
Abstract

Keywords
The topic of elderly homicide is important for two major reasons. First, nearly every publication on elderly homicide indicates that we are closing in on a very large increase in the elderly population. Second, while the number of elderly homicides is small, they have a number of characteristics that differentiate them from other age groups of victims.
The “Senior Tsunami”
While it is discussed in more detail in the articles in this issue, what is called the “senior tsunami” is a very large increase in the elderly population because those born between 1945 and 1965—the baby boomers—will have turned 65 in 2011 (Brookings Institute, 2010; Frey, 2007).
What contributes to the increase even more is that the World War II generation—born between 1936 and 1945—is currently part of the 65 and older group. According to Frey (2007, p. 1) just as the World War II generation, “plowed its way through the nation’s school systems, labor market, housing market, and stock market, it continually broke the mold, transforming both public and private institutions in its path,” we can expect similar massive, but as yet unknown, changes as the “baby boomers” enter and add to the above 65 group. Figure 1 shows the population percent increase for the next two decades as the result of the baby boomers and WW II generation entering the 65 and above population according to Frey.

Growth in U.S. total and senior populations by decade, 1970-2030.
Figure 1 shows a 15% increase in the above 65 population from 2000 to 2010 and an above 35% increase in the decade 2010 to 2020. The above 65 population finally begins to decline in the decade 2020 to 2030.
What this will mean in terms of elderly homicide is unclear. There will almost certainly be more incidents of elderly homicide, but it is unknown whether this will also mean an increase in rates and/or a change in the type of victimization (Krienert & Walsh, 2009; Weaver, Martin, & Petee, 2004).
Characteristics of Elderly Homicides
Before reviewing the studies in this issue, it is useful to briefly describe the current status of research on elderly homicide. As is generally known, the elderly have a low rate of homicide victimization. According to Bureau of Justice Statistics (http://www.bjs.gov/content/homicide/tables/vagetab.cfm), the homicide rate for victims 50 and above was 2.6 per 100,000 in 2005. The victimization rate for those above 50 was lower than for any other group except those under 14.
Roberts and Willits (2013) and other contributors to this issue have pointed to the importance of lifestyle/exposure and routine activities in explaining elderly homicide. This is certainly the case for elderly who live alone and thereby provide a target for victimization. Before summarizing the articles for this special issue, I describe first the homicide victimization of another group whose lifestyle and routine activities also contributes to their victimization.
Nursing Homes, Caregivers, and Elderly Homicides
Nursing homes have been plagued for decades with reports of physical abuse, neglect, and theft of personal property. These reports finally led to nursing home reforms contained in the Omnibus Budget Reconciliation Act of 1987. Despite this federal law, there has never been a systematic study of the prevalence of abuse in nursing homes (Hawes, 2003).
What makes the underreporting of homicides possible in nursing homes is the relationship between abuse and homicides. Abuse can and does occur and is concealed; on occasion a homicide is concealed. For example, Corey, Weakley-Jones, Nichols, and Theuer (1992) report that an 88-year-old nondiabetic White male was given a fatal insulin injection by an attending nurse. Ten days after death, an anonymous call to the coroner’s office led to an exhumation, autopsy, and a decision that the cause of death was a homicide. The nurse confessed, was found incompetent to stand trial, and her nursing license was revoked.
A complication is that autopsies are required by law only for certain causes of death such as homicide and suicide (Gruszecki, Edwards, Powers, & Davis, 2004). “Because of the serious, chronic illnesses suffered by these patients, attending physicians are often willing to sign death certificates without personally investigating the circumstances surrounding the patient’s demise” (Corey et al. 1992, p. 222).
A statistical analysis conducted by Nemetz, Leibson, and Naessens (1997, p. 179) of 139,063 deaths taken from the 1986 National Center for Health Statistics mortality tapes for four states (Kentucky, Maryland, Minnesota, and Washington) provides a statistical view of the problem.
