
Abstract
This study examined factors associated with 9-month outcomes of 78 preschoolers with autism spectrum disorder ([ASD]; 66 males, mean age = 44.8 [7.0] months) receiving preschool special education services. Use of recommended intervention practices was observed in each student’s primary educational setting: autism-only (n = 28), mixed-disability (n = 25), and general early education (n = 25). Recommended practice use across setting types and developmental changes were compared using generalized estimating equations. Autism-only settings had the highest implementation of classroom structure, classroom environment, and curriculum and instruction. General early education had greater implementation of practices to support social and peer relationships. Supporting social and peer relationships was the largest predictor of gains, controlling for setting type; the association was greater for children with lower initial receptive language or developmental skills. These findings highlight the importance of supporting and promoting peer engagement in students with ASD across preschool placement types.
This study examined the associations between characteristics of community-based preschool early intervention services and outcomes for children with autism spectrum disorder (ASD). Children with ASD who receive high-quality early intervention (EI) can make large gains in cognitive, communication, and adaptive behaviors skills, with positive long-term effects (Reichow et al., 2012; Weitlauf et al., 2014). Most studies demonstrating these gains were conducted in university-based research settings using expert clinicians and highly manualized interventions.
As Kasari and Smith (2013) note, few children served in public schools are represented in studies examining the “evidence base” because most studies are of small size and include homogeneous samples. In addition, these studies often exclude children who are more impaired, minimally verbal, non-English speaking, or who have multiple disabilities. While emerging research demonstrates that if expert support is offered, evidence-based interventions (EBIs) can be implemented in community settings (Shire & Kasari, 2014; Suhrheinrich et al., 2020; Vivanti et al., 2014), these studies provide little insight into outcomes associated with current community practices and usual care in authentic school settings.
Studying intervention as it is delivered in community settings can provide important insights into which practices may be most effective, given the resources available in these settings (Stahmer & Aarons, 2009). To date, few studies have measured both the type and the quality of intervention in community-based school settings and the associated outcomes. In addition, few studies have included diverse samples that represent the full range of backgrounds and functioning of children with ASD. The little research in this area suggests that EBIs for ASD rarely are found delivered to fidelity in the community (Stahmer et al., 2005; Wood et al., 2015) and that usual care is not associated with as large of gains as in expert-implemented interventions (Nahmias et al., 2019). Existing studies of outcomes in community settings are limited in that many were retrospective (Flanagan et al., 2012), lacked a comparison group, or relied on outcomes only from one program, type of intervention, or intervention setting (e.g., Eapen et al., 2013; Fernell et al., 2011; Magiati et al., 2007).
In addition to varying in the extent to which they use evidence-based practices, preschool EI settings vary considerably in the extent to which children with ASD interact with typically developing children. In the United States, the Individuals with Disabilities Education Improvement Act (2004) requires that students with disabilities, including autism, be educated in the least restrictive environment, stating that “to the maximum extent appropriate, children with disabilities . . . are educated with children who are nondisabled.” Most research to date has evaluated interventions implemented outside regular education classrooms that do not routinely offer such opportunities (National Research Council, 2001; Odom et al., 2010), and it has not compared inclusive with noninclusive settings. The few comparative studies are inconclusive (Boyd et al., 2014; Harris et al., 1990), although recent research is promising that EBIs (specifically Group-Early Start Denver Model) can be implemented in settings with peers without disabilities with similar outcomes to autism-specific settings (Vivanti et al., 2019).
To our knowledge, only one study has examined how community preschool setting characteristics are associated with child outcomes. Nahmias et al. (2014) found that children with ASD who received preschool special education services in inclusive placements had higher cognitive scores when they finished preschool than children who received preschool early intervention in more restrictive placements. This was particularly the case for children with baseline higher communication skills, lower social-emotional skills, and poorer adaptive behavior. The authors hypothesized that inclusive placements provide more opportunities to interact with typically developing peers, which, in turn, may be associated with better outcomes, but they lacked the data to test this hypothesis. This study also was hampered by its retrospective design, different measurement tools at baseline and follow-up, and limited characterization of both children and intervention.
Across intervention programs, children with ASD vary in their response to treatment, and predicting which children will respond to which intervention remains a challenge. In addition to the moderators of outcome reported by Nahmias and colleagues (2014), language abilities (Kasari et al., 2008), social communication skills (Kasari et al., 2008; Yoder & Stone, 2006a, 2006b), adaptive behavior (Eldevik et al., 2010; Flanagan et al., 2012; Remington et al., 2007), IQ (Eldevik et al., 2010; Magiati et al., 2007; Perry et al., 2011; Remington et al., 2007), object exploration (Carter et al., 2011; Yoder & Stone, 2006a, 2006b), age (Flanagan et al., 2012; Perry et al., 2011), and autism severity (Remington et al., 2007) have emerged as potential moderators of outcomes for young children with ASD. Their interaction with characteristics of preschool settings in predicting outcomes has not been examined prospectively.
We built on the study by Nahmias et al. (2014) and other research by following preschoolers with ASD as they received publicly funded preschool special education services. We carefully characterized children at baseline, measured characteristics of the intervention they received, and assessed outcomes at 9 months. This study takes advantage of the variation in authentic school-based intervention practices and provides insight into interventions characteristics most associated with positive outcomes and whether those outcomes differ by child characteristics. We attempted to replicate the findings from the Nahmias et al. (2014) paper and, given the more careful measurement, also explored other moderators, taking an agnostic approach. Findings from this study can provide a benchmark against which to measure future progress in community-based preschool interventions. If certain intervention characteristics are associated with better outcomes, it can lead to experimental studies of which strategies work best in authentic preschool settings.
Method
Participants
The sample consisted of children with ASD receiving preschool early intervention in a U.S. urban school district. Children were eligible for this study if they (a) were between 36 and 59 months of age, (b) had a documented diagnosis of ASD, and (c) received services through the county’s public preschool special education or behavioral health system. Exclusion criteria were (a) caregivers did not speak English or (b) either the caregiver or classroom staff for a given child did not provide informed consent to participate. The sample was recruited on a rolling basis through the preschool special education system from July 2014 to August 2016.
