
Abstract
Objective. To examine gender differences in the association between beliefs in heart disease preventability and 10-year incidence of coronary heart disease (CHD) in a population-based sample. Methods. A total of 2,688 Noninstitutionalized Nova Scotians without prior CHD enrolled in the Nova Scotia Health Study (NSHS95) and were followed for 10 years. Risk factors, health behaviors, and incident CHD were assessed. Participants responded “yes” or “no” to a question about heart disease preventability. Survival models, adjusted for age, income, total and high-density lipoprotein cholesterol, and systolic blood pressure, were used to estimate the relation between health belief and incident CHD. Gender differences in the relation between health beliefs and health behaviors were assessed. Results. Gender was a significant moderator of the relation between belief and CHD incidence; specifically, women who believed heart disease could be prevented were less likely to have incident CHD events compared with women who believed heart disease could not be prevented (hazard ratio [HR] = 0.36, 95% confidence interval [CI] = 0.24-0.55, p < .001). This relation was not found for men. Belief was also related to smoking behavior for women (β = −0.70, odds ratio [OR] = 0.50, 95% CI = 0.33-0.74, p = .001) but not for men. Smoking significantly mediated the relation between health beliefs and incident CHD for women (z = −1.96, p = .05), but not for men. Conclusion. Health belief in prevention and subsequent smoking was an important independent predictor of incident CHD in women but not in men.
Coronary heart disease (CHD) is the leading cause of death among women and men in the United States, accounting for about 1 of every 5 deaths (Lloyd-Jones et al., 2010). It is well documented that certain health behaviors and lifestyle choices, such as smoking, eating high-fat foods, lack of exercise, and exposure to stress, influence the development of CHD (Yusuf et al., 2004). However, previous studies have also shown that knowledge about CHD risk factors correlates only weakly with participation in physical activity and maintenance of a healthy diet, and it does not have a significant influence on smoking cessation or adherence to blood pressure and cholesterol-lowering treatments (Alm-Roijer, Stagmo, Uden, & Erhardt, 2004).
There are a number of prominent theories concerning people’s tendency to engage in positive health behaviors. These include the health belief model (Becker, 1974), protection motivation theory (Rogers, 1975), theory of reasoned action (Ajzen & Fishbein, 1977), social learning theory (Bandura, 1986) and the theory of planned behavior (Ajzen & Madden, 1986), with each theory highlighting a particular determinant of health behavior such as motivation, behavior enactment, or multistage processes (Armitage & Conner, 2000). Although these theories concern a range of different predictors of health behaviors, none take into account people’s fundamental belief in preventability of disease as a factor in motivation or behavior change. Although much of the current literature discusses risk perception (Byrne, Walsh, & Murphy, 2005; DiMatteo, Haskard, & Williams, 2007; Hay, Coups, & Ford, 2006), overall belief in disease preventability may also be a determinant of health behaviors and as such may inform our ability to conduct health education and prevention strategies.
This study was guided by the health belief model, and specifically examined whether people’s perceived preventability of disease would affect their preventive health behaviors and their health outcomes. The original health belief model proposed by Becker (1974) suggested that some people use preventative health behaviors to avoid disease whereas others do not, depending on their perceived threat of disease, their perceived susceptibility, their perceived severity of disease, and their perceived benefits of health-seeking action countered against the inherent barrier (Figure 1). Although the health belief model does not directly include perceived preventability of disease in its conceptual framework, we chose this model as we viewed beliefs in prevention to be proxies for beliefs about susceptibility and threat and as having the same fundamental relation to behavior and outcomes. Other models do not contain constructs for which prevention beliefs could serve as a reasonable proxy.
