
Abstract
Peer-mediated instruction and intervention (PMII) is a systematic, evidence-based method for addressing the social-communication needs of children with autism spectrum disorder (ASD). Despite existing research on this practice, gaps remain in the implementation of PMII. The purpose of this empirical review was to examine recent applications of this evidence-based practice and systematically assess the quality of the analytic approaches implemented. Recent studies selected for this review included participants with ASD and targeted social-communication skills. The Scientific Merit Rating Scale (SMRS) was used to review the quality of the research studies, and the results suggest that PMII continues to be an effective practice. These results indicate that future research should focus on larger study Ns, particularly for those who are preschool-age, and include measures of generalization and maintenance as well as treatment integrity measures of peers’ actions. The effectiveness of PMII relative to positive developmental outcomes is discussed.
The study of peer-mediated instruction and intervention (PMII) was conceived with a focus on creating supportive contexts for the social interactions of individuals with disabilities as a response to the movement toward inclusion for students with disabilities in classrooms (Odom et al., 2003; Odom, Hoyson, Jamieson, & Strain, 1985; Odom & Strain, 1986). More recently, researchers have continued to study the impact of PMII on social skills development of young children with autism spectrum disorders (ASD) by focusing on training and teaching peers to initiate and respond to socialization with the learner with ASD in the context of preschool classroom environments (e.g., Katz & Girolametto, 2013; Owen-DeSchryver, Carr, Cale, & Blakeley-Smith, 2008; Thiemann & Goldstein, 2004).
PMII is a method for teaching “typically developing peers ways to interact with and help learners with ASD acquire new social skills by increasing social opportunities within natural environments” (Neitzel, 2008, p. 1). The intervention begins with the selection and training of peers, with the purpose of teaching them specific skills and strategies needed to successfully communicate, interact, and sustain communicative interactions with their classmates with ASDs (Neitzel, 2008; Odom & Strain, 1986; Sperry, Neitzel, & Engelhardt-Wells, 2010). In early childhood settings, the initial training is followed by a session where the peer and learner with ASD play in a supported and structured setting. This structured play session provides the peer an opportunity to receive coaching, prompting, or reinforcement from the trained adult in the environment (Katz & Girolametto, 2013; Neitzel, 2008; Sperry et al., 2010). Next, PMII is implemented in the natural classroom setting with attention to classroom arrangement and the availability of meaningful activities and materials that promote interactions between the learner with ASD and his peers (Jung, Sainato, & Davis, 2008; Neitzel, 2008; Sperry et al., 2010). The trained peers are guided to play in the same area or attend the same cooperative learning group as the child with ASD. Through this process, multiple opportunities to facilitate social-communication skills are incorporated and include learning to respond to others, engaging in reciprocity within activities, as well as interacting consistently with individual peers in structured group settings (Goldstein, Kaczmarek, Pennington, & Shafer, 1992; Neitzel, 2008; Odom & Strain, 1986; Sainato, Goldstein, & Strain, 1992). Additionally, typically developing peers also benefit from opportunities to practice social skills (Laushey & Heflin, 2000).
PMII is particularly effective for learners with ASD because they may not be motivated to simply observe their peers without reinforcement; this is a challenge that is addressed through the implementation of this intervention. In PMII, when the learner with ASD receives social-communication bids and responses from a peer, the learner can advance beyond simply observing and be reinforced for his social initiations and responses (DiSalvo & Oswald, 2002; Koegel, Dyer, & Bell, 1987; Schmidt & Stichter, 2012). PMII facilitates multiple opportunities for children with ASD to engage in activities, as their peers become models for engaging with the activity appropriately and meaningfully (Jung et al., 2008; Sperry et al., 2010). The inclusive classroom environment provides tremendous potential for continuous opportunities for social interactions and increased engagement for children with ASD and their typically developing peers in a variety of activities both in and out of the classroom (Downing, 2010; Hart & Whalon, 2011; Ryndak & Alper, 2003). But, in order for children with ASD to optimally benefit from such inclusive practices, teachers must employ specific, evidence-based strategies and interventions to ensure the inclusive placement is providing optimal experiences and repeated opportunities to support their social-communication needs (Bass & Mulick, 2007; Hart & Whalon, 2011; Lee, Odom, & Loftin, 2007; Sperry et al., 2010).
Numerous studies have indicated that PMII is an effective, evidence-based intervention that capitalizes on the potential social learning opportunities when children with ASD are able to watch and interact with their peers (Goldstein et al., 1992; Kasari, Rotheram-Fuller, Locke, & Gulsrud, 2012; Katz & Girolametto, 2013; National Autism Center [NAC], 2009; National Professional Development Center [NPDC] on Autism Spectrum Disorders, 2010; Odom et al., 2003). In recent years, there has been a greater focus on PMII as an evidence-based practice (EBP) due to the increase in children identified with ASD. As such, it is necessary to identify and implement the most effective practices for these children (ASD: Data and Statistics, Prevalence, 2014; Carter, Sisco, Yun-Ching, & Stanton-Chapman, 2010; NAC, 2009; Schmidt & Stichter, 2012).
