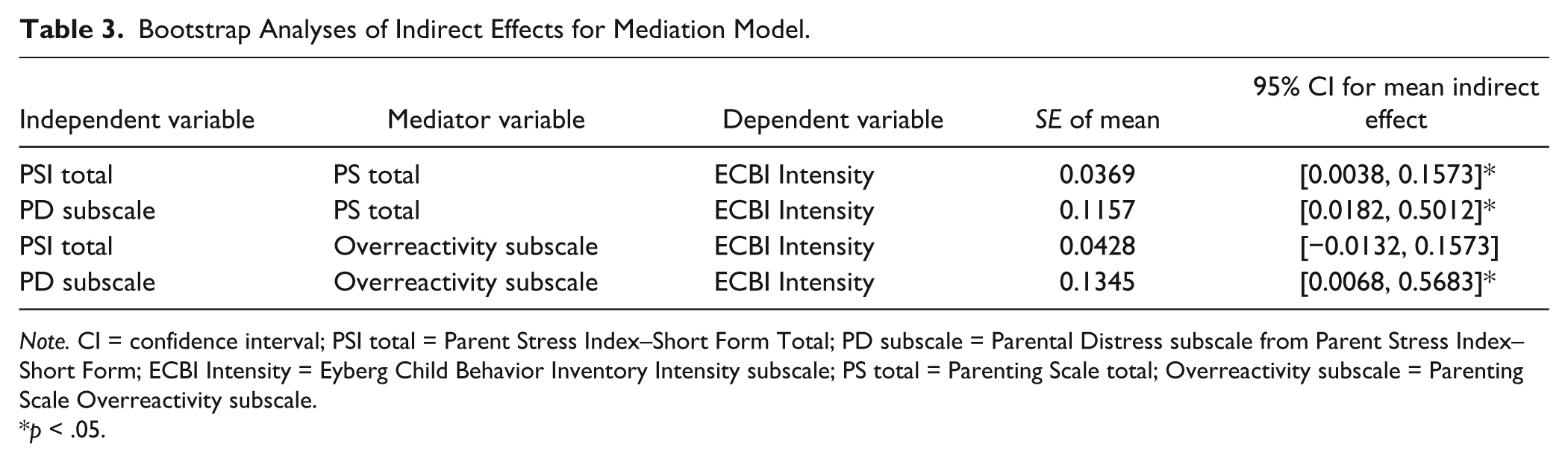
Note. CI = confidence interval; PSI total = Parent Stress Index–Short Form Total; PD subscale = Parental Distress subscale from Parent Stress Index–Short Form; ECBI Intensity = Eyberg Child Behavior Inventory Intensity subscale; PS total = Parenting Scale total; Overreactivity subscale = Parenting Scale Overreactivity subscale.
p < .05.
To test the hypothesis that parental discipline strategies mediate the association between parenting stress and child disruptive behaviors, the Total Score on the Parenting Scale was used as a measure of discipline strategies, and PSI Total Score was used as a measure of parenting stress. ECBI Intensity score was used as a measure of the frequency of child disruptive behaviors. Results indicate a significant mediation effect (SE = 0.0369, 95% CI = [0.0038, 0.1573]), indicating that parental discipline strategies mediate the link between parenting stress and frequency of child disruptive behavior.
To further examine the specific aspects of parent stress, the Total Score on the PS was used as a measure of discipline strategies, and the PD subscale score of the PSI-SF was used as a measure of parenting stress. Results indicate a significant mediation effect (SE = 0.1157, 95% CI = [0.0182, 0.5012]). Thus, parental discipline strategies serve as a mediator between parent stress and child disruptive behavior.
To more closely examine specific types of discipline strategies, additional exploratory analyses were conducted. To further investigate the significant mediation effect of parental discipline strategies, the Overreactivity subscale of the PS was analyzed separately within the same model. For this analysis, the PSI-SF Total score was used as a measure of parenting stress, and the ECBI Intensity score was used as a measure of the frequency of child disruptive behaviors. Results do not indicate a significant indirect effect (SE = 0.0428, 95% CI = [−0.0132, 0.1573]). For the second analysis, the Overreactivity subscale of the PS was used as a measure of discipline strategies, and PD subscale score of the PSI-SF was used as a measure of parenting stress; the ECBI Intensity score was used as a measure of the frequency of child disruptive behaviors. Results indicate a significant mediation effect (SE = 0.1345, 95% CI = [0.0068, 0.5683]). Thus, parental discipline strategies that involve harsh and over corrective interactions serve as a mediator between parent stress and child disruptive behavior. The other subscale on the PS was not investigated, as it did not produce a significant zero-order correlation between the model variables.
Discussion
We investigated the parent–child relationship by examining associations between parent stress, parental discipline strategies, common child disruptive behavior problems, and level of ASD symptoms. Collectively, we demonstrated complex associations among these variables. Forty-one percent of children displayed clinical levels of disruptive behavior problems. These results are consistent with Kaat and Lecavalier’s (2013) review of recent studies of children with ASD documenting prevalence rates of comorbid oppositional defiant disorder and conduct disorder up to 37%. Child disruptive behavior problems often result in strained parent–child relationships (Gadow, Devincent, Pomeroy, & Azizian, 2005; Lecavalier, 2006; Lecavalier et al., 2006; Tonge & Einfeld, 2003). Parents were highly likely to experience clinical levels of parent stress, corroborating the substantial body of literature on parent stress in families of children with ASD (Blacher & McIntyre, 2006; Dunn et al., 2001; Eisenhower, Baker, & Blacher, 2005; Gupta, 2007; Tomanik, Harris, & Hawkins, 2004).