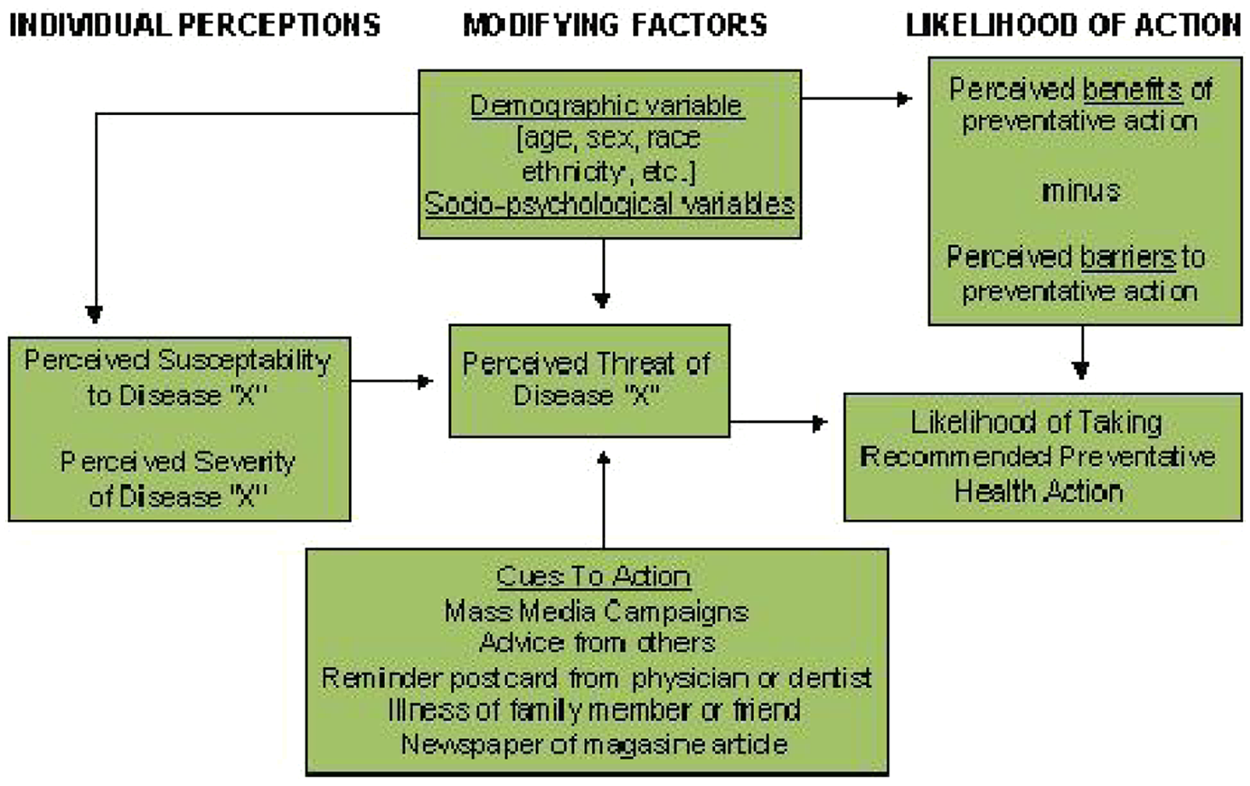
Becker’s health belief model
Research generated by the health belief model has often found that women behave more consistently in relation to their health attitudes and beliefs than do men (Armitage, Norman, & Conner, 2002; Courtenay, Mccreary, & Merighi, 2002; Tarrant & Cordell, 1997; Weijzen, de Graaf, & Dijksterhuis, 2009). Evidence suggests that men and women differ in their beliefs about vulnerability to disease and their subsequent engagement in preventative health behaviors. Gender socialization influences health behavior, including men and women’s perceptions of and use of their bodies, and their psychosocial adjustment to illness (Sabo, 2000). Overall, men are more likely to adopt attitudes and beliefs that undermine their health and well-being, including being less likely to perceive themselves as vulnerable to disease (Courtenay, 2000; Eisler, 1995; Sabo, 2000; Tarrant & Cordell, 1997; Williams, 2003). This can be seen as a consequence of gender socialization, as men and adolescent males who adopt traditional or stereotypic beliefs about masculinity have greater health risks than their peers with less traditional beliefs (Courtenay, 2000; Eisler, 1995; Lippa, 2000). As a result, men often engage in riskier behaviors such as smoking, maintaining a poor diet, failing to exercise, and abusing alcohol, whereas women tend to engage in health protective behaviors (Courtenay et al., 2002; Kaplan & Marks, 1995; Nicholas, 2000). This gender-specific perception of health risk and subsequent health behavior is seen in nearly every racial and ethnic group (Courtenay et al., 2002).
Although there are well-documented gender differences in attitude-behavior consistency, the influence of this gender difference on disease outcomes is less well established. For example, although one ecological study showed that up to 40% of the gender differences in cardiovascular risk mortality can be attributed to differences in five health behaviors (Jackson et al., 1997), there are no longitudinal, population-based studies that have demonstrated that gender differences in the attitude-behavior link are consequential, particularly in heart disease.
Accordingly, the primary goal of this study was to test the hypothesis that gender moderates the relation between belief in CHD preventability and CHD incidence in a large, population-based sample of participants from Nova Scotia, Canada. That is, we examined whether the magnitude of the association between belief in CHD preventability and CHD incidence varied for men versus women. We further examined whether differential participation in health behaviors by men and women mediates the relation between health beliefs and incident CHD outcomes. Specifically, we examined whether a specific health behavior (i.e., smoking) could be a mechanism by which health belief confers increased risk of CHD incidence. We chose to examine smoking as it is a well-known behavioral risk factor for CHD that is monolithically negative (there are no good reasons to smoke) and is largely a matter of choice (there are no mitigating factors where a physician might encourage a patient to keep smoking).