The effect of death in a nursing home on the risk of autopsy varies as a function of age. For example, for 65-year-old men, the odds of autopsy for deaths outside the nursing home are 4.5 times those for deaths inside a nursing home. By contrast, for 85-year-old men, the odds of autopsy for deaths outside the nursing home are 10.4 times those for deaths inside a nursing home.
Caregivers
As Karch and Nunn (2011) and Abrams, Leon, Tardiff, Marzuk, and Sutherland (2007) note, there is relatively little research on caregivers. Much homicide research characterizes victim–offender relationships in general terms such as spouse or family member but does not discuss the role the perpetrator played in the victim’s life.
The most extensive of the few studies of caregivers in relation to homicide of the elderly was done by Karch and Nunn (2011) using data from the National Violent Death Reporting System. Of the 68 cases where the victim was 18 years or older, 29 victims were 50 to 79 years (42.6%) and 33 victims were 80 years or older (48.5%). Most of the victims were women (63.2%) and White (88.2%). In the age range of 50 to 79 about half were married while those age 80 or higher were most often widowed. Comparisons were made for types of caregivers and all ages. Comparisons were also made by type of homicide: by neglect (n = 17), by physical injury (n = 21), or homicide followed by suicide of the offender (n = 30), but not for specific age groups.
For those 80 years and above, husbands and sons were the most common caregiver offenders. For those in the 50 to 79 year group, husbands were the most frequent (20.7%), followed by wives (17.2%). The majority of the caregiver homicides occurred in a house or apartment. Firearms were used in about one third of the cases and “intentional neglect” was listed as the weapon in 24% of the cases.
Among the intentional neglect cases were two that were motivated by financial gain. The sons/caregivers in the following case needed a place to live and the mother’s support.
An 84-year-old White woman died while under the care of her two sons. The sons placed a bed in the basement, left her in urine soaked diapers and linens filthy with vomit, refused to treat her bedsores, discontinued her medication to treat her “naturally,” and provided her with cigarettes while connected to an oxygen machine. An unknown person reported them to authorities and when the fire department arrived, the sons indicated they thought she had had a stroke because she lost the use of her legs and had been deteriorating for 10 days. The sons told police they kept her in the basement because they needed a place to live and needed her financial support. They had installed video cameras in the basement, so they could watch her from monitors upstairs and didn’t have to go down to the basement. (Karch & Nunn, 2011, p.12)
Who You Calling Old?
As a way of introducing the articles for this issue, this title, borrowed from Lynn Addington’s (2013) article in this issue, captures both the defensiveness and reluctant acknowledgment of old age in our society. This is evident in the Pew Research Center (2009, p. 7) report when the interviewers asked,
Are You Old? Certainly not! Public opinion in the aggregate may decree that the average person becomes old at age 68, but you won’t get too far trying to convince people that age that the threshold applies to them. Among respondents ages 65-74, just 21% say they feel old. Even among those who are 75 and older, just 35% say they feel old.
In her innovative analysis of elderly homicide, Addington points out that the first step is to define what is meant by elderly. Defining elderly can be done in terms of common health, physical, or cognitive abilities, which is the best practice from the perspective of medical practitioners. In addition to ages, Table 1 below gives examples of physical and cognitive abilities. However, from a practical point of view, Addington is correct in pointing out that an easy-to-use measure is needed for research purposes.
