
Abstract
This systematic review evaluates interventions using active video games (AVGs) to increase physical activity and summarizes laboratory studies quantifying intensity of AVG play among children and adults. Databases (Cochrane Library, PsychInfo, PubMed, SPORTDiscus, Web of Science) and forward citation and reference list searches were used to identify peer-reviewed journal articles in English through March 2011. Studies that used off-the-shelf AVGs to increase physical activity with quantitative outcomes or studies that quantified intensity of AVG play were included. Information on sample characteristics, AVGs employed, study design and conditions, outcome measures, results, and conclusions was extracted by two researchers. Intervention studies were ranked on design quality. Thirteen interventions and 28 laboratory studies were identified. All laboratory studies demonstrated that AVGs are capable of providing light-to-moderate intensity physical activity. However, only three interventions supported AVGs as an effective tool to significantly increase physical activity or exercise attendance. As AVGs are becoming more popular, additional research is needed to determine how to capitalize on the potential of AVGs to increase physical activity.
Keywords
Physical inactivity among adults and children is a major contributor to diseases associated with obesity (World Health Organization, 2010). The World Health Organization estimates that physical inactivity is associated with more than 2 million deaths each year, including 10% to 16% of cases of breast cancer, colon cancer, and diabetes as well as 22% of heart disease (World Health Organization, 2010). The Centers for Disease Control and Prevention recommends that adults participate in at least 150 minutes of moderate physical activity every week for disease prevention (Centers for Disease Control and Prevention, 2008a). However, incorporating physical activity into a daily routine is difficult for many children and adults. Recent estimates suggest that U.S. individuals aged 6 years and older spend approximately 55% of the day engaged in sedentary behaviors (Matthews et al., 2008); 25% of Americans do not participate in any leisure-time physical activity (Centers for Disease Control and Prevention, 2008b).
Many formalized attempts have been made to encourage people to be more physically active. These interventions have become technologically sophisticated, using the multimedia capability of websites (Goran & Reynolds, 2005; Marshall, Leslie, Bauman, Marcus, & Owen, 2003) and tailored e-mail messages (Hageman, Walker, & Pullen, 2005). More recently, a new form of interactive gaming (termed as exergaming or active video gaming) has emerged, and researchers have begun examining whether these potentially more fun and engaging platforms are equivalent to moderate to vigorous physical activity (MVPA) or have the potential to promote healthy active behaviors. In this systematic review, we adopt the term active video games (AVGs) to refer to commercially available off-the-shelf video games that require players’ body movements for game play.
Objective
A number of reviews of intervention studies and laboratory energy expenditure studies of AVGs have been published recently (Biddiss & Irwin, 2010; Daley, 2009). However, the most recent systematic review (Biddiss & Irwin, 2010) only focuses on children. As more than half of American adults play games (Lenhart, Jones, & Macgill, 2008), and 29% of Americans older than50 years play video games (Entertainment Software Association, 2011), and nearly a third of adults older than 65 years play games daily (Lenhart et al., 2008), it also is important to review the current literature on the potential of using AVGs for physical activity promotion among adults and older adults. This review will include two different types of studies. The first type is the laboratory study that quantifies the intensity of AVG play to establish whether an AVG is capable of providing the intensity of physical activity recommended. The second type is the intervention study that uses an AVG to increase physical activity. Therefore, the objectives of this review are (a) to systematically summarize laboratory studies that validate the intensity of AVGs as a physical activity promotion tool among children (younger than 18 years) and adults (18 years and older) and (b) to systematically evaluate the effectiveness of intervention studies using AVGs to increase physical activity among children and adults.
Method
Data Source
To ensure a comprehensive inclusion of relevant studies, two waves of literature searches were conducted. The first wave covered literature published between January 1995 to October 2010, and the second wave covered literature published between October 2010 and March 2011. In each wave, three search strategies were adopted. First, two researchers conducted systematic literature searches using five databases (Cochrane Library, PsychInfo, PubMed, SPORTDiscus, and Web of Science) for articles from English language, peer-reviewed publications using the following two groups of keywords in combination: “physical activit*, exercise, weight loss, obesity, motor activit*, leisure activit*, physical fitness, physical education, physical training, sports” and “video game, computer game, active video game, and exergame.” Two researchers screened the search record by evaluating the titles and the abstracts using the inclusion and exclusion criteria. The screening resulted in 69 articles in Wave 1 and 22 articles in Wave 2. The full-text of these 91 articles was obtained. Further evaluation of the full-text using the inclusion and exclusion criteria resulted in 40 articles. The second search strategy was a forward citation search conducted in the Social Science Citation Index using the included articles. No additional articles were found. The third search strategy was a reference list search of the included articles and one additional article was identified. In total, 41 articles were included in this systematic review.
Study Inclusion and Exclusion Criteria
First, the study must have employed at least one off-the-shelf AVG. Research on off-the-shelf AVG arcade games that are not intended for home use was not included (Ridley & Olds, 2001). Non-off-the-shelf AVG or virtual reality–based computer games were not included. Second, the AVG was either used as a tool to increase the amount of physical activity or was quantified in terms of AVG intensity. Studies that used AVGs for other purposes such as depression (Rosenberg et al., 2010), attention and memory (Russell, 2009), physical fitness (Lotan, Yalon-Chamovitz, & Weiss, 2010), balance (Studenski, Perera, Keller, Spadola-Bogard, & Garcia, 2010), or obesity treatment (Murphy et al., 2009; Radon et al., 2011) were excluded. Third, only studies with objective outcome measures were included. Studies with only qualitative outcomes such as focus group studies or studies with only physical activity–related psychological outcomes (e.g., preference of AVG; Epstein, Beecher, Graf, & Roemmich, 2007) but no quantitative physical activity outcomes were excluded. Fourth, conference proceedings, posters, and abstracts were not included. Fifth, literature review or commentary articles were not included. Sixth, studies that were conducted with physical rehabilitation patients were not included.
