
Abstract
An unintended consequence of tobacco control’s success in marginalizing smoking is that smokers may conceal their smoking from those who are best positioned to help them quit: health care providers (HCPs). The purpose of this study was to identify the prevalence of, and factors related to, nondisclosure of smoking to HCPs. Data were obtained from a cross-sectional survey of adults from a nationally representative Knowledge Networks online panel in March to April 2011. Current and former smokers (n = 2,803) were asked questions about nondisclosure, tobacco use, cessation behavior, and perceived social unacceptability of smoking. All variables significantly related (p < .05) to nondisclosure in bivariate logistic regression were included in the multivariate logistic regression model, which also adjusted for gender, age, race, marital status, and education. Approximately 1 in 10 smokers (12.9%) and 5.8% of former smokers has withheld their smoking status from HCPs. Ever smokers who were 18 to 34 years, those who had used a prescription medication or behavioral therapy in their last quit attempt, and those who were uncomfortable discussing smoking with their HCP were more likely to report nondisclosure than those in their respective comparison groups. Respondents who perceived either medium or high smoker-related stigma (odds ratio [OR] = 1.70, 95% confidence interval [CI] = 1.05, 2.77 and OR = 2.60, 95% CI = 1.51, 4.48, respectively) and those who reported concealing smoking to gain benefits from health insurance were also significantly more likely to have kept smoking a secret from an HCP (OR = 5.66, 95% CI = 1.88, 17.02). Smokers should be encouraged to be forthright about their smoking in order for practitioners to offer treatment and services that increase their chances of quitting.
Keywords
Over the past half century, tobacco use in the United States has become increasingly socially unacceptable (Alamar & Glantz, 2006). The proliferation of smoke-free indoor air laws, increasing tobacco taxes, and antismoking media campaigns have all contributed to a reduction in cigarette consumption (Alamar & Glantz, 2006). One unintended consequence of tobacco control’s success in marginalizing smoking is that smokers may be more likely to conceal their smoking status from those who are best positioned to help them quit: health care providers (HCPs; Stuber & Galea, 2009).
Certain populations are more likely to underreport their smoking status than others, including pregnant women, those enrolled in cessation studies, people with tobacco-related diseases, and cancer patients (Martínez, Reid, Jiang, Einspahr, & Alberts, 2004; Murray, Connett, Lauger, & Voelker, 1993; Pell, 2008; Shipton et al., 2009; Webb, Boyd, Messina, & Windsor, 2003). An early study of “deception” among smokers found the level of discordance between self-report and biochemical verification to be as high as 40% in subjects enrolled in trials to stop smoking (Sillett, Wilson, Malcolm, & Ball, 1978). In 2001, a Chicago community study found underreporting of tobacco use to be rare, but occurring in higher rates among people who also underreport use of other illicit substances. This suggests that as tobacco becomes an increasingly stigmatized behavior, respondents’ reluctance to disclose begins to parallel that of drug use (Fendrich, Mackesy-Amiti, Johnson, Hubbell, & Wislar, 2005). Because self-reported smoking behavior is a valid indicator of smoking status in most large population surveys (Assaf, Parker, Lapane, McKenney, & Carleton, 2002; Velicer, Prochaska, Rossi, & Snow, 1992; Yeager & Krosnick, 2010), the high degree of discrepancy between self-reported smoking and biochemical marker levels in cessation trials or other, smaller studies might be explained by elevated cotinine levels resulting from secondhand smoke exposure, measurement error, or medications (Yeager & Krosnick, 2010). Alternatively, this inconsistency may be because of social desirability bias, as social stigma may result in underreporting of smoking among current smokers in the setting of a cancer prevention study, prenatal care, or in a cessation trial in which the subjects are under greater perceived pressure to quit.
Although social desirability bias may explain underreporting of smoking in cessation trials or other health-related outcome studies, little is known about prevalence of or motivation for concealing one’s smoking status outside of these contexts, specifically in the health care setting. One study on this topic reported on data from New York City residents collected in 2005 (Stuber & Galea, 2009). Among the 835 current smokers surveyed, 8% reported ever having kept their smoking a secret from an HCP. Factors related to nondisclosure were high levels of perceived smoker-related stigma and strict no-smoking rules within the household.
The current study used a large, nationally representative sample to measure the prevalence and examine the factors related to nondisclosure, including the perception of smoking as socially unacceptable and as a “habit” versus an addiction, as well as cessation attitudes. Given the broad impact of smoking on health and the potential influence that HCPs can have on patients who smoke, it is critical to further investigate the issue of nondisclosure of smoking status to HCPs to increase opportunities for cessation and improve health outcomes.
Method
Sample
Data were obtained from a cross-sectional survey of 2,803 current and former smokers. The survey was fielded in March to April 2011 using Knowledge Networks’ KnowledgePanel®, a nationally representative online panel of adults aged 18 years and older. Panel members were recruited through national random samples, originally by telephone (1999-2009) and starting in April 2009 almost entirely by postal mail. Since panel members were recruited from both telephone and address-based methods, Knowledge Networks has implemented several technical processes to merge samples sourced from these frames to preserve the nationally representative structure of the overall panel. Unlike Internet convenience panels (i.e., “opt-in” panels), no one can volunteer to be on the panel. Instead, recruitment uses dual sampling frames that include listed and unlisted telephone numbers, telephone and nontelephone households, cellphone-only households, and households with and without Internet access. Members are supplied with the Internet and hardware if needed. All new members complete a profile survey that collects essential demographic information used for determining study eligibility and weighting. This is updated annually, with members typically active for 3 years. Members are rewarded for completing surveