
Abstract
This study models primary abstinence and age at first sex in a cross-sectional sample of Ghanaian youth aged 17 to 22 years. The aim is to examine how reproductive knowledge and social cognitive factors jointly affect the choice to initiate sex. Among males, the authors find that reproductive knowledge is negatively associated with abstinence. Its negative association, however, is moderated by the extent of adult support a respondent receives. Among females, reproductive knowledge is positively associated with abstinence. Its positive association is moderated by the extent of household sex communication. Correspondingly, when age at first sex is modeled, knowledge is a negative predictor among females. Its effects are mediated by household sex communication. A third social cognitive variable, perceived permissive peer attitudes about sex, is not associated with knowledge but is a protective factor for sexual initiation for both sexes. Though causal direction cannot be established, the results suggest that cognition affects sexual initiation both directly and through complex social mechanisms. The evidence provides theoretical support for comprehensive adolescent sexual and reproductive health interventions that promote abstinence and other safe sex behaviors through social as well as individual pathways.
In recent years, African youth have been exposed to a range of sexual risk reduction interventions (Agha, 2002; Hindin & Fatusi, 2009). In addition to educating young people about sexuality, pregnancy, contraception, HIV/AIDS, and other sexually transmitted diseases (STDs), adolescent sexual and reproductive health (ASRH) interventions advocate specific behavioral choices such as abstinence, monogamy, and condom use. The theory underlying the earliest, first-wave ASRH interventions was that, given the information, a young person will rationally choose to adopt these protective behaviors. Measurable behavioral changes, however, were usually quite modest (Hindin & Fatusi, 2009). Where program treatment effects did occur, they were generally not uniform.
More recent ASRH programs anticipate multiple causal mechanisms and incorporate a comprehensive package of interventions such as working with parents, using peer educators, and organizing “enter-education” events. Second-wave interventions use classrooms, workplaces, and public events to disseminate safe sex messages. Employing multiple strategies and communications channels, these comprehensive interventions aim to induce social as well as individual effects on targeted behaviors (Ross, Dick, & Ferguson, 2006). Knowledge and peer assessments are examples, respectively, of individual and social effects. The varied strategies of comprehensive ASRH interventions reflect the complex relation between cognition and behavioral change. Recent research findings support the comprehensive approach. In Ghana, the country we study here, social connectedness—measured by peer relationships and school attendance—and parental monitoring have been shown to affect sexual decision making among adolescents (Biddlecom, Awusabo-Asare, & Akinrinola, 2009; Kumi-Kyereme, Awusabo-Asare, Biddlecom, & Tanle, 2007). Karim, Magnani, Morgan, and Bondl (2003) showed that normative perceptions (perceived peer norms), particularly the belief that one’s peers are sexually active, increases the probability of sexual debut among a sample of Ghanian youth aged 14 to 24 years.
Various approaches have been used to conceptualize behavioral change processes. According to social cognitive theory, knowledge about a particular health risk, expected outcomes should a particular behavior be adopted, and the observed behaviors and outcomes of others all combine to form an actor’s self-efficacy (Bandura, 1986, 1990). Like other psychological theories, social cognitive theory posits that knowledge about risky behaviors and how to reduce risk predicts adoption of safe-sex practices (through the self-efficacy mechanism). It adds, however, a social component in that the decision process is also influenced indirectly by the perceived belief or the appraisals of significant others about the risk and the response to it. Social cognitive theory might therefore explain change processes caused by exposure to second-generation ASRH interventions. Behavioral change, in other words, may depend on social effects and not just individual cognition. In this article, we probe these theoretical social processes by modeling one ASRH outcome, sexual initiation as a function of reproductive knowledge, and three social cognitive constructs: parental communication about sex, adult support, and perceived peer attitudes toward sex. We test whether reproductive knowledge (cognition) interacts with one or more of these social variables, affecting the behavioral choice differentially, that is, changing the direction or strength of the relationship between predictor and dependent variable (moderation). We also test whether reproductive knowledge operates through one of the social variables (mediation). A social variable, in other words, could explain some of the causal effect (Baron & Kenny, 1986). There may be a direct knowledge effect as well as indirect effects through one or more social cognitive mechanisms that jointly affect sexual initiation and age at first sex.