Data Extraction
Each of the eligible studies was categorized as a laboratory study, in which intensity of playing AVGs was quantified, or an intervention study, in which AVGs were used in an attempt to increase physical activity either at home or in a clinical or professional setting. Two researchers examined the included articles and extracted data including (a) methodological details (e.g., sample characteristics, study design, outcome measures); (b) types of AVGs used; (c) key findings pertaining to activity intensity, for example, metabolic equivalent (MET), 1 change in sedentary behavior and physical activity pattern, body mass index (BMI), and the potential for physical activity promotion (e.g., adherence, motivation for play, enjoyment, rating of perceived exertion), and gender difference; and (d) conclusion.
Data Synthesis
The laboratory studies were ranked by the intensity of the AVG (Table 1). The ranking index includes five levels: (a) L indicates that the METs among all the AVGs tested equal to light intensity physical activity (1.5-2.9 METs), (b) M indicates that all the AVGs tested equal to moderate intensity physical activity (3-6 METs), (c) LM indicates that some of the AVGs tested equal to moderate intensity physical activity (3-6 METs) and some equal to light intensity physical activity (1.5-3 METs), (d) MV indicates some of the AVGs tested equal to moderate intensity physical activity (3-6 METs) and some equal to vigorous intensity physical activity (>6 METs), and (e) LMV indicates that the AVGs tested include light, moderate, and vigorous intensity levels.
Sample Size and Active Video Game Intensity in Laboratory Studies
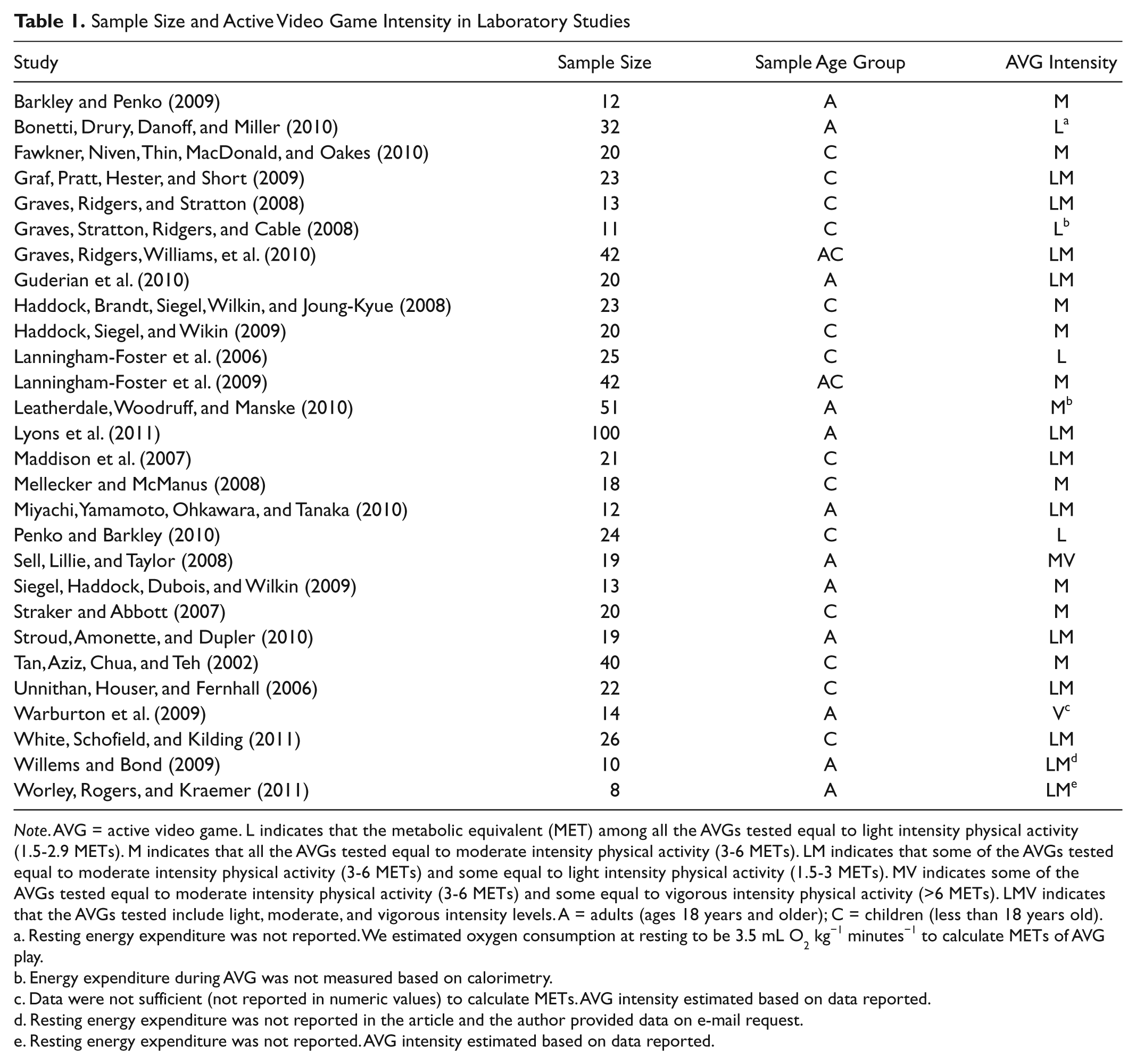
Note. AVG = active video game. L indicates that the metabolic equivalent (MET) among all the AVGs tested equal to light intensity physical activity (1.5-2.9 METs). M indicates that all the AVGs tested equal to moderate intensity physical activity (3-6 METs). LM indicates that some of the AVGs tested equal to moderate intensity physical activity (3-6 METs) and some equal to light intensity physical activity (1.5-3 METs). MV indicates some of the AVGs tested equal to moderate intensity physical activity (3-6 METs) and some equal to vigorous intensity physical activity (>6 METs). LMV indicates that the AVGs tested include light, moderate, and vigorous intensity levels. A = adults (ages 18 years and older); C = children (less than 18 years old).
