
Abstract
Cervical cancer is preventable with treatment of precancerous lesions and treatable at early stages. Hispanics have higher rates of cervical cancer and lower rates of screening. Ayndando a las Mujeres con Informaccion, Guia, y Amor para su Salud (AMIGAS) is an intervention to increase cervical cancer screening in U.S. women of Mexican origin. AMIGAS was developed with the participation of the community using intervention mapping (IM). Following the IM process, the authors completed a needs assessment, development of program objectives, selection of intervention methods and strategies, and program design. A benefit of IM is its linkage with community-based participatory research as it includes engagement of community members to identify and refine priority areas. The success of this strategy suggests it a useful tool for other populations. The resulting intervention program is currently being tested for efficacy and cost-effectiveness in three sites: El Paso, Texas; Houston, Texas; and Yakima, Washington.
Keywords
Both the incidence and mortality from cancer of the uterine cervix have decreased dramatically in the United States since the introduction of the Papanicolaou (Pap) test in the 1950s. Each year 12,000 women are told they have cervical cancer and about 4,000 women in the United States die from this preventable disease (U.S. Cancer Statistics Working Group, 2010). Worldwide, cervical cancer continues to be an important public health problem, and in many developing countries, it is still a leading cause of cancer death in women (World Health Organization, 2009). Cervical cancer is both treatable and curable if found early, and the Pap test can find premalignant lesions before they become cancer (Agency for Healthcare Research and Quality [AHRQ], 2010). Current screening guidelines for cervical cancer in the United States for women of average risk recommend that women begin screening at the age of 21 years or within 3 years of onset of sexual activity, whichever comes first. Women with three consecutive negative cytology tests can be screened every 3 years (AHRQ, 2010).
Even though substantial efforts have been made in the United States to reduce cervical cancer incidence and mortality by increasing screening, there remains a need to increase screening rates among certain racial and ethnic minority groups (Curry, Byers, & Hewitt, 2003). Hispanic women have traditionally had lower screening rates than non-Hispanic women (Castrucci et al., 2008). Furthermore, there are variations in socioeconomic status and acculturation among Hispanic women that may negatively influence screening. Women of Mexican heritage have lower cervical cancer screening rates compared with other Hispanic subgroups (Ramirez, Suarez, Laufman, Barroso, & Chalela, 2000). Although national rates of cervical cancer screening for Hispanic women are now comparable with those of non-Hispanic White women (85% and 83%, respectively, in 2008; Centers for Disease Control and Prevention [CDC], 2008), rates of screening are lower on the U.S.-Mexico border with only 80% of women reporting having a Pap test within the past 3 years (Texas Department of State Health Services, 2007).
Based on strong evidence of its effectiveness in increasing cervical cancer screening, the U.S. Community Preventive Services Task Force recommends interventions that include a one-on-one education strategy (Task Force on Community Preventive Services, 2008). However, few intervention approaches have been tested with Hispanic populations and, therefore, may not address the most important cultural and linguistic barriers and facilitators to cervical cancer screening faced by Hispanic women, particularly women who live in rural or U.S.–Mexico border areas. To increase cervical cancer screening in Hispanic women, developing and testing theoretically based, culturally and linguistically appropriate interventions is the first step. One method for developing such a program is using intervention mapping (IM; Bartholomew, Parcel, Kok, Gottlieb, & Fernandez, 2011).
Intervention Approach
IM is an intervention planning method that provides a system for “integration of theory, empirical findings from the literature, and information collected from the target population” (Bartholomew, Parcel, Kok, & Gottlieb, 2001, p. 546) to develop culturally appropriate and theoretically sound interventions. IM is a process for bridging the gap between theory-based research and the development of appropriate interventions for practice. It uses an ecological approach that enables developers to focus both on individual and environmental factors which affect behaviors while requiring input from the communities that will be affected and the individuals intended to deliver the intervention (Kok, Schaalma, Ruiter, van Empelen, & Brug, 2004). It is an approach that is ideally suited to the involvement of community members, as it requires the input of all stakeholders in the development of the intervention.
The purpose of this article is to describe how IM was used in the context of a community-based participatory research (CBPR) approach to develop a culturally appropriate, theoretically sound intervention for Hispanic women (women of Mexican heritage) living along the Texas–Mexico border. This intervention, “Ayudando a Las Mujeres con Informacion, Guia y Amor para su Salud” (AMIGAS), was developed to be delivered by lay health workers (promotoras de salud), as this approach has been found to be successful in other programs with this population (Fernandez et al., 2009). Detailed descriptions of intervention development are important so that researchers and practitioners can adapt interventions to settings and populations other than the original one, thus improving likelihood of replicating and maintaining an effect (Kegeles et al., 2000; Kok et al., 2004).
Health education specialists regularly use logic models as they consider ways to intervene with communities on specific health issues. One of these models is the PRECEDE/PROCEED model (Green & Kreuter, 1999). Unfortunately, although educators can see the logic of moving from research results to theory to the need for a planned intervention, the actual work of considering the many predisposing, enabling, and reinforcing factors, the theoretical constructs involved, and the possible strategies that might be used may be overwhelming. Little is published that describes how these planning and development processes of health education have been put into practice (Green, 2000; Nutbeam, 1996).
The IM process originated as a tool to assist health education specialists in moving from the needs and resources assessment phases of The PRECEDE/PROCEED model to the development of interventions. The six steps of the IM process are (a) needs assessment, (b) creating matrices of proximal program objectives and theoretical constructs, (c) choosing theoretical methods and practical strategies, (d) designing a program, (e) developing adoption and implementation plans, and (f) monitoring and evaluating the program. These steps not only guide the researcher but also require involving members of the community and potential end users of the intervention to improve the likelihood of dissemination and use by practitioners because the design and format are designed to match the population and delivery setting (Glasgow, Lichtenstein, & Marcus, 2003). Our Community Advisory Board (CAB), which was developed specifically for the formative research phase of this project—initial development of AMIGAS—included practitioners from the community, members of community-based organizations, lay community health workers (promotoras de salud) who were already involved in community work, and members of the priority community. The core group was made up of 10 people that met quarterly, originally to oversee the research that was being conducted in the community and later to help in the development of the intervention. During intervention development, they helped recruit others from the community who were involved in various aspects of intervention development, such as reviewing what had been found in the survey research, clarifying what the data might mean, deciding what intervention methods would be most appropriate, giving input on the development of materials, and recruiting women to assess materials before final development.
CBPR is described as
scientific inquiry conducted in communities in which community members, persons affected by condition or issue under study and other key stakeholders in the community’s health have the opportunity to be full participants in each phase of the work: conception–design–conduct–analysis–interpretation–conclusions– communication of results. (U.S. Department of Health and Human Services, 2008)
In reality, researchers may use concepts of CBPR but not necessarily all of them or in all phases of research. In developing the AMIGAS intervention, we included our community members in several aspects of the development of the program, as will be described in this article, but they were not involved in the collection and analysis of the qualitative and quantitative data or the development of data collection tools beyond reviewing the language for clarity.
In CBPR, the community should participate in the budgeting of the project when possible. The original AMIGAS project was funded through a cooperative agreement between the University of Texas School of Public Health and CDC. The budget for the project was developed by the researchers and the CAB had modest input on how to spend the money as the project unfolded. The second phase of the project was a contract between CDC, Battelle Centers for Public Health Research, several community-based organizations, and their lay health workers who modified and updated AMIGAS. The Lay Health Worker Advisory Council (LHWAC), which was formed in the second phase to modify the intervention, had input into how the money in the contracts was spent (Figure 1).