Procedure
The study was approved by the University of Pennsylvania Institutional Review Board. Students were assessed at two time points: “T1” at entry to the study and “T2” after 9 months of publicly funded preschool EI services. This time frame of 9 months was selected because it is the standard length of the academic year. Students were assigned to EI placements based on usual practices by service coordination teams, based on parent preference and provider availability, in accordance with Part B of Individuals with Disabilities Education Act (2004) and the state educational code (which both require that students with disabilities are educated in the least restrictive environment).
Measures
Mullen Scales of Early Learning (MSEL)
Our primary outcome measure was the MSEL (Mullen, 1995), a standardized, reliable, and valid measure of early cognitive development for children from birth to 68 months old. The Early Learning Composite (ELC) is based on four MSEL scales (visual reception [VR], fine motor [FM], expressive language [EL], and receptive language [RL]). The MSEL covers the full age range of our sample. Because more than half of the sample had T-scores below 20 on the RL and EL scales at baseline, developmental quotients (DQ) were calculated by dividing the age equivalent by the child’s chronological age in months and multiplying by 100 as done in similar situations (see Eapen et al., 2013; Kaale et al., 2012). For the ELC, the DQ was calculated by first averaging the age equivalences of the VR, FM, EL, and RL scales. The change on the MSEL ELC DQ between baseline and follow-up was used as the primary dependent variable. MSEL EL and RL scores were explored as predictors of change.
Educational Program Review
Our primary independent variables were derived from the Educational Program Review (EPR), a measure of classroom characteristics that was developed to characterize the quality of “business as usual” preschool settings in which children with autism receive early intervention services. It was adapted from the Professional Development in Autism Program Assessment (PDA, 2008) that was developed as part of a U.S. Department of Education Office of Special Education and Rehabilitative Services–funded center at the University of Washington for training personnel to provide evidence-based educational services to students. Adaptations of the PDA have been validated (Hume et al., 2011) and used in other studies of preschool intervention (Boyd et al., 2014; Suhrheinrich et al., 2020). The EPR consists of 50 items on seven subscales: Teaming, Classroom Structure, Classroom Environment, Curriculum and Instruction, Social/Peer Relationships, Management of Challenging Behaviors, and Building a Positive Instructional Climate. Items are rated on a 1 to 5 scale (1 = Minimal/no implementation, 3 = Partial Implementation, to 5= Full implementation) by a rater based on a 60-min direct observation, classroom staff interview, and review of the child’s Individualized Education Program. Sample items include “a daily schedule of activities is used by students and staff, individual schedules are utilized if necessary” (Classroom Structure); “a low student-teacher ratio is maintained to insure instructional fidelity and appropriate intensity of intervention” (Classroom Environment); and “staff plan daily opportunities for children with ASD to interact successfully with typically developing peers and use a range of evidence-based instructional strategies during these interactions” (Social/Peer Relationships). Postdoctoral fellows, graduate students, and bachelor’s level research assistants with experience in ASD interventions were trained to reliability by an expert coder. A subset EPRs was independently rated to assess ongoing interrater reliability. The Management of Challenging Behaviors scale was not included in analyses due to insufficient interrater reliability, and the Teaming scale was not included due to missing teacher interviews from four providers that impacted the ability for raters to score this scale. The remaining five scales demonstrated excellent interrater reliability, all above .75 (Fleiss, 1986). The intraclass correlations (ICC) for each scale were as follows: Classroom Structure = .81, Classroom Environment = .91, Curriculum and Instruction = .88, Social/Peer Relationships = .94, and Building a Positive Instructional Climate = .78. The EPR was conducted in the early education setting in which the student had spent the most time at approximately 4 and half months after study enrollment. Observations and provider interviews were scheduled based on the preferences and availability of providers and families.
Early education setting type
This also was used as an independent variable and was coded based on teacher report during the EPR as autism-only (i.e., class primarily composed of students with an educational classification of autism), mixed-disability (i.e., class composed of students with a variety of educational classifications), or regular early education environment (e.g., typical preschool, daycare, reverse mainstream classroom, inclusion classroom).
Community autism diagnosis
An autism diagnosis was confirmed using the Autism Diagnostic Observation Schedule–Second Edition (ADOS; Lord et al., 2012) or the Social Communication Questionnaire (SCQ; Rutter et al., 2003). The ADOS is a semi-structured play-based assessment considered to be the gold-standard observational measure for diagnosing ASD. It was administered by a graduate student or postdoctoral fellow in psychology trained to research reliability and supervised by a licensed clinical psychologist. Calibrated Severity Scores were used in analyses. The SCQ is a brief parent questionnaire that evaluates the presence of ASD based on questions from the Autism Diagnostic Interview–Revised (Lord et al., 1994). Raw scores were used as a measure of parent-reported ASD symptoms. In children under 5 years old, the SCQ has been found to have a sensitivity of .80 and a specificity of .60 to detect the presence of ASD versus nonspectrum when using a cut-off score of 11, and a sensitivity of .68 and a specificity of .74 when using a cut-off score of 15 (Corsello et al., 2007), so the cut-off score of 15 was also used to confirm a community ASD diagnosis.
Student adaptive functioning
This was measured using the Adaptive Behavior Assessment System–Second Edition (Harrison & Oakland, 2003), a parent-report questionnaire used to assess adaptive behavior in the home. Subscales include Communication, Social, and Daily Living Skills, which can be combined into a Global Adaptive Composite. Because our previous work suggests the potential role of adaptive behavior and social-emotional skills in moderating treatment effects (Nahmias et al., 2014), standard scores from the Social Composite and Global Adaptive Composite were explored as moderators.
Developmental Play Assessment (DPA)
The DPA was adapted from Lifter (2000) to measure children’s interest in playing with objects and toys. This measure was administered as described in Carter et al. (2011). Briefly, an assessor presented two standard sets of toys within the child’s reach for approximately 3.5 min each during a free-play session. Object interest (i.e., the number of toys with which children used differentiated play) at Time 1 was coded by raters trained to reliability. Interrater reliability was excellent (ICC = .93). Object interest was explored as a moderator due to its association with treatment gains in other studies (Carter et al., 2011; Yoder & Stone, 2006a, 2006b).