PMII has met the NPDC rigorous scientific criteria for being considered an EBP (NPDC on Autism Spectrum Disorders, 2010). In addition to the NPDC, the NAC also evaluated the most effective interventions for a wide range of children with ASD (NAC, 2009). The NAC reported on the quality of empirical research on interventions for individuals with ASD, and included an analysis of reviewed literature published between 1957 and 2007 that evaluated studies for treatment effects and in addition, created the Scientific Merit Rating Scale (SMRS; NAC, 2009) to evaluate studies. It is an objective rating scale and includes five categories: research design, measurement of the dependent variable, measurement of the independent variable (treatment integrity), participant ascertainment, and generalization/maintenance. Within each category, specific criteria are listed, and each set of criteria corresponds to a score of zero to five. For example, the criteria for a score of 5 (highest possible) in treatment integrity include (a) implementation accuracy measured at greater than or equal to 80%, (b) implementation accuracy measured in 25% of total sessions, (c) and interrater agreement for treatment fidelity greater than or equal to 80%. Using the SMRS, the NAC determined that PMII was an “established” practice, meaning the following criteria have been met: (a) several published, peer-reviewed studies exist with SMRS scores of three, four, or five and (b) beneficial treatment effects for a specific target have been documented. While PMII has been identified as an EBP, continued investigation of the current applications of this practice is warranted to continue to advance the practice and to understand the implications for future research and practice. Since 2007, PMII research has been conducted and has garnered more attention based on the significance and impact of inclusive practices reported in classroom contexts (Ganz et al., 2012; Kasari et al., 2012; Katz & Girolametto, 2013).
The purpose of this systematic review was to evaluate current PMII research published between 2004 and 2014 and examine the design and methodology of recent studies as well as the quality of the analytic approaches implemented. For this review, we narrowed the search to focus on those studies that used PMII to address social-communication needs of learners with ASD. Social-communication skills of children with ASD are pivotal to their success in inclusive settings; therefore, we selected only studies that addressed such skills to bring focus to the experimental design, methodology, outcomes, and future directions for the study of PMII (Bass & Mulick, 2007; Hart & Whalon, 2011). This is in contrast to a review conducted by Chan and colleagues (2009), which included articles in which both social-communication and academic needs were addressed. Further, Chan and his colleagues analyzed the method of training, intervention components, and certainty of evidence, but they did not use a robust analytic measure that would examine indicators of quality research and EBP (NAC, 2009), such as the SMRS. In addition, Chan’s review did not restrict the publication years of selected studies. Thus, this current review will describe the quality of current PMII empirical research published within the last 10 years, depict the growth and expansion of this practice as determined by published studies, examine implications for practice in inclusive settings, and explore future directions for research given the increasing number of individuals with ASD included in general education classrooms.
Systematic Empirical Literature Review
The specific aims of this review include the following: (a) describe and analyze the design, methodological, and analytic approaches used in PMII research published between the years of 2004 and 2014; (b) examine the sample of participants and settings of recent PMII research; (c) examine outcomes of recent PMII studies; (d) analyze the quality of the recent studies of PMII with respect to research design, generalization and maintenance, and treatment integrity; (e) explore the implications for practice for teaching children with ASD; and (f) outline gaps in the research and propose directions for future research given the most current PMII literature.
Literature Search: Methodological Approach
A systematic search of the literature was conducted by the first author, beginning with an electronic database search of EBSCOhost, Academic Search Complete, ERIC, PsycARTICLES, and PsycINFO, using various combinations of the following keywords: peer-mediated intervention, peer-mediated, peer interactions, peer mediation, peer intervention, peer training, peer socialization, autism, autism spectrum disorder, ASD, evidence based interventions, social communication interventions. The search revealed 139 abstracts, which were evaluated and selected for a full-text reading by the first author if they met the following criteria: empirical articles published in peer-reviewed journals between 2004 and 2014, included an intervention for participants with ASD, and included an intervention which was peer-mediated. The abstract review resulted in 36 full-text articles to be read by the first author; additionally, a second evaluator reviewed the same 139 abstracts to select for full-text reading, and interrater agreement was 100%. Studies were excluded from this review for the following reasons: (a) if the recipients of the intervention did not exclusively include children with ASD; (b) if the study did not include typically developing peers; (c) if peer training did not occur; or (d) if the intervention did not target social-communication skills. After reading the 36 full-text articles and applying the criteria for selection described above, the first author identified a total of 17 studies for inclusion in this review. The method for the search process was aligned with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement (Moher, Liberati, Tetzlaff, Altman, & The PRISMA Group, 2009). Figure 1 depicts the PRISMA flow diagram for the search process used in this review.
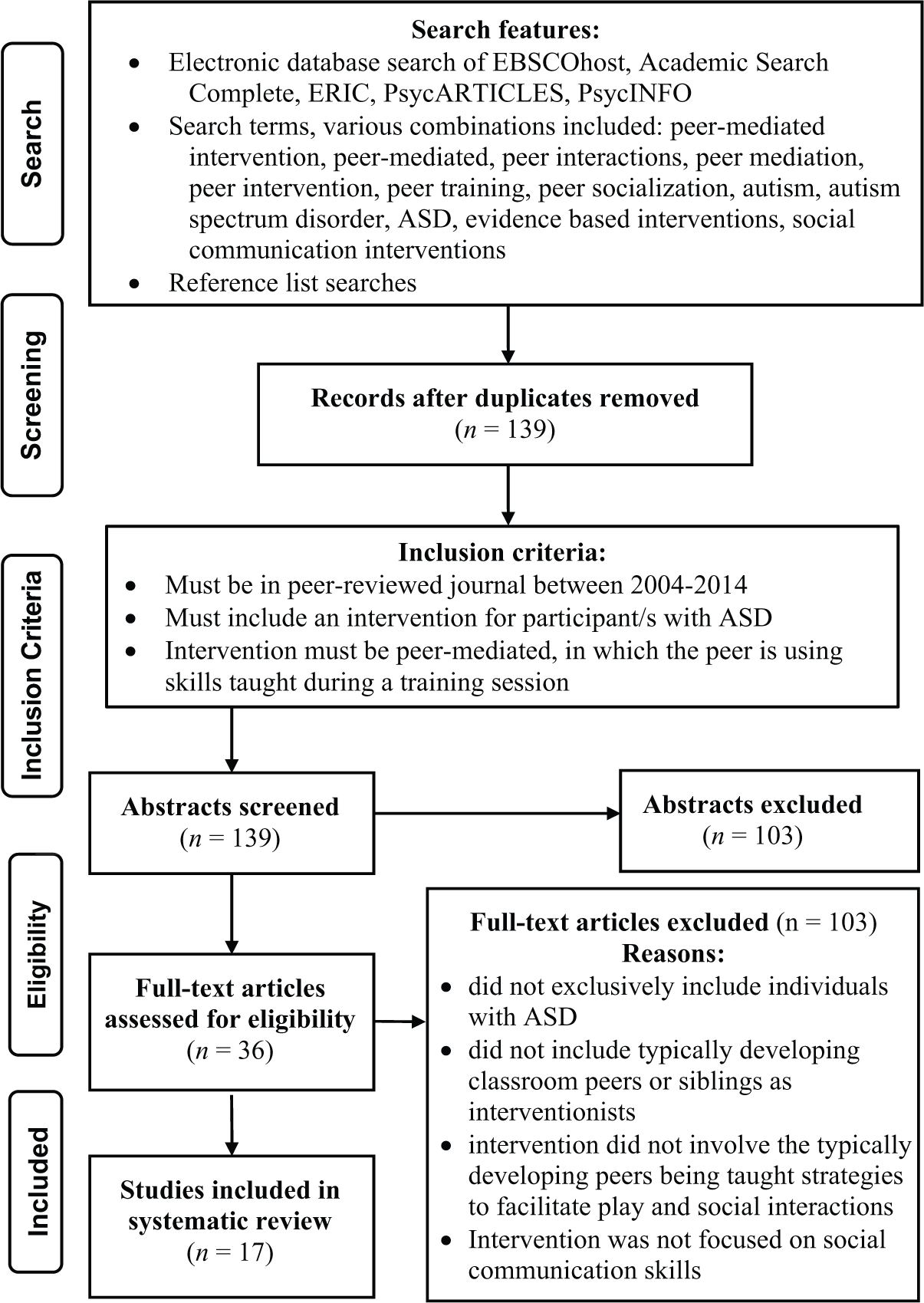
Flow diagram for the search and inclusion criteria for studies in this review.
Systematic Review: Experimental Design and Methodology
The first aim of this review was to describe and analyze the design, methodological approaches, and analytic techniques used in recent PMII research. The most noticeable finding among these 17 studies was that 16 exclusively utilized single-subject design methods. This frequency of the use of single-subject design methods is consistent with previous research in PMII and social skills interventions in general (Matson, Matson, & Rivet, 2007; Odom et al., 2003; Odom & Strain, 1986; Odom et al., 1985). Though most of the studies identified by this review were single-subject design studies, one study used a large-group randomized control trial (RCT) design (Kasari et al., 2012) that compared the effectiveness of two interventions: one where the adult met with the child with ASD and an intervention where the peers in the classrooms were taught strategies for interacting with the child with ASD and subsequently engaged the child on the playground. This RCT design provided an opportunity for comparison of the effects of two different social skills interventions for a large group of elementary school-age children with ASD. The design of this study revealed noteworthy findings: when the adults interacted with children in an intervention context, the results were not as positive as when the intervention also included peer-mediated approaches. Further, the results of this study suggest that the effectiveness of PMII was statistically significant when peer-mediated instruction was incorporated, as compared with interventions facilitated exclusively by an adult (Kasari et al., 2012).
Participants and settings
Fifteen of the studies that met the selection criteria for this review included participants with ASD over the age of 5. Table 1 includes the number of participants in each study and their ages. The majority of earlier research studies on PMII includes younger, preschool-age children (Odom et al., 1985; Odom & Strain, 1986; Odom & Watts, 1991; Owen-DeSchryver et al., 2008). In fact, as shown in Table 1, nine of the 17 studies published between 2004 and 2014 included participants who were 10 years of age or older. Further, only three of the studies included participants under the age of 5. This is a critical finding, as it highlights the need for continued high-quality studies and applications of PMII for preschool populations.