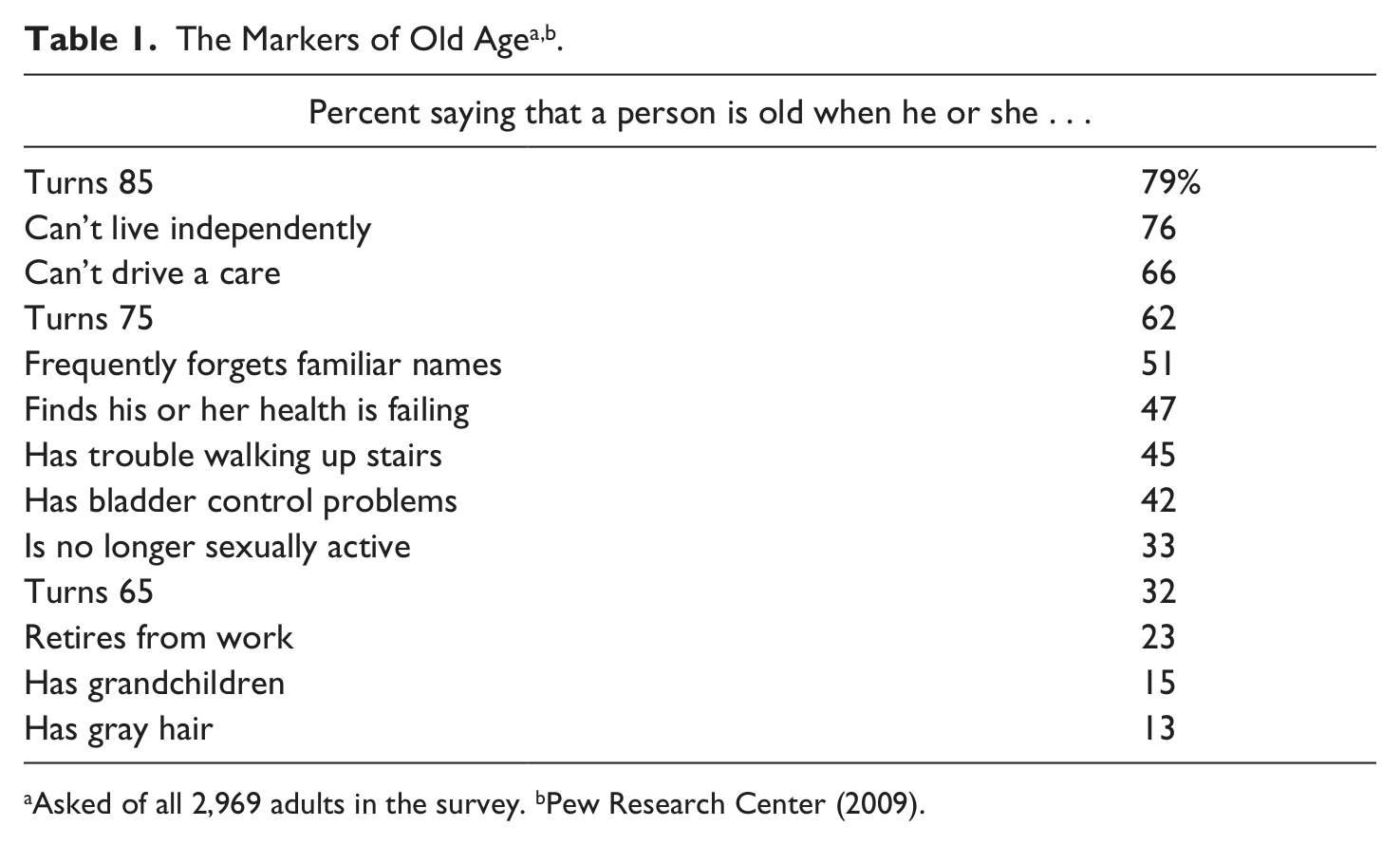
Asked of all 2,969 adults in the survey. bPew Research Center (2009).
Given that the elderly are living longer and healthier lives, it seems unlikely that a single number will suffice to delimit a heterogeneous population. Multiple categories of age would seem to address the problem of a chronological age definition recognizing differences in an elderly population.
In their articles in this issue, Lynn Addington (2013) and Carolyn Rebecca Block (2013) use a variation of the strategy suggested by the Census Bureau (1996). For the Census Bureau, 65 and above defines what is meant by “elderly.” But, in addition, it also uses the subcategories of 65 to 74 years as “young old,” 75 to 84 years as “aged,” and 85 years and above as the “oldest old.”
