
Abstract
Mindfulness is an ancient practice, derived from Buddhism and recently adapted for the treatment of depression and other psychological conditions. The mechanism of action is thought to involve the extinction of habitual or conditioned responses to internal cognitive and emotional content. In turn, this relies on mechanisms of attentional control and emotion regulation. The resulting state of consciousness is sometimes described as equanimity. This conceptual review paper explores the process of achieving equanimity within a homeostatic framework. The result is a model of moodfulness, which combines mindfulness with Homeostatically Protected Mood to provide a new theoretical view of recovery from symptoms of depression. This model presents a case for mindfulness restoration of mood homeostasis following homeostatic defeat.
Mindfulness and the Alleviation of Suffering
According to Buddhism, the practice of mindfulness is a form of mental training in pursuit of the elimination of suffering. While there are a number of traditions, each emphasizing different aspects of the original teachings, for most Buddhists, the practice is connected to an overarching philosophical goal of enlightenment, or nirvana, a state that is cultivated through continuous discipline and dedication (Bodhi, 2011; Olendzki, 2003).
For psychologists, the potential for mindfulness to reduce misery has been compelling, although in secular hands, the emphasis has shifted from spiritual transcendence to symptom relief. Over the past 40 years, the psychological literature has blossomed with research, interventions, and techniques for infusing psychological treatments with mindfulness. Overall, these report positive outcomes. Meta-analytic evidence demonstrates beneficial effects on diverse disorders, including anxiety, depression, addiction, and chronic pain (Bawa et al., 2015; Chiesa & Serretti, 2011; de Vibe et al., 2017; Li et al., 2017; Vøllestad et al., 2012). Mindfulness performs as well as evidence-based treatments for depression, such as cognitive-behavioral therapy (CBT) and anti-depressants, significantly outperforming other control conditions, with effect sizes ranging from Cohen’s ds of .23 to .55 (Goldberg et al., 2018). Confirmatory evidence from another large meta-analysis (Khoury et al., 2013) demonstrated mindfulness to be as effective as pharmacology and CBT for the treatment of depression, with effects up to Hedge’s g of .61, while mindfulness-based cognitive therapy (MBCT) is likewise as effective as pharmacological treatments (Kuyken et al., 2015, 2016).
These positive findings have also attracted some warnings regarding the quality of the studies, citing concerns with the clinical methodology and the generalizability of the results (Van Dam et al., 2018). However, accepting that the research indicates some therapeutic benefit of mindfulness, there is yet no consensus on the mechanisms by which mindfulness acts on psychological symptoms.
Our conceptual review proposes a novel model, which places the relationship between mindfulness and depression within the theory of subjective wellbeing (SWB) homeostasis (Cummins, 2016). While there are signs of an emerging interest in investigating the links between SWB and mindfulness (Jones, 2020), the two fields have not yet been integrated. Our review, then, is by nature preliminary, conceptual, and theoretical. While it draws on existing empirical evidence, specific empirical testing of the new model lies in the future.
We first provide an initial overview of the relationship between Buddhism and psychology. We then explore the mechanisms of mindfulness and its outcome state, equanimity. The theory of SWB homeostasis and its underlying key variable, Homeostatically Protected Mood (HPMood), is then described. Finally, depression, understood as SWB homeostasis defeat, is linked to HPMood and equanimity, forming the proposed model.
Buddhism and Psychology
In this century, there has been an exponential growth of scientific studies into mindfulness (Van Dam et al., 2018), but psychological interest in what Buddhism has to say about the mind and its relationship with suffering is much older. In introducing her translation of a key Buddhist text, the Dhamma-Sangani, which is a compendium of states or phenomena, C. A. F. Rhys Davids (1900) comments, “even a superficial inspection of the manual should yield great promise to anyone interested in the history of psychology” (p. xvi). Indeed, such interest was evidenced by such notable 20th-century psychological and psychoanalytical thinkers as William James, Carl Jung, and Eric Fromm, each of whom wrote extensively on Buddhism’s psychological components (e.g., Fromm et al., 1960; James, 1902; Jung, 1969). But the interaction between Buddhism and Western science has not been without controversy (Harrington & Dunne, 2015; Stanley, 2012; Van Dam et al., 2018). One obvious area of contrast lies in the notion of self.
Buddhist practitioners believe that all phenomena—including the “self”—are empty of inherent existence. They observe that an individual’s “self” exists neither in any of its constituent parts (body, mind, thoughts, perceptions, and consciousness) nor in the whole (Shonin et al., 2014). Instead, Buddhist philosophers propose a process known as “dependent origination,” in which interconnected phenomena co-arise with each other, with one thing leading to another as a result of this dependence, which in turn becomes our present-moment reality (Khong, 2003; Van Gordon et al., 2017). In other words, there is no inherent self, other than that constructed in the present (Stanley, 2012). As a result, Buddhist mindfulness focuses on recognizing that the construction of self—and the clinging or grasping of desire that such construction facilitates—is in fact the cause of suffering (Olendzki, 2003). Thus, Buddhists strive to end suffering by removing the “illusion of (self as) a continuous, fixed, separate entity” (Chodron, 2019, p. 113).
This Buddhist premise, sometimes described as “non-self” (Shonin et al., 2014), contrasts starkly with Western psychological therapy, which commonly proposes a strengthening of self, or self-concept, as a treatment for psychopathology. Such psychological therapy usually involves understanding the overarching narrative of the individual and their experiences (Kwee, 2013), as well as examining maladaptive thoughts and thought processes, particularly those involving self-blame or inadequacy to “correct . . . (these) erroneous judgements” (Beck, 1964, p. 571). This approach is clearly at odds with the Buddhist practice of non-judgmental acceptance of all thoughts (Bodhi, 2011).
It is notable that most psychological researchers and practitioners in this area avoid this larger philosophical conflict. Mindfulness interventions are often removed from their broader Buddhist context, commonly by incorporating mindfulness within behavioral and cognitive therapy. Examples include dialectical behavior therapy (DBT; Linehan, 1993), which emphasizes mindfulness as a way to gain acceptance over emotional experiences, and thus changing habitual behavioral responses to them, such as self-harm; MBCT (Segal et al., 2012), which emphasizes awareness of thinking patterns; and acceptance and commitment therapy (S. C. Hayes et al., 2006), which incorporates mindfulness as a way of achieving psychological flexibility.
Such separations of mindfulness, from its original ethical framework, have, according to Harrington and Dunne (2015), led to its use as a commodity. It has been used to promote such things as weight loss, better sex, and workplace productivity. This detachment from its origins has made mindfulness “hostage to values that are tangential or even anathema to the traditions from which the practice arose” (Harrington & Dunne, 2015, p. 621).