Classroom observation of on-task behavior
A validated measure was used to assess participants’ on-task behavior during instructional time via direct observations (Pisacreta et al., 2011). Observers were trained to 90% interrater reliability using scoring videos by a master coder before field-based observations. Ongoing interrater reliability was assessed in the field and was excellent (ICC = 0.99) (Fleiss, 1986). Participants were observed for 10 min during a typical classroom activity (e.g., academic instruction, circle time). Observers coded whether the student was on-task or off-task utilizing an interval-based coding system. The percentage of intervals the student was observed “on-task” was used in analyses.
Demographic data
These were collected from parents and classroom staff. Collections were done at Time 1 and Time 2 to use as covariates in analyses.
Analytic Strategy
All analyses were conducted using SPSS version 25. First, we conducted one-way analysis of variance (ANOVA) for continuous variables by site type. Bonferroni-corrected post hoc comparisons were utilized to explore differences by setting type on continuous variables. Chi-square tests were used to compare dichotomous variables by site type. Exact tests were used in analyses with dichotomous variables in which cell counts were below 5. Cohen’s d was used as an effect size metric. Cohen’s d can be interpreted as follows: 0.2 ≈ small, 0.5 ≈ medium, and 0.8 ≈ large (Cohen, 1988). Next, we used generalized estimating equations (GEE) with an independent correlation matrix and robust standard errors to assess change over time on the MSEL ELC across all participants, with teacher clusters at Level 2 to account for children nested within teachers. GEE was then used to examine the effects of child characteristics (e.g., baseline scores and demographic features) and setting characteristics (e.g., EPR scales and setting type) on changes in the MSEL ELC. We first examined unadjusted models to determine which putative moderators and covariates would be included in the final adjusted model. Variables with an unadjusted association with the outcome significant at p
Testing moderating effects
We tested for interactions between setting and EPR subscales and child characteristics that were included in the adjusted model (e.g., Time 1 MSEL RL, MSEL ELC, on-task behavior). Statistically significant interactions were then probed for regions of significance using the method described by Preacher et al. (2006). The region of significance defines the specific values of a moderator at which the regression of an outcome (i.e., MSEL ELC change) on a focal predictor (e.g., setting type and EPR scale) moves from nonsignificance to significance. If a region of significance contains no data, that region is considered uninterpretable.