The use of multiple categories of the elderly opens up new research and policy possibilities. A major advantage is that the adoption of multiple categories by researchers greatly facilitates communication and replication. Current research comparing the elderly is limited by variation in how elderly is defined and unwittingly compares very heterogeneous samples. By using subcategories, it is also possible to draw similarities and differences across the subcategories. Also noteworthy is that variations in what is defined as elderly are not limited to researchers. The national survey by the Pew Research Center (2009) indicates that almost 3,000 respondents do not agree with the census categories, for example, but do indicate the importance of using subcategories of old.
Table 1 indicates that what constitutes old age has expanded significantly from the previous marker of 65; only 32% indicated that persons age 65 are old. A clear majority (79%) said that turning 85 was old and 62% said that turning 75 was old.
Table 1 also indicates that respondents are aware of markers used by gerontologists and medical professionals. For example, “can’t live independently” or “can’t drive a car” indicates a high degree of agreement on what would be considered the aged.
While we have noted that researchers have not settled on a classification of elderly, a wide disparity also exists among the respondents of the Pew survey: younger respondents see old age as beginning much younger than older respondents.
These generation gaps in perception also extend to the most basic question of all about old age: When does it begin? Survey respondents ages 18 to 29 believe that the average person becomes old at age 60. Middle-aged respondents put the threshold closer to 70, and respondents ages 65 and above say that the average person does not become old until turning 74. (Pew Research Center, 2009 pp. 2-3)
Does It Make a Difference?
Addington used 2007 and 2008 data from the National Incident Reporting System to study elderly homicide at different ages. She used the Census subclassifications mentioned earlier. Although the differences in Addington’s research were not always statistically significant, one of the major findings is that the greatest differences are seen between the “young-old” (65-74 years) and the “oldest old” (85 years plus) groups. Compared to the young-old group, in the oldest old group a higher percentage of victims are female, killed by family members, and with personal contact such as strangulation. A higher percentage of the young-old are killed with knives and in argument-related events compared to the oldest old.
Comparing elderly to nonelderly homicides, Addington found similarities between the youngest and oldest victims, including a high percentage of homicides by family members in argument-related circumstances for both groups.
Addington makes the salient point that a multiple-category classification of elderly is important to theoretical explanations. Several explanations of elderly homicide rely on routine activity/lifestyle theory. Multiple-category definitions suggest that routine activities and lifestyles vary substantially among the elderly and help explain differences in weapons and types of offenders. For example, the finding that the oldest old are killed by personal contact while younger old are killed by firearms suggests a “frailty” hypothesis that points to important variations in elderly lifestyle.
Victims and Offenders
Block’s (2013) research on elderly homicide draws on the Chicago Homicide Dataset (CHD), which is not only the most detailed collection of homicide data for a major city in the United States but is also the best known in the field. The CHD includes all homicides known to the Chicago police from 1965 through 2000; the CHD from 1965 through 1995 is archived in the National Archives of Criminal Justice Data.
From what we have discussed, it is clear that researchers and the public are becoming aware that there are differences among elderly age groups. In her study, Block follows the Chicago Department of Aging on defining elderly as beginning at age 60 and further breaks elderly into 5-year intervals for analysis: 60 to 64, 65 to 69, 70 to 74, 75 to 79, 80 to 84, and 85 and older. Unlike most of the other articles in this special issue, Block discusses characteristics of both victims and offenders.
Victims
Block explores variations in trends from 1965 through 2000. Rates for males and females above the age of 60 show a rapid increase from 1965 to the mid-1970s, then show a general decline to 2000. While the increase is particularly strong for males, it is also seen for females. While the numbers are too small to calculate annual rates, the decline from the mid-1970s seems to hold for all age groups and for both genders.
