
Abstract
The aim of this article was to compare the characteristics and outcome of homicide and non-homicide mentally disordered patients all of whom had been hospitalised. Seventy-four patients with a homicide conviction were compared with 521 convicted of a non-homicide offense. The former group were older, were more likely to be diagnosed with schizophrenia but less likely to have suffered from childhood adversity, and had less criminality. They also had fewer convictions during the follow-up. Little distinguished these two groups with both suffering from multiple disadvantages suggesting the need for ongoing care and support.
Background
Improved epidemiological sampling and more sophisticated systematic reviewing have helped clarify the relationship between the presence of a mental disorder and the likelihood of violent behavior. There is now a general acceptance, for instance, that certain mental disorders such as schizophrenia lead to a modest increase in violence (Fazel, Gulati, Linsell, Geddes, & Grann, 2009; Fazel, Langstrom, Hjern, Grann &, Lichtenstein, 2009; Mullen, 2009). This association is increased further in the case of substance misuse (Fazel & Grann, 2004; Steadman et al., 1998) and personality disorder (Yu, Geddes, & Fazel, 2012). The objective of this study was to focus on the relationship of mental disorders to homicide, arguably the most serious form of violence, by comparing the characteristics and course after discharge of a group of mentally disordered offenders convicted of homicide with a group of non-homicide mentally disordered offenders who had been admitted to the same hospital.
Mental Disorder and Homicide
Two recent literature reviews reported a positive association between schizophrenia, antisocial personality disorder and drug or alcohol abuse and homicide for men and especially for women (Richard-Devantoy, Olie, & Gourevitch, 2009; Woodward, Nursten, Williams, & Badger, 2000). Conversely, the risk of homicide was not elevated in patient populations with affective disorders, anxiety disorders, dysthymia, and mental retardation. Both reviews emphasized the need for more research because of the limited and overall poor quality of the available literature.
Various designs can be used to investigate the relationship between mental disorder and homicide. One of the most common of these is to take a sample of homicides and then retrospectively examine the presence of mental disorders within the sample and compare their rates with those in the general population (Fazel & Grann, 2004). This approach identified that a history of psychosis is common among persons convicted of homicide. For instance, Fazel, Gulati, et al. (2009) identified five studies that reported that the risk of homicide was 0.3% in persons with psychosis compared with 0.02% in the general population, resulting in an increased odds ratio of 19.5 (14.5-25.8). Bennett, Ogloff, Mullen, Wallace, and Short (2011) also found that 8.7% of 435 homicide offenders that they examined had a diagnosis of schizophrenia with a relative risk (RR) 13.11 (95% confidence interval [CI] = [14, 18.80]) more than in a general population community sample. Likewise, Eronen, Tiihonen, and Hakola (1996b) analyzed data on 93 homicide offenders with schizophrenia among 1,423 arrested during a 12-year period and found that schizophrenia increased the odds ratio 10 times compared with the general population. The odds ratio was 17 times higher in males with co-existing alcoholism.
Fazel, Buxrud, Ruchkin, and Grann (2010) used a case control design to compare the characteristics of schizophrenic patients who were convicted of a homicide within 6 months after being discharged from a hospital with other patients with psychosis discharged over the same period who did not commit any violent offenses. They found that on admission, the presence of poor self-care, substance misuse, and being hospitalized previously for a violent episode were important in predicting homicide, as were medication non-compliance and substance misuse post discharge.
As many of these studies used a lifetime diagnosis, it is unclear whether the mental disorder had a direct causal connection with the homicide. Shaw et al. (2006) attempted to tease out the nature of any potential association using data from a national inquiry into a consecutive series of homicide convictions in the United Kingdom between 1996 and 1999. They found that although 34% of the sample had a lifetime diagnosis of a mental disorder, only 10% had symptoms of mental illness at the time of the offense. They concluded that most perpetrators of homicide were neither acutely ill nor under mental health care at the time of the offense. Their findings echoed results from the Martone et al. (2013) study in the United States, which, in an unselected sample of defendants charged with homicide between 2001 and 2005, found that 58% had at least one Axis I or II diagnosis (47% with substance misuse) and 37% had prior psychiatric contact. Despite these high lifetime prevalence rates, only 8% of those with Axis I disorders were receiving treatment in the 3 months prior to the homicide. Their pattern of findings again suggests that there are limited opportunities for mental health providers to intervene to prevent homicide.