Curiously, however, the teachings attributed to the Buddha do not explicitly prescribe ethical action. The teachings direct an eightfold path, of which mindfulness is but one element, alongside such things as “right thought,” “right action,” and “right livelihood,” without ever defining “right.” Instead, Buddhist practitioners must obtain that knowledge by examining the contents of their own minds (Khong, 2003). Therefore, some scholars argue that Buddhism is a kind of “radical empiricism” (Segall, 2003, p. 92) where followers are urged not to take even the Buddha’s word as authority. In Buddha’s words, quoted by Segall (2003, p. 107): “ehipassika: come and see for yourself.”
Such reflective practice has also been described as a “science of experience in which the stream of consciousness itself, as it is presented to the attentive and carefully trained observer, is the field of investigation” (Olendzki, 2003, p. 14). This process of attending, in a trained way, to the present stream of consciousness, is actually one description of mindfulness. In this it shares, with most Western psychological approaches, a reliance on introspection, or an understanding of the subjective experience (Olendzki, 2003; Segall, 2003).
What Is Mindfulness?
In its secular application, the most common definition for mindfulness is “paying attention in a particular way: on purpose, in the present moment, and nonjudgmentally” (Kabat-Zinn, 1994, p. 4). However, the Pali word sati, which was first translated as mindfulness in the 19th century (T. W. Rhys Davids, 1881) is more accurately translated as recollection, or memory. Some interpret sati as a call to remember, or stay focused on, in your present moment (Gethin, 2011), while others expand the meaning, suggesting mindfulness is a kind of attention that allows efficient encoding and recollection of experiences (Vago & David, 2012; Wallace & Shapiro, 2006). Still others propose “lucid awareness” (Bodhi, 2011) or bare attention (Nyanaponika, 1962) as what the Buddha meant in his mindfulness teachings. In turn, bare attention is understood as noticing, “observing all phenomena—physical, mental and emotional—whatever is presently taking place in the mind” (Gunaratana, 2011, p. 135).
Some of these semantic differences stem from differences in practice. There are generally thought to be two broad schools—those emphasizing concentration, sometimes describes as samatha, and those emphasizing insight, experiential enquiry, or vipassana (Batchelor, 2011). Concentration practice develops focused attention, and involves directing and sustaining attention on a chosen object (such as the breath, or a candle); and training the mind to disengage from distracting stimuli (Lutz et al., 2008). Most novice practitioners are taught focused attention, and many teachers consider such practice as foundational training for later development of open and undirected practices that attend to whatever emerges in consciousness on a moment-to-moment basis (Bodhi, 2011). It is thought that these open monitoring practices (Lutz et al., 2008), or the ability to contemplate whatever phenomena arise, are advanced techniques that support the capacity for wisdom and discernment (Grossman & Van Dam, 2011).
Generally speaking, most mindfulness-based psychological interventions are manualized programs that progress through these practices, drawing primarily on focused attention techniques, but including some analytical practices such as non-judgmental observation of thoughts and feelings, and sometimes incorporating both of these into practices. An example is loving-kindness meditation, in which the focus is cultivating compassion for oneself and others (Harrington & Dunne, 2015; Lippelt et al., 2014).
The mindfulness practices that these psychological interventions draw on share a common intended outcome: freedom from suffering, or “the endless cycle of desire and aversion” (Gunaratana, 2011, p. 6) and the attainment of nirvana. Nirvana is literally translated as “extinction.” In Buddhism, it refers to the extinction of processes, such as craving, clinging, or grasping to thoughts or emotions that cause suffering (Buddhaghosa, ca. 412/2010).
How Does Mindfulness Work?
Cognitive processes
Researchers have yet to agree on the mechanisms by which mindfulness operates, and there are likely as many proposals and possibilities for mechanistic operations as there are varieties of mindfulness practices (Hölzel et al., 2011). One of the earliest, and most influential, theoretical models involves cognitive processes. This suggests that training in three components of mindful practice—intention, attention, and attitude—creates a shift in an individual’s perspective of themselves and their circumstances (Shapiro et al., 2006). The authors call this shift in perspective “re-perceiving.” They propose that intention and attitude combine to create self-regulation, such that the sustained observation of one’s inner experiences enables the ability to “stand back” and witness the drama of the personal narrative, rather than being immersed in it (Shapiro et al., 2006, p. 377). In this regard, mindfulness has been described as “non-judgemental observation of the ongoing stream of internal and external stimuli as they arise” (Baer, 2003, p. 125). In a similar vein, other authors describe re-perceiving as a decoupling of consciousness and mental content, thereby creating a “mental gap” between awareness and the objects of attention (Brown et al., 2007, p. 216).
These descriptions imply that the process of decoupling the contents of the mind from the self creates a sense of neutrality. However, many researchers propose that what flows from this change in perspective is not neutrality but “positive reappraisal,” or the ability to attribute positive meaning to stressful events (Garland, 2007; Garland et al., 2011). This positivity is attributed to viewing thoughts as temporary phenomena. Thus, re-perceiving, which has also been described as decentering (Bernstein et al., 2015, 2019), is thought to be a protective mechanism against the kind of negative thinking characteristic of chronic depression (Lutz et al., 2015; Segal et al., 2012).
In summary, it is commonly taught that the practice of non-interfering observations of previously distressing stimuli (negative thoughts) leads to desensitization and extinction of previously conditioned responses that yield the negative affect. Through such practice, habitual negative reactions are extinguished, while novel appraisals and positive responses are promoted (Farb et al., 2014; Hölzel et al., 2011; Roemer et al., 2015). Such extinguishment of negative emotional reactions, through mindfulness-based exposure, has been experimentally supported, and has also been found to survive later re-exposure (Uusberg et al., 2016). Some researchers, however, propose that monitoring present-moment experience can increase, rather than decrease, affective reactivity, unless it is coupled with affective strategies such as acceptance (Monitoring and Acceptance Theory; Lindsay & Creswell, 2017, 2019). These elements of affective adaptation suggest a second candidate for mindfulness’s effectiveness, which is emotion regulation.
Emotion regulation
Emotion regulation is “the processes by which individuals influence which emotions they have, when they have them and how they experience and express these emotions” (Gross, 1998, p. 275). The literature and models explaining these processes are extensive, but can be summarized as involving cognitive and behavioral strategies that are evoked to alter the conscious experience of emotions (Gross, 2015a). Such proposed cognitive strategies include attentional deployment and reappraisal. It is therefore logical that mindfulness, which involves both attentional deployment and reappraisal, is considered an emotion regulation strategy.