A few of the findings in this richly detailed study are that elderly victims are more likely to be non-Latino and less likely to Black or Latino, intimate partner homicides occur less frequently for elderly than younger age groups, and robbery and burglary increase with age.
The Chicago Data Set is very specific as to location of the homicide. The elderly are more likely to be killed in their own homes and the percent increases as the victims age. What is noteworthy is that elderly victims are more likely to be killed in the workplace compared to younger victims. For males, the percent killed in the workplace is highest in the age group 60to 64 while for women, the percent killed is highest at 60 to 64 years.
Offenders
Homicide offending is rare for the elderly compared to younger age groups. Only 1.7% of 27,561 offenders were age 60 or older. Women offenders followed a similar pattern. By the late 1990s, there is little difference between the number of older men and women committing homicide.
Elderly offenders were more likely to commit suicide than younger adults and the difference held when the victim was an intimate partner. For offenders who killed an intimate partner, ages 70 to 79 were most likely to commit suicide.
The preceding briefly summarizes a small number of findings reported by Block. As the author notes, the article was intended to fill substantial gaps in our knowledge of elderly homicide victims and offenders and she has succeeded in this goal.
Felony Homicides
Roberts and Willits’ (2013) study finds that elderly violence is characterized by a disproportionate number of felony homicides. Among the possible reasons are failing health, social isolation, and inactivity. Because of the latter, lifestyle/exposure and routine activities perspectives suggest a decrease in older adults’ frequency of conflict homicide. By the same token, the decrease in the possibilities of interaction may also reduce the amount of guardianship thereby increasing their attractiveness as targets.
While previous research has made extensive use of the lifestyle/exposure and routine activities theories, much of the research on elderly homicide has not included measures of lifestyle/exposure or routine activities. In their article in this issue, Roberts and Willits (2013) investigate the effects of a number of independent variables on felony homicides. The authors then apply the same model to argument-related homicides.
Using Supplementary Homicide Report data, the authors calculate the number of felony- and argument-related homicides for the populations above 65 for 195 cities with a population of 100,000 or more from 2000 to 2005. They construct indicators of impairment, inactivity, and social isolation for each city’s percentage of adults above 65 who were living alone, with a disability, and not working. They also include two opportunity variables: areas with high daytime nonoccupancy and high robbery rates. The authors hypothesized that overall robbery rates would be significantly related to other measures of felony-related homicides but not argument-related homicides.
Using negative binomial regression, Roberts and Willits found a positive significant relationship between older adults living alone and felony-related homicides, while the relationship for argument-related homicides was not significant. They also found that older adults with disabilities and robbery rates were significantly related to both felony and argument-related homicides.
The Robert and Willits research shows that older persons with disabilities and living alone may increase risks for felony-related homicides, but the additional difficulties of caring for disabled persons by younger caregivers could lead to more violent arguments.
It is also noteworthy that robbery rates were related to both felony- and argument-related homicides. The authors suggest that robbery may be an indicator of general violence in a city rather than something specific to elderly persons.
Elderly Homicide Offenders
The article by Feldmeyer and Steffensmeier (2013) is different from other articles in this issue in that it focuses on elderly homicide offenders. The research fills an important gap by evaluating patterns of elderly homicide over time and across race/ethnic populations. It also examines shares of elderly homicide arrests relative to younger groups across race/ethnicity and over time.
While understanding trends in homicide offending has present and future importance, another important outcome of studying elderly offenders is a better knowledge of the growing number of elderly in our prison population. At this point, it is unclear why there is an increase in elderly persons in prison. Finally, this article contributes to our understanding of the intersection of elderly homicide patterns with race/ethnicity as well as the proportionate shares of offending among age groups.
Data were drawn from the California Uniform Crime Reporting program for the 1985 to 2009 period. Data from this source are superior to that available from the national Uniform Crime Reporting program because there are codes for both ethnicity and race. California has clear and unambiguous classifications of Hispanic as well as White, Black, Asian, and Native Americans. In addition, California is large and has a very racially and ethnically diverse population.