Study Sample, Location, and Quality (Research Design, Generalization, and Maintenance).
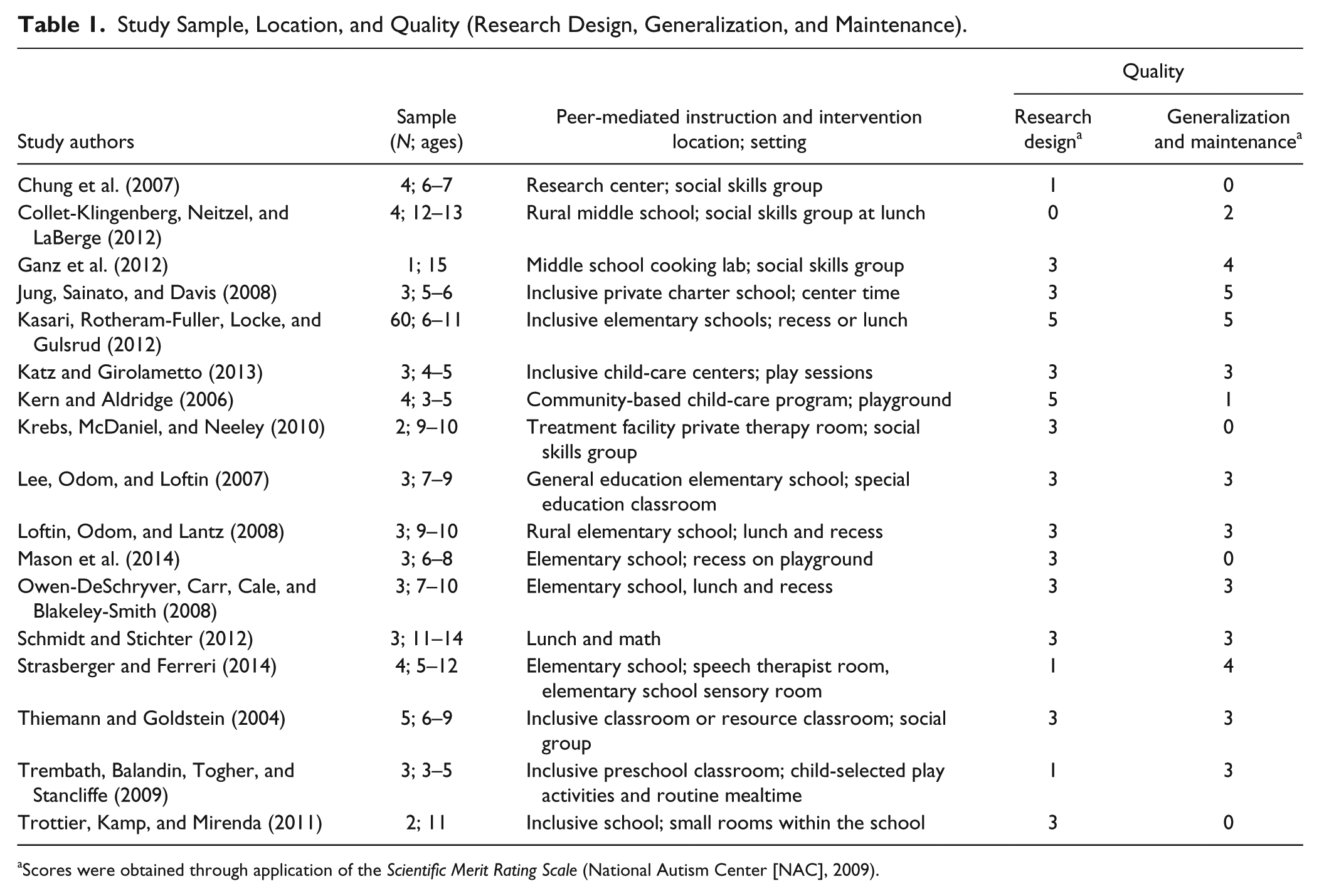
Scores were obtained through application of the Scientific Merit Rating Scale (National Autism Center [NAC], 2009).
Recent studies of PMIIs have been conducted both in social skills groups as well as in natural contexts and settings, such as the general education classroom. Table 1 includes a list of the location and setting for each study. For example, some studies were conducted in a school setting, but the intervention itself was not conducted in the general education classroom; rather, it was conducted in a social skills group or other separate setting (Collet-Klingenberg, Neitzel, & LaBerge, 2012; Ganz et al., 2012; Strasberger & Ferreri, 2014; Trottier, Kamp, & Mirenda, 2011).