The ability of mindfulness to provide emotion regulation through attentional deployment has also been explored by Farb et al. (2014), who adapted Gross’s model. The proposition is that the attentional deployment extinguishes habitual responses to averse emotional experiences. This is achieved through the engagement and direction of effortful cognitive resources to attend to the experience, rather than to distract from it. Crucial to this process is the attentional focus on the sensory nature of the experience. This is thought to disrupt automatic appraisals, thereby allowing new perceptions to emerge. In an expansion on this notion, Garland et al. (2015) propose that mindfulness creates regulation through the cultivation of positive mental states. Thus, this increased attentional focus on the emotional experience, along with non-judgmental awareness, strengthens the prefrontal cognitive control mechanisms, which are then better able to downregulate affect generation from brain regions such as the amygdala (Tang et al., 2015).
Further understanding about the impact of mindfulness as influencing affective perceptions comes from research into mindfulness treatment for pain, which has established that mindfulness—in particular focused attention—alters the subjective experience of pain (Zeidan et al., 2011). More specifically, mindfulness acts not on the sensory experience of pain itself but on the perception of its unpleasantness. Thus, the pain experience is altered by a transformation of one’s subjective relationship to it (Grant & Zeidan, 2019).
Adding to this theme, a proposed Buddhist psychological model of mindfulness (Grabovac et al., 2011) also contributes understanding to emotion regulation. The proposed mechanism concerns the process by which a physical sensation, thought, or feeling occurs in the stream of consciousness. First, awareness of the event arises and evokes a feeling tone (pleasant, neutral, or unpleasant), leading to the habitual reaction of either “attachment” (usually to pleasant tones) or “aversion” (to unpleasant tones). This attachment or aversion creates mental proliferation or the continuous production of additional mental events following the original feeling tone. Such mental proliferation can be interrupted through sustained attention on an object such as the breath. The result is an awareness of the feeling tones, and their stimuli, without any follow-on mental proliferation.
Emotion regulation is also thought to come from interoceptive awareness, which is a core element of many mindfulness practices, and involves mindfully observing bodily sensations. The tradition stems from the first of four mindfulness establishments (body, feelings, mind, phenomena) taught by the Buddha (Bodhi, 2011). Interoceptive awareness developed from mindfulness has been proposed to elicit a kind of “bottom-up” embodied cognition that supports self-regulation (Khoury et al., 2017). It is perhaps not surprising, then, that mindfulness is also thought to engage physiological regulation.
Physiological regulation
In addition to cognitive and emotion regulation, there is emerging evidence that mindfulness acts on autonomic biological systems. Research in this area is nascent, and some authors have expressed caution about the quality of studies and variability of objective biomarker measurements (Christodoulou et al., 2020; Rådmark et al., 2019). Nonetheless, a recent meta-analysis of randomized control trials has found that mindfulness training reliably decreases physiological markers of stress, resulting in lower cortisol, heart rate, blood pressure, and cytokine levels (Pascoe et al., 2017). Such systems are largely governed by their own regulatory processes, particularly involving homeostatic control. It has been proposed that mindfulness supports such homeostatic control by decoupling the sensory and affective components of stressors (Vago & David, 2012). For example, mindfulness (partly, but not exclusively, through the relaxation response) increases cardiorespiratory synchronization and contributes to a shift toward parasympathetic activity and modulation of the autonomic nervous system. This in turn reduces physiological symptoms of anxiety, such as increased heart rate and irregular breathing, in turn reducing the experience of anxiety (Jerath et al., 2014). Thus, through generalized physiological quieting, mindfulness may aid in the maintenance of physiological homeostatic systems. Homeostasis is, therefore, an additional concept with which to explore mindfulness’s role in prevention of and recovery from distress.
What Is Homeostasis?
The term homeostasis was coined by Harvard physiologist Walter Cannon after he observed that blood sodium and glucose levels remained remarkably stable even when challenged by variations in the availability of their substrate. However, he also recognized that these variables exhibited variation within a stable range, hence, the Greek word homeo (meaning similar), and stasis (stable), describing processes that involve both variation and constancy (Cannon, 1929, 1932). In his masterwork, he writes of homeostasis, “the word does not imply something set and immobile, a stagnation. It means a condition—a condition which may vary, but which is relatively constant” (Cannon, 1932, p. 24).
Since Cannon, the understanding of biological systems has evolved considerably, and it is generally agreed that homeostatic systems are commonplace within biology (Chrousos, 2009; de Kloet et al., 2005). In any such system, the optimal resting level of the managed variable is described as its setpoint; a term borrowed from engineering and first applied to physiology within a few decades of Cannon’s writings (Hardy, 1953; Yates & Urquhart, 1962). As predicted by Cannon, homeostatically managed variables normally fluctuate within a limited range around their setpoint (setpoint range) in response to changing conditions impinging on each homeostatic system. Under normal conditions, the level of each managed variable is restrained to move within its setpoint range. While temporary transgressions outside that range are also adaptive and normal, prolonged transgressions are a signal of pathology.
While for most of its history, homeostasis has been considered in relation to physiological systems, the term is increasingly being applied to psychological processes. In a review for Nature, homeostasis was described as a “dynamic equilibrium” that governs all life forms and is managed by both physiological and behavioral responses (de Kloet et al., 2005, p. 463). In a similar vein, Damasio (2018) describes homeostasis as “the collection of coordinated processes required to execute life’s unthought and unwilled desire to persist and advance into the future through thick and thin” (p. 34). Further extending this general concept to social science, Montgomery (2018) proposes that some contemporary psychological disorders, such as post-traumatic stress disorder and depression, result from a lack of evolutionary adaptation to modern living. He describes psychological wellbeing as a homeostatic state, as a form or emotional homeostasis that reflects the underlying physiology.
This form of connection, between body and mind, is the concern of much contemporary research. One such exploration is the proposal that individual regulatory (homeostatic) systems interact with each other in dynamic, complex networks involving both physiological functioning and mood regulation. The resulting systemic resilience stems from a “dazzling web of mechanisms” that involve the mood, cognitive, and physical subsystems, with each of them contributing to the entire organism’s resilience (Scheffer et al., 2018, p. 11888).
Can Mindfulness Support Homeostasis?
The connection between mindfulness and physiological systems is receiving increasing research attention, as has been already indicated. For example, a recent meta-analysis of randomized control trials found evidence that mindfulness training decreases physiological markers of stress (Pascoe et al., 2017). However, the responsible mechanism remains uncertain. One proposal, stemming from a literature review, suggests that cardiorespiratory synchronization, elicited through mindfulness, creates decreases in intrinsic cellular excitability, and thus modulates the autonomic nervous system. They call this process “homeostatic modulation” (Jerath et al., 2014).
Such proposals assume that mindfulness influences physiological systems already known to be governed by homeostasis. It is a larger step in logic to consider whether mindfulness can activate a psychological homeostatic system designed to defend a crucial psychological variable.