Results
Sample Description
Students
As seen in the Participant Flow Diagram in Appendix A, 78 students completed the MSEL at T1 and T2, completed the EPR, and met ASD criteria on either the ADOS or SCQ, and therefore could be included in the analytic sample. Descriptive statistics for these students are presented in Table 1 and Appendix B. At the time of the EPR, 28 participants received services in an autism-only setting from 20 different providers, 25 in a mixed-disability setting from 17 different providers, and 25 in a regular early education environment setting from 25 different providers. Students were predominately male (84.6%) and most had a household income below US$40,000 (58.7%). The plurality of child participants were Black (43.6%), which is consistent with the ethnic background of students receiving preschool special education services in the school district. Ninety-seven percent met autism spectrum cut-off scores on the ADOS, with 3% meeting only on the SCQ. As seen in Table 1, some baseline participant characteristics varied by setting, including sex. Students in regular early education environments had statistically significantly higher receptive language, expressive language, developmental skills, adaptive behavior and social skills, and they had lower clinician-rated ASD symptoms than did students in the other two settings (all p-values < .05). Students in autism-only settings also were diagnosed at a younger age, on average, than children in the other two settings (both p-values < .05).
Characteristics of Student Participants in Community Preschool Study.
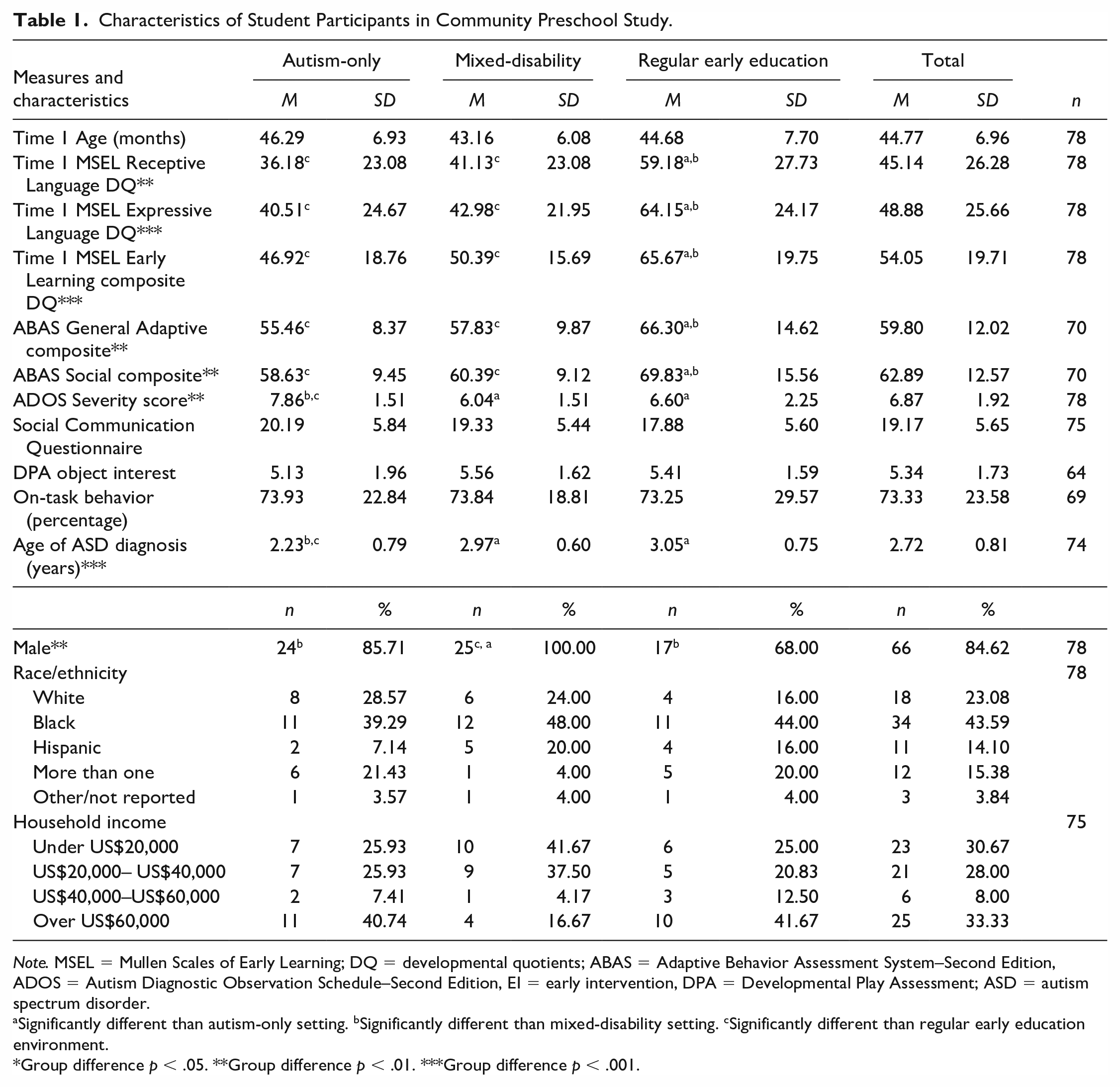
Note. MSEL = Mullen Scales of Early Learning; DQ = developmental quotients; ABAS = Adaptive Behavior Assessment System–Second Edition, ADOS = Autism Diagnostic Observation Schedule–Second Edition, EI = early intervention, DPA = Developmental Play Assessment; ASD = autism spectrum disorder.
Significantly different than autism-only setting. bSignificantly different than mixed-disability setting. cSignificantly different than regular early education environment.
Group difference p < .05. **Group difference p < .01. ***Group difference p < .001.
Classroom staff
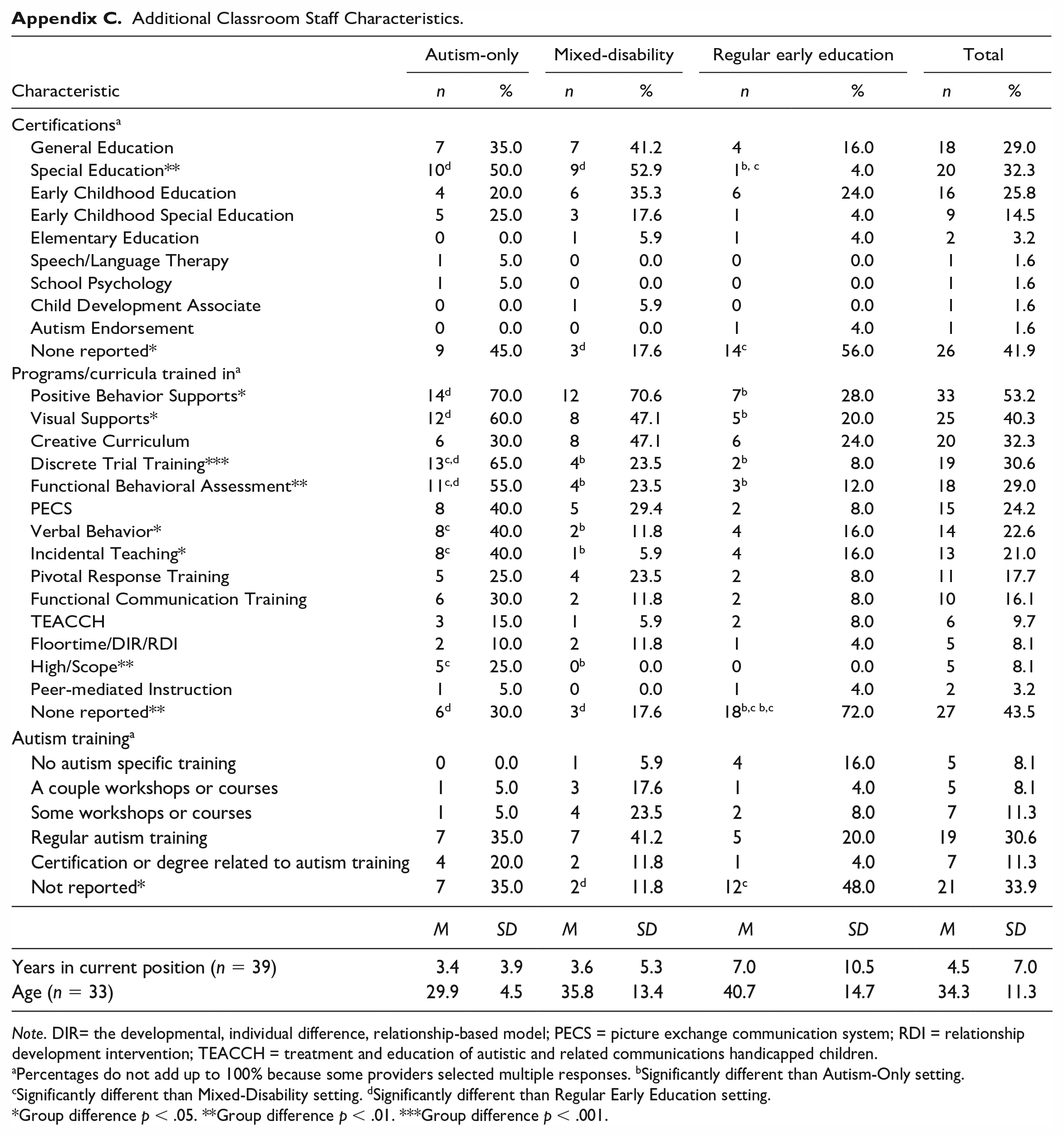
As seen in Table 2 and Appendix C, of the 62 participating classroom staff that completed the demographic questionnaire, providers were largely female (97%) and White (66%). Less than half reported receiving regular autism training; many reported receiving training in programs and curricula that vary in their evidence base. Most staff (66%) were special education preschool teachers.