Study outcomes of PMII
PMII studies have demonstrated effectiveness for increasing the social-communication skills for learners with ASD (e.g., Ganz et al., 2012; Kasari et al., 2012; Lee et al., 2007). All of the studies included in this review documented positive outcomes and increases in social-communication skills in both the frequency and duration of these skills. Additionally, several studies demonstrated a functional positive relationship upon introduction of PMII. In addition, several of these studies reported increases in the number of initiations and responses used by individuals with ASD (Jung et al., 2008; Owen-DeSchryver et al., 2008; Strasberger & Ferreri, 2014). Other studies documented increased duration of the interactions of the child with ASD and the peer (Katz & Girolametto, 2013; Lee et al., 2007; Schmidt & Stichter, 2012). In one study, the children with ASD increased number of gestures, verbal utterances, vocalizations, and activations of their communication device (Trottier et al., 2011). Additionally, Kasari and colleagues (2012) found that an intervention that was peer-mediated was more effective than one that was implemented by paraprofessionals for improving the amount of times the student with ASD was engaged with peers, as compared to being unengaged with others.
Systematic Review: Indicators of Research Quality
While it is important to examine the results of these studies, it is also critical to systematically review the quality of the research design methods utilized (Cook, Tankersley, & Landrum, 2009; Gersten, Fuchs, Coyne, Greenwood, & Innocenti, 2005; Odom et al., 2005). Such analyses of the quality of empirical studies can inform necessary future directions of research to continue to advance this practice. In their report, the NAC (2009) evaluated studies for the quality of research methods using the SMRS, which was specifically designed and used to evaluate the quality of studies that included individuals with ASD as participants. Therefore, given that a selection criterion for our review was that the study included participants with ASD, the SMRS was considered to be the most appropriate tool to use to review the quality of research selected for inclusion in this review. The SMRS provides an objective rating of the scientific merit of the study’s research design, and this is the first systematic review to date that has utilized the SMRS for purposes of evaluating the quality of peer-mediated intervention studies. The SMRS provides a rigorous and objective method for analyzing research design quality based upon specific, fact-based criteria, including the number of comparisons of control and treatment conditions, number of participants, and number of data points per condition. Additionally, in their review, Chan and colleagues (2009) evaluated studies for “certainty of evidence”; however, they did not employ a robust, scientific measure such as the SMRS, likely due to the timing of the NAC’s (2009) report. Therefore, given the availability of the SMRS and the need to identify effective interventions for individuals with disabilities (Cook et al., 2009), it was appropriate to apply the SMRS criteria to analyze the quality of PMII research included in this review. For the purposes of this targeted review, we applied the SMRS guidelines to analyze the quality of the following elements of each study: research design, generalization and maintenance, and measurement of the independent variable in each study. These three SMRS indicators of research quality were considered central in understanding the variability in the current research studies, as well as critical in corroborating the findings of Chan et al.’s (2009) review; the lack of treatment integrity measures were noted, thus it was important to examine any changes in treatment integrity reporting in studies since 2009.
Research design
In the current review, the SMRS was used to assess the quality of each study’s research design. The main considerations for research design in the SMRS include the following: (a) number of comparisons of control and treatment conditions; (b) number of data points per condition; and (c) number of participants; and (d) the potential for data loss (NAC, 2009). The criteria for research design quality are equivalent for all single-subject designs; however, the NAC offers different criteria for studies that used alternating treatments design (NAC, 2009). Within the SMRS, each number on the rating scale (0–5) is associated with specific set of criteria for scoring. To ensure consistency with analysis and scoring in this review, each study needed to meet all of the criteria for a score to be assigned that specific score in this review. For example, to be assigned a rating of three in research design, a study needed to include all of the following components: (a) minimum of two comparisons of control and treatment conditions; (b) greater than three data points per condition; (c) greater than two participants; and (d) have some possible data loss (NAC, 2009). In the event that a study did not meet all of the criteria for a specific score, we assessed the study for meeting the criteria for the next, lower tier score. The first author and a second rater independently read each of the 17 studies included in this review and rated each for quality of research design; Interrater agreement was calculated at κ = 100% (Cohen, 1960). As depicted in Table 1, 11 of the studies selected for this review demonstrated sound research design, scoring a three or greater when the SMRS standards were applied.
Despite the large number of studies that scored three or greater, there were others that did not demonstrate the same rigor in their research designs. Among the articles in this review, the most common reasons for an SMRS score of two or less in research design was including too few participants (Ganz et al., 2012; Krebs, McDaniel, & Neeley, 2010; Trottier et al., 2011) and the number of data points per condition not being greater than three (Chung et al., 2007; Katz & Girolametto, 2013; Strasberger & Ferreri, 2014). A small number of participants is common in research including participants with ASD; however, given that one study selected for this review included a large number of participants to conduct an RCT (Kasari et al., 2012), it is possible to include larger numbers of participants. It is important to note that this RCT met the SMRS criteria for a score of five in research design for a group study because it included two groups, random assignment, and greater than 10 participants. Another reason for a low score in research design was related to the number of data points per condition not being greater than three. Several studies had at least one baseline condition with two or three baseline data points (Chung et al., 2007; Katz & Girolametto, 2013; Schmidt & Stichter, 2012; Strasberger & Ferreri, 2014; Trembath, Balandin, Togher, & Stancliffe, 2009).
Generalization and maintenance
In addition to research design, the quality of generalization and maintenance measures of each study was also analyzed by applying the SMRS standards to the generalization and maintenance data reported in each study. Table 1 includes a list of the SMRS scores (0–5) assigned to each study for the generalization and maintenance of the intervention. The first author and a second rater reviewed all of the articles selected for inclusion in this review and rated the quality of generalization and maintenance measures; interrater agreement was calculated at κ = 100% (Cohen, 1960).