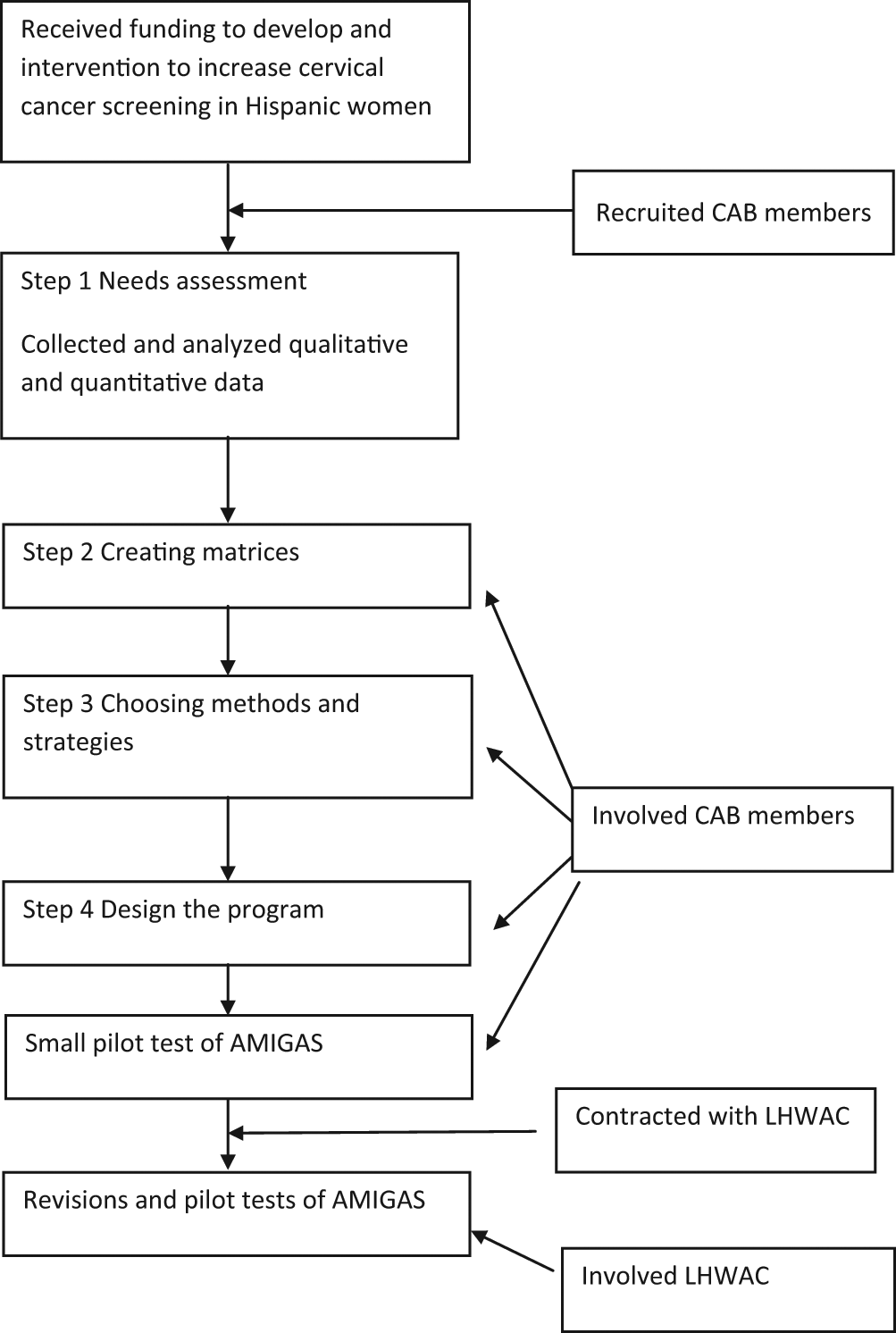
The AMIGAS development process
Method
Our research protocol was approved by the University of Texas Health Science Center–Houston Committee for the Protection of Human Subjects.