Characteristics of Staff in Participating Preschool Classrooms.

Note: GenEd = General Education; SPED = Special Education; voc. = vocational.
Significantly different than autism-only setting. bSignificantly different than mixed-disability setting. cSignificantly different than regular early education setting.
Group difference p < .05. **Group difference p < .01. ***Group difference p < .001.
Use of Recommended Practices by Setting
As seen in Figure 1, the use of recommended practices based on the EPR varied by setting. Autism-only settings had significantly higher scores on classroom structure, classroom environment, and curriculum and instruction recommended practices than regular early education environments (all ps < .01, d = 1.7, 0.9, and 1.5, respectively). Mixed-disability settings had significantly higher scores on classroom structure (p < .001, d = 1.0) and curriculum and instruction (p < .001, d = 0.9) practices than regular early education environments, but lower classroom structure scores than autism-only settings (p = .006, d = −0.8). Regular early education environments settings had significantly higher implementation of recommended strategies to support social and peer relationships than the other two settings (all ps < .001, d = 1.6 for autism-only and 1.2 for mixed-disability).
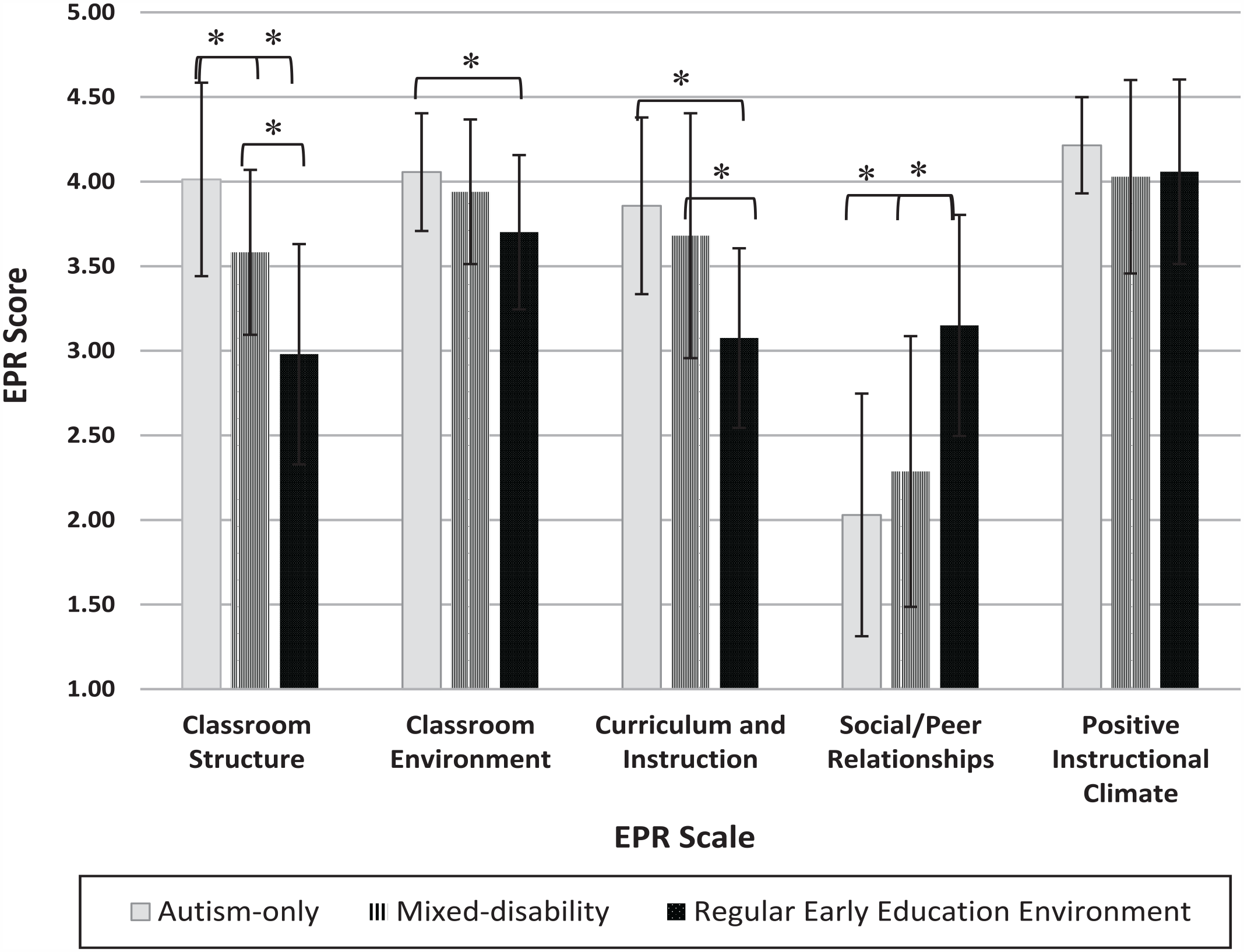
Use of recommended practices by setting type.
Developmental Outcomes
Full sample
The group means across all three groups improved in the Mullen ELC score between Time 1 (M = 54.05, SE = 2.44) and Time 2 (M = 56.41, SE = 2.72, B = 2.36, p = .03).
Unadjusted models
Table 3 presents the results of the GEE analyses predicting change in overall developmental ability, as measured by the MSEL ELC. In unadjusted analyses, only on-task behavior observed at baseline significantly predicted changes in Mullen ELC scores.
Unadjusted and Adjusted Generalized Estimating Equations on MSEL Early Learning Composite Change Score.