A series of mediation analyses were conducted to examine the complex associations involved within the parent–child relationship. We demonstrated that parental discipline strategies mediated the association between parent stress and child disruptive behavior problems. The use of certain discipline strategies may result in an increased risk for the development or maintenance of disruptive behavior problems. Specifically, we examined parental discipline strategies that are classified as harsh or punitive. After analyzing the model with an index of parent stress calculated independently of child behavior, harsh parental discipline strategies mediated the association between parent stress and intensity of child disruptive behavior problems. Our results are the first to examine different parenting strategies and their influence on stress and child variables. These findings support the growing emphasis in conducting behavioral parent training to decrease child disruptive behavior problems through improving the parent–child relationship and modifying parental discipline strategies (e.g., Aman et al., 2009; Bearss et al., 2013; Durand et al., 2013).
Our findings provide further support for theoretical models outlining complex associations between parent stress, parenting behavior, and child behavior problems (Deater-Deckard, 1998; Hastings, 2002). This is consistent with Osborne and colleagues (2008), who found that the parent behavior of limit-setting mediated the association between parent stress and child disruptive behavior problems. Lecavalier et al. (2006) found bi-directional effects between parent stress and child disruptive behavior problems. However, Zaidman-Zait et al. (2014) found evidence for both bi-directional and unidirectional effects for parent stress and child disruptive behavior. Thus, one plausible interpretation of our results is that high levels of stress may impair parents’ ability to use effective discipline strategies, which in turn influences child disruptive behavior. This is supported by Totsika et al. (2013) who found that maternal well-being predicted later child disruptive behavior. Alternatively, ineffective parenting may lead to increases in child disruptive behavior problems, which in turn increases parents’ stress. However, parent stress and parental behavior are also likely bi-directional (Osborne & Reed, 2010). In addition, child disruptive behavior problems may lead to parent stress and adversely affect parents’ ability to use effective discipline strategies. Therefore, more research is needed to explore these reciprocal associations. We hypothesize that parenting behaviors have a direct effect on child disruptive behavior problems and should be an area for treatment and future research.
The current study has several notable strengths. First, the study had a large sample of children across the United States. All had a confirmed diagnosis of ASD, with varying levels of ASD symptoms. Our sample included young children, who most often received intervention. Well-validated measures were used to assess multiple factors simultaneously. Our data support existing theoretical models, providing a more thorough understanding of interactions involved within the parent–child relationship. The level of ASD symptoms was measured separately from disruptive behavior problems, which yields a clearer interpretation of results. The rate of clinical levels of disruptive behavior problems was documented.
This study also had limitations. Although participants represented a variety of geographic locations, the sample was not ethnically diverse. Caution should be used when applying these results to parents of children with ASD of other ethnicities. All data were obtained through parent report, and this common method variance may have contributed to the associations among variables. Future research would benefit from multiple informants to reduce method variance. Participants were registered with an online network. These parents have access to considerable information about ASD and may be more proactive in their parenting role than parents who are not registered with this network. It is unclear to what extent families in our study may differ from other families. In addition, our study relied solely on rating scales. Direct observation would greatly enhance the current findings. Finally, while the ECBI has often been used with children with ASD, separate norms have not been examined.
Future research is necessary to replicate the current findings with a more ethnically diverse sample and with families who are not engaged in parent groups or research groups. Disruptive behavior problems in children with ASD warrant further study, including identifying when disruptive behaviors emerge in children with ASD, and how those behaviors may change over time. Longitudinal studies that examine how ASD symptom severity, child disruptive behavior problems, and parent stress interact over time would be beneficial. Temporal precedence and directionality would allow for improved treatments and allow treatments to follow an order that may maximize gains for both the child and the parent. Assessing the rate of disruptive behavior problems for parents versus other providers (e.g., teachers) may provide further insight into parent–child interactions.
Direct observation of parent–child interactions and parent strategies would allow for a functional analysis to determine how certain strategies relate to child disruptive behavior problems. The existing parent training programs for children with ASD primarily focus on child behavior and do not emphasize changes in parent–child interactions. Treatments that reduce parent stress should assess if collateral changes occur in parenting strategies, child disruptive behavior, and child gains. Parent training programs designed to improve ASD symptoms alone should be compared with programs designed to improve ASD symptoms and decrease child disruptive behavior problems. Outcomes should include measures of parent and child variables.
Results from the current study have several clinical implications. Existing parent training programs for young children with ASDs should focus on parents as well as the children (Karst & Van Hecke, 2012). Comprehensive treatments for children with ASD should take into account parents’ stress, well-being, and specific challenges that exist in the parenting role. Parents may benefit from specific behavioral treatments to handle common child disruptive behavior problems when problems are oppositional in nature versus a skill deficit.
It is hoped the current study contributes to gaps within the ASD literature and will serve as a stepping stone for future research in this area. Overall, the study demonstrated that a large proportion of children with ASD present with high levels of child disruptive behavior. Parents of children with ASD exhibit elevated levels of parent stress. Children with more frequent and a greater number of ASD symptoms tended to have more behavior problems, and these families tended to report higher levels of parent stress. Evidence-based practices for parents to improve child ASD symptomatology largely do not address parent stress, child disruptive behavior problems, and the family context as a whole. Research into comprehensive treatments for children with ASD should focus on needs of the family as a whole as many variables are interrelated.
Footnotes
Acknowledgements
The authors would like to thank the families who spent their time completing the study and the Interactive Autism Network for assistance in recruitment. In addition, the authors would like to thank R. Matt Alderson, PhD, and Lana Beasley, PhD, for reviewing the manuscript and serving on the panel for the lead author’s master’s thesis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.