Needs Assessment (Step 1)
Needs assessment data may come from the literature, behavioral theories, and new data collection. To better understand why Hispanic women, especially those on the U.S.–Mexico border, were not being screened for cervical cancer, the AMIGAS research team (the university researchers and research assistants) completed a review of the literature, and conducted 13 focus groups (representing age categories: 18-25 years, 26-39 years, and ≥40 years) with 84 Hispanic women from El Paso (Byrd, Chavez, & Wilson, 2007). Results of the focus groups confirmed the content validity of existing survey instruments, informed the use of local vocabulary regarding cervical cancer, perceptions about risk for cancer, and benefits versus barriers to screening, and identified preferences about types of interventions and methods of intervention delivery.
These qualitative data were used in conjunction with the health belief model (Rosenstock, 1974), the theory of planned behavior (Ajzen, 1991), social cognitive theory (Bandura, 1989), and the transtheoretical model (TTM; DiClemente & Prochaska, 1985) to develop a quantitative survey to provide additional information. The instrument was piloted with 50 women from the priority population and then administered in 500 door-to-door surveys of Hispanic women aged 18 to 70 years. We selected women for the survey by identifying block groups from the areas of El Paso where there was a high concentration of Hispanic women and income levels were low. We randomly selected 50 block groups and systematically approached households door-to-door until 10 eligible women from each block group completed a survey. Together, the findings from the literature, focus groups, and surveys provided detailed information about predisposing, enabling, and reinforcing factors associated with cervical cancer screening (Table 1).
Predisposing, Reinforcing, and Enabling Factors From Theories Used in the AMIGAS Surveys and Focus Groups
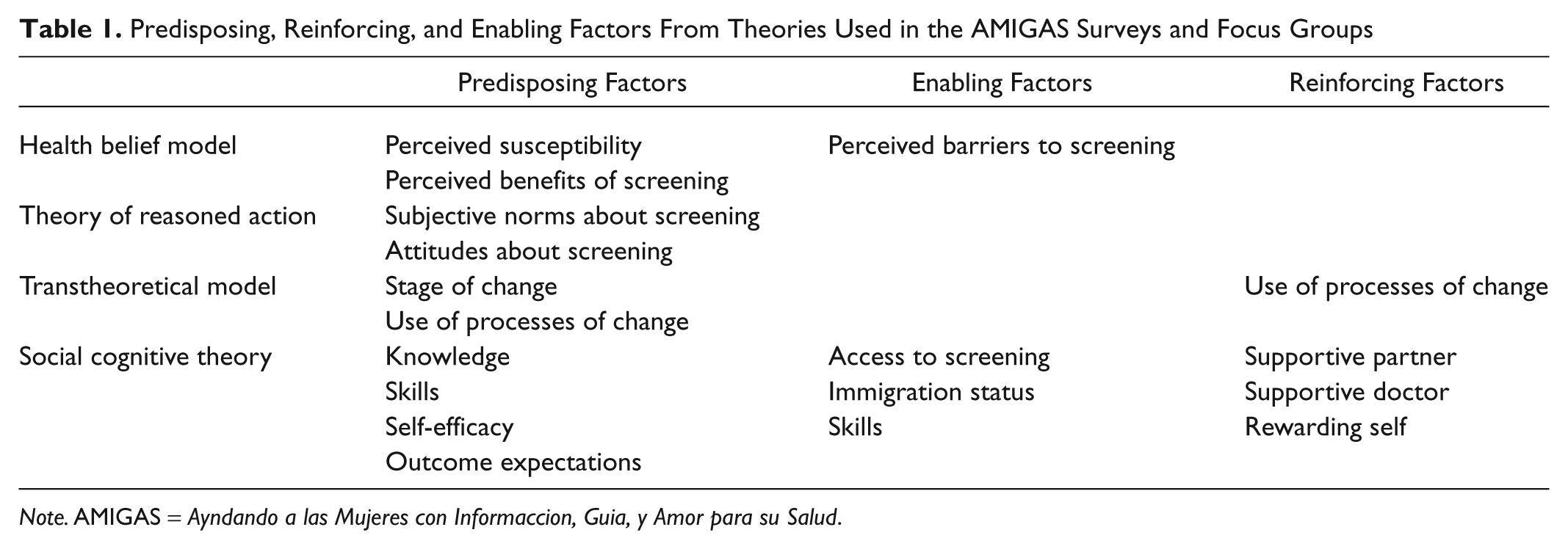
Note. AMIGAS = Ayndando a las Mujeres con Informaccion, Guia, y Amor para su Salud.