Previous work supports this approach. According to the integrative model, environmental constraints (that hinder risky practices) and social normative pressure (to act as significant others do) are two of eight components that determine whether an individual will engage in a specific health-related action (Fishbein, 2000). In a recent review of the U.S. adolescent sexual behavior literature, Buhi and Goodson (2007) demonstrated that empirical support is strongest for three integrative model components: intention, environmental constraints (e.g., time alone with the opposite sex), and social normative pressure (peer influences). In this article, we model the latter two components. Time spent with, and support received by, adults are our environmental concepts. We use perceived peer beliefs and practices regarding safe sex practices to tap the peer influence component.
Methods
Sampling
We examine data generated by an evaluation of the comprehensive African Youth Alliance (AYA) ASRH project in Ghana (John Snow Incorporated, 2007). The evaluation was carried out by the University of Ghana Institute for Statistical, Social and Economic Research (ISSER) and JSI Research and Training Institute, Inc.
A random sample of 180 municipalities was selected from Ghana’s 2000 household census. A total of 88 municipalities were selected within specific clinic service areas where the AYA interventions were carried out. Matching municipalities were then selected based on population, distance to capital cities, presence of a health facility, and child mortality levels. Once municipalities were identified, two-stage stratified cluster sampling was used to obtain the required sample (Dorofeev & Grant, 2002). Enumeration areas (EAs) were stratified by municipality, and then 105 EAs from the intervention areas and 75 EAs from the control areas were randomly selected using probability proportional to size (Dorofeev & Grant, 2002). The target sample size was 3,500 young people aged 17 to 22 years. Actual sample size was 3,416.
Data Collection Instruments
A standard individual questionnaire captured information on location, identification, and background characteristics; self-reported exposure to the AYA interventions; knowledge, attitudes, perceived risk, and motivation to avoid unsafe sex and unwanted pregnancy; and sexual and other health behaviors. A second questionnaire, administered to parents, included a roster of household occupants, an inventory of household assets, and a series of questions to measure parents’ perceptions of local ASRH issues. Survey item responses were coded discretely as yes/no or Likert-scaled (strongly agree, agree, neither agree nor disagree, disagree, strongly disagree).
Validity was increased by using questions and question sequences from previously validated instruments such as the Demographic and Health Surveys. The instruments were translated into three local languages (Twi, Ga, and Fante). After a field test, final revisions were made to the instruments. The University of Ghana Institutional Review Board reviewed and approved the protocol and instruments before conducting the study.
Data Collection and Data Entry
Fieldwork took place from April 20, 2006, to June 5, 2006. Data were collected by five field interviewer teams. All interviewers and supervisors were college juniors and seniors or graduates younger than 35 years. Wherever possible, interviewers were assigned to regions that spoke their native languages. Interviewers received 1 week of training. The training included a review of field procedures, ethical issues, and interviewing techniques.
Maps were collected from the Census Office for each sample EA and were provided to the five team supervisors. In the field, the teams divided each EA into segments of approximately 20 to 40 households each and then randomly selected one of those segments for study. All households in the selected segments were visited, and attempts were made to interview all eligible youth in those households. The household questionnaire was completed only if the household had an eligible youth.
In the case of households with eligible youth (age 17 to 22 years) who were not present at the first visit, or households with no one at home, at least three visits were made before dropping the household from the list. All interviews were verbal, face-to-face. Interviewers recorded all responses on the standardized questionnaires. Before conducting interviews, the interviewers obtained informed consent from heads of household, from the youth themselves, and from the parents of 17-year-old youth. In all youth interviews, respondents and interviewers were of the same sex, and the interviews were conducted in private. The 3,416 completed interviews included 1,836 females and 1,580 males from 2,855 households. Of these, 250 interviews were rejected, either because subjects were out of the target age range or because substantial numbers of items were incomplete. Data from completed questionnaires were double entered at the University of Ghana ISSER Centre using the EpiInfo program. After cleaning, the final data set consisted of 3,166 interviews.
Variables
Dependent variables
The first outcome we model is sexual initiation: whether or not a respondent reported ever having had sexual intercourse. We did not distinguish between vaginal and anal intercourse. The second outcome is age at first sex. This variable is approximately normally distributed.
Independent variables
To measure reproductive knowledge, we combined three items the responses to which were most strongly correlated with age at first sex. Two were multiple response items: “What causes AIDS?” and “What are the signs of a sexually transmitted disease?” The third question was “Is it possible for a girl to get pregnant if the boy withdraws before ejaculation?” We weighted correct responses to these questions with +1 and incorrect responses with −1. We treat this as a simple additive index.