As depicted in Table 1, five studies included in this review were rated zero for generalization and maintenance according to the SMRS criteria. While many studies scored low for this category, seven studies were rated moderately, with a score of three. Of these studies that scored three, some included only maintenance measures (Loftin, Odom, & Lantz, 2008; Thiemann & Goldstein, 2004), while others included only generalization measures (Lee et al., 2007; Schmidt & Stichter, 2012; Trembath et al., 2009). According to the SMRS, for generalization and maintenance quality, studies were scored as a “three” because they either included generalization measures or maintenance measures, but not both. The SMRS ratings of four and five for generalization and maintenance require that both generalization and maintenance measures be included. The use of generalization measures in recent PMII studies is important to examine, particularly since PMII is an intervention that promotes generalization for learners with ASD in interactions with their peers in natural settings (Neitzel, 2008; Schmidt & Stichter, 2012; Sperry et al., 2010). Currently, there are few studies that report on PMII generalization outside of the classroom context. In fact, of the studies in this review that included generalization and maintenance measures (Ganz et al., 2012; Jung et al., 2008; Kasari et al., 2012; Lee et al., 2007; Schmidt & Stichter, 2012; Strasberger & Ferreri, 2014; Trembath et al., 2009), none of them included the child’s home as a generalization setting.
Treatment integrity
The quality of measurement of treatment integrity for each of the studies was also examined by evaluating the implementation accuracy, the number of sessions for which implementation accuracy data were collected, and the presence of interobserver agreement (IOA). SMRS scores were assigned to each study as an overall measure for the quality of measurement of the independent variable (see Table 2).
Quality: Treatment Integrity Data Across Studies.
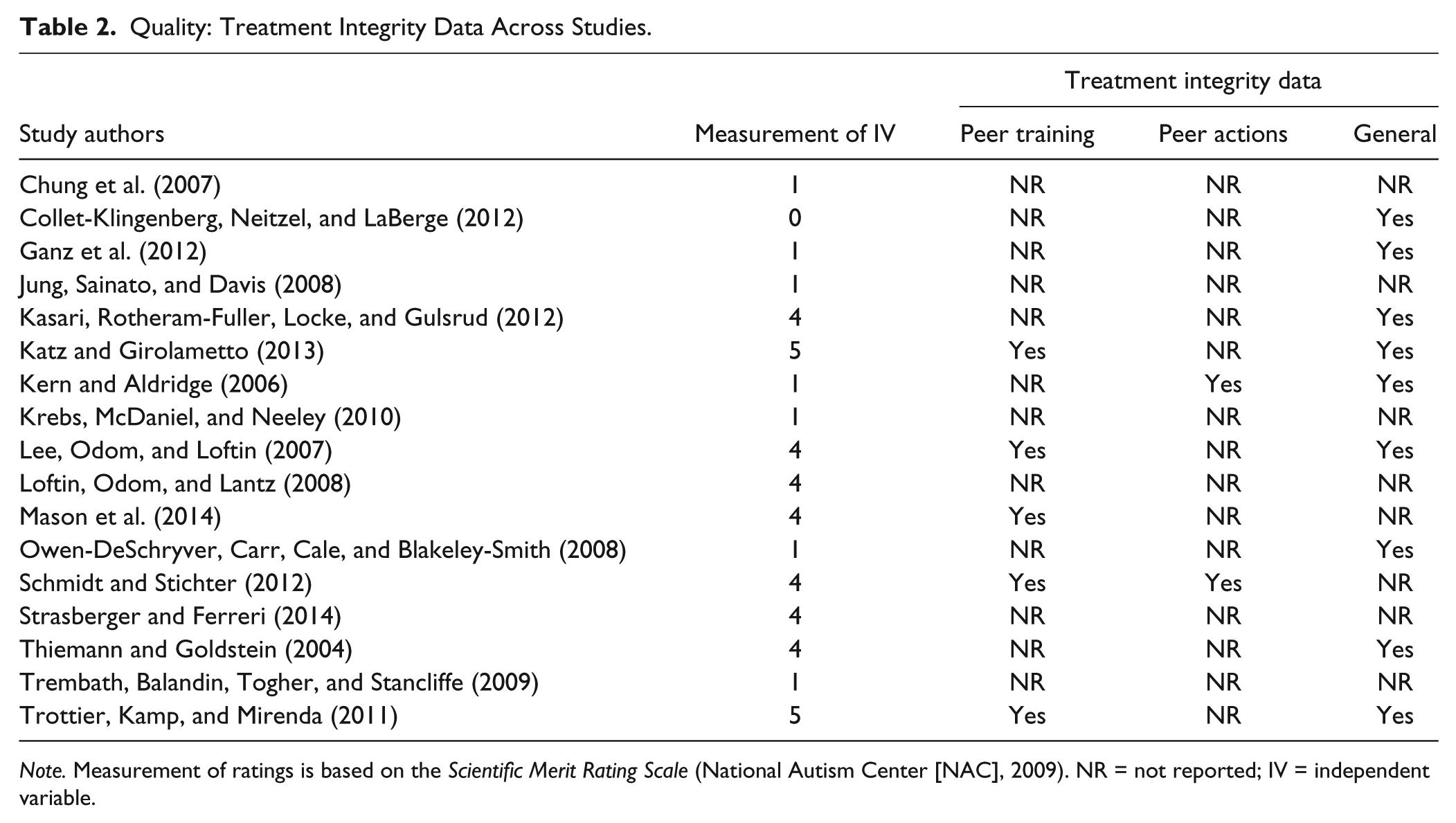
Note. Measurement of ratings is based on the Scientific Merit Rating Scale (National Autism Center [NAC], 2009). NR = not reported; IV = independent variable.