Creating Matrices of Program Objectives (Step 2)
The matrices created through the IM process clarified exactly who and what should change to meet the overall objective of the program, that is, “women aged 18 and over will have a Pap test at least every three years.” Developing the matrices is best done by a group, which in our case, included investigators, public health students, and members of our CAB. Matrices are created by crossing the performance objectives (what a woman has to do to get a Pap test; make an appointment, attend the appointment, etc.) with the determinants of these objectives. The resulting “change objectives” in each cell of the matrix are what guide program content, methods, and strategies. Change objectives are written to be specific, changeable, and either behavioral or environmental.
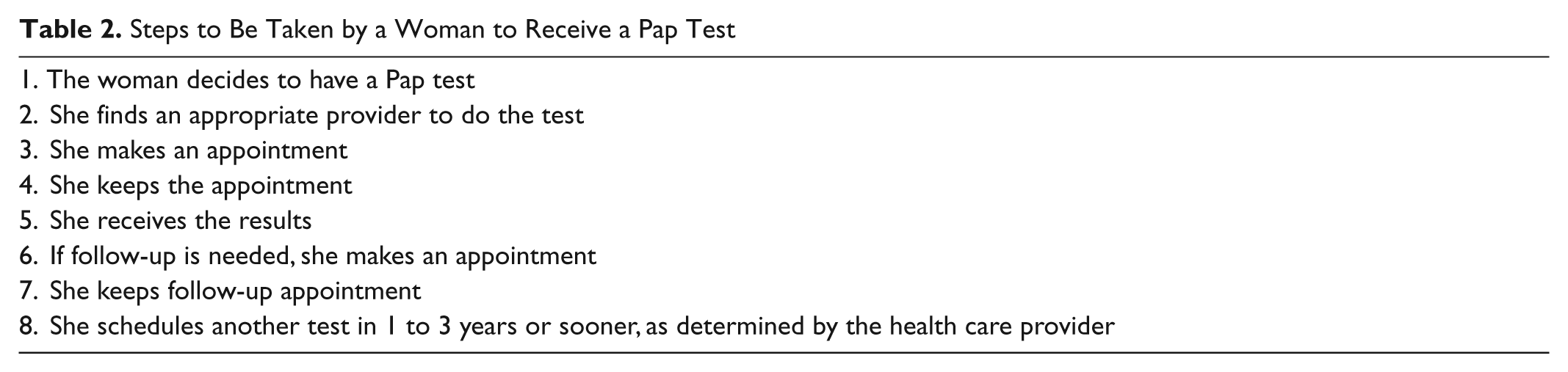
The first two behavioral objectives stated that women would get a Pap smear at least every 3 years and that they would begin screening at the age of 18 years or earlier if they were sexually active (based on the screening guidelines current at the time). We reviewed the matrices with the CAB and chose the theoretical methods corresponding to the determinants identified. The CAB provided input and made recommendations about what methods seemed most appropriate, feasible, and effective. The group discussed possible strategies and used the matrices to assure that the strategies matched the change objectives. Although the CAB looked to the researchers for expertise in behavioral science theory, the lay health workers and the members of the priority community acted as our cultural and linguistic experts, and all members of the CAB gave input into the acceptability of methods chosen. The CAB, in keeping with the recommended steps of IM, believed that it was important to break down the steps that needed to occur to achieve these objectives (Table 2).