We used a large population-based sample to understand how these theories play out in a more naturalistic setting. Additionally, as our data set includes 10-year ischemic cardiac disease outcomes, we were able to test not only the effect of health beliefs on health behaviors but also its subsequent implications on long-term disease outcomes. Given that data were collected in Canada, we were able to link participants’ baseline survey data with their medical records. The universal structure of the Canadian health care system further removed participants’ barriers to health care, which may have been a confounder if we had considered at the association of prevention beliefs and health outcomes in a cohort from the United States. Thus, we were able to test how health beliefs and subsequent health behaviors actually affected CHD incidence, which allows us to make some causal inferences that would not be possible cross-sectionally or in nations without universal health coverage.
Method
The Nova Scotia Health Study (NSHS95) was a population-based survey implemented by Heart Health Nova Scotia in partnership with the Nova Scotia Department of Health to estimate the distributions of selected health indicators and preventive practices of Nova Scotians. The sample was selected in 1995 based on a probability-sampling frame designed by Statistics Canada, the national statistical agency and census bureau, to be representative of the Nova Scotia population by age, gender, and geographic location. Those who were ineligible because of pregnancy, breastfeeding, ill-health, or disability were screened out as their CHD risk factors (e.g., weight, blood pressure, and diabetes) were not considered stable at entry.
In 1995, 3,217 study participants were enrolled in NSHS95; 2,688 of these participants provided consent for follow-up and did not have a previous CHD. The targeted population consisted of all noninstitutionalized Nova Scotians, aged 18 years and older, whose names were listed in the Medical Service Insurance register, the government-sponsored, universal health insurance plan. At the time of enrollment, participants completed a survey ascertaining CHD risk factors and health behaviors. During a 10-year follow-up period, information on CHD incidence was extracted from two national health registries for CHD incidence and linked to participants’ NSHS95 data. The province provides universal health care coverage for all its residents, thus assuring that all survey participants had access to the same level of health care and that events were recorded using a full-capture surveillance system. The overall recruitment percentage (72%) is comparable with other large health surveys, and weights applied from propensity score analyses to test for response bias revealed no meaningful biases (Lawson, 1999).
Survey Procedure
A group of 29 public health nurses completed a 5-day training session to learn the techniques for contacting participants and collecting data. From March through November of 1995, participants responded to a questionnaire that included questions regarding their health beliefs and that took approximately 90 minutes to complete. Participants also attended a health care clinic for assessment of fasting lipid levels, blood pressure, and anthropometric measures.
Measures
Demographics and traditional CHD risk factors
Participants’ age and sex were recorded from the provincial medical registry, and then verified by the nurse interviewer during the home session. Smoking, physical activity level, alcohol consumption, family history, and presence of diabetes were gathered during the home interview. Smoking status was coded such that those who reported that they had never smoked or had not smoked over the past year were defined as nonsmokers and those who reported currently smoking or having quit within the past year were defined as active/recent smokers. Other traditional cardiovascular risk factors, including total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, and blood pressure were ascertained either during the home visit or a clinic visit approximately 1 week later. Income was recorded in 1 of 15 ordinal categories.
Health beliefs
All participants were asked, “Based upon what you have heard or read, do you believe that heart disease can be prevented?” Participants answered “yes” or “no” to this question.
Incident CHD events
Our primary outcome was hospitalization or death by any CHD event based on International Classification of Diseases (ICD)-9 codes. Incident CHD hospitalizations and deaths for the 10 years following NSHS95 administration were determined from the provincial health care registry. A hospitalization was considered to be a CHD event if one of the discharge codes was for ischemic heart disease (ICD-9 codes 410.x, 411.x, 413.x, and 414.x and ICD-10 codes I21.x, I23.x, I24.x, and I25.x). This included acute myocardial infarction and other forms of acute ischemic heart disease but excluded old or previous myocardial infarctions (codes 412 and I22/I25.2). All hospitals submit discharge information to the provincial health care registry for reimbursement. Furthermore, reimbursements for hospitalizations that occur outside Nova Scotia are paid by the provincial plan. Thus, the provincial health care registry captures all hospitalizations for which the government-sponsored plan makes payment. The dates of all CHD events were obtained. To limit the analyses to incident events, we excluded participants with a CHD diagnosis prior to their baseline survey by searching for documentation of a CHD event in the 5 years prior to their survey date using the data sources described above. Additionally, participants who had multiple outcomes were censored in survival analyses at the time of their first event, thus there are no multiple events for participants.