Factor analysis identified seven items, Likert-scaled, that best combined to measure parental sex communication. The items were multiple responses to a single question on the household head interview: “How often do you talk about the following topics in this household?” (Responses: Young peoples’ health, the disease called HIV, ways for young people to avoid pregnancy, ways for young people to prevent STD, abstinence from sex, having only one sexual partner, relationship between boyfriends and girlfriends). The Cronbach’s alphas were .89 for males and .90 for females.
To measure adult social support, respondents were asked which adult most supported them. Half of the respondents identified a parent. Eighty-five percent identified a relative. The best index was formed by 14 Likert-scaled responses to the question: “[Thinking about that adult with whom you spend the most time] Please tell me if you strongly agree, agree, neither agree nor disagree, disagree, or strongly disagree with the following statements about your relationship with this person”: She or he supports and encourages me; she or he gives me attention and listens to me; she or he shows me affection; she or he praises me; she or he comforts me; she or he respects my sense of freedom; she or he understands me; she or he trusts me; she or he gives me advice and guidance; she or he provides for my necessities; she or he gives me money; she or he buys me things; she or he has open communication with me; she or he spends time with me (α = .90 for males, α = .94 for females).
Three Likert-scaled questions formed the best additive scale for perceived peer attitudes toward sex (perceived peer norms): “Most of my friends believe it is OK to have sex with a steady girlfriend or boyfriend”; “Most of my friends believe it is OK to have sex with more than one partner in one month”; “Most of my friends believe that one should have regular sex to avoid health problems” (α = .56 for males, α =.34 for females).
To measure socioeconomic status, we used an approach based on household assets (Filmer & Pritchett, 2001). Principal component analysis was used to examine the correlations among 15 household assets. The items were binary: safe water; safe toilet; permanent floor; permanent roof; gas, electric, or kerosene cooking fuel; electricity; radio; television; video recorder; telephone; refrigerator; computer; bicycle; motorcycle; car (α = .79 for both sexes). The first principal component (eigenvalue) is used to generate the wealth index. We created a five-category variable from this continuous variable.
Data Analysis
Of the 3,166 young people, 1,553 (49%) responded that they had had sex and stated their ages at first sex. We use logistic regression models to model sexual initiation. The probability of sexual initiation is modeled as a function of reproductive knowledge and the additive and interactive effects of parental sex communication, adult support, and peer attitudes toward sex. Moderation is assumed to occur when reproductive knowledge interacts with parental sex communication, adult support, or perceived peer attitudes, that is, the t test for any of these interaction terms is significant at the p < .05 level. Data exploration revealed an additional set of covariates that correlated with sexual initiation—respondent’s age, ethnicity, employment history, religiosity, whether respondent’s father works in a primary occupation (agriculture, mining, forestry), and whether respondent’s parents are married. We control for these in all models. Controlling for age will also control for unobserved effects that may be age dependent, such as recall or reporting bias, as well as cohort effects such as changes in schools or economic shocks. Schooling and school enrollment and self-reported exposure to AYA were not correlated with the outcomes, so we do not model their effects. Males and females are modeled separately.
For the subset of sexually initiated youth, we use linear regressions to model the age at first sex (dependent variable), conditional on the same covariates. We add interaction terms in these models as well to test whether a candidate’s social cognitive variable moderates the effects of the knowledge variable on the outcome. We test for mediation in those models where the knowledge variable and one of the social cognitive variables are jointly significant. In the mediation models, which were also estimated using Stata, we specify reproductive knowledge as the independent variable and parental communication, adult support, and perceived peer attitudes as the candidate mediating variables. We use both parametric Sobel–Goodman and nonparametric bootstrapped tests to ascertain statistical significance of the mediation effects (Baron & Kenny, 1986).
In all, we fit 12 additive and interactive sexual initiation models—six for males and six for females. Of these, two models showed significant interactions, one for each sex. For age at first sex, we first fit baseline models for both sexes. Significant social cognitive variable slopes were found only among females. We fit mediation models for these three. Results are shown in a table later in the text.
All eligible youth in sample households were interviewed so it is likely that siblings share some unmeasured characteristics. Standard errors might be underestimated because of this intraclass correlation. Second, data are generated at both individual and household levels of aggregation. In all our models, we correct for these potential design effects, specifying household as the primary sampling unit.