In addition, interrater reliabilities were calculated after the first and second author rated each of the 17 articles for treatment integrity, and the agreement for the SMRS treatment integrity ratings was κ = 89.82% (Cohen, 1960). The results of the analysis of the quality of measurement of the independent variable indicated a discrepancy across included studies because a similar number of studies were rated high (Kasari et al., 2012; Katz & Girolametto, 2013; Lee et al., 2007; Loftin et al., 2008; Mason et al., 2014; Schmidt & Stichter, 2012; Strasberger & Ferreri, 2014; Thiemann & Goldstein, 2004) as were rated low (Chung et al., 2007; Collet-Klingenberg et al., 2012; Ganz et al., 2012; Jung et al., 2008; Kern & Aldridge, 2006; Krebs et al., 2010; Owen-DeSchryver et al., 2008; Trembath et al., 2009). Nine of the studies in this review included adequate measurement of the independent variable by scoring a four or five when the SMRS rating scale was applied. However, the remaining studies either scored a one or zero; in fact, six studies in this review did not include measures of treatment integrity at all. Only two studies included in this review met the criteria for a score of five for measurement of the independent variable (Trottier et al., 2011; Katz & Girolametto, 2013). According to the SMRS, a score of five for treatment integrity would be assigned to a study that met the following criteria: implementation accuracy measured at greater than or reached 80% for elements of the intervention for which data were collected, implementation accuracy measured in 25% of total sessions, IOA for treatment integrity is greater than or reached 80% for elements of the intervention for which data were collected.
Of the studies that included treatment integrity measures, it was fairly common for treatment integrity data to be collected only during the peer-training phase of the intervention (Katz & Girolametto, 2013; Lee et al., 2007; Schmidt & Stichter, 2012; Trottier et al., 2011). On the other hand, it was far less common for data to be collected for the peer’s actions during the intervention; that is, only two of the 17 included studies reported treatment integrity results for the actions of the typical peer participants (Kern & Aldridge, 2006; Schmidt & Stichter, 2012). Table 2 includes details of the aspects of studies for which treatment integrity data were collected including whether it was collected for peer training and/or the peer’s actions. In their study, Schmidt and Stichter used a checklist with a rating scale (0–2) to collect data on whether the trained peer achieved the goal of the session. They collected data for the same days that data were collected from the learners with ASD, and the results indicated a high level of treatment integrity, ranging from 80% to 100%. As depicted in Table 2, general data may have been collected for the typical peer’s actions; however, these were not categorized as either treatment integrity or procedural fidelity data that could be delineated from the studies.
The typically developing peer is an active and essential component to the successful outcomes of PMII; he or she is the recipient of training on strategies to initiate and sustain social interactions with the learners with ASD (Neitzel, 2008). The lack of treatment integrity data collected for the peer’s actions reveals a significant gap in the current literature because measurement of the independent variable is critical to establishing experimental control and internal validity (Gast, 2010).
Conclusion
The results of the studies in this systematic review indicate the importance of implementing PMII whereby peers are taught the skills needed to successfully interact with the learners with ASD (e.g., Kasari et al., 2012; Katz & Girolametto, 2013; Lee et al., 2007). Overall, participants in the majority of the reviewed studies demonstrated an increase in social-communication skills, including initiations, responses, and continuations, when peer training occurred (e.g., Chung et al., 2007; Ganz et al., 2012; Jung et al., 2008; Lee et al., 2007; Loftin et al., 2008). Further, training typically developing peers creates the opportunity for learners with ASD to engage socially with their peers across a variety of activities and contexts, which is particularly important in inclusive classroom settings (Bass & Mulick, 2007; Sperry et al., 2010).
Implications for Practice
Given the comprehensive social-communication needs of young children with ASD, it is imperative that teachers and other related service professionals recognize the potential for an increase in social-communication skills as a result of the PMII. For example, Katz and Girolametto’s (2013) intervention resulted in improvements in the number and length of social interactions, including smiling and verbalizing to their peers. Other skills reported to be positively affected include prompted and unprompted responses to social requests (Jung et al., 2008). These are important skill acquisitions for young children with ASD; thus, it is important to consider embedding this instruction into everyday routines to promote generalization of these skills across contexts (Jung et al., 2008).