Steps to Be Taken by a Woman to Receive a Pap Test
Personal determinants of the behavior change were drawn from the AMIGAS assessment, relevant literature, and the theoretical constructs applied when conceptualizing the assessment and included knowledge, skills, self-efficacy, outcome expectations, and attitudes. External determinants included reinforcement, social norms, and availability or accessibility. Table 3 shows selected cells from the final matrix as an example of how a performance objective relates to determinants. An additional matrix of environmental conditions was also created (not shown). The initial goal of the AMIGAS intervention was not to address environmental- and policy-level issues; however, the matrix of these factors allowed for future intervention development that might include environmental and political factors.
Sample Cells From Matrices for U.S. Women of Mexican Descent

Selecting Intervention Methods and Strategies (Step 3)
Successful interventions begin with behavioral change theory as a component of intervention development, but the methods suggested by theory must be operationalized as actual strategies. For example, one method suggested by theory would be observational learning, and the actual strategy might involve a video of a role model successfully doing a particular behavior. In IM, it is suggested that intended participants are involved in the development of program ideas so their perspectives are integrated into the methods and strategies. We reviewed the IM matrices with our CAB and chose the appropriate theoretical methods based on their input. Possible strategies to operationalize the theoretical methods were discussed, with final selection made by the researchers and the CAB using the matrices to assure that the strategies matched the change objectives (e.g., increasing self-efficacy). For example, it was clear from our survey data that a woman who had an outcome expectation that having a Pap test would make her feel she was doing something good for her family was more likely to have been screened. We operationalized this outcome expectation using a role model on the AMIGAS video, talking about how taking care of one’s health is like taking care of family and community. The construct of reinforcement was operationalized, as suggested by members of the CAB, by showing the young woman in the AMIGAS video preparing to reward herself after her Pap test by going to the mall and by showing the physician in the video congratulating the woman for taking care of her health.
Designing a Program (Step 4)
Step 4 of IM includes a description of the components of the intervention, completed program materials, and program protocols. These components of the intervention must be linked back to the previous steps, requiring a review of the IM matrices.
The CAB had many suggestions about the components of the intervention, how the intervention should be delivered, and whether the materials were culturally appropriate. For example, the idea for the video was approved by the CAB, and the Spanish translation was approved by the young women who became the actors in the video. When the video script was returned to the CAB for approval, they felt that some of the Spanish language was inappropriate for middle-aged women even though the words were commonly used in the community. These words and phrases were reworded so that they were appropriate for women in the priority population. The CAB also approved the decision to use local ‘real’ people in the video instead of actors.
Results
From the focus groups and quantitative surveys, we discovered that there were several predisposing, reinforcing, and enabling factors associated with ever having had a Pap test and with the TTM stage of change (precontemplation, contemplation, preparation, action, maintenance, or relapse) of the women regarding readiness to be screened. Predisposing factors that were associated with no screening (or nonadherence to regular screening) included embarrassment about the test, fear of finding out something might be wrong, discomfort associated with the Pap test, low perception of susceptibility to cervical cancer, and lack of knowledge about the test and the screening recommendations. Reinforcing factors included having an intimate partner that approves of having the test, having a doctor that reminds the woman about the test and encourages it, and knowing other women who get tested for cervical cancer. Enabling factors included low-cost screening, having a clinic available and accessible, being a U.S. resident, and having transportation and child care. Additionally, our findings suggested that messages should emphasize that receiving a Pap test may reduce worry and anxiety, and that finding cervical abnormalities in the early stages is more likely to result in successful treatment.
Table 4 describes the determinants, methods, and strategies that were chosen in the development of the intervention. The final intervention package included a video using actors from the community, a flip chart for use by the lay health worker to reinforce the video messages in a dialogue, a list of providers in the area with information about how to access health care services, a speculum and a cytobrush, a Pap test record card, and a lay health worker training manual. The video used modeling techniques and featured two young women, and the mother and grandmother of one of the young women. The video was developed to influence knowledge, skills, self-efficacy, outcome expectations, attitudes, reinforcement, and social norms. The intervention package also included an implementation guide for the lay health workers that outlined how to use the intervention materials.