Further doubt about the causal relationship of mental disorder to homicide is provided by Large, Smith, Swinson, Shaw, and Nielssen (2008) who examined the official homicide statistics in England and Wales between 1946 and 2004 and found that both the total rate of homicide and the rate due to mental disorder rose steadily until the mid-1970s. However, the rate due to mental disorder declined thereafter whereas the rate of other homicides continued to rise. This pattern is replicated in data from New Zealand, which showed that the percentage of all homicides committed by mentally abnormal offenders fell from 19.5 in 1970 to 5 in 2000 (Simpson, McKenna, Moskowitz, Skipworth, & Barry-Walsh 2004). It is unclear from the U.K. data as to whether the decline in the mentally disordered homicides was due to improved service provision or to changes in legal tests in establishing a causal connection between the homicide and the mental disorder.
The Role of Substance Misuse
The presence of comorbid substance misuse is an important confounder to consider in the relationship between schizophrenia (together with other psychoses) and homicide. In their systematic review and meta-analysis of the relationship between schizophrenia and violence, Fazel, Langstrom, et al. (2009) found that most of the excess risk of violent crime (defined as any criminal conviction for homicide, assault, robbery, arson, any sexual offense, illegal threats, or intimidation) in those with schizophrenia was mediated by substance misuse comorbidity. Hence, the risk of violence in populations with schizophrenia without substance misuse was similar to the general population, whereas the risk of violence posed by those with schizophrenia and substance misuse was comparable with that in populations diagnosed with substance misuse without schizophrenia. Although the risk of homicide was also increased in those with substance misuse (odds ratio = 10.9, 95% CI = [3.4, 34.9]), the risk of homicide in those with psychosis was increased even more so (odds ratio = 19.5, 95% CI = [14.7, 25.8]) with or without substance abuse. Thus, substance misuse had a major mediating role between psychosis and violence but it exerted a lesser influence between psychosis and homicide (Fazel, Gulati, et al., 2009).
Bennett et al. (2011) found higher rates of substance misuse in homicide offenders with or without schizophrenia, than in the general population. They concluded that comorbid substance misuse could not explain the association between homicidal violence and schizophrenia.
Their results are partially contradicted by data from the U.K. National Confidential Inquiry between 1997 and 2006 (Swinson et al., 2011) that showed that the number of homicides committed by those with schizophrenia increased at an annual rate of 4%, although this trend did not continue for the final 2 years of the data collection (Large et al., 2008). The authors noted that an increase in the use of drugs and alcohol at a similar magnitude during that period led to the conclusion that the misuse of drugs was the likeliest explanation of the association between homicide and mental disorder.
In summary, there appears to be some evidence that schizophrenia and other psychoses are more strongly associated with homicide as compared with other crimes of violence and that although substance misuse plays a role, it is not the sole explanation.
Homicide Recidivism
Given that homicide is uncommon, it is not surprising that the literature provides little evidence about the association between its recurrence and the presence of a mental disorder. In a recent review of homicide, Liem (2012) made the point that although repeated homicide is rare, occurring in only 1% to 3% of those convicted for homicide, lesser misdemeanors such as parole violations and arrests for drug offenses are common among those released after a homicide conviction, with other violent offenses seen in 7% to 16% of offenders. In a 25-year follow-up of 92 paroled homicide offenders, Liem, Zahn, and Tichavsky (2014) found rates of 54%, 15%, and 3% for any recidivism, violent recidivism, and another homicide, respectively.
Several studies have examined the contribution of mental disorder to homicide recidivism. In their study of 13 homicide recidivists in Finland, Tiihonen and Hakola (1994) found that the offenders either suffered from severe alcoholism and personality disorder (11 cases) or from schizophrenia (2 cases). Similarly, Eronen, Hakola and Tiihonen, in a 13-year follow-up of 1,649 homicides committed in Finland, found 36 homicide recidivists of whom 67% suffered from alcoholism, 64% had a personality disorder (in most cases, combined with alcoholism), 11% had schizophrenia, and 6% had major depression. A previous homicide led to a tenfold increase in the likelihood of a repeat homicide compared with the general population; this increased to being 250 times more likely in the first year after being released from prison.
Golenkov, Large, Nielssen, and Tsymbalova (2011) assessed recidivism among a cohort of 133 Russian homicide offenders with schizophrenia and found that 11% of the offenders committed a repeat homicide within 4 to 19 years of the original offense. An acute exacerbation of schizophrenic symptoms, interrupted treatment, and reduced access to care were associated with the repeat offense. Unfortunately, no figures were reported on other forms of criminal recidivism in this study.