Results
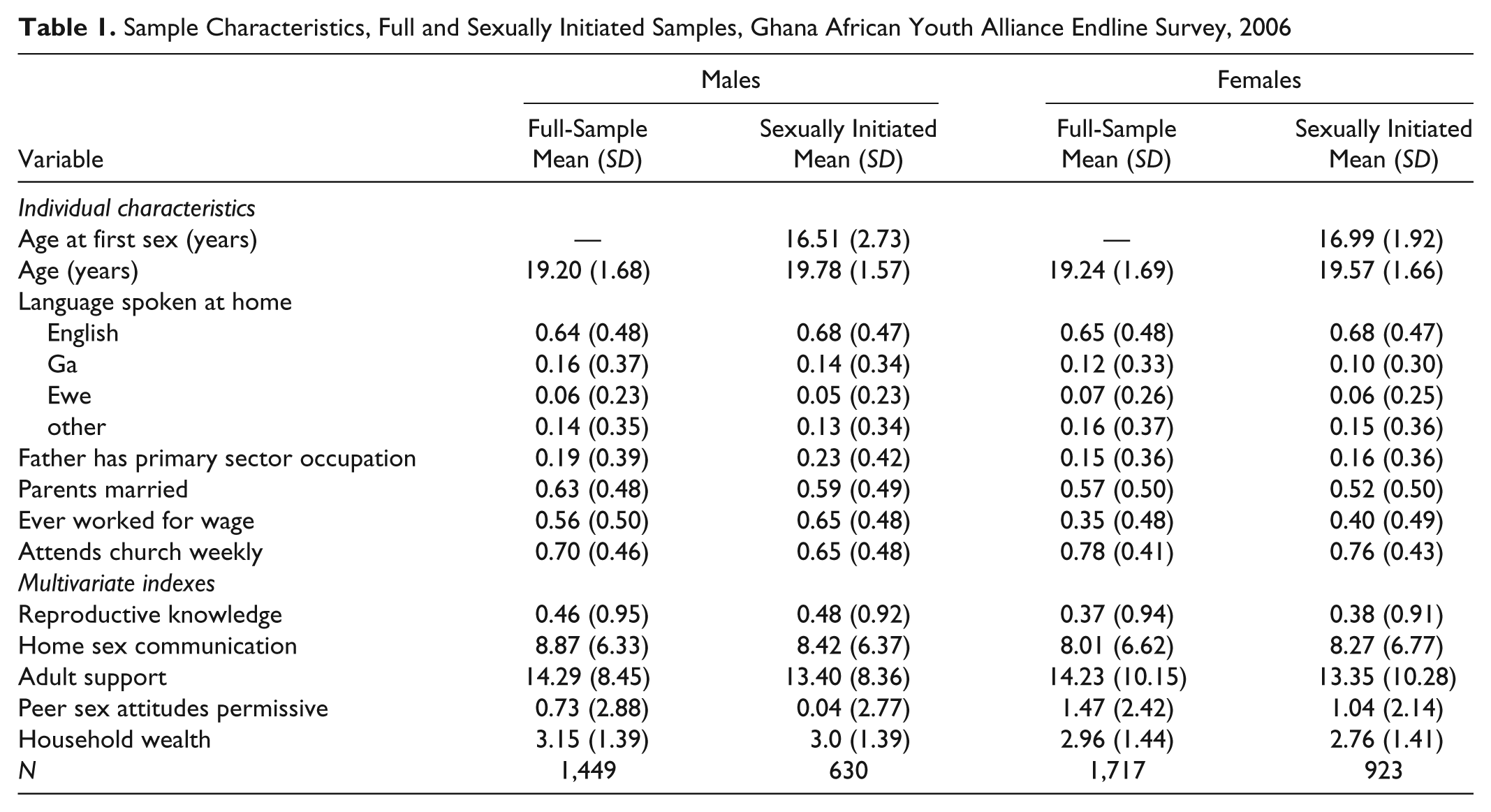
Overall, 43% of males and 49% of females reported they had had sex. The mean age at first sex was 16.5 years for males and 17.0 years for females (Table 1).
Sample Characteristics, Full and Sexually Initiated Samples, Ghana African Youth Alliance Endline Survey, 2006
Sexual Initiation
Logistic model results for sexual initiation are shown in Table 2. In these multiple regressions, all coefficients are jointly estimated. Looking first at additive models (Models 1 and 3), several control variable coefficients are significant. For both sexes, higher socioeconomic status, having parents who are currently married, and regular church attendance are all negatively associated with the probability of sexual initiation, whereas having ever worked for a wage is a risk factor. Among males, those whose fathers have a primary sector occupation (farmers, foresters, or miners) are more likely to have had sex. Reproductive knowledge is not significantly associated with sexual initiation for either sex. Two of the three social cognitive variables are significant for both sexes. Respondents who perceived their peers as having permissive views on sexual matters were less likely to report having had sex themselves as were those who reported relative high levels of adult support. Among males, the more communication about sex reported by the parent, the more likely the respondent was still celibate.