Resting energy expenditure was not reported. We estimated oxygen consumption at resting to be 3.5 mL O2 kg−1 minutes−1 to calculate METs of AVG play.
Energy expenditure during AVG was not measured based on calorimetry.
Data were not sufficient (not reported in numeric values) to calculate METs. AVG intensity estimated based on data reported.
Resting energy expenditure was not reported in the article and the author provided data on e-mail request.
Resting energy expenditure was not reported. AVG intensity estimated based on data reported.
The intervention studies were ranked by whether the AVG was found to increase physical activity (Table 2). The ranking index has four levels: (a) + indicates that the AVG treatment was more effective than the no treatment control group in increasing the amount of physical activity, exercise attendance, or energy expenditure in the exercise sessions; (b) 0 indicates that the AVG treatment was not significantly different from the no treatment control group in increasing physical activity; (c) I indicates indeterminate results due to lack of control group or lack of non-AVG comparison group; and (d) − indicates that the comparison group resulted in greater physical activity attendance rate than the AVG treatment group.
Sample Size, Active Video Game Effectiveness, and Study Design Quality Score
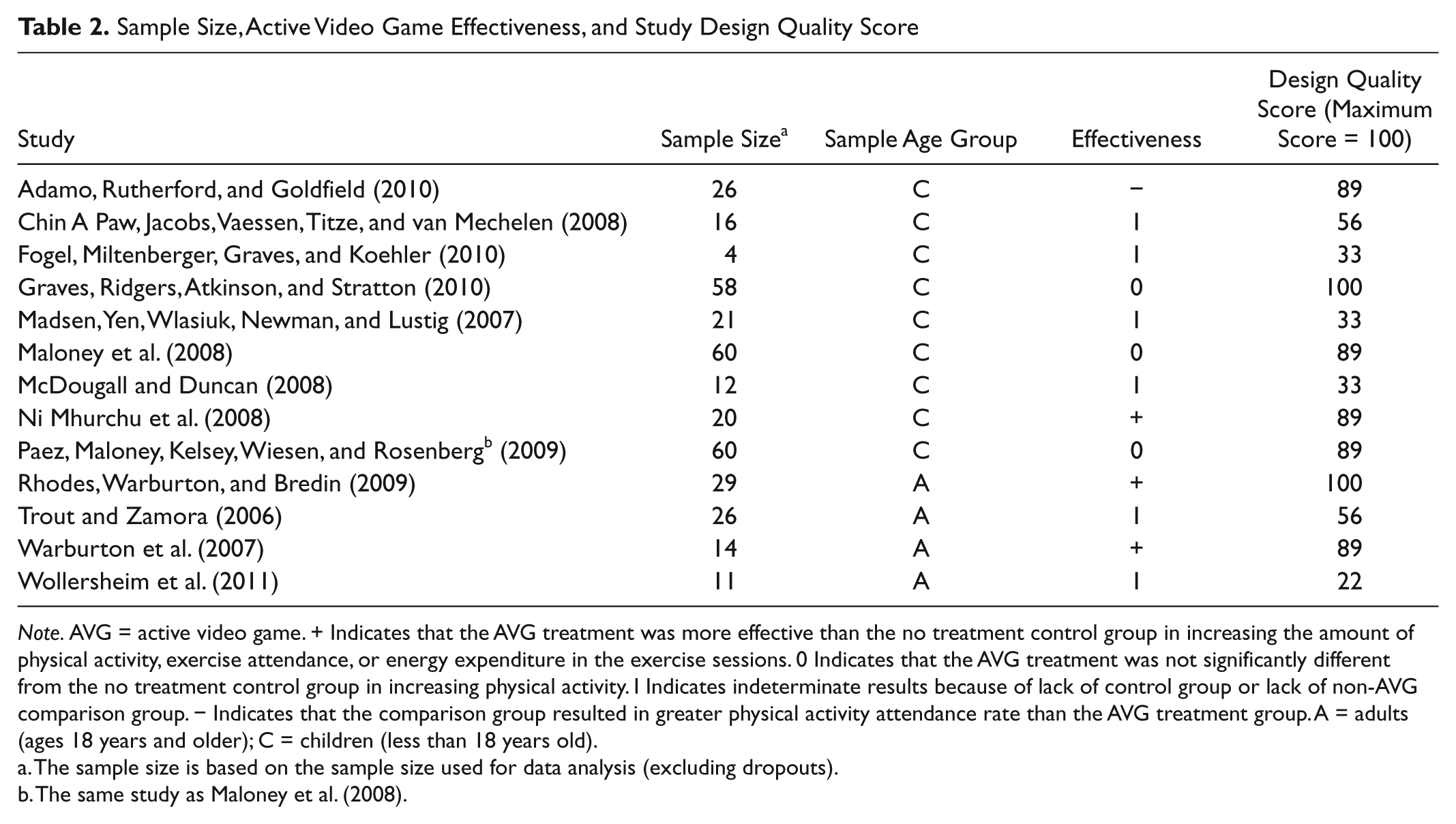
Note. AVG = active video game. + Indicates that the AVG treatment was more effective than the no treatment control group in increasing the amount of physical activity, exercise attendance, or energy expenditure in the exercise sessions. 0 Indicates that the AVG treatment was not significantly different from the no treatment control group in increasing physical activity. I Indicates indeterminate results because of lack of control group or lack of non-AVG comparison group. − Indicates that the comparison group resulted in greater physical activity attendance rate than the AVG treatment group. A = adults (ages 18 years and older); C = children (less than 18 years old).