AMIGAS Intervention Determinants, Methods and Strategies

Note. AMIGAS = Ayndando a las Mujeres con Informaccion, Guia, y Amor para su Salud.
Refinements to the AMIGAS program occurred from 2005 through 2007 to address changes in the screening guidelines and to assure that the intervention would be useful in different communities outside the U.S.–Mexico border region. Refinements were directed by the LHWAC and primarily involved the development of additional educational components. The LHWAC was an advisory group that was different from the CAB and that included lay health workers and clinic directors from Yakima, Washington, Hood River, Oregon, and San Diego, California. Message cards (based on a woman’s stage of change) were designed to allow a lay health worker to work one-on-one with women to understand and address barriers, feelings, beliefs, and experiences of the women. The message cards incorporated specific messages identified during the original focus groups about women’s feelings, beliefs, social support, and barriers/facilitators associated with Pap testing. Helpful messages (printed on the back of the cards) were created by the LHWAC to aid the lay health worker in addressing each of these issues. Group games were developed for use in group settings, building on similar messages and counter messages. To address lack of knowledge about Pap testing and cervical cancer, new materials were developed to complement earlier materials, including simpler and low-literacy body diagrams for posters or handouts, a promise sheet (“mi promesa”) to allow women to make a written commitment to screening, and a summary sheet for women to keep.
Initial testing and validation of the refined educational material and lesson plans were done through two half-day workshops with promotoras who work with women in the priority population. Each workshop began with a mock session led by a member of the LHWAC followed by a facilitated discussion of the materials. The first workshop was held in San Diego, California, in April 2007 with nine promotoras. The second workshop was held in Yakima, Washington, 2 months later with eight promotoras. All the promotoras were also members of the priority population. Both workshops were conducted in Spanish. Revisions were made to the materials after each workshop. To test the use of the materials in a one-on-one setting, members of the LHWAC conducted three pilot sessions; two in Spanish and one in English. The sessions were observed by the trainers. The promotoras were able to use the lesson plans as they had been trained to, and reported that supporting materials were clear and easy to use. Minor edits and clarifications to the instruction guide were made following the sessions.
The AMIGAS intervention is currently being evaluated in a randomized controlled trial in three diverse sites: El Paso and Houston, Texas and the Yakima Valley, Washington. Some members of the original CAB have continued to work with us to oversee the evaluation of the project.
Discussion
The continued involvement of the CAB was integral to developing an intervention that could be disseminated in geographically diverse settings. Although community members may not have a background in the theoretical constructs, we found that they are well able to understand the constructs if they are explained in lay terms. Following the IM process, CAB members assisted in the choice of methods and strategies, guided the development of the video and the flip chart, assessed the cultural appropriateness of the materials before they were finalized, and guided the format and packaging of the intervention to increase its acceptability to others in future dissemination activities. Their input was anchored in concerns for feasibility and sustainability of program implementation in resource-restricted organizations. While the current randomized controlled trial emphasizes the internal validity of the intervention findings, the novel integration of CBPR and IM aims to ensure that the intervention has not ignored external validity and is relevant to various populations, settings, and times. Furthermore, the use of IM in the context of CBPR enhanced the rigor of both evidence-based intervention development and practice-based evidence.
In addition, the CAB saw their role as “keeping the researchers honest,” thus assuring the community that we were working with them to solve a public health problem and not merely using the community as a research laboratory. Many of the original CAB members continue their involvement by assisting with recruitment of women for the current trial of the AMIGAS intervention and will assist in communicating the results of the trial to the community.