In a later systematic review and meta-analysis of homicide recidivism and schizophrenia, Golenkov, Nielssen, and Large (2014) compared the rates of homicide recidivism in the published and unpublished literature. They found that the rates of recidivism in three published studies (4.3%, 4.5%, and 10.7%) were substantially larger than in the 11 unpublished studies. They calculated that the pooled estimate from the latter was 2.3%, indicating a publication bias such that the published reports had recidivism rates 10 times greater than the unpublished studies. Thus, the rates of repeated homicide among those with mental disorder appear to be comparable with rates in those without mental disorder, although there are very few studies reporting on the former.
In the light of these uncertainties, this study has two specific aims. The first is to compare the characteristics at admission of mentally disordered homicide offenders (hereafter known as homicide offenders) with other mentally disordered non-homicide offenders (hereafter known as non-homicide offenders), both of whom had been admitted to the same secure psychiatric facility. Differences found between these two groups may be suggestive of features that characterize the homicide offender. The second aim is to determine the course of the two groups within the institution and to compare their outcomes after discharge.
To address the aims of the study, we used two different design strategies. For the first aim, a cross-sectional comparison was made between the homicide and non-homicide offenders. For the second aim (i.e., the follow-up study), a comparison was made of the outcome for the homicide offenders with a matched group drawn from the non-homicide offenders.
Method
It may be useful for those not familiar with how the United Kingdom manages mentally disordered offenders to describe briefly how its criminal justice system processes offenders. All detainees charged with murder are offered a psychiatric evaluation. When an offender is charged and incarcerated, he or she may be transferred to hospital for a psychiatric evaluation and/or treatment either while on remand or after sentence. Transfer of prisoners is either to a high secure or medium secure hospital depending on the perceived risk or the seriousness of the offense. Very few individuals claim to be not guilty by reason of insanity (NGRI), with the vast majority with a successful psychiatric plea being given manslaughter because of diminished responsibility.
The vast majority of patients transferred to a medium secure hospital in the United Kingdom suffer from mental illness (usually schizophrenia) as clinicians are reluctant to admit those with personality disorders, deeming the condition not to be treatable (Grounds, Melzer, Fryers, & Brugha, 2004). In this respect, the admitting policies of the unit described in this article are unusual as it had a dedicated personality disorder unit and hence admitted more personality disordered patients than is usually the case.
Homicide Case Sample
The homicide group comprised 73 individuals drawn from a consecutive series of the 595 first admitted patients (502 male, 93 female) to Arnold Lodge Medium Secure Hospital in Leicester, the United Kingdom, between 1983 and 2003. This group was made up of 49 patients with an index offense of homicide and another 24 patients with an index offense of attempted homicide. The overall outcome of this series has already been described in a series of papers (Clarke, Davies, Hollin, & Duggan, 2011; Clarke et al., 2013; Davies, Clarke, Hollin, & Duggan 2007) indicating that their course after discharge was poor with a greatly increased mortality together with rates of reconviction and readmission of 50% and 40%, respectively. Davies et al. (2007) give in detail the characteristics of these patients.
The 49 homicide patients (46 males, 3 females) and the 24 attempted homicide patients (23 males, 1 female) were combined because they had similar characteristics with the exception of age at admission. Patients with a homicide conviction (M age = 36.4 years, SD = 10.4) were significantly older on admission than the patients who had attempted homicide (M age = 28.8 years, SD = 9.4), t(71) = 3.0, p < .01. Length of stay, number of past convictions, Mental Health Act (MHA) classification, diagnosis, ethnicity, admission source, discharge location, and reconvictions were similar and this is consistent with the findings of both Maden, Swinton, and Gunn (1994) and Putkonen, Collander, Honkasalo, and Lönnqvist (2001). In addition, one patient with a previous conviction for homicide but with a non-homicide offense at the time of admission was also included in the homicide group.
Matched Control Sample
To analyze the second aim, the course of the homicide group’s stay in security and the outcome after discharge, a matched control sample of 74 patients was drawn from the 521 patients in the original admission cohort without a homicide index offense. Five variables were used in the matching process: gender, age at admission (18-25 years, 26-33 years, 34-41 years, 42 years and above), diagnosis (mental illness, personality disorder), a history of early criminal offending (first offense before or after 17 years of age), and the presence or absence of a “grave” index offense.