All deaths are reported to provincial offices, which in turn notify the national census bureau, Statistics Canada, which applies a nationally consistent process of determining the underlying cause of death. Specifically, these data were converted to the ICD codes by staff at Statistics Canada, and only those codes listed above qualified as fatal CHD. Data were extracted by Population Health Unit of Dalhousie University. Participants were observed for up to 10 years, from the date of their initial visit in 1995 until the earliest of the following: 10-year anniversary of their initial visit date, March 2005, date of emigration, death from causes other than CHD, or documented incident CHD.
Analysis
Means and frequencies were calculated for descriptive purposes, with t tests and chi-squares calculated to test for differences between genders and health beliefs. Cox proportional hazards models were constructed to determine whether health belief predicts incident CHD over and above traditional cardiovascular risk factors. Specifically, we estimated the hazard ratios (HRs) of health belief for incident CHD, adjusted for age at baseline to control for cohort and healthy survivor effects, income as a marker for socioeconomic status, and used a decomposed Framingham risk score to control for traditional cardiovascular risk factors (total and HDL cholesterol, systolic blood pressure) because we were interested in the possible mediating effects of health behaviors such as smoking. We entered a cross-product gender-by-health belief interaction term in our Cox proportional hazards models to test whether gender moderates the relation between belief in CHD preventability and actual CHD incidence
If we found a significant moderator effect, we would then stratify the sample by gender to test whether smoking mediates the relation between health belief and incident CHD for men or women. We used Baron and Kenny’s (1986) definition of mediation, where the independent variable is associated with the dependent variable, the independent variable is associated with the mediator, and the mediator is associated with the independent variable in the model. Thus, we initially established that health belief was associated with incident CHD in women but not men using Cox proportional hazard models, we then used moderated logistic regression, to test the relation between health belief and smoking, controlling for each of the