Logistic Multiple Regression: Sexual Initiation Controlling for Selected Individual and Household Factors, African Youth Alliance Endline Survey, Ghana 2007
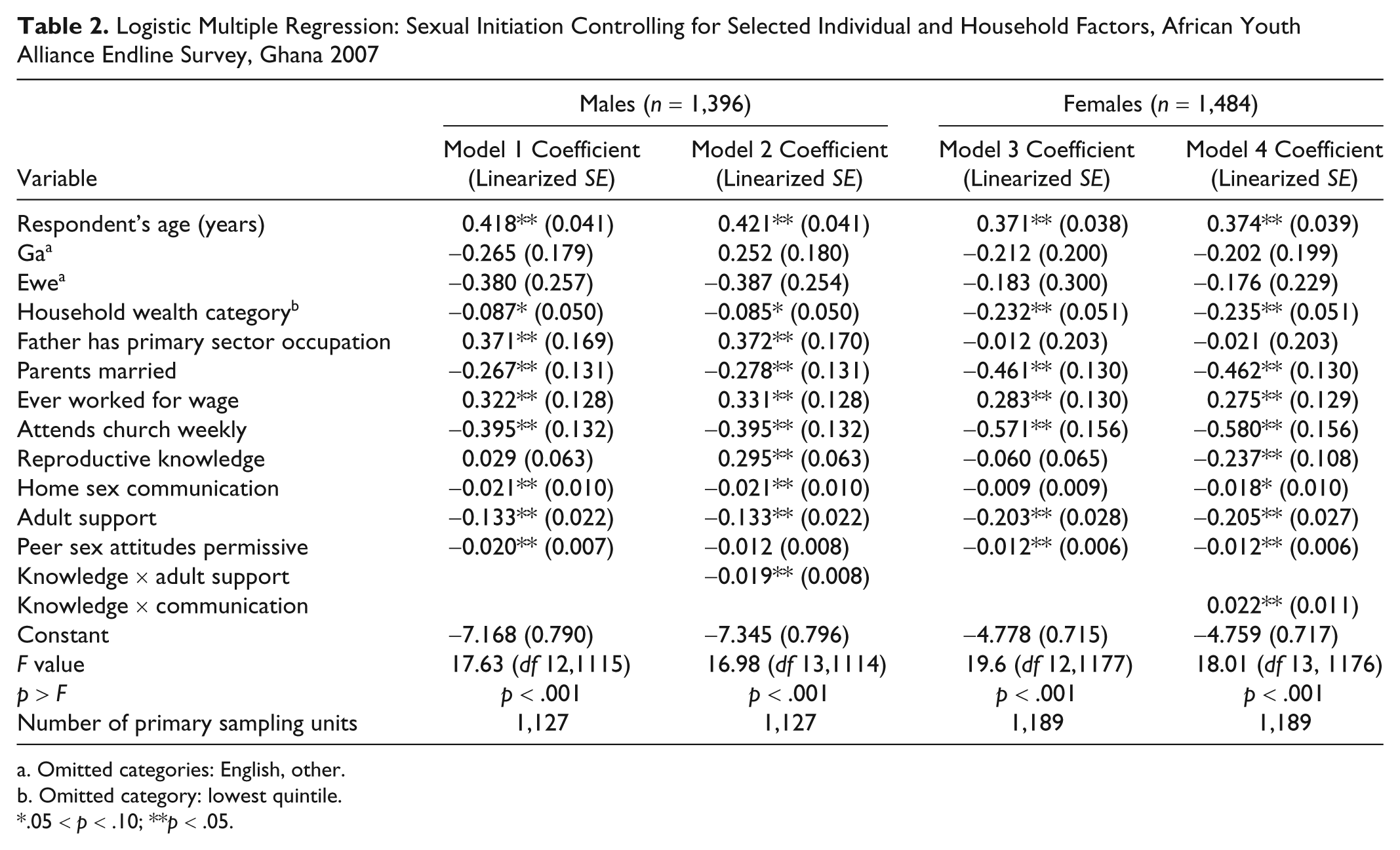
Omitted categories: English, other.