The notion may not be so far-fetched. Other researchers have proposed mindfulness as a mechanism of supporting internal homeostasis (Vago & David, 2012), while mindfulness practitioners and teachers often use descriptions akin to homeostasis to describe the role mindfulness has on global, and in particular, emotion regulation. For example, Batchelor (2011) proposes that mindfulness involves four “great efforts”: cultivating conditions so that negative states do not arise, letting go of negative states that do arise, cultivating conditions so that positive states arise, and sustaining positive states once they have arisen. These four efforts can be loosely translated as a system managing its variable at its optimal point of functioning and taking corrective action to restore balance when required (Ramsay & Woods, 2014). In other words, homeostasis. The analogy has more than heuristic value and warrants further exploration and testing.
What Variable Might Mindfulness Be Defending?
Given that mindfulness extinguishes conditioned responses to thought and emotion, the residue in consciousness that follows this extinction is a possible candidate for a psychological variable protected by homeostasis.
Then, what must be considered, is the quality of the mental space created by mindfulness. If the normal emotional and cognitive dominance of consciousness is extinguished, what takes their place? Or, put in a Buddhist frame, what happens when the reflexive response of grasping and clinging to objects, emotions, and cognitions subsides? While the ultimate answer to that question is nirvana, or freedom from suffering, such enlightenment requires the deconstruction of a sense of inherent self, or non-duality (Grabovac et al., 2011; Kudesia & Nyima, 2015), and is the goal of Buddhist meditators. One of the precursors to this non-dual state is the ability to respond to stimuli with “calm and impersonal receptivity,” or equanimity (Kudesia & Nyima, 2015, p. 918). The mental state achieved from mindfulness practice is often described as equanimity (Olendzki, 2006), and it has been proposed that equanimity is the outcome state that mindfulness research should investigate (Desbordes et al., 2015; Hadash et al., 2016).
Equanimity as a Homeostatic Outcome of Mindfulness Practice
Most Buddhist texts translate equanimity, a core Buddhist virtue, to mean a “neutral feeling, a mental feeling which leans neither to gladness nor dejection” and is manifested as “peacefulness” (Bodhi, 2012, pp. 34, 116). More contemporary definitions include the simple term “emotional balance” (Williams & Kabat-Zinn, 2011, p. 3). Equanimity is not indifference. Rather, as described by Desbordes et al. (2015), it is an even and unbiased response to the objects of awareness and a form of emotion regulation. In essence, it is viewed as a “balanced reaction to the joys and miseries of mental experience that protects the mind from emotional agitation” (Weber, 2017, p. 152). Such descriptions also evoke the components of homeostasis, suggesting there is some merit in further testing the role of equanimity in psychological homeostasis.
In understanding the descriptions of equanimity and balance used by these authors, the use of “neutral” does not mean the absence of affect. To the contrary, renown Zen Buddhist master, Thich Nhat Hanh (2011) describes the neutral feelings that result from mindfulness as “very pleasant” and “wonderful.” He is not alone in that description. In a recent exploration of the three “feeling tones”—pleasant, unpleasant, and neutral, Batchelor (2018) points out that the so-called neutral tones are in fact experienced as “restful and peaceful and thus slightly pleasant” (p. 62). While the description of equanimity as a feeling, or mental state, is common (Pagis, 2015), equanimity is also described as a “quality of awareness” (Grabovac et al., 2011, p. 159) a skill to be cultivated (Lindsay & Creswell, 2019) and an effect of mindfulness practice that leads to increased well-being (Eberth et al., 2019).
In this regard, equanimity could be understood as a mental process that facilitates the cognitive and emotional regulation mechanisms described above. The Buddhist texts also refer to equanimity as one of four “immeasurables,” a desired attitude that is limitless in range (Bodhi, 2012), although that description has not deterred the emergence of a number of proposed equanimity scales in recent years (Juneau et al., 2020; Rogers et al., 2020; Weber & Lowe, 2018). These different descriptions and definitions are not surprising, given the centrality of equanimity to the Buddhist process of enlightenment. Indeed, equanimity is linked to advanced states of concentration, achieved after the earlier phases (which coincide with joy and bliss) are transcended. The Buddha’s words for this advanced state has been translated as “absolute purity of mindfulness” (Powers, 2007, p. 84).
Notwithstanding those conceptual differences, the representation of equanimity as a balanced mental attitude, or quality of mind, is perhaps the most common interpretation of equanimity in the psychological literature to date. It infers both a state that can be developed (with practice) as well as an effect of that practice (Juneau et al., 2020). Attributes of equanimity encompass the notion of non-reactivity to stimuli (Dreyfus, 2011). Bringing these thoughts together, the state of equanimity, produced through the development and practice of mindfulness, is a balanced mental state, devoid of reactivity to emotional content, and experienced as a slightly activated positive affect.
Is there an equivalent to this end-state in Western psychological thinking? A candidate variable is proposed by the theory of SWB homeostasis (Cummins, 1995, 2016) and is known as Homeostatically Protected Mood (HPMood). HPMood has been described as neurophysiological and comprising the simplest, constant, non-reflective, feeling underlying consciousness (Cummins, 2010). Crucially for our proposal, it is important to note that HPMood is not strongly attached to the views of the self except in an abstract way (Cummins, 2016): It is the residue in consciousness once self-referencing emotion and cognition are reduced from dominance in consciousness. It is also only experienced in the moment: One cannot access one’s levels of HPMood from the past. It therefore follows that mindfulness, which extinguishes the dominance of cognition and emotion in consciousness, and which grounds the subjective experience firmly in the present, would create the conditions by which this underlying mood is more directly accessed. Before exploring HPMood in more detail, the broader theory of SWB homeostasis will be described.
The Theory of SWB Homeostasis
The theory of SWB homeostasis was developed to account for a remarkably consistent finding in social science research: Most people are mostly happy with their lives, most of the time. Empirical evidence for the stability of SWB first emerged in 1934, when Hartmann found a .70 test–retest correlation for his subjective happiness scale administered to a sample of 195 college students, 4 weeks apart (Hartmann, 1934). Since then, SWB stability has been demonstrated in many longitudinal studies. For example, Palmore and Kivett (1977) found no change in life satisfaction in age–sex cohorts over a 4-year period; while a community sample of almost 5,000 adults studied over a 3-year period yielded similar results (Costa et al., 1987).