The sample size is based on the sample size used for data analysis (excluding dropouts).
The same study as Maloney et al. (2008).
Following previous literature (Norman et al., 2007), the design quality of the intervention studies were rated based on nine methodological characteristics: randomization, use of a control group, isolation of the AVG, pre–post test design, participant retention, baseline groups equivalence, use of missing data, analysis of power or effect size, and use of validated measures (Tables 3 and 4). Each study’s score was calculated as the percentage of the maximum obtainable score. Three researchers independently checked the scores for accuracy.
Design Quality Scoring Criteria for Intervention Studies
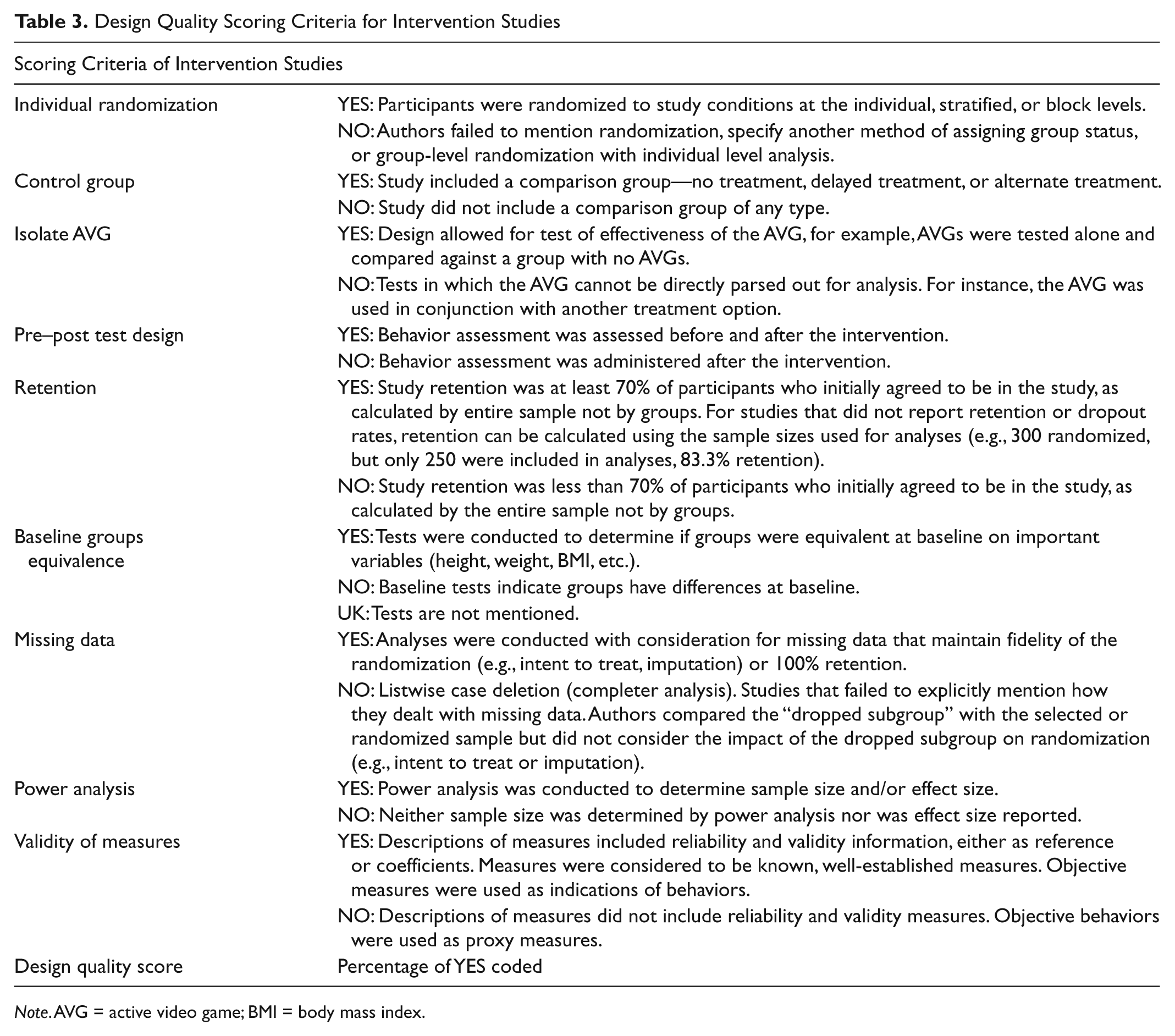
Note. AVG = active video game; BMI = body mass index.