aforementioned covariates. Finally, we used a Cox proportional hazard model in which smoking predicted incident CHD, controlling for belief in CHD preventability and the other covariates for men and women separately. We used a Sobel test to test the significance of mediation found using the classic Baron and Kenny mediation criteria (Baron & Kenny, 1986; Preacher & Leonardelli, 2001; Sobel, 1982). Our decision to use the classic Baron and Kenny approach rather than bootstrapping was based on the need to use different analytic framework (survival and logistic regression) models to test the different hypothesized relations.
All analyses were performed using Statistical Package for Social Science (SPSS) software Version 18 (SPSS, 2010).
Results
Descriptive statistics for the participants included in the analysis are presented in Table 1, as are significant differences between genders and health beliefs. There were 235 (8.7%) incident CHD events (226 nonfatal, 9 fatal) during 26,570 person-years of observation (incidence rate = 8.84 events/1,000 person-years). As seen in Table 1, many standard risk factors were associated with both health beliefs and gender, such as cholesterol and systolic blood pressure. We then adjusted for age, cholesterol, systolic blood pressure, and income as they were possible confounders.
Characteristics for Consented Participants (N = 2,688)
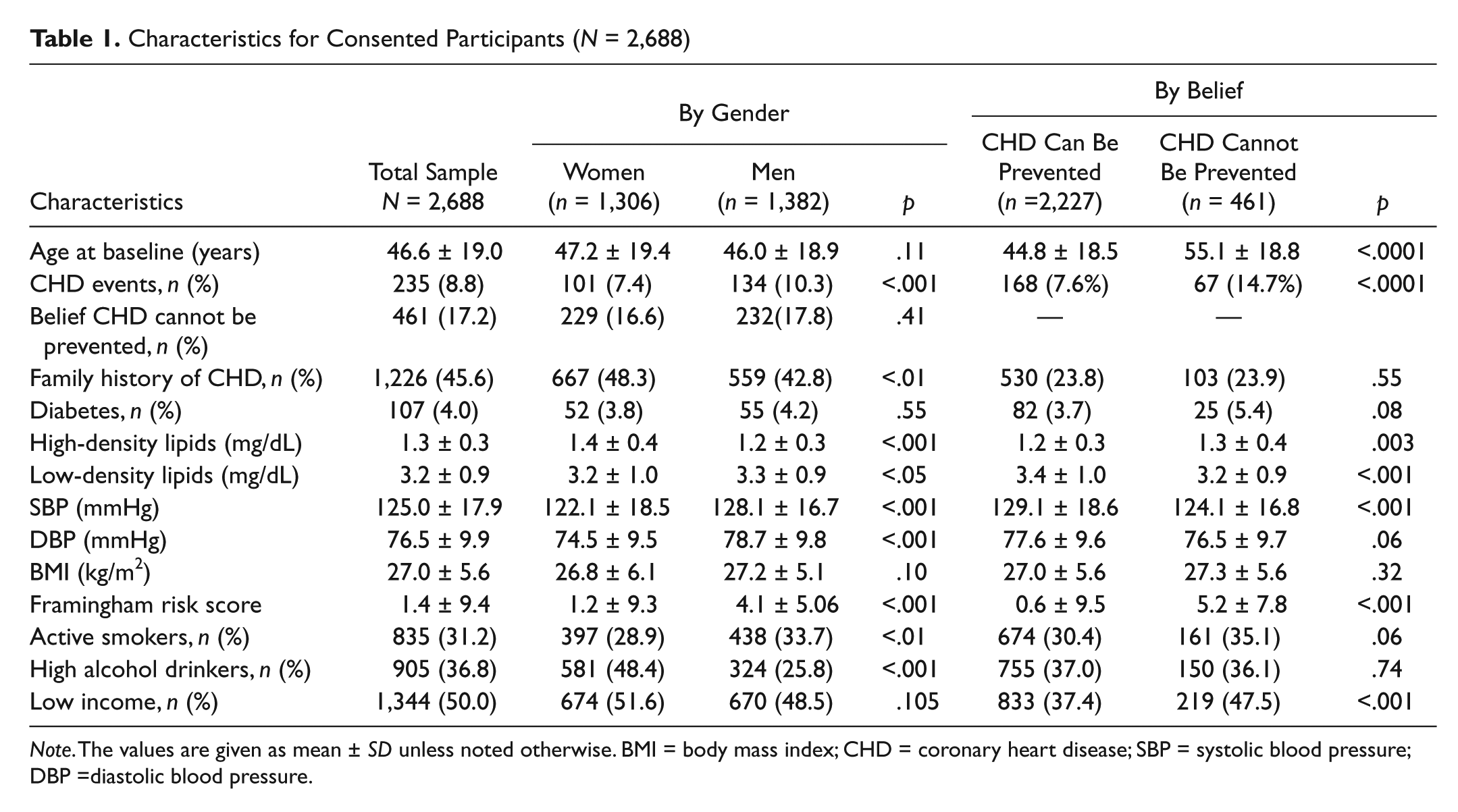
Note. The values are given as mean ± SD unless noted otherwise. BMI = body mass index; CHD = coronary heart disease; SBP = systolic blood pressure; DBP =diastolic blood pressure.
Gender significantly moderated the relation between belief in CHD preventability and CHD incidence (HR = 0.48, 95% confidence interval [CI] = 0.27-0.86, p = .013) as hypothesized (Figure 2). This moderating effect remained after adjustment for age, total and HDL cholesterol, systolic blood pressure, and income (HR = 0.38, 95% CI = 0.19-0.78, p = .008).
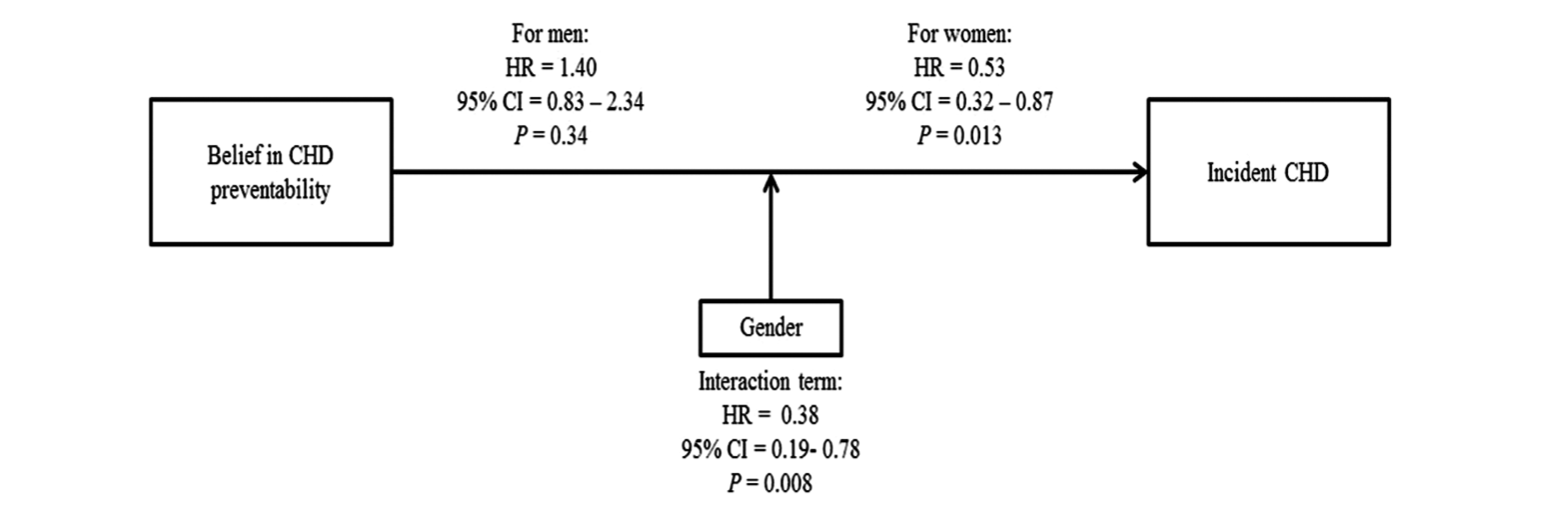
Model linking belief in CHD preventability, gender, and incident CHD outcomes