Systematic use of IM can help assure that the program is clearly described to permit replication, compatible with the priority population, and that dissemination issues are anticipated throughout (Kok et al., 2004). IM in the context of CBPR can set the stage for the efficacy and effectiveness of an intervention to be addressed simultaneously and make the resultant intervention ready for dissemination (Glasgow et al., 2003). IM lends itself to, and in fact encourages, the involvement of community members. From the early collection of qualitative and quantitative data, to the development of matrices and the selection of theoretical methods and intervention strategies, community members can be involved. This involvement of community members should lead to interventions that are culturally and linguistically appropriate, whereas the use of theory should increase the efficacy of interventions. In our case, the researchers had worked with the priority community for several years, and had a great deal of respect for the “in the trenches” knowledge of the members of the CAB. Because of previous work together, the CAB members were aware that the researchers saw them as equals in the process and there was a reciprocal respect for the expertise and perspectives of the CAB and the researchers.
IM clearly links intervention strategies to theoretical models and constructs. By identifying an intervention’s core strategies and components, we can provide guidance for future use of the intervention so as to maintain its efficacy while allowing for maximum local flexibility. By understanding what it takes to implement this intervention in the field, we can provide guidance to decision makers or managers in organizations who may find the intervention appealing. In addition, conditions are currently such that policy and environmental interventions could be developed to increase the impact of the AMIGAS intervention. Through use of IM, we have already assessed the environmental and policy determinants and are in a position to act on them in future interventions.
It is important to note that new innovations in reducing incidence of cervical cancer have been developed since the creation of AMIGAS. Although the development of the HPV vaccine and HPV DNA test have the potential to change the rates of cervical cancer dramatically, women will still need to be screened for cervical cancer, since about 30% of cervical cancers are not caused by the HPV types covered by the vaccine (Muñoz et al., 2003). For young girls being vaccinated today, we do not yet know for how many years the vaccine will provide protection. HPV DNA testing for primary cervical cancer screening has not been shown to be beneficial, and its role in cervical cancer detection is uncertain (Curry et al., 2003). However, future iterations of the AMIGAS intervention may need to be revised to include HPV vaccine and HPV DNA test information as knowledge evolves while continuing to emphasize the message that cervical cancer screening is important for all women.
Limitations
Ideally in CBPR, communities should be involved in every phase of the research process from deciding on the problem, developing the design of the research project, data collection and analysis and development of interventions, and in communicating findings to the community. We view CBPR as a continuum, with “true” CBPR at one end, in which the community is involved in and then ultimately owns the project, to the “usual way of doing business” at the other end, where the researchers maintain all of the decision-making power and control of the project. In many cases, as in the development of the AMIGAS intervention, the problem to be addressed was decided by the funding agency, based on sound epidemiologic data showing that cervical cancer and low screening rates were a problem in the Hispanic community. In our case, although the community was not involved directly in the choice of the problem to be addressed, or in the development of data collection instruments or collection and analysis of data, we were able to integrate many aspects of CBPR through the use of IM for intervention development. Once we decided that an intervention should be developed, we involved the CAB in the project. Given time and funding constraints, it is likely that this method will be used by many researchers in the future who want to make sure that at least some CBPR methods will be used in their work with communities. At later stages, when the AMIGAS intervention was being revised, the LHWAC had much more input and control and the lay health workers (who were also members of the priority community) were full contributors to, and often led, the process. In this project, the CAB was a volunteer body, but in future efforts we plan to include honoraria for the CAB in the research budget.
Conclusion
CBPR methods are recommended as a means of working collaboratively with communities in developing programs that will be considered appropriate, efficacious, and sustainable. IM is an intervention development method that lends itself to the inclusion of community members and that allows both researchers and lay collaborators to better understand how theoretical constructs can be used to develop methods and strategies for health education.
Footnotes
Acknowledgements
We wish to acknowledge the community members who participated in our work, especially the members of the Community Advisory Board and the promotoras for their invaluable contributions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
The contribution was supported in part by research funded by CDC Contract No. 200-2002-00573 Task Order No. 3. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.