Data Sources
The patients’ admission characteristics were obtained from medical records held at Arnold Lodge. Data capture forms were designed to record admission variables (demographics, admission details, MHA classification, criminal history, family and childhood history, schooling and employment, mental health, substance misuse, discharge details) and outcomes for each year of follow-up for each case in the study (reconviction, psychiatric contact, accommodation, employment). The post-discharge outcome data were gathered up to the census date of 30th June 2003 (20 years after the first admission) with multiple sources used where possible to corroborate the accuracy of the data. Clinical and readmission data were obtained from records at Arnold Lodge, other psychiatric and general practice services, the Special Hospital Case Register, the Home Office Mental Health Unit, and the Office for National Statistics. The reconviction data were obtained from the Offenders Index and the Police National Computer. The electoral roll (UK-Info Disk Version 10) and the LexisNexis database of newspaper reports were also used.
Statistical Analysis
Comparisons were made between the homicide and non-homicide groups at pre-admission and admission (Aim 1) and between the homicide and control group at post-discharge follow-up (Aim 2). Among the pre-admission data, we examined childhood factors (i.e., evidence of childhood aggression or violence, a history of childhood sexual abuse, and a history of secure institutional care in childhood) and criminological factors (i.e., prior convictions for homicide, robbery, arson, assault involving actual bodily harm [ABH] or grievous bodily harm [GBH] and wounding, child sexual offense, and adult sexual offense) to assess parity between the homicide and non-homicide groups.
For Aim 2, the post-discharge follow-up data included mortality, rehospitalization, and reconviction. The reconviction figures for specific offenses were examined for the whole follow-up period. To replicate the original analysis reported by Davies et al. (2007), reconvictions for “grave” or “standard list” offenses were also examined within 2 years of discharge, 5 years of discharge, or at any time within the follow-up period using the Home Office standard method for reporting reconviction. This classifies convictions as either “grave” or “standard list” offenses (Home Office, 2002). Grave offenses are those for which the maximum sentence is life imprisonment, plus arson not endangering life, and include murder, attempted murder, robbery, rape, and arson. Standard list offenses are all other indictable offenses tried in either a Crown Court or a Magistrate’s Court. The Home Office also standardizes its reporting of reconviction, for example, at 2 years and 5 years following the date of release from prison.
Case-control comparisons were made using t tests or non-parametric Mann–Whiney U tests for continuous variables and chi-square tests or Fisher’s Exact Test as appropriate, for categorical variables.
Ethical Approval
Ethical approval for the study was granted by the Trent Multi-Centre Research Ethics Committee (MREC) and the project was conducted under Section 60 of the Health and Social Care Act 2001. Section 60 approval allowed for the collection of patient-identifiable National Health Service (NHS) data without patient consent, thereby enhancing the comprehensiveness of the data collection.
Results
Pre-Admission Characteristics
Aim 1
Although the majority of patients admitted overall were men (84.4%), the homicide group (94.6%) comprised significantly more men than the non-homicide group (82.9%), χ2(1) = 6.70, p < .05. Those in the homicide group showed less childhood disturbance with only one quarter (24.2%) being recorded as violent or aggressive in childhood, significantly fewer than in the non-homicide group (37.3%), χ2(1) = 4.07, p < .05. They were also less likely to have suffered sexual abuse or experienced institutional secure care as a child.
Those in the homicide group had less criminality: They were, for instance, significantly older when first convicted (M = 21.2 years, SD = 9.4) compared with the non-homicide group (M = 17.7 years, SD = 6.6), t(67) = 2.8, p < .01. More than one half of the non-homicide group (54.2%) had four or more previous convictions, significantly more than the homicide group (36.1%), χ2(1) = 8.32, p < .01. Significantly more patients in the non-homicide group (48.7%) compared with the homicide group (23.9%) had a previous conviction for ABH/GBH or wounding, χ2(1) = 15.41, p < .001, and for a sex offense (10.4% vs. 2.8%), χ2(1) = 4.24, p < .05 (see Table 1).
Characteristics of the Homicide and Non-Homicide Groups.