Omitted category: lowest quintile.
.05 < p < .10; **p < .05.
Continuing with Table 2, two interactions were significant and these are reported in Models 2 and 4. Among males, the level of reproductive knowledge becomes a positive predictor of sexual initiation (i.e., higher levels of knowledge are associated with lower levels of primary abstinence), when the knowledge/adult support index interaction term is added. The negative interaction shows that knowledge is less of an explanatory factor, the higher the adult support score. Among females, reproductive knowledge and household sex communication significantly interact. Specifying the interaction causes both variables to become significant protective factors. Here the interaction is positive: The more household sex communication reported by the parent, the more protective the knowledge effect.
Age at First Sex
We next estimated the corresponding ordinary least squares (OLS) models for sexually initiated youth. In additive models (results not shown), permissive peer sex attitudes is the only significant covariate among males (other than age) and its effects on age at first sex are protective. Males who perceive their peers to have permissive sex values tend to wait longer to initiate sex. Among females, socioeconomic status, having parents who are married, and regularly attending church all have the same protective effects as in the earlier models. In contrast, age at first sex is lower for females whose fathers work in the primary sector. It is also lower for females with higher levels of reproductive knowledge. Looking at the social cognitive variables, the intensity of intrahousehold communication about sexual matters is also associated with lower age at first sex for females. As with males, perceived permissive peer sex attitudes are associated with older ages of initiation.
In these additive models, the older the respondent at the time of the survey, the longer that respondent waited to have sex. This may signify a cohort effect: Adolescents may be initiating sex at earlier ages than their older counterparts in the survey.
Indirect Effects on Age at First Sex
Since reproductive knowledge was insignificant in the male additive OLS model, we explore its indirect effects only among females. These models are shown in Table 3. In the earlier logistic models, factors protective for sexual initiation are negatively signed; protective factors ought to be positively signed when the outcome is age at first sex. The opposite should be true for risk factors. A comparison of Tables 2 and 3 shows this is largely the case.
Linear Multiple Regression of Age at First Sex on Knowledge With Selected Mediators, African Youth Alliance Endline Survey, Ghana 2007 (n = 923 Females)
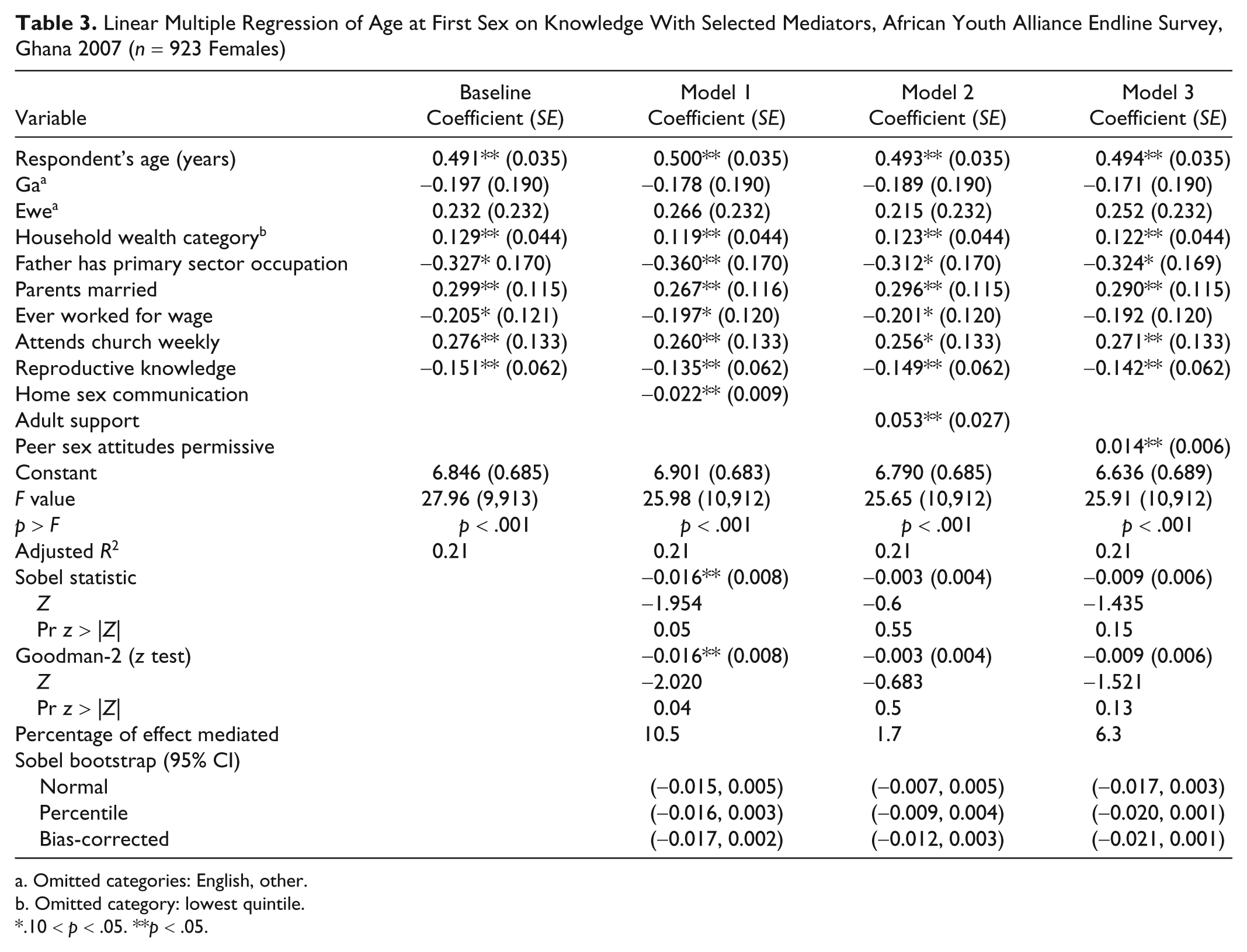
Omitted categories: English, other.
Omitted category: lowest quintile.
.10 < p < .05. **p < .05.