Stability has also been demonstrated in cross-sectional data. The first evidence came from an analysis of 16 unrelated studies of general population life satisfaction, involving samples totaling more than 100,000 people from Europe, North America, and Australia (Cummins, 1995). Cummins converted each study’s mean population score into the percentage of its scale’s maximum. He found the combined scores formed a mean of 75.02 percentage points (pp), with a standard deviation of just 2.74 pp. Subsequent data from the ongoing Australian Unity Wellbeing Index (AUWBI) project, which has involved 60,128 participants in 32 surveys over the past 16 years (Capic et al., 2018), provide further evidence of this population stability. During these 16 years, the average level of SWB of the Australian population varied less than 3 pp, with the mean of each survey lying between 72 and 76 pp (the mean for the 16 years is 75.4).
The consistency of these data provided the basis for a proposition that homeostasis might be the underlying cause of SWB stability. However, the essential element for such a proposal is the demonstration of setpoints, corresponding with the level of SWB that is being homeostatically defended. This evidence did not emerge for a further 20 years when Cummins et al. (2014) and then Capic et al. (2017) demonstrated setpoints for SWB, within general population samples, as normally distributed and positive, lying between 70 and 90 pp.
A conceptual challenge for the theory of SWB homeostasis is that SWB is not a single homogeneous variable. This was first demonstrated by Davern et al. (2007), with cross-sectional data from the AUWBI series (Capic et al., 2018). Davern et al. (2007) analyzed the relationship between SWB, cognition, and affect, with the choice of affects advised by the circumplex model, based on valanced and activated octants (Russell, 2003). They found that 90% of the variance in SWB was accounted for by three affects from the circumplex model—along with a measure of cognition based on multiple discrepancies theory (MDT; Michalos, 1985). Two later studies confirmed the role of affect, but found that MDT made little contribution after the variance attributed to affect had been accounted for (Blore et al., 2011; Tomyn & Cummins, 2011). Later research found the affective portion to be a specific blend of hedonic valence and arousal that sit between 353° and 18° on the circumplex, which is mildly pleasant and activated (Hartley-Clark, 2014, p. 183, Figure 20). Thus, it has most recently been deduced that the three affects—happy, content, and alert—are the closest approximation to the constant affective content of SWB (Cummins et al., 2018).
HPMood
This affective content of SWB was initially described as “core affect” (Davern et al., 2007, p. 435). This term followed Russell’s (2003) description of this basic affect, as a neurophysiological state consciously accessible as the simplest raw, non-reflective feelings present in all emotion and mood. Russell’s (2003) core affect was also described as “primitive, universal and simple . . . irreducible to anything else psychological” (p. 148). Finally, core affect was also proposed to be an underlying background affect, which Russell described as object-free or free-floating. This distinguished it from affect that is attributed to an object, which we could perhaps summarize as “I feel x because of y.”
The later naming of this variable as HPMood (Cummins, 2010) was considered necessary to make it clear that the variable is a mood, not an emotion. Emotions are transient, may be strong or weak, and represent a response to a percept or the affective component of a memory (Ekkekakis, 2013; Holland & Kensinger, 2010). Mood, on the contrary, is an unchanging, weak, diffuse, non-specific affective state (Ekkekakis, 2013). HPMood is abstract and refers to the most basic general feelings about the self (Cummins, 2016). Thus, it is proposed HPMood comprises the combined affects, “happy, content and alert” as the simplest, unchanging, non-reflective, feeling. HPMood is hard-wired for each individual and represents the tonic state of affect that provides a source of non-specific, activation energy, or motivation for behavior (Cummins, 2010).
Crucial to this understanding is HPMood is an affective state not attached to a situation or event (Cummins, 2016). However, this state can co-exist with other states of attention, such as mindfulness, or even absorption in a cognitive task, as in these instances, the attention is focused on the object, not the affect. The level of HPMood reflects the individual’s SWB setpoint (Capic et al., 2017). Thus, provided there is no contamination in consciousness obscuring access to HPMood, when someone is asked to subjectively rate their well-being, they will draw upon this mildly pleasant, free-floating affective state to influence their answer (Cummins et al., 2018).
Because, in its purest form, HPMood is devoid of both emotion and cognition, by its nature, it is also devoid of the broader narrative self-reference, which is generated by the development of a personal story to explain emotional responses to stimuli (Farb et al., 2007). The experience of this setpoint, without the influence of concurrent emotion, is the conscious experience of a mildly positive and activated mood, or a sense of what we call moodfulness. True to its nature, moodfulness is usually encountered as a mild background context to momentary experience. The purpose of SWB homeostasis, then, is to protect our sense of moodfulness. However, being moodful does not mean that the only affect in consciousness is HPMood. Normally, an individual’s moment-to-moment conscious access to this underlying, affective state will be obscured by the coincident presence of emotion.
Measuring HPMood
HPMood normally co-exists with emotion in consciousness. However, as emotions are normally stronger than moods, responses to momentary levels of SWB tend to reflect the level of emotion in consciousness, rather than the underlying mood. Thus, the changing levels of SWB reflect the influence of emotion. The influence of HPMood is also contained within each SWB response, even though it is normally invisible within cross-sectional data. However, the presence of HPMood can be demonstrated by using longitudinal data.
With such data, contamination can be statistically removed through covariance, as demonstrated by Cummins et al. (2014) and confirmed by Capic et al. (2017). The procedure examines the within-person standard deviation of SWB scores over time. The logic, then, is that the emotional content is responsible for the variation in longitudinal SWB data, while the HPMood component remains constant. Thus, at the level of each individual respondent, using an iterative process, SWB values lying beyond two within-person standard deviations are considered outliers caused by emotion and progressively eliminated. This procedure is repeated until no outliers are detected. Then, the mean SWB of the remaining scores is considered to approximate the level of HPMood for that person. A full description of the process is provided in the two above publications.
Independent confirmation of the differential role of SWB and emotions comes from a meta-analysis. Houben et al. (2015) report an inverse association between wellbeing and the degree of change in emotion over time. They analyzed change over time as the amount of variability, instability, and inertia in the psychological wellbeing scores, and found effect sizes (measured as backward-transformed correlations) of between .15 and .20 for the change indicators. As the authors point out (p. 922), this pattern is consistent with psychological wellness being characterized by homeostatic control. Put another way, psychological dysfunction, in this context can be interpreted as emotional fluctuations in reporting SWB and, when extreme, indicate homeostatic defeat.
These results are echoed in other research which specifically investigates the relationship between depression and resilience using ecological momentary assessments and the mathematical construct of “critical slowing down” (CSD), which suggests that the time lag between perturbation and recovery is indicative of systemic resilience—the longer it takes for a perturbation to be regulated, the lower the resilience (van de Leemput et al., 2014; Wichers et al., 2016). These studies, which measure CSD through auto-correlations and variance between elements of the system, conclude that emotion variability is an indicator of low resilience and thus an early warning of depression.