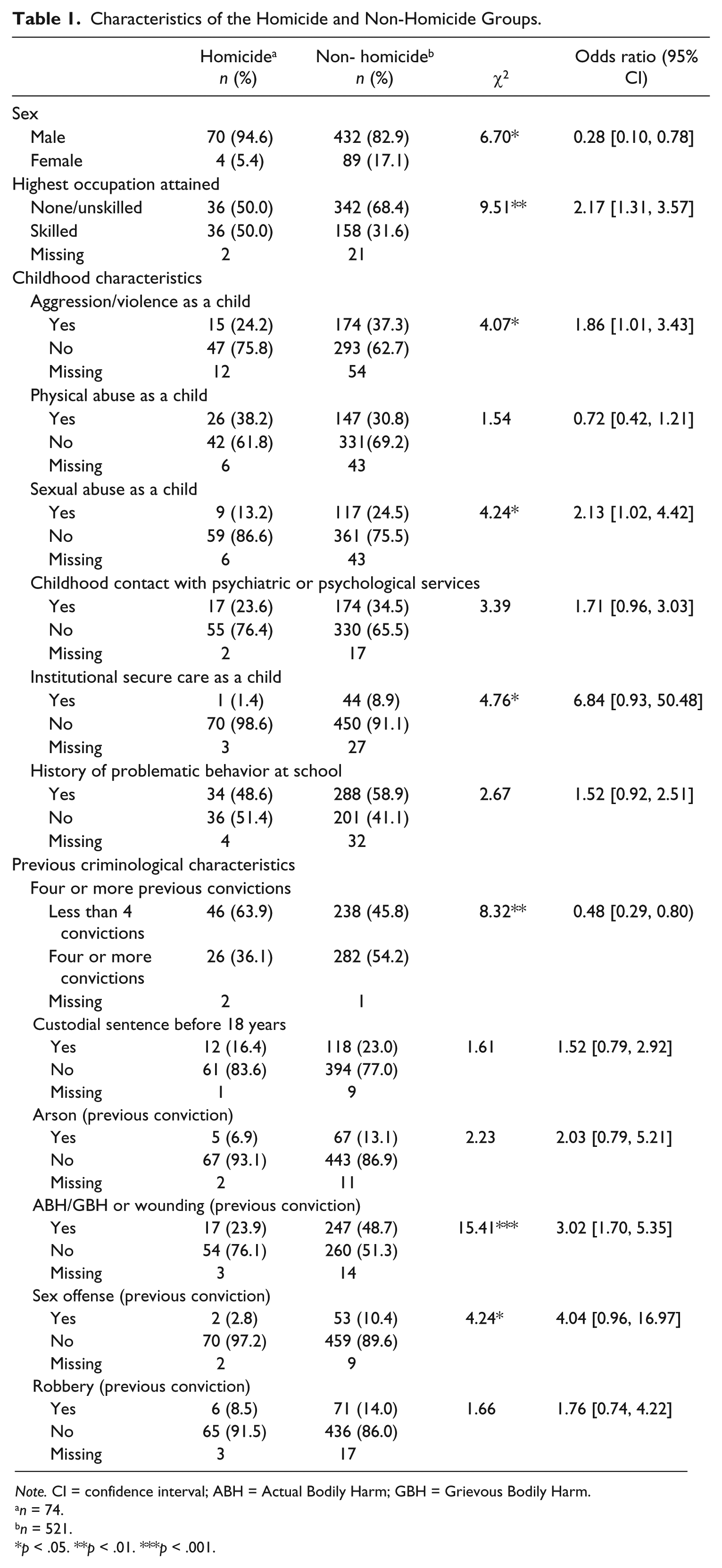
Note. CI = confidence interval; ABH = Actual Bodily Harm; GBH = Grievous Bodily Harm.
n = 74.
n = 521.
p < .05. **p < .01. ***p < .001.
Admission Characteristics
Aim 1
The admission characteristics of the two groups are presented in Table 2. Patients in the homicide group (M = 34.0 years, SD = 10.6) were significantly older when admitted compared with the non-homicide group (M = 29.3 years, SD = 8.8), t(88) = 3.7, p < .01. Overall, the majority of patients (67.2%) had a MHA classification of Mental Illness whereas approximately one quarter (26.6%) had a MHA classification of Psychopathic Disorder. Using these two classifications, significantly more people in the homicide group (84.3%) compared with the non-homicide group (69.9%) had a classification of Mental Illness, χ2(1) = 6.27, p < .05.
Admission Characteristics of the Homicide and Non-Homicide Groups.