In addition, given the effectiveness of PMII as a social-communication skills intervention, it is important for practitioners to recognize the value and importance of inclusive contexts given that the presence of typically developing peers provides access and opportunities for implementing PMII as an intervention. Within inclusive settings, there are repeated and contextually appropriate opportunities for the intervention to occur. In sum, PMII has been effective in supporting the individual with ASD to increase their social-communication skills in both inclusive classroom settings and the school’s playground (Kasari et al., 2012; Katz & Girolametto, 2013; Kern & Aldridge, 2006). Overall, it is imperative that practitioners are knowledgeable about the implementation steps of peer-mediated interventions; therefore, ongoing dynamic professional development that includes classroom coaching and mentoring is warranted so that all educators are trained in methods for facilitating peer supports in natural contexts. The findings of this review suggest the importance of practitioners’ awareness and the inherent value of including typical peers with peers with ASD within a variety of contexts both in and out of the classroom (Kasari et al., 2012; Schmidt & Stichter, 2012).
Study Limitations
We focused our review on recent research of PMII as a way to understand the current growth of the practice as well as the recent applications of this work in classrooms. However, it may be possible that studies published prior to 2004 utilized strong research designs that are not accounted for in this current review. We used a systematic process for conducting the search of the literature, as developed by the Prisma group (Moher et al., 2009). Additionally, we used various combinations of Boolean search terms to maximize the articles identified in the search. It is important to note that despite these methods, current PMII research may not have been identified.
Future Directions for Evidence-Based Studies in PMII
A systematic review of these current PMII studies suggest future research directions in the following five areas: (a) increase implementation of PMII with young children who are in preschool, (b) use high-quality research designs including larger numbers of participants, (c) include generalization and maintenance measures of social-communication skills across settings, (d) include treatment integrity and independent variable measures, and (e) implement social validity measures. In this review, only three studies included participants under the age of 5 years old. It is possible that this empirical literature gap could be due to limitations of classroom-based interventions in inclusive preschool settings, or that interventions to address the social-communication skills of young children are occurring in settings where typically developing peers are not present. Regardless, future classroom-based intervention research must continue to include young, preschool-age children with ASD as well as related service professionals such as speech-language pathologists (Katz & Girolametto, 2013). Additional studies that include this collaborative effort to promote social-communication skills of young children in inclusive settings is needed to advance our understanding of the magnitude of positive change that can be documented in inclusive classrooms.
In addition to including young participants in future studies, there is a need to implement high-quality analytic designs with large numbers of participants. That is, future studies should use robust research designs, such as including a sufficient number of comparisons of control and treatment conditions, and a sufficient number of data points per condition to examine change and influences of change over time. For example, a multiple baseline study investigating the impact of an intervention across multiple participants should have at minimum, a baseline, intervention, and maintenance phase. Further, the NAC (2009) recommends greater than five data points per condition to meet the requirements for the greatest SMRS score of five. Additionally, in a review of social-communication skill interventions for children with ASD, Matson et al. (2007) called for group research designs to be used; however, there was only one RCT study identified in this review (Kasari et al., 2012). This may be due to the fact that it is often difficult to find classrooms and groups large enough to implement an RCT especially in the area of children with ASD in inclusive classrooms. Given that this research design allowed for an alternative intervention comparison, this particular study was able to demonstrate that the peer-mediated interventions were most effective.
There is an overwhelming need for future studies to include generalization and maintenance measures given that social-communication skills interventions are most successful when an individual can generalize the new learning to new individuals, activities, and settings (Bellini, Peters, Benner, & Hopf, 2007). However, to date, little of this work has been reported in the empirical literature especially for children in preschool (Bass & Mulick, 2007; Kaiser & Roberts, 2011). For example, PMII implemented in the preschool and school context could occur primarily in the classroom, and students could be supported to generalize the skills with the same peers in other contexts such as the cafeteria and playground. There is already evidence that this approach holds promise (e.g., Kasari et al., 2012). Additionally, in-home interventions could support the generalization of skills to the home context or the neighborhood playground with either the child’s siblings or peers from school through planned and targeted play interactions with peers.
To examine the issue of treatment integrity measures within PMII, researchers should collect treatment integrity data for the typical peer’s actions as well as the targeted child with ASD (Trottier et al., 2011). The need for peer-related treatment integrity data has been identified as a future direction for research (Chan et al., 2009; NAC, 2009); however, in this review, only one of the seven PMII studies conducted since 2009 have reported treatment integrity data for the peer (Schmidt & Stichter, 2012). This gap in the literature must be addressed to ensure that the peer’s actions, such as initiating interaction with the student with ASD, are occurring consistently in multiple contexts and thus the bidirectional influences of these interactions can be assessed when examining barriers, challenges, and successes in the peer–peer interactions. Furthermore, there is also a need for greater focus on reports of social validity data in PMII studies (Ganz et al., 2012; Owen-DeSchryver et al., 2008). These data could inform the positive developmental outcomes of the PMIIs, as well as the concomitant effects, perspectives, and experiences of the peers, parents, teachers, and the individuals with ASD who are also implicated in the intervention practices.
Footnotes
Acknowledgements
The authors would like to thank Chandi Parikh for her assistance with establishing reliability ratings of the research quality for the studies discussed in this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.