While Feldmeyer and Steffensmeier’s research discusses trends in elderly homicide by race/ethnic categories, the most interesting findings involve whether there are race/ethnic differences in the elderly share of homicide offending relative to younger groups and whether the elderly share of homicide has changed over the 1985 to 2009 period. As expected, the measure of involvement share—Proportionate Age Involvement (PAI)—indicates that the elderly share of homicide is less than 5% for the total population and below 4% for Blacks and Hispanics when compared to younger populations.
In terms of temporal trends, the elderly share of homicide offenders increased from 3.8% to 4.8% from 1985 to 2009, but has remained generally stable. For the three largest racial groups, Black and Hispanic groups have retained generally stable PAIs over the time period. However, the White share of Proportionate Age Involvement has increased from about 6% in the 1980s to more than 10% after the 1990s. The increase occurred because of a decline in younger White homicide rates.
The final step in the research was to apply the Augmented Dickey-Fuller time series technique to determine changes in elderly homicide trends. This rigorous test indicated that the trends remained stable for elderly shares of homicide offending for the total population and all five race/ethnic groups, even with a significance level of p < .10.
Homicide-Suicide
Homicide-suicide is an event in which after committing a homicide the offender commits suicide. As Bridges (2013) notes in his article in this issue, the state of knowledge about homicide-suicides is lacking because there are no comprehensive national and state statistics given the lack of a uniform reporting system for these events. Undoubtedly, another major reason for data and research shortcomings is that homicide-suicides fall between the typical boundaries of two disciplines, public health and criminology, and have been studied independently (Liem, 2010; Riedel, 2008).
The article by Bridges examines homicide-suicides from 1968 to 1975 using Supplementary Homicide Reports (SHR), which ceased reporting homicide-suicides in 1975. The SHR underwent a major change in 1976 and most research using the SHR dates from that period. To determine the reliability of data prior to 1976, Bridges compares the number of homicide-suicides in the SHR to research done by others who collected data from a separate source, such as police departments. While comparisons are limited, the data do seem to agree with the alternative sources.
Homicide-suicide is a rare form of violence and for the elderly, it occurred most often among Whites and most of the victims were women. The second most common type of homicide-suicides involved a child killing parent. Almost all of the weapons were either handguns or other firearms. Among the elderly, homicide-suicides of spouses killing spouses were the predominant form of victim–offender relationship. While no patterns over time were analyzed, the findings for homicide-suicides from 1968 to 1975 are similar to homicide-suicide patterns in more recent research.
Conclusions
Many of the authors in this issue point out that research on elderly violence and homicide is lacking. It is clear that attention paid to abuse of the elderly is less than the attention paid to child abuse. As Shields, Hunsaker, and Hunsaker (2004, p. 125) noted, “Whereas the child abuse movement has prompted extensive investigation and received publicity over the past three decades, attention to elder abuse and neglect has been relatively deficient in medical and legal arenas.”
While research presented here helps to correct this imbalance, one of the major problems is the lack of consensus on what is meant by “elderly.” While subcategories have been suggested, more research will help to create agreement on the object of study.
It is important to consider that gender, race/ethnicity, and age are the three staples of most social science and criminological research and explanation. In the 20th century we have seen social changes, still occurring, in race/ethnicity and gender that have had a monumental affect on criminal law and the general quality of social life. To see the differences, women and minorities of today need only consider the quality of life of their parents and grandparents.
But what of age? Driven by demographics, what will be the major changes in the 21st century in the policies and treatment of the elderly? It seems clear now that the notion of elderly will come to have a more complicated meaning than being 65 and over. And what does that mean with respect to elderly homicide and violence? For example, will elderly homicide victims of nursing home and caregiver abuse be considered a more serious crime than robbery homicide? All that can be said with assurance at this time is that we do, indeed, live in interesting times.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.