Homeostatic Resilience
The homeostatic system that protects HPMood is proposed to operate using the same broad principles as within physiology, in which effector responses counteract perturbations in the managed variable, here SWB. These principles are extensively described elsewhere (Cummins, 2016, 2017), and will be summarized here, with an emphasis on those processes that overlap with current understanding of mindfulness mechanisms.
When SWB homeostasis is threatened, defensive cognitive strategies such as self-esteem, perceived control, and optimism (Cummins & Nistico, 2002) are part of the immediate automatic response. Each of these are “positive buffers” that are in “intimate, conscious interaction with momentary experience” (Cummins & Wooden, 2014, p. 227) and are strongly perfused with HPMood (Lai & Cummins, 2013). When these resources are activated, there is a change in perspective of the challenging event and the meaning it has for the self. Thus, these could be further investigated to determine whether they echo the previously described cognitive mechanisms involved in mindfulness practice, in particular, reappraisal and decentering, which separate the notion of “self” from negative stimuli (Shapiro, 2009). From the perspective of homeostasis theory, these cognitive mechanisms protect the inherent positivity of HPMood. From the perspective of mindfulness practice, these processes are also described in homeostatic terms, with the suggestion that they lead to self-regulation (Shapiro et al., 2006; Tang et al., 2015). Although these processes are largely conscious, and in the case of mindfulness practices deliberately so, they also involve the underlying long-term automatic processes of habituation and adaptation.
Habituation and Adaptation
Habituation is the process by which a system decreases its response to a specific stimulus after repeated exposure (Rankin et al., 2009). It is a function of primitive learning that has been described as a “fundamental form of behavioural plasticity” (Thompson, 2009, p. 3). In the context of SWB, it is the mechanism by which an individual learns to tolerate mild-to-moderate persistent stressors, such that the event that once caused significant distress (e.g., a diagnosis of a chronic disease) over time loses its power to dominant consciousness, and so SWB.
Habituation is also the underlying cognitive mechanism involved in exposure therapies, in which a feared negative stimulus is habituated. Such therapies are generally effective in the treatment of anxiety disorders and post-traumatic stress disorder (Myers & Davis, 2007; Watkins et al., 2018). As has already been discussed, there is growing evidence that emotional exposure, and subsequent extinction of habitual emotional reactions, is the mechanism by which mindfulness reduces emotional distress (Uusberg et al., 2016). Therefore, both mindfulness and SWB homeostatic resilience involve the process of exposure; propositions that could be further tested in future research.
Adaptation is also automatic and often unconscious. It is a process by which challenging experiences are internally assessed and contrasted with prior experience, which reduces the perceived intensity of the experience. In the SWB literature, adaptation has mostly been referred to as hedonic adaptation, and is described as the process by which people typically acclimatize to events or stimuli that initially provoked intense positive or negative emotional responses (Armenta et al., 2014; Lucas et al., 2003; Luhmann & Intelisano, 2018). This form of adaptation is best understood through Adaptation Level Theory (Helson, 1964), which has been used to explain both sensory adaptation (adapting to the presence of a foul odor) and adaptation to affective states. Affective adaptation explains how the emotional effects of a positive or negative experience attenuate over time (Frederick & Loewenstein, 1999; Lyubomirsky, 2010).
While the adaptation process is largely automatic, it can also involve consciousness by directing attention away from the experience (Frederick & Loewenstein, 1999, p. 302) and, in this regard, has resonance with the process theory of emotion regulation (Gross, 2015b). Adaptation theory has also been used to describe the role of increased attention to the challenging event, a technique emphasized in mindfulness practice. According to Wilson and Gilbert (2008), attention allocation creates appraisal, accommodation and cognitive assessment, until the negative affect is “explained away.” While these authors do not consider mindfulness in this context, the process they identify has similarities with mindfulness attention, reappraisal, and emotion regulation discussed earlier. The similarities between mindfulness mechanisms and SWB habituation and adaptation deserves further investigation.
In summary, mindfulness mechanisms include positive reappraisal, exposure, and decentering, all of which have been previously described. Not only have these mechanisms been implicated in recovery from depression (Fresco et al., 2007; A. M. Hayes et al., 2007; Segal et al., 2019; Troy et al., 2010), but they are similar to the cognitive mechanisms and habituation that are part of SWB homeostasis. Mindfulness creates a “mental gap” between awareness and its objects (Brown et al., 2007, p. 216), or “a ‘space’ between one’s perception and response” (Bishop et al., 2004, p. 232). It effectively holds at bay the force of the emotional content, thus allowing the underlying mood (HPMood) to emerge to awareness, as the affective residue achieved while experiencing a general state of equanimity. We have described this as the experience of moodfulness, with moodfulness defined as conscious access to HPMood. This picture of moodfulness, however, is incomplete without an understanding of the relationship between SWB homeostasis and depression.
SWB Homeostasis and Depression
SWB homeostasis can withstand some modest level of challenge through the deployment of defensive resources. However, when the strength of challenge exceeds homeostatic capacity, homeostasis is defeated. In such cases, measures of HPMood and SWB will be flooded with emotional content, and SWB will move outside its setpoint range. Moreover, SWB will remain outside the range until homeostatic control is re-established.
The sum of these processes causes the relationship between SWB and challenging agents to be non-linear, as shown in Figure 1.