Design Quality Analysis of Intervention Studies

Note. AVG = active video game.
Results
This systematic review included 41 articles that were classified into two categories: 28 laboratory studies quantifying intensity of AVG play (Table 5) and 13 AVG-based physical activity intervention studies (Table 6).
Summary of Laboratory Study Characteristics

Note. BS = between-subjects design; CB = conditions counterbalanced; F = number of female participants; M = number of male participants; MD = mixed design; N = Sample size, PR-PT = pretest to posttest design (resting/sedentary activity is treated as pretest); PT = posttest only; RO = conditions in random order; WS = within-subjects design; NA = not applicable; MET = metabolic equivalent.
Summary of Intervention Study Characteristics
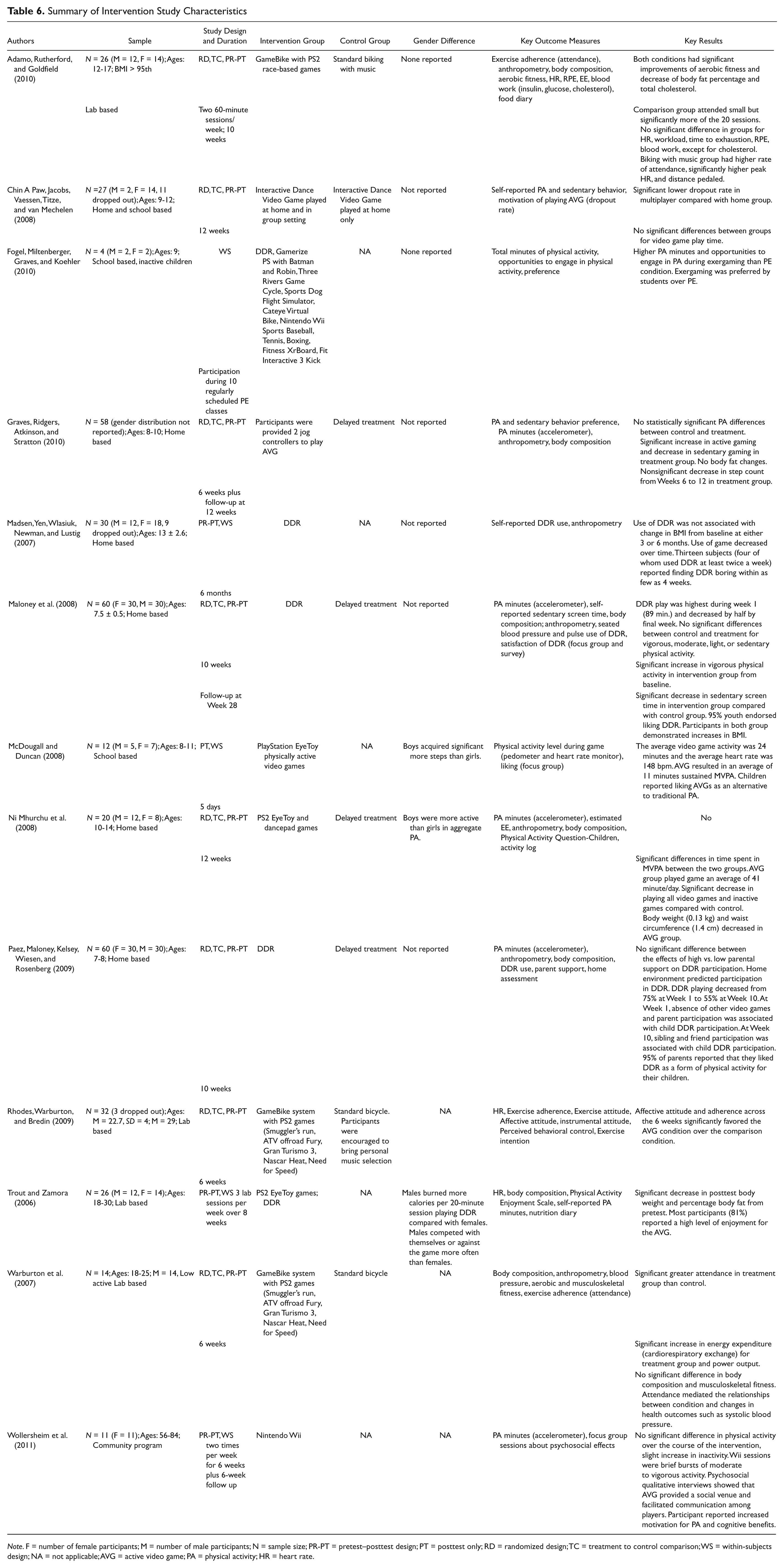
Note. F = number of female participants; M = number of male participants; N = sample size; PR-PT = pretest–posttest design; PT = posttest only; RD = randomized design; TC = treatment to control comparison; WS = within-subjects design; NA = not applicable; AVG = active video game; PA = physical activity; HR = heart rate.