We added interaction terms to the OLS models to test whether the social cognitive variables moderate the effects of reproductive knowledge on age at first sex. In contrast to the logistic models, no significant interactions were found (results not shown).
We did, however, find evidence of mediation. Knowledge, in other words, operates directly, through cognition, and indirectly through other channels. Comparing the additive OLS models with those shown in Table 3, most of the regression coefficients, as one would expect, are equivalent. They are also similar across the three mediation models shown in Table 3, implying that the models are robust.
The baseline model in Table 3 includes the control variables and reproductive knowledge but not the social cognitive variables. Examining the first mediation model, reproductive knowledge remains a negative predictor of parental sex discussion as it is in the auxiliary equation (results not shown). The candidate mediator in this model is the extent of parental sex discussion. Its effects are negative as they are in the earlier OLS model (results not shown). The Sobel–Goodman statistics are both significant, but the nonparametric bootstraps do not show a significant mediation effect. The model estimates that about 11% of the negative cognitive effect on age at first sex operates through the parental discussion mechanism.
In Model 2, reproductive knowledge has the same negative effect as in the baseline model. The candidate mediator, perceived permissive peer group attitudes toward sex, has a positive association with age at first sex. There is no evidence of moderation in this model.
Model 3 shows the effects of reported adult support. The more such support, the model shows, the longer a respondent waited to have sex. The mediation test statistics fall short of statistical significance.
Summarizing, the results in Table 3 suggest that, for females, reproductive knowledge is mediated by just one of the three social cognitive constructs—the home communication mechanism. Though the Sobel–Goodman statistics are significant, we would be on stronger inferential ground if the nonparametric tests were also significant.
Discussion
This study examines the effects of reproductive knowledge and social cognitive factors on a young person’s decision to initiate sex and on the age of sexual initiation. Our results are consistent across model specifications and are generally consistent with earlier Ghanaian studies (Biddlecom et al., 2009; Karim et al., 2003; Kumi-Kyereme et al., 2007; Sallar, 2008). These studies suggest that the environmental and social normative components of the integrative model (Fishbein, 2000) do affect adolescent sexual decision making.
Looking first at covariates, for both sexes socioeconomic status, religiosity, and intact household structure are protective factors against sexual initiation, whereas employment outside the home and having a father engaged in the primary sector are risk factors. Glover et al. (2003) reported similar findings in their study of adolescents in three Ghanaian towns.