As seen in Table 2, we next stratified the sample by gender, and found that women who answered that they believed in the preventability of CHD were significantly less likely to have an incident CHD event within 10-year follow-up than women who did not believe in heart disease preventability (HR = 0.36, 95% CI = 0.24-0.55, p < .001) in a Cox regression model. After adjusting for covariates, findings for women were still significant (HR = 0.53, 95% CI = 0.32-0.87, p = .013). While the association was significant for men in the unadjusted model (HR = 0.64, 95% CI = 0.44-0.95, p = .028), the association was no longer significant after adjusting for the covariates (HR = 1.34, 95% CI = 0.83-2.34, p = .20).
Pathway, Unit of Change, and Regression Parameters

Note. CHD = coronary heart disease; HR = hazard ratio; OR = odds ratio.
Adjusted for age at baseline, total cholesterol, systolic blood pressure, and income.
p < .05. **p < .01.
To further examine the relation between health belief and incident CHD, we next considered if smoking was a mediator in the relation of health beliefs and incident CHD for men and women separately. We first established that health belief in preventability predicted less smoking in a logistic regression for women (β = −0.70, odds ratio [OR] = 0.50, 95% CI = 0.33-0.74, p = .001) but not for men (β = −0.31, OR = 0.73, 95% CI = 0.50-1.07, p = .11) after adjusting for covariates. Smoking also significantly predicted increased risk for incident CHD for women (β = 0.68, HR = 1.97, 95% CI = 1.13-3.42, p = .017) but not for men (β = 0.19, HR = 1.21, 95% CI = 0.74-1.99, p = .44), after adjusting for health belief and the additional covariates in a Cox regression model, thus meeting the classic Baron and Kenny’s (1986) criteria of a mediator. We tested the significance of the mediated relation with a Sobel test and found that smoking was a significant mediator of the relation between health belief and incident CHD for women (z = −1.96, p = .05). This model can be seen in Figure 3.
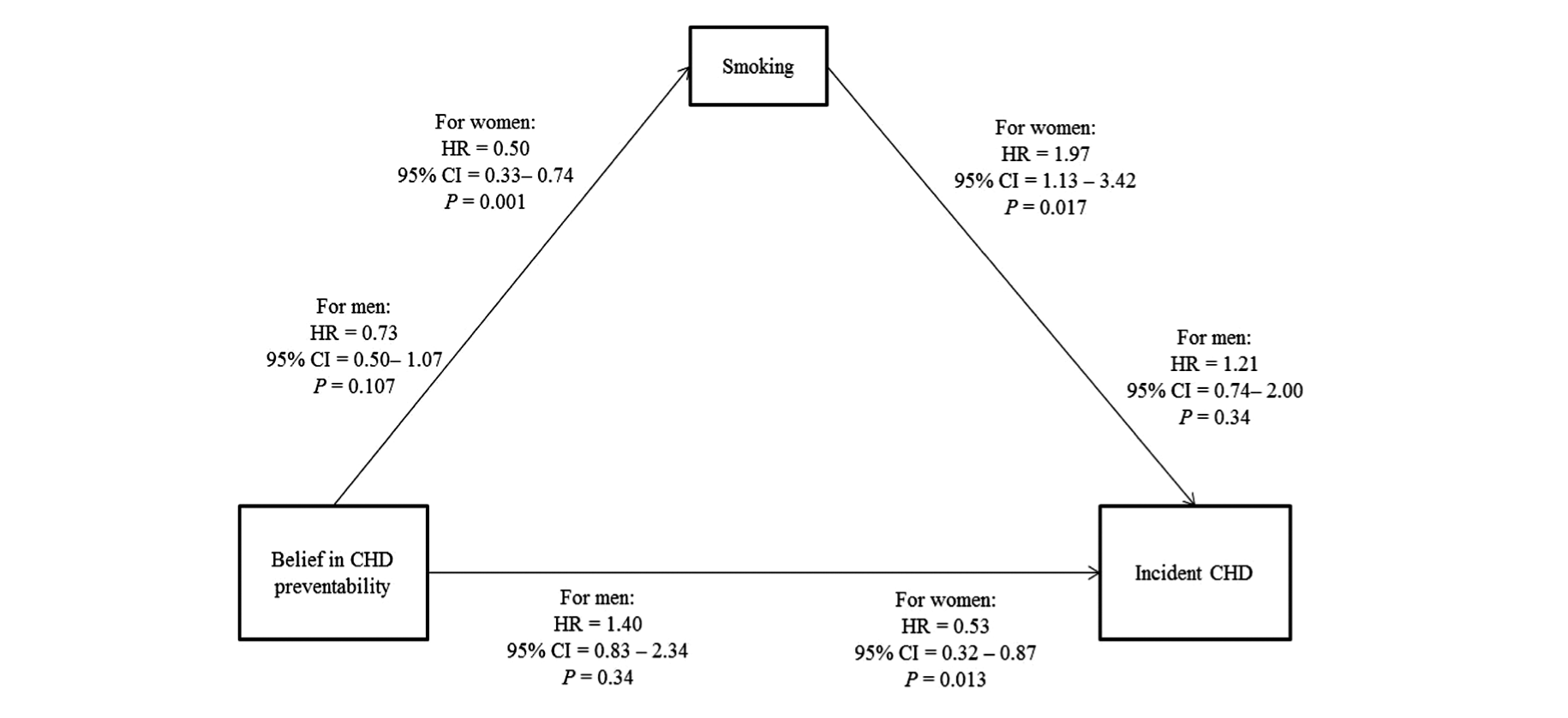
Model linking belief in CHD preventability, smoking, and incident CHD outcomes by gender
Discussion
We found that gender was a significant moderator in the relation between health belief and incident CHD in this large, randomly selected population-based sample. Although belief in CHD preventability was associated with lesser risk of incident CHD for women, the same was not true for men. We further found that women who believed that heart disease can be prevented were significantly less likely to engage in CHD behavioral risk factors such as smoking, leading to a lower incidence rate of CHD in this sample. For men who believed that heart disease can be prevented, engagement in smoking was affected to a lesser