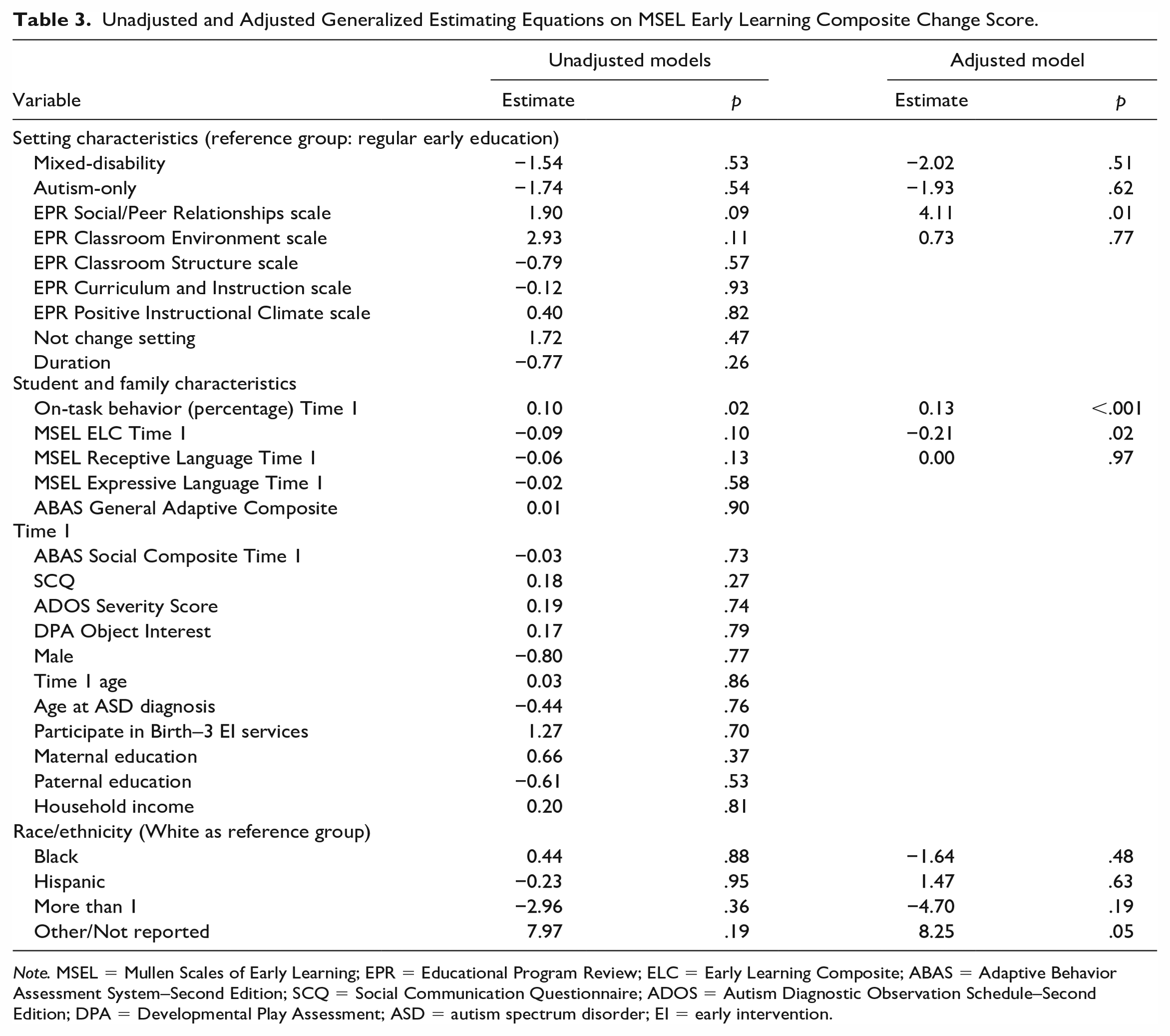
Note. MSEL = Mullen Scales of Early Learning; EPR = Educational Program Review; ELC = Early Learning Composite; ABAS = Adaptive Behavior Assessment System–Second Edition; SCQ = Social Communication Questionnaire; ADOS = Autism Diagnostic Observation Schedule–Second Edition; DPA = Developmental Play Assessment; ASD = autism spectrum disorder; EI = early intervention.
Adjusted models
Table 3 presents the results of the adjusted GEE analysis predicting change in MSEL ELC. In the adjusted analysis, only variables with a bivariate association statistically significant at p < .2 were included. Here, teacher use of recommended practices supporting social and peer relationships, child on-task behavior and MSEL ELC at Time 1 each statistically significantly predicted children’s developmental outcome at p < .05. Each point increase on the EPR Social/Peer Relationships scale was associated with a 4.11-point average increase in MSEL ELC change score. Each minute increase in observed on-task behavior was associated with a 1.30-point average increase in MSEL ELC change score. There were no statistically significant main effects for setting type.
Interactions
Of the initial putative moderators found in Nahmias et al. (2014), only receptive language on the MSEL met the criteria for inclusion in the adjusted model. Receptive language moderated the association between the implementation of recommended practices to support social and peer relationships (based on the EPR) and developmental changes (B = −0.12, SE = 0.03, p < .001; see Appendix D). Only the lower region of significance was interpretable (to the left of the vertical dotted line in Appendix D), meaning that for children with baseline MSEL RL developmental quotients below 58.43, children with lower baseline receptive language scores made greater gains on the MSEL ELC in settings with higher EPR Social/Peer Relationship Scale scores.
Baseline MSEL ELC also met criteria for inclusion in the adjusted model and was explored as a moderator. Baseline developmental scores moderated the association between the implementation of recommended practices to support social and peer relationships and developmental changes (B = −0.14, SE = 0.04, p < .001). Only the lower region of significance was interpretable (to the left of the vertical dotted line in Appendix D), meaning that for children with baseline MSEL ELC developmental quotients below 37.92, children with lower baseline receptive language scores made greater gains on the MSEL ELC in settings with higher EPR Social/Peer Relationship Scale scores.
On-task behavior did not moderate the association between the EPR Social/Peer Relationship Scale and MSEL ELC changes (p > .16). No tested variable moderated the association between setting type and developmental gains (p-values > .16).