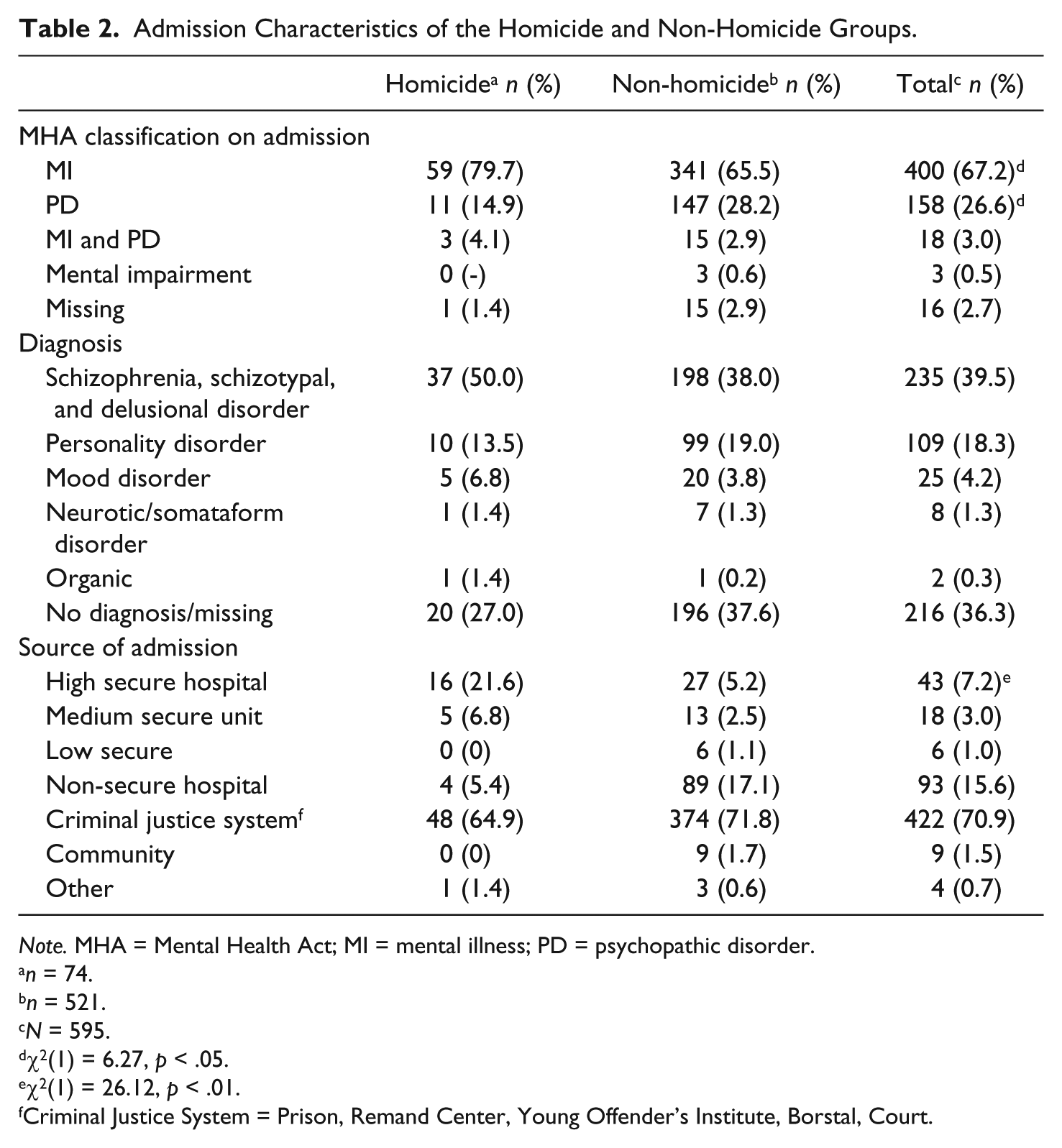
Note. MHA = Mental Health Act; MI = mental illness; PD = psychopathic disorder.
n = 74.
n = 521.
N = 595.
χ2(1) = 6.27, p < .05.
χ2(1) = 26.12, p < .01.
Criminal Justice System = Prison, Remand Center, Young Offender’s Institute, Borstal, Court.
The majority of patients in both the homicide (64.9%) and non-homicide groups (71.8%) were admitted from the criminal justice system. A significantly larger percentage of the homicide group (21.6) compared with the non-homicide group (5.2) were admitted from a High Secure Hospital, χ2(1) = 26.12, p < .01, indicating that they were admitted as part of a step-down in security as they progressed through their treatment.
Comparison of Homicide Group With a Matched Control Group
Aim 2
The index offenses for the matched control sample of 74 persons were as follows: 17 arson (23.0%), 5 rape (6.8%), 10 indecent assault (13.5%), 13 robbery (17.6%), 23 GBH/wounding (31.1%), 4 threats to kill (5.4%), and 2 possession of offensive weapon (2.7%). Patients in the homicide group (Mdn = 365.5 days) had a significantly longer first admission compared with patients in the non-homicide control group (Mdn = 240.5 days), U = 1,750, z = −2.03, p < .05.
A total of 62 (83.8%) of the homicide group and 72 (97.3%) of the non-homicide group were discharged before the census date in 2003. One patient in the control group died during hospitalization. There were no significant differences in the percentages of patients in the homicide and control groups discharged to the various services/locations: community (25.8%, 23.9%), prison (33.9%, 26.8%), high secure hospital (14.5%, 11.3%), other medium secure hospital (1.6%, 0%), low secure hospital (3.2%, 1.4%), and non-secure hospital (21.0%, 36.6%).
Mortality
The mean length of follow-up to the census date or death of the patient was 7.70 years (SD = 4.63) for the homicide group and 10.03 years (SD = 4.13) for the control group, t(131) = 3.07, p < .01. Four (5.4%) of the homicide group (3 from natural causes and 1 from suicide) and 10 (13.5%) from the control group (5 from natural causes, 4 from suicide, and 1 from misadventure; i.e., where there was insufficient evidence that the deceased intended to kill himself) died during the follow-up period. This pattern was not statistically significant.
Institutionalization
Of the 133 patients discharged from Arnold Lodge, 32 (24.1%) were known to have remained in an institution (prison or hospital) throughout the follow-up, significantly more patients from the homicide group (23, 37.1%) than the control group (9, 12.7%), χ2(1) = 10.80, p < .01. Seven patients from the homicide group and seven patients from the control group were recalled to hospital during the follow-up.
Reconviction
Table 3 gives the reconviction rates for specific offenses across the whole of the follow-up period. There were no significant differences in the number reconvicted from each group within 2 years. However, more of the control group, 24 patients (37.5%), were reconvicted of a standard list offense within 5 years, compared with 5 patients (12.2%) in the homicide group, χ2(1) = 8.01, p < .01; odds ratio 0.23 (95% CI = [0.08, 0.67]). A similar increase was found in standard list offenses over the entire follow-up period. The mean time from discharge to first conviction for the patients in the homicide group (M = 5.42 years, SD = 4.45) was not significantly different from the controls (M = 3.60 years, SD = 2.57), t(14) = 1.34, p > .05.
Reconviction Rates by Time and Offense Type for Homicide and Control Groups.

Note. CI = confidence interval.
Homicide n = 54, Non-homicide n = 68.
Homicide n = 41, Non-homicide n = 64.
Homicide n = 61, Non-homicide n = 70.
Homicide n = 61, Non-homicide n = 69.
Fisher’s Exact Test (all p values were non-significant).
p < .05. **p < .01. ***p < .001.
Further Violence or Aggression
Violence or aggression that did not lead to a conviction included physical assault, threats of physical assault, and damage to property was also examined. Some of these incidents matched criminal definitions but for various reasons did not lead to a conviction (e.g., not reported, not prosecuted) whereas others would not have matched criminal definitions but nevertheless were documented in case files. Two years after discharge, 14/57 patients (24.6%) from the homicide group and 14/69 (20.3%) from the control group were known to have been involved in a violent or aggressive incident that did not lead to a conviction. Five years after discharge, the number of patients known to have been involved in a violent or aggressive incident that did not lead to a conviction had increased to 18/50 patients (36.0%) from the homicide group and 26/67 (38.8%) from the control group. These differences between the homicide and control groups were not significant for violent or aggressive acts that did not lead to a conviction.
Homicide Convictions During the Follow-Up
A total of 5 patients were convicted of homicide from the 595 patients originally admitted, a recidivism rate of 0.8%. Three men were reconvicted of homicide (i.e., manslaughter) during the follow-up; one from the homicide sample (albeit the index offense at his initial admission was attempted murder) and two from the matched control group (both had an index offense of GBH at their initial admission). All three offenses took place in the community, and the victims included a parent, a prostitute, and a stranger. One patient from the matched control group was convicted of two counts of attempted murder in addition to his manslaughter conviction. All three patients had a MHA classification of Mental Illness and two had been admitted to Arnold Lodge from a high secure hospital and one from prison: One was at Arnold Lodge for less than 1 year and two were inpatients for more than 2 years. All three were discharged to hostels in the community. Two men from the non-homicide group but not in the matched control group were also convicted of manslaughter in the follow-up.
Readmission
Overall, the rate of readmission to hospital was high. Although reasons for readmission were not available for all cases, the most common were due to recurring psychiatric symptoms and the level of risk posed to themselves and others. Where readmission data were available for 57/62 and 61/71 for the homicide and control group, respectively, 66.7% of the former and 77.0% of the latter were readmitted to a psychiatric hospital during the follow-up. In all, 15 (24.2%) patients from the homicide group and 13 (18.3%) from the control group were readmitted to Arnold Lodge at least once: 2 patients from the homicide group and 3 patients from the control group were readmitted twice and 1 patient from each group was readmitted 3 times. Further readmission information for the full cohort is available in Clarke et al. (2013).