extent than it was among women. Support for our hypotheses lend support to the literature suggesting the importance of accounting for patients’ gender in formulating treatment and prevention protocols (Brown & Bond, 2008; Von Bothmer & Fridlund, 2005; Wardle et al., 2004) as well as demonstrate the consequences of gender differences in attitude-behavior consistency.
We also found that age was a contributing factor to how people perceived the preventability of heart disease. Older people tended to believe that heart disease cannot be prevented and had higher cardiovascular risk factors. Our findings suggest that as people age, and they are more susceptible to cardiovascular risk factors, they become more fatalistic about their ability to prevent heart disease.
This finding adds to literature on the health belief model, given that this literature has traditionally not considered the importance of the perception of preventability. Our study suggests that the belief that a disease is preventable, in and of itself, is an important predictor of long-term health outcomes for women. Most studies that have tested health behavior theories have relied on cross-sectional correlational designs with no prospective data to corroborate findings (Weinstein, 2007). Moreover, although some studies have examined the effect of health beliefs on CHD recurrence and lifestyle change after an acute coronary event (Byrne et al., 2005; Stafford, Jackson, & Berk, 2008), few prospective studies have examined the effects of health beliefs on CHD incidence. Thus, our findings add valuable insight into how health beliefs affect long-term health outcomes.
Gender, Health Beliefs, and Prevention
Our findings match those of previous studies that have reported gender differences in health beliefs and preventive health behavior adherence. Studies have consistently shown a gender difference in attitude–behavior consistency, with women’s intentions more highly correlated with behavior (Nigg, Lippke, & Maddock, 2009; Weijzen et al., 2009) compared with men. Men within nearly every racial and ethnic group are more likely than women to engage in behaviors and adopt beliefs that are detrimental to their health (Courtenay et al., 2002). Our study shows that although both men and women tend to believe that heart disease can be prevented; for women, this translates more strongly into a direct change in their preventive health behavior.