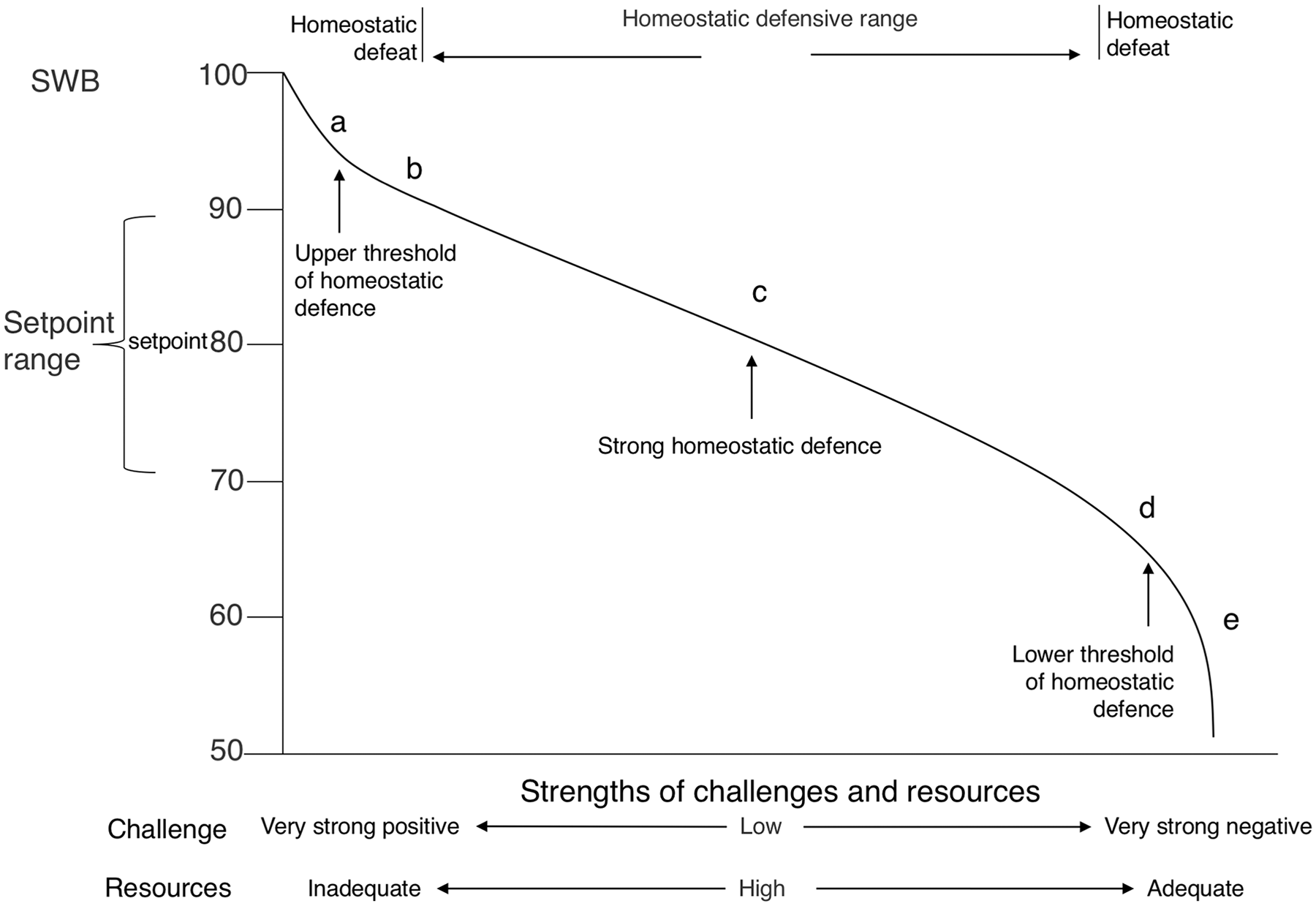
Changing levels of SWB as homeostasis is challenged.
The theory of SWB homeostasis explains not just SWB stability, through the defense of HPMood, but also change. As such, it is an evolution from earlier theoretical notes relating to happiness setpoints (e.g., Lykken & Tellegen, 1996), which assumed, without empirical support, that movements of SWB away from their setpoint were necessarily temporary, such that the level of SWB would always return to setpoint. This idea of impermanence has been commonly repeated in critiques of SWB setpoints, although recent reviews have recognized that complex dynamics involving stability and change are involved (Luhmann & Intelisano, 2018). For its part, homeostasis theory proposes that long-term change in SWB is caused by the persistent domination of challenging conditions over resources. This is an important aspect of understanding because some researchers have erroneously interpreted long-term change in SWB as evidence that setpoint theories have been “falsified” (Headey & Muffels, 2018, p. 862). Such declarations misunderstand homeostatic theory. Long-term change in SWB indicates a failure of resources, not of theory. When those long-term changes indicate a chronic failure of homeostasis, the likely implication is depression (Cummins, 2010).
The formal diagnosis of a major depressive episode involves the experience of persistent low mood and/or loss of pleasure in formerly pleasurable activities (American Psychiatric Association, 2013). It seems intuitive, therefore that such symptoms would equate to low levels of life satisfaction and wellbeing. At a broad level, the proposed inverse relationship finds ready support from the life satisfaction and wellbeing literature. For example, Headey et al. (1993) found depression and life satisfaction to be separate, yet highly negatively correlated (~–.6) constructs, while Friberg and Melin (1996) found a linear negative relationship between the number of self-reported depression symptoms and a quality of life measure, which includes subjective assessments of mood and energy. There is also emerging evidence of shared genetic influences on both psychopathology and levels of wellbeing or life satisfaction (Kendler et al., 2011; Nes et al., 2013). Moreover, both large-sample population studies (Strine et al., 2009) and longitudinal studies (Rissanen et al., 2011) have reported that low levels of life satisfaction are associated with later episodes of depression. Results such as these have encouraged researchers to question whether SWB measures can form a screening tool for risk of depression (Bartels et al., 2013).
Further exploration of the relationship between SWB and depression must, however, confront two crucial methodological issues. The first involves nomenclature. As has been discussed, homeostatic theory concerns the infusion of mood, specifically HPMood, into SWB. Thus, while many instruments purport to measure “quality of life” or the like, unless they specifically assess a subjective reflection of mood or affect, they are unlikely to be measuring SWB. One well-studied SWB instrument that has reliably demonstrated the infusion of HPMood is the Personal Wellbeing Index (PWI), and so this index features strongly in the following discussion.
The second issue involves the failure of most analyses to recognize the predicted non-linear relationship between levels of SWB and depression. Homeostasis theory predicts that the relationships will plateau, as resources rise to protect SWB from the challenge (see Figure 1). This plateau should be evident for mild levels of challenge (Cummins, 2010). Empirical supporting evidence comes from Bittar (2009). Analyzing cross-sectional PWI data, she demonstrated that while levels of SWB dropped as depression ratings increased, this fall was slight as depression increased from moderate to severe levels, before dropping more steeply as depression scores reached extremely severe (p. 130). She proposed that the PWI was as reliable an indicator of depression as other common depression screening measures.
A reasonable conclusion from these results is that low-level SWB and indicators of depression are linked. However, a more determined understanding of the relationship between SWB homeostatic defeat and depression requires a longitudinal study that could first establish the active relationship between SWB and depression symptoms while in homeostatic defeat.
In summary, there is certainly a relationship, at some level, between depression and homeostatic defeat. It therefore follows that the provision of additional homeostatic resources would be effective interventions for depression, by enabling the homeostatic system to better counter a challenge. If such support was sufficient to enable SWB to enter its setpoint range, then the homeostatic system would resume automatic control over negative emotions. If, however, these resources remain inadequate to deal with the level of challenge, then emotion will continue to dominate the conscious awareness of SWB. Therefore, the process by which such homeostatic defeat is restored may be by either, or both of, the weakening of the emotional reaction and the recruitment of homeostatic resources. Mindfulness aids in both processes.
Moodfulness: A Synthesis
To date, mindfulness has not been considered in the context of SWB homeostasis theory. However, a possible synthesis of these two bodies of research is as follows. When SWB is within its setpoint range, HPMood, as a mildly pleasant, free-floating affective state, effectively contributes to the experienced level of SWB. Emotion is normally also present but does not dominate the subjective experience of wellbeing. However, as emotions become stronger, homeostatic control is challenged. As emotion strength continues to rise, it generates strong and concomitant cognitions such as rumination, worry, and so on. As such, emotions begin to dominate consciousness, and increasing pressure is placed on the subjective experience of well-being to shift—acutely or chronically—away from its HPMood setpoint. The more SWB moves away from setpoint, the more conscious access to HPMood is reduced.
Resources, including cognitive mechanisms such as positive buffers, habituation, and adaptation, are homeostatically employed to counter such perturbations. If these counter measures are successful, homeostasis is maintained. If, on the contrary, such resources are insufficient to overcome the stressors, emotional dysregulation continues, and SWB plummets below its setpoint range as homeostasis is defeated. This defeat leads to an increased risk of depression.
Mindfulness acts as a circuit breaker in this downward spiral through the application of attention, emotion, and physiological regulation mechanisms, including reappraisal and exposure. Through these regulatory mechanisms, mindfulness reduces the intensity of the emotional content and assists in extinguishing maladaptive cognitive responses. Both self-focused emotion and cognition (“I am not good enough,” “I feel sad because I have no friends”) are transcended into mental phenomena or body sensations that are accompanied by curiosity rather than reactivity: In other words, they are met with equanimity. Such engagement, framed within the context of non-judgmental awareness, enables the partial or complete separation of the attribution of the distress to a situation, object, or the self.
The successful end result of these processes, over time, is to regenerate a state of consciousness, which allows the underlying mood (HPMood) to resurface as an active component of SWB. That is, a return to the experience of moodfulness, as the normally functioning state of consciousness, under conditions where emotion and cognition do not chronically overpower HPMood. Equanimity, then, is an outcome of the mindfulness processes engaged to dampen the overpowering mental content. Equanimity is the cognitive (non-judgmental) and affective (peaceful) experience of HPMood: the state of moodfulness.
Future Directions
The moodfulness model offers new understanding for the interaction between mindfulness and the homeostatic mood system. It explains how exposure, cognitive reappraisal, and emotion regulation are central to the effectiveness of mindfulness as a treatment for mood disorders, particularly depression. It thereby integrates mindfulness with the theory of SWB homeostasis, which explains both stability and change in SWB. However, areas that warrant further consideration include the following.
First, Buddhist philosophy assumes the path to happiness or the alleviations of suffering can be cultivated (Wallace & Shapiro, 2006), and that mindfulness practice (along with other components of the religious path) leads to the cultivation of nirvana, which has been described as a state of “transcendent bliss and peace” (Bodhi, 2011, p. 21). At first consideration, these might contradict the model. However, these two concepts are compatible with moodfulness when the cultivation of happiness is the cultivation of conditions that enable the normal experience of HPMood to emerge in consciousness. Then, the act of “cultivation” is a practice, which increases conscious access to enduring HPMood or the experience of moodfulness.
Second, our model focuses on the therapeutic mechanisms of mindfulness, concerning the treatment of psychological disorders. It is not proposed to explain the impact of long-term, intensive, meditation practice, such as that experienced by dedicated Buddhist monks and other practitioners who have committed to a path leading to enlightenment. For this group, mindfulness practice has been described as leading to “rapture, a form of pleasure that lies above and beyond anything that can be experienced in the normal state of consciousness” (Gunaratana, 2011, p. 12). It is possible, given this broader view, that our model has fallen into the trap warned by Grossman and Van Dam (2011), of exploring not mindfulness per se, but a feature of consciousness that is related to mindfulness. While it is almost certainly true that HPMood cannot explain all experiences of bliss, rapture, and insight that derives from long-term mindfulness practice, it can perhaps form a bridge to further such understanding.
Third, the model focuses on the cognitive and affective elements of mindfulness, omitting somatic processes. This is an issue because such processes are a core part of mindfulness training as outlined in the Satipatthana Sutta, the “discourse on the Establishment of Mindfulness,” a significant text in the Buddhist teaching (Bodhi, 2011). This text describes the four “establishments” (components) of mindfulness as contemplating “the body in the body . . . feelings in feelings . . . mind in mind . . . phenomena in phenomena” (Bodhi, 2011, p. 21). Indeed, many mindfulness practices lead to increased somatic awareness, or attention to body sensations, and the emergence of body sensations in consciousness is a core element of present-moment awareness. Such somatic awareness could form part of the stress reduction outcomes of mindfulness practice. Further insight into this possibility requires a systematic study into the relationship between physiological stress, psychological stress, and homeostatic restoration.
Fourth, we have not explored whether other psychological disorders might also involve the failure of SWB homeostasis, particularly those that involve habituated responses to stimuli, such as post-traumatic stress disorder and anxiety disorders. Given there is emerging evidence that mindfulness can provide beneficial results for these symptoms (Chiesa & Serretti, 2011; Hopwood & Schutte, 2017; Khoury et al., 2013), knowledge about the relationship between these conditions and SWB homeostatic defeat could also help to inform our model.
Finally, a technical challenge to testing this proposed model is that while certain homeostatic defeat is indicated by a level of SWB below 50 pp (Cummins, 2010), when such an evaluation is made within a single measurement, this could indicate a short-term acute event that may only temporarily defeat homeostasis. Chronic homeostatic defeat can only be confidently concluded through longitudinal data and, at best, the establishment of individual setpoints. These requirements prescribe challenging conditions of measurement for clinical purposes.
Conclusion
The conscious state created through mindfulness practice, described as equanimity, deserves more research attention. It is intriguing that this state, which is so central to Buddhist teachings, creates a mental gap, or space in consciousness, that reduces reactivity to cognition and emotion. Such reduction, in conditions of psychopathology, could allow for the re-emergence in conscious experience of the biologically determined, mildly activated, and slightly positive affect known as HPMood. This new understanding offers a practical advantage. If, as proposed, homeostatic defeat is the precursor of depression, then any activity that can restore normal homeostatic functioning can be used to aid recovery from depression. Instructed mindfulness offers such a restorative activity. Here, the associated mechanisms of exposure, decentering, and reappraisal reduce the pathological dominance of emotion and cognition in consciousness, allowing the natural homeostatic state of HPMood to emerge as present-moment awareness. It is thus possible that investigations into the scientifically derived theory of SWB homeostasis have serendipitously led to this link with ancient spiritual practice. Such a confluence of religion, philosophy, and science is an important step to better understanding of how human suffering can be eased.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.