Discussion
This study provides some of the most rigorous observational evidence of both expected outcomes across a variety of preschool early intervention programs in authentic school settings and the association of characteristics of these programs with developmental outcomes.
We found differences among autism-only, mixed-disability, and regular early education settings on many characteristics. Classroom staff in autism-only settings demonstrated greater implementation of recommended practices related to classroom structure, classroom environment, and curriculum and instruction than staff in regular early education environments, and greater classroom structure than in mixed-disability settings. Classroom staff in mixed-disability settings demonstrated greater implementation of recommended practices related to classroom structure and curriculum and instruction than staff in regular early education environments. Implementation of recommended practices for supporting social and peer relationships was highest in regular early education environments.
The characteristics of students in the three setting types also differed, although there was substantial overlap. Students receiving preschool special education services in regular early education environments had significantly higher receptive language, expressive language, developmental scores, adaptive behavior, and parent-reported social skills on average than students in placements primarily comprised of other students receiving special education services (i.e., autism-only and mixed-disability settings). Students in autism-only settings had higher clinician-observed autism severity and were diagnosed at a younger age than children in mixed-disability and regular early education environments. There also were more males in mixed-disability settings than in regular early education environments. These differences in child characteristics among the setting types were not observed in the Nahmias et al. (2014) study, in which there were minimal differences among children in different settings.
In this more rigorously designed prospective study, the results of our earlier work regarding the role of setting on outcome (Nahmias et al. 2014) were not replicated. However, in adjusted analysis, implementing recommended practices to support social and peer relationships was associated with positive outcome, even after controlling for other setting and child characteristics. Settings that served only children with ASD had higher implementation of almost all recommended practices, but only implementation of strategies to support social/peer relationships (more common in regular early educational environments) was significantly associated with overall developmental gains. While this finding is provocative, it is important to keep in mind that use of recommended classroom structure, curriculum and instruction, and classroom environment strategies may be associated with gains in domains not assessed in this study, such as challenging behaviors or academic readiness. A previous study (Boyd et al., 2014) found that children in community programs with at least partial implementation of recommended practices across domains, as measured by the EPR (average scores above 3 in each domain), demonstrated significant improvements in autism symptoms and severity, communication, and fine motor skills. Another possible explanation for the results of this study may be that community providers in this study need more training/support to appropriately individualize and tailor their use of recommended practices (Kasari & Smith, 2016). That is, positive EPR scores, averaged across students in the classroom, may not have captured important individual differences in how intervention was implemented.
While previous studies of interventions targeting social skills have demonstrated gains in those skills (National Autism Center, 2015; Odom et al., 2010; Steinbrenner et al., 2020), less research has explored the effect that targeting social and peer relationships has on developmental outcomes. One exception is a randomized controlled trial (RCT) of training in a school-based comprehensive treatment model (learning experiences and alternative program for preschoolers and their parents [LEAP]), which includes peer-mediated interventions as a core component. LEAP resulted in developmental gains (in addition to improved language, reduced autism symptom severity, improved social behavior and reduced problem behavior) compared with the control condition (Strain & Bovey, 2011). Supporting social and peer relationships may lead to improved attention when interacting with others, resulting in improved performance during developmental testing. Previous research with elementary school children without ASD (McClelland et al., 2000) found associations between learning-related social skills and later academic performance. In elementary school-age children with ASD (Pellecchia et al., 2016), increased social phobia symptoms were associated with decreased developmental gains. It may be that by targeting the core social deficit of ASD (American Psychiatric Association, 2013) leads to increased learning opportunities and generalization of gains by enabling children with ASD to take more advantage of interactions with peers that model age-appropriate behavior, social, play, and language skills.
Student characteristics also were associated with outcome. Specifically, increased on-task behavior predicted positive developmental changes. This suggests that children’s abilities to sustain attention and participate in the learning opportunities (or how well their early education placement facilitates this for them) are important predictors of developmental gains across setting types. Preschool students with ASD with poorer executive functioning may have worse intervention outcomes, which is consistent with some findings from children without ASD (Riggs et al., 2006). Our results are based on on-task behavior during typical classroom activities; therefore, it is unclear whether they are primarily driven by the student (e.g., the child’s executive functioning, including attention) or by the setting (e.g., teachers with better classroom management skills) characteristics. Further research is warranted to explore the relative contributions of these child and setting factors to impact developmental outcomes for preschoolers with ASD receiving community EI.
We found that greater implementation of recommended practices to support social and peer relationships was associated with greater developmental gains on average for children with ASD in our sample, and especially those lower baseline receptive language or developmental skills. This may suggest that a common educational approach of placing more severely impaired children with ASD in separate education settings away from typically developing peers (Strain, 2017) may result in a missed opportunity to maximize developmental gains. As Pellecchia and colleagues (2016) suggested, programs may need to adapt their educational approach to address social impairment and support social interactions, as these skills and opportunities may be necessary precursors to improving response to educational interventions.
Several study limitations warrant mentioning. First, students were not randomly assigned to placement, so unmeasured confounders of the association between placement and outcome cannot be ruled out (e.g., co-morbid concerns or disabilities, challenging behaviors, and broad attentional deficits). Challenges inherent with working with low-resource families (e.g., phone disconnection) and in authentic school settings (e.g., staff turnover) resulted in incomplete data collection. Our measurement of the intervention received was limited to a snapshot of the student’s programming, so we may not have fully captured the all of the intervention practices used with the student, consistency of strategy use, or intervention variability across the 9 months. Our primary outcome measure, the Early Learning Composite Developmental Quotient from the Mullen Scales of Early Learning, may not have been sensitive to more subtle or proximal developmental changes.