Looking at reproductive knowledge, our evidence suggests that this variable has opposite effects in males and females. More knowledgeable males were less likely to be celibate, whereas the opposite is true for females. That is, greater knowledge is positively associated with abstinence among females, but counterintuitively, not for males. However—and also counterintuitively—among females who have ever had sex, reproductive knowledge is associated with younger age at first sex. The conventional view is that knowledge should have a protective effect: forewarned is forearmed. Our evidence suggests otherwise. A decision to initiate sex may itself cause young women to want to be more informed and to learn more about sexuality. Alternatively, sexually active women are simply more knowledgeable about STDs, HIV, pregnancy, and so on. Because the data are cross-sectional, causal order is ambiguous. It is also possible that some unmeasured variable(s) causes both knowledge and sexual initiation, that is, knowledge and sexual initiation may be endogenous. 1 Longitudinal research and/or qualitative studies are needed to identify the true knowledge/celibacy relationship.
Looking at the three social cognitive variables, all are protective with respect to sexual initiation (Table 2). The more their parents discuss sex with them and the more adult support they receive, the more likely that young Ghanaians remain abstinent. Karim et al. (2003) also found a positive association between household sex communication and abstinence among Ghanaian males. Biddlecom et al. (2009) and Kumi-Kyereme et al. (2007) reported similar findings for adult support, although they defined it differently. In those studies, the closer their parents monitored them, the less likely young Ghanaians were to have had sex in the preceding 12 months (i.e., primary or secondary abstinence).
Interestingly, primary abstinence, which we model, was more likely if respondents thought that their peers have permissive attitudes about sex. This may reflect a social comparison phenomenon. A young person may naturally perceive himself or herself as more cautious than others. This peer perception finding is at variance with Karim et al. (2003). In that study, Ghanaian adolescents of ages 12 to 24 years who perceived their peers to be sexually active were more likely themselves to be sexually active. The difference could be because of the measures used. 2
In summary, our results reveal that knowledge affects sexual initiation both directly and indirectly. The significant interactions in our models suggest two distinct moderation mechanisms. For males, adult support moderates the positive cognitive association with sexual initiation. For females, household sex communication reduces the protective effect of cognition. Thus, the social cognitive variables affect males and females differently through their moderating effect on reproductive knowledge. We find a third social cognitive mechanism among sexually initiated females. Knowledge, the mediation models show, is mediated by household discussion about sexual matters. Knowing about reproduction and talking about it with one’s parents are jointly associated with younger ages of sexual initiation. Parental communication apparently channels some of the negative reproductive knowledge effects on this outcome. Clearly, social effects on sexual initiation and age at first sex vary by gender.
A number of limitations to this study must be acknowledged. Because the data are cross-sectional, causal order of reproductive knowledge and sexual initiation cannot be established. This is true for all models reported here. A second limitation is that self-reported sexual behaviors are possibly biased (Mensch, Hewett, & Erulkar, 2003). Respondents may feel uncomfortable or they may tend to give socially desirable answers. Third, measures might have been more valid and precise had resources permitted. Using items from earlier surveys conferred some degree of validity, however, we did not systematically test the validity of the items we added to the instruments. The reliability of one of our social cognitive indices—that for perceived peer attitudes—was noticeably low. More precise items in our questionnaire might have averted this. Fourth, our use of the social cognitive and integrative models is more suggestive than definitive. A more robust operationalization of the integrative model would incorporate measures of its other dimensions—skills, self-efficacy, self-image, emotional reactions to sexual initiation, and so on.
Directions for Future Research
Overall, our results generally agree with Buhi and Goodson (2007): Environment and peer influences affect adolescent sexual decision making. More careful longitudinal studies, and/or qualitative research, are needed to verify this and to determine the true magnitude and direction of any direct causal effects. Qualitative research in individual settings would also be useful in determining how support mechanisms work and what messages could work best through different sorts of networks (e.g., peer, family, other adult). It is hoped that more research, using different sociocognitive measures, will reveal more about the interesting gender differences we observed.
Implications for Health Education Practice
Though our results do not fully elucidate the mechanisms, they do suggest, as others have in varying settings, that comprehensive ASRH interventions that investigate, understand, and tap into familial and peer support mechanisms, in addition to providing accurate factual information, may be more successful in promoting abstinence and delay of sexual initiation than approaches that simply provide young people with information.
Footnotes
The authors declared the following potential conflicts of interests with respect to the authorship and/or publication of this article:
The original research and some time working on the article was carried out as part of Jessica Posner’s and Timothy R. Williams’s work as employees of John Snow, Inc. (JSI), a public health consulting company, under a grant from the Bill and Melinda Gates Foundation (BMGF). Neither JSI nor BMGF have any interests or products that are represented or discussed in the contribution. Therefore, there is no conflict of interest.
The authors received financial support for the research but not for the authorship of this article.