Discussion
Main Findings
Four main findings distinguished the two groups at admission: The homicide group was older, had less childhood disturbance and less criminality, and were more likely to have a diagnosis of schizophrenia. As homicide is the gravest of crimes, it may seem surprising that the mentally disordered homicide patient in this series was typically an older man who suffered from schizophrenia with less childhood disturbance and less evidence of criminality. That schizophrenia was the predominant disorder in the homicide was not unexpected given the association reported in another study (Fazel, Langstrom et al., 2009). In addition, Hodgins (2009) proposed that those with schizophrenia who engage in violence can be categorized into three groups depending on their antecedent pattern of violence. Her description of her Type 111 offenders with schizophrenia as “ . . . men in their late thirties with chronic schizophrenia and no history of antisocial or aggressive behaviour who kill, or try to kill, someone, often a care giver” (p. 57) is similar to many in this series. This suggests that the first presentation of schizophrenia to the criminal justice system can therefore be a homicidal act as mental health services and perhaps families of the patient have contained the disturbance up to that time so that it did not come to the attention of criminal justice agencies.
The lack of a difference between the homicide group and the non-homicide matched control for overall mortality and cause of death is striking as is the high number of suicides among the matched controls. This pattern reflects the very high standardized mortality rate in the series of patients, which was 6 times that expected in the general population (Davies et al., 2007) with a twelvefold increase in women (Sahota et al., 2010).
The greater number of non-grave offenses at both 5 years and overall for the non-homicide group is not surprising given their high frequency of offending pre-admission. Whether the lower frequency of reoffending among the homicide group over the longer term was due to the characteristics of the individual or the degree of extra surveillance and support they received after discharge is impossible to answer. We note, however, that the rate of violent and aggressive incidents that did not lead to a conviction was similar between the homicide and non-homicide groups (36% and 39%, respectively). One of the 74 patients (1.4%) in the homicide group went on to kill again and, despite their detention and treatment in a psychiatric hospital, and 5 patients from the entire series (0.8%) went on to commit a further homicide during the follow-up period. These figures are similar to those reported in the literature (Liem, 2012). Both groups had high levels of readmission to hospital with more than two thirds of both groups being readmitted to a psychiatric hospital during the follow-up period.
Comparison With Other Studies
This study, to our knowledge, is the first of its kind. Although Dirks-Linhorst and Kondrat (2012) found that NGRI pleas for murder and other crimes resulted in an increased duration of hospitalization post 1996 in Missouri, this is only of limited relevance for this investigation as only seven of the entire Arnold Lodge sample (1%) were detained on an insanity plea. Although all of the patients had a mental disorder for them to be detained in the hospital for treatment, the results nonetheless supported findings cited in the introduction (Fazel, Gulati, et al., 2009) that, of the major mental illnesses associated with homicide, it is schizophrenia and other psychoses that had the strongest association. This disparity in the diagnoses may, of course, be no more than the practice of admitting psychiatrists to such units in the United Kingdom where there has been a tradition to exclude offenders with personality disorders as they are deemed not to be treatable (Grounds et al., 2004).
Limitations
This study had a number of limitations that we acknowledge. First, the data come from a single unit that admitted patients over a 20-year period. Thus, the findings may not generalize to other facilities in other jurisdictions over different time periods. Second, the data clinicians recorded at the time of the patients’ admission were often poorly described, especially in the early phase of the unit’s history. In particular, substance misuse—an important comorbidity in those who engage in violent behavior—was poorly recorded because its importance was not recognized 30 years ago (Corbitt, Larkin, & Duggan, 1999). It is possible that an increase in several indices of severity (including that of substance misuse) in the admission characteristics of those admitted to this unit over time (Gibbon et al., 2012) is a function of improved clinical recording. A further limitation was that the diagnosis was clinically based rather than determined by standardized research criteria. Finally, the outcome is confounded by some patients in the homicide group (56.5%) spending longer both at Arnold Lodge and in other secure facilities thereafter, thereby reducing their time at risk, in turn, affecting the likelihood of their reoffending.
Conclusion
This study sought to distinguish mentally disordered offenders admitted to a medium secure hospital on the basis of the presence of a conviction for homicide. Despite identifying some differences, both at the time of their admission and during the follow-up, the groups had more in common than they had differences. Both had an increased rate of mortality together with high levels of recidivism and reconviction during the follow-up. This poor outcome is a reflection of the multiple disadvantages that both groups suffered from indicating the need for ongoing care and supervision prior to and subsequent to their admission.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.