Despite these limitations, there are promising implications of this research. Using recommended practices to support social and peer relationships emerged as an important predictor of developmental gains for children with ASD receiving preschool special education services. Although the implementation of these strategies was greater in regular early education environments than settings that were primarily compromised of students receiving special education services, receiving preschool special education services in an inclusive classroom per se was not associated with more positive outcomes. This finding suggests that opportunities to interact with peers may be important for promoting gains, but inclusion alone is not sufficient. Consistent with the conclusions of Gutierrez et al. (2007), opportunities to interact must be paired with staff support to promote gains. In addition, while implementing strategies to support social and peer relationships was lower in autism-only and mixed-disability settings, it was not zero, suggesting opportunities to foster strategies to support social/peer engagement in those settings. Strategies by educational staff such as providing positive feedback to promote and maintain social interactions, not interfering with ongoing positive peer interactions, facilitating interactions by supporting and suggesting successful ways to interact with peers, encouraging peer partners or buddies, and considering peer relationships when assigning seats or groups can be implemented in a variety of preschool educational placement types.
Footnotes
Appendix
Additional Classroom Staff Characteristics.
| Characteristic | Autism-only | Mixed-disability | Regular early education | Total | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Certifications a | ||||||||
| General Education | 7 | 35.0 | 7 | 41.2 | 4 | 16.0 | 18 | 29.0 |
| Special Education** | 10 d | 50.0 | 9 d | 52.9 | 1b, c | 4.0 | 20 | 32.3 |
| Early Childhood Education | 4 | 20.0 | 6 | 35.3 | 6 | 24.0 | 16 | 25.8 |
| Early Childhood Special Education | 5 | 25.0 | 3 | 17.6 | 1 | 4.0 | 9 | 14.5 |
| Elementary Education | 0 | 0.0 | 1 | 5.9 | 1 | 4.0 | 2 | 3.2 |
| Speech/Language Therapy | 1 | 5.0 | 0 | 0.0 | 0 | 0.0 | 1 | 1.6 |
| School Psychology | 1 | 5.0 | 0 | 0.0 | 0 | 0.0 | 1 | 1.6 |
| Child Development Associate | 0 | 0.0 | 1 | 5.9 | 0 | 0.0 | 1 | 1.6 |
| Autism Endorsement | 0 | 0.0 | 0 | 0.0 | 1 | 4.0 | 1 | 1.6 |
| None reported* | 9 | 45.0 | 3 d | 17.6 | 14 c | 56.0 | 26 | 41.9 |
| Programs/curricula trained in a | ||||||||
| Positive Behavior Supports* | 14 d | 70.0 | 12 | 70.6 | 7 b | 28.0 | 33 | 53.2 |
| Visual Supports* | 12 d | 60.0 | 8 | 47.1 | 5 b | 20.0 | 25 | 40.3 |
| Creative Curriculum | 6 | 30.0 | 8 | 47.1 | 6 | 24.0 | 20 | 32.3 |
| Discrete Trial Training*** | 13c,d | 65.0 | 4 b | 23.5 | 2 b | 8.0 | 19 | 30.6 |
| Functional Behavioral Assessment** | 11c,d | 55.0 | 4 b | 23.5 | 3 b | 12.0 | 18 | 29.0 |
| PECS | 8 | 40.0 | 5 | 29.4 | 2 | 8.0 | 15 | 24.2 |
| Verbal Behavior* | 8 c | 40.0 | 2 b | 11.8 | 4 | 16.0 | 14 | 22.6 |
| Incidental Teaching* | 8 c | 40.0 | 1 b | 5.9 | 4 | 16.0 | 13 | 21.0 |
| Pivotal Response Training | 5 | 25.0 | 4 | 23.5 | 2 | 8.0 | 11 | 17.7 |
| Functional Communication Training | 6 | 30.0 | 2 | 11.8 | 2 | 8.0 | 10 | 16.1 |
| TEACCH | 3 | 15.0 | 1 | 5.9 | 2 | 8.0 | 6 | 9.7 |
| Floortime/DIR/RDI | 2 | 10.0 | 2 | 11.8 | 1 | 4.0 | 5 | 8.1 |
| High/Scope** | 5 c | 25.0 | 0 b | 0.0 | 0 | 0.0 | 5 | 8.1 |
| Peer-mediated Instruction | 1 | 5.0 | 0 | 0.0 | 1 | 4.0 | 2 | 3.2 |
| None reported** | 6 d | 30.0 | 3 d | 17.6 | 18b,c b,c | 72.0 | 27 | 43.5 |
| Autism training a | ||||||||
| No autism specific training | 0 | 0.0 | 1 | 5.9 | 4 | 16.0 | 5 | 8.1 |
| A couple workshops or courses | 1 | 5.0 | 3 | 17.6 | 1 | 4.0 | 5 | 8.1 |
| Some workshops or courses | 1 | 5.0 | 4 | 23.5 | 2 | 8.0 | 7 | 11.3 |
| Regular autism training | 7 | 35.0 | 7 | 41.2 | 5 | 20.0 | 19 | 30.6 |
| Certification or degree related to autism training | 4 | 20.0 | 2 | 11.8 | 1 | 4.0 | 7 | 11.3 |
| Not reported* | 7 | 35.0 | 2 d | 11.8 | 12 c | 48.0 | 21 | 33.9 |
| M | SD | M | SD | M | SD | M | SD | |
| Years in current position (n = 39) | 3.4 | 3.9 | 3.6 | 5.3 | 7.0 | 10.5 | 4.5 | 7.0 |
| Age (n = 33) | 29.9 | 4.5 | 35.8 | 13.4 | 40.7 | 14.7 | 34.3 | 11.3 |
Note. DIR= the developmental, individual difference, relationship-based model; PECS = picture exchange communication system; RDI = relationship development intervention; TEACCH = treatment and education of autistic and related communications handicapped children.
Percentages do not add up to 100% because some providers selected multiple responses. bSignificantly different than Autism-Only setting. cSignificantly different than Mixed-Disability setting. dSignificantly different than Regular Early Education setting.
Group difference p < .05. **Group difference p < .01. ***Group difference p < .001.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors thank our funders, Autism Speaks (Grant #8874; PI Mandell) and the McMorris Autism Foundation (PIs Nahmias & Yerys). The research reported here was also supported in part by the Institute of Education Sciences, U.S. Department of Education, through grant #R305B090015 to the University of Pennsylvania. The opinions expressed are those of the authors and do not represent the views of the Institute or the U.S. Department of Education.