A recent meta-analysis has shown that smoking is more predictive of CHD for women than for men (Huxley & Woodward, 2011). Our findings shed further insight into this association, suggesting that perhaps for women, smoking is an indicator of a belief that heart disease cannot be prevented. This underlying belief may have some unmeasured effect in overall CHD health and engagement in preventive health behaviors.
Women and Perceived Cardiovascular Risk
Additionally, this study contributes to previous literature that has shown that women do not recognize that CHD can be prevented (Christian, Rosamond, White, & Mosca, 2007; Mosca et al., 2005; Mosca, Ferris, Fabunmi, & Robertson, 2004). Research has shown that women in particular are more likely to attribute their CHD to positive family history than to other major modifiable risk factors (Mosca et al., 2006; Murphy et al., 2005). Although the majority of a sample of 1,024 women in one study recognized that engaging in certain activities such as exercise, weight loss, and reducing dietary intake of cholesterol and salt may reduce the risk of heart disease, only 38% actually had a discussion about heart disease with their physician (Mosca et al., 2004). Thus, our findings highlight the importance of patients’ beliefs in preventability when considering their engagement in preventative behaviors, treatment adherence, and long-term cardiac outcomes.
Clinical and Public Health Implications
These results support the critical need to understand and test the mechanisms by which belief in the preventability of CHD confers increased risk of incident CHD. This program of research has important public health implications for health education, and reinforces the need to tailor our health promotion efforts to each gender. Understanding which health beliefs lead people to engage in health-seeking behavior will allow for more tailored and targeted health education and cognitive interventions. Our results suggest that such interventions may be particularly effective for women. For men, however, our results suggest that strategies to strengthen the link between health beliefs and health behaviors may be more important, through better health education and community outreach.
Our study shows that the first step to any intervention or prevention program could include an assessment of what people believe about their health or about their specific health behaviors. Thus, a health practitioner could focus not only on identifying health behaviors that need to be modified but also on the patient’s beliefs about the preventability of disease and health consequence. Our results suggest that effective education about the control patients may have over their health may be particularly important. Targeted public health campaigns to address this issue could also be useful, as well as physician education on this matter.
Study Limitations
In addition to the lack of well-measured health behaviors, other than smoking, further limitations of this study include the reliance on one question to measure health beliefs. A more comprehensive structured interview with a validated health belief instrument (e.g., Multidimensional Health Locus of Control scale; Wallston, Wallston, & DeVellis, 1978) may have yielded a more reliable and valid assessment of health beliefs, although it may have demanded more time of participants and interviewers.
Although our primary independent variable was reliant on a single question, it was straightforward and directly measured how people felt about the preventability of heart disease. Other studies measuring health beliefs and perceived susceptibility have also used similar questions, such as Courtenay et al.’s (2002) use of items such as “I believe I have control over my future health.” Indeed, the fact that we were able to detect differences in gender, even after adjusting for possible confounders, attests to the strength of this study measure, despite its limitations.
An additional limitation of our study was a reliance on smoking as a health behavior to measure mediation. The finding that smoking was related to women’s beliefs but not men’s should be considered in the context of the addictive nature of smoking (Bruijnzeel, 2012; Castañé, Berrendero, & Maldonado, 2005; Dani & De Biasi, 2001). Although our study also had crude measures of alcohol consumption and physical activity, we do not believe that either of these measures was reliable or valid. Additionally, neither of these variables was related to health beliefs in supplemental analyses (not shown), thus not passing the initial test of mediation.
As the data we have presented here are for 10-year CHD outcomes, and the average age at baseline is 46 (with participants as young as 18 years old included), much of what we are capturing is early heart events. Given that women tend to have events later than men, our study is limited as we are not able to show the full scope of heart disease outcomes in women.
Another weakness of our findings is the unknown generalizability from Canada to the United States. Yet the nationalized Canadian health care system allowed us to retrieve and link health care utilization data in a manner that would have been considerably more difficult in the United States.
Conclusion
Health belief in the preventability of illness was found to be an important independent predictor of incident CHD in women but not in men. Risky health behaviors, such as smoking, in turn mediated the effect of health beliefs on incident CHD for women but not for men.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
The study was supported by grants HP-10260 from the National Institutes of Health, Bethesda, MD, as well as HL-080665, HL-088117, HL-076857, HL-084034, HL-072866, and HL-04458 from the National Heart, Lung, and Blood Institute, Bethesda, Md. This project was also supported by Grant UL1 RR024156 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH) and NIH Roadmap for Medical Research. The National Health & Welfare of Canada, the Nova Scotia Department of Health, and the Heart and Stroke foundation of Canada all supported the original data collection. The study sponsors had no role in the study design, collection, analysis, writing, or interpretation.