Laboratory Studies
Of the 28 laboratory studies, sample sizes ranged from 8 to 100 participants. Eleven of the studies included adult samples, 2 used both children and adults, and 15 were aimed at children. All but 5 of the studies used both male and female participants. Five studies examined single gender sample. Most of the laboratory studies consisted of multiple conditions for each participant to play various types of AVGs (5-10 minutes on each game). All but two studies (Graves, Stratton, Ridgers, & Cable, 2008; Leatherdale, Woodruff, & Manske, 2010) used noncalorimetric methods to estimate AVG intensity and energy expenditure. Five studies measured participants’ liking or enjoyment of AVGs. Eleven studies also measured participants’ perceived exertion of playing AVGs. In the order of most to least common, in general the conditions included AVG play, sedentary game play, and a traditional physical activity, such as walking on a treadmill. The most commonly used AVGs were associated with the Nintendo Wii console and the Wii Balance Board (e.g., Wii Sports, Wii Fit), followed by dance pad–based games (e.g., Dance Dance Revolution [DDR], Zigzag Xer-Dance) and games for the PlayStation2 EyeToy. Other AVG systems included Exerstation, a full-body isometric game controller for the Xbox 360, GameBike, and the XaviX system.
Among the 28 studies testing the intensity and energy expenditure of AVG play, two studies (Sell et al., 2008; Warburton et al., 2009) found that some of the AVGs included in the studies equal to vigorous physical activity. Ten studies found that all the AVGs tested equal to moderate physical activity. Twelve studies found that the AVGs tested equal to light-to-moderate physical activity. Four studies found that the AVGs employed equal to light-intensity physical activity (Bonetti, Drury, Danoff, & Miller, 2010; Graves et al., 2008, Lanningham-Foster et al., 2006; Penko & Barkley, 2010). Eighteen studies reported gender differences, with nine finding significant differences between males and females on at least one of the dependent variables. Five studies recruited single gender sample, and the remaining five studies did not report whether gender difference was examined.
Intervention Studies
The duration of the intervention studies ranged from 5 days to 6 months. Most of the studies took place between 6 and 12 weeks and included a follow-up after the treatment was concluded. Four studies used adult participants, whereas 9 were aimed at children. One study involved female-only participants, 1 study involved male-only participants, and the rest of the 11 studies used both genders. Five of the intervention studies were based out of the home, 4 out of a laboratory, 2 based at school, 1 based at both home and school, and 1 out of a community program. Five studies used accelerometers to objectively measure physical activity. Most of the studies also recorded BMI and heart rate. However, only two studies tested for estimated energy expenditure during AVG play. The most commonly used AVGs were dance pad–based games, such as DDR, followed by games involving the PlayStation 2 EyeToy. Other AVGs included games played on the Wii console (e.g., Wii Sports) and the GameBike system.
Among the 13 intervention studies, 8 employed randomized control trials (Table 3). Samples sizes ranged from 12 to 60 participants. The design quality of the studies ranged from a score of 22 to 100, with a mean score of 68. Two thirds of the studies explained how they dealt with missing data or did not have missing data. Three studies conducted power analysis for sample size calculation. Two studies failed to retain at least 70% of the participants.
Three studies found that the AVG treatment was more effective than the control group or the comparison group in increasing the amount of physical activity or exercise attendance. Three studies found no difference between the AVG intervention and the control group. One study found that the AVG treatment was worse than the comparison condition in influencing exercise attendance and energy expenditure during exercise. Six studies had indeterminate results, indicating that the study design was not adequate to demonstrate whether the AVG intervention was effective due to lack of a control group or non-AVG comparison group.
Discussion
The goal of this systematic review was to provide a comprehensive synthesis of the current state of knowledge pertaining to the potentials of AVGs for physical activity promotion for both children and adults. Forty-one studies published between 2002 and 2011were included in this review, adding 18 laboratory studies and 7 intervention studies that were not included in Biddiss and Irwin (2010). The discussion section is organized by the summary of findings and implications of laboratory studies and intervention studies for two age groups: children and adults. Limitations are also discussed.
AVG Intensity
This review included 28 laboratory studies quantifying intensity and energy expenditure of AVGs among healthy children and adults, which adds substantially more studies to the summary of 12 such studies in Biddiss and Irwin (2010). All the lab studies that compared enjoyment of AVGs and other traditional exercise activities found that AVGs were better liked than traditional exercises, such as treadmill walking or jogging (Barkley & Penko, 2009; Graves, Ridgers, Williams, et al., 2010; Penko & Barkley, Sell et al., 2008).
Children
This review added seven studies on AVG intensity and energy expenditure among children that were not included in Biddiss and Irwin (2010). These seven studies provide a consistent finding that playing AVGs generally is equivalent to light-to-moderate physical activity among children. In addition, children rated the perceived exertion of playing AVGs to be similar to activities with lower intensity (Haddock, Siegel, & Wikin, 2009). In other words, AVG play demands physical exertion from the players yet they are so engaged in the games that they are not aware of the physical exertion. This suggests that AVG may be a good starting point to engage sedentary children to a more active lifestyle by overcoming one of the most significant barriers of physical activity—fatigue. However, it needs to be noted that only relying on AVGs as a tool for physical activity among children is not enough since the light-to-moderate intensity of AVG play does not meet the daily 60-minute MVPA goal for children.
Adults
This review provides the first systematic summary of intensity of AVG play among adults, which reveals similar results as in the children sample. The intensity of AVG play among adults was light to moderate. Adults rated the perceived exertion of AVG play to be similar to activities with higher metabolic requirement (Warburton et al., 2009), suggesting that AVGs also are a good tool to involve physical inactive adults to start a more active lifestyle. In particular, two studies also examined AVG play among older adults (Graves, Ridgers, Wiiliams, et al., 2010; Guderian et al., 2010). Not surprisingly, energy expenditure of AVG play among older adults was found to be less than children and young adults. In fact, older adults enjoyed the lower intensity AVGs such as Wii Fit more than their younger counterparts (Graves, Ridgers, Williams, et al., 2010). Seniors’ rating of the perceived exertion of an AVG (Wii Fit) was relatively low (Guderian et al., 2010). Overall, the light-to-moderate intensity of AVGs suites the recommended physical activity for the older adults, making them a more suitable tool of physical activity for the older adults than for children.
AVG Physical Activity Interventions
Thirteen intervention studies that used AVGs to promote physical activity among nonrehabilitative individuals were systematically reviewed. Overall, only three studies demonstrated that playing AVGs resulted in increased physical activity compared with the control group or the comparison group. Among these 13 studies, only six overlapped with Biddiss and Irwin’s (2010) systematic review of AVGs to promote physical activity in children.
Children
Only one study with children found that the AVG was effective in increasing physical activity. Among the nine AVG-based interventions with children, four studies reported the participants’ attitudes toward AVG, and one reported the parents’ attitudes. Three studies reported that the children liked the AVG (Fogel Miltenberger, Graves, & Koehler, 2010; Maloney et al., 2008; McDougall & Duncan, 2008), and one study reported that most children found the AVG boring within 4 weeks (Madsen, Yen, Wlasiuk, Newman, & Lustig, 2007). More than 90% of parents liked AVG as a form of physical activity for their children. Overall, the nine AVG intervention studies with children demonstrated that usage of AVGs was low after the initial period. This implied that although studies found that AVGs are typically liked or enjoyed more than traditional exercise (Barkley & Penko, 2009; Graves, Ridgers, Williams, et al., 2010; Penko & Barkley, 2010; Sell, Lillie, & Taylor, 2008) in a short lab session, relying solely on self-directed use of an AVG over time might decrease the success of such interventions. It has been suggested that deploying AVGs in a group setting and incorporating multiplayer mode may contribute to sustained usage of an AVG (Daley, 2009; Russell, 2009). Additionally, rather than using one game, multiple games, especially games with story and plot development (Baranowski et al., 2011), might be needed for sustainability.
Only one study (Adamo, Rutherford, & Goldfield, 2010) specifically targeted overweight and obese children, employing the GameBike system. Unlike the studies with adults that found GameBike increased exercise adherence compared with standard biking training or biking training with music, this study found that biking with music was found to be more effective than GameBike (biking with video game play) in exercise adherence and time spent in vigorous intensity and distance among overweight children. Nevertheless, both biking with music and biking with video game play improved physical fitness similarly. Two studies using AVGs for overweight and obese children (Murphy et al., 2009; Radon et al., 2011) were not included in the systematic review because of their lack of physical activity measures (physical fitness and weight reduction were the main focus of these two studies). Although Murphy and her colleges (Murphy et al., 2009) found that the AVG improved aerobic fitness and other health-related outcomes among overweight adolescents compared with the delayed control group, Radon et al. (2011) found that obese children in a clinical setting had low interest in the devices when they were offered the options to freely choose to play AVGs. Thus, the suitability of using AVGs for weight reduction for adolescents cannot be ensured. The intervention protocol of Murphy et al. (2009) was not described in detail; therefore, it is unknown whether the AVG treatment was administered at home in a self-directed manner or in a lab with a structured program. However, the overall findings of this systematic review suggest that although AVGs have the potential to engage and motivate inactive individuals, especially those who log a significant portion of sedentary time in screens (e.g., video game play), relying on AVG alone for weight loss is not realistic, especially if AVGs are not used in a structured program but are only offered to the participants for self-directed use. Although active video gaming is generally considered as a nonprogrammed physical activity, researchers should study whether using these AVGs in a more structured manner may increase the usage.
Adults
This review provides the first systematic summary of evidence regarding the potential of AVGs for physical activity promotion among adults. Adults had positive attitude toward AVGs and found AVGs to be enjoyable (Rhodes, Warburton, & Bredin, 2009; Trout & Zamora, 2006; Wollersheim et al., 2011). Only two interventions targeting adults employed the design of randomized controlled trial, and both studies demonstrated that AVG increased physical activity attendance. In fact, both studies employed the GameBike system. The GameBike requires the player to pedal and steer on a stationary bike to control the gameplay (e.g., car racing). Unlike the Wii system in which the body movement is completely self-directed, allowing the players to exploit energy saving strategies while playing games, the GameBike has resistance settings to ensure the energy expenditure for MVPA. It seems that the GameBike has the potential to be used in a more structured physical activity promotion program for adults, capitalizing on the motivating power of video game play.
Only one intervention study involved older adults. The finding suggests that although older adults perceived an improved sense of physical, social, and psychological well-being from playing Wii, the overall physical activity level did not change from baseline after the introduction of Wii. The lack of change may be explained that only two participants played the games standing up. All the other participants chose to play the games sitting down, either because of a lack of physical mobility or as a result of peer influence. Two participants even dropped out because of embarrassment about using the Wii. This finding suggests that researchers need to consider the setting of an AVG-based intervention for the target population, especially for special groups such as older adults and the obese and overweight population.
Implications
When introducing AVGs as a tool to increase physical activity, the following precautions need to be taken. First, AVGs are not a replacement of MVPA, especially authentic physical activities or sports. Although most of the studies demonstrated that all the AVGs tested are equivalent to moderate intensity physical activity, most of them just surpass the minimal threshold of 3 METs. However, such intensity of AVGs makes them good tools for physical activity promotion for special groups, such as older adults or patients in physical rehabilitation. In fact, one study has demonstrated the potential of using AVGs to increase physical activity among adolescents with spina bifida (Widman, McDonald, & Abresch, 2006).
Second, different types of AVGs are equipped with different hardware. Some are upper body movement focused, such as the games played on the Wii console; some are lower body movement focused, such as the games played on the dance pad or the Wii balance board; and some involve both the upper and the lower bodies, such as the games played on the PlayStation2 EyeToy and the GameBike. Overall, playing AVGs focusing on the lower body and the whole body has more energy expenditure than AVGs focusing on the upper body (Peng, Lin, & Crouse, 2011). Yet it is not always true that the AVG that has the greatest intensity and produces the greatest energy expenditure is always the best choice for all the populations. Those high-intensity AVGs usually require greater video game skills and increased levels of physical fitness to start with. One study (Lyons et al., 2011) found that AVGs with greater energy expenditure were perceived by adults to be less enjoyable than AVGs with less energy expenditure. It seems that starting an intervention program using high-intensity games for obese and inactive participants may not ensure high attendance and engagement.
Third, for different populations, the AVG may also have different impacts. For instance, one study (Lanningham-Foster et al., 2009) found that AVG play can count as moderate physical activity for children but can only count as light physical activity for adults. Gender difference was also found in 10 included studies, generally favoring the use of AVG play for males. Additionally, energy expenditure was found to be greater among experienced players than inexperienced players (Sell et al., 2008). Overweight participants were also found to enjoy AVGs more than nonoverweight participants (Lyons et al., 2011). Therefore, when considering employing AVGs for physical activity interventions, the characteristics of the target population need to be considered.
Fourth, it also remains unknown whether energy expenditure would be different in different settings (e.g., free play at home with friends and family; competitive play in a group setting). It would be interesting to examine whether energy expenditure would increase when individuals play in a multiplayer or competitive way. On the other hand, when the players are too eager to win, they may adopt energy saving strategies to win the game without much energy expenditure (e.g., shaking the wrist to play Wii Tennis). In addition, the group-based AVG intervention may encourage participation for children, yet it may discourage participation for individuals who are embarrassed to exercise in front of other people such as older adults or overweight or obese individuals. Only one study (Bonetti et al., 2010) included in the review investigated playing against another player and found no difference of energy expenditure compared with solo play. Furthermore, although the energy expenditure of playing AVG in the laboratory demonstrated that AVG play is equivalent to light-to-moderate physical activity, energy intake during AVG play is an important issue to consider, particularly in the nonlaboratory setting, which is usually the case in the natural game play setting at home with friends and family. In fact, one study (Mellecker, Lanningham-Foster, Levine, & McManus, 2010) found that the participants consumed 383 cal/h of food during AVG play.
Limitations
This review highlighted some limitations of current research in AVG-based physical activity interventions. First, only one intervention study (Rhodes et al., 2009) specified a theoretical rationale (theory of planned behavior). However, research has shown that physical activity interventions designed and measured using behavioral theories are more likely to be successful. In fact, the AVGs in this review included only those available off-the-shelf and are not designed with the purpose to increase physical activity. As an increasing number of studies have begun to develop active games that are built for specific purposes but unavailable commercially (Betker, Desai, Nett, Kapadia, & Szturm, 2007; Housman, Scott, & Reinkensmeyer, 2009; Peng, Winn, Pfeiffer, Crouse, & Lin, 2010). More research is needed to study how health promotion practitioners, researchers, and game designers can work together to take advantage of the active platform of video gaming and specifically design physical activity promotion games. With guidance from health behavior change theories, it is reasonable to assume that active games specifically designed to promote physical activity may be more suitable to be used in physical activity interventions than the off-the-shelf AVGs. Second, the sample sizes of all the included studies were very small, limiting adequate power of these research studies. Third, 6 of the 13 intervention studies did not provide an adequate design to test for effectiveness of the AVG intervention because of lack of a control group without AVG treatment.
In conclusion, the current research shows that AVGs are capable of providing light-to-modest physical activity for both children and adults. However, little support is found regarding the long-term efficacy of using AVGs in nonstructured and self-managed manner for physical activity promotion. It seems that it is more promising to employ AVG in structured exercise programs in a group, given that the target population is comfortable exercising in a group setting. In addition, specifically designed physical activity promotion AVGs guided by behavior change theories are needed.
Although AVGs are not new conceptually (Sinclair, Hingston, & Masek, 2007), the use of such games that provide physical activity in daily life is just beginning to be evaluated. Since 2006 when Nintendo debuted the Wii—a home video game console system with a controller that requires physical activity for many of its games—the at-home AVG options have significantly increased. Recently, Microsoft and Sony released active play accessories to the Xbox 360 (Kinect) and PlayStation 3 (Move), respectively. This means that the three most popular video game systems have AVG options for people to play at home. It stands to reason that these too will be used in physical activity interventions. Additionally, mobile smart phones, tablet computers, and other portable gaming devices are emerging as possible AVG platforms. Besides their portability, these platforms also offer functions such as geospatial location tracking, pedometers, location-based knowledge presentation, and many other technologically sophisticated features that will make AVGs increasingly accessible and easily incorporated into daily life.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This research was supported by a grant from the Robert Wood Johnson Foundation’s Pioneer Portfolio through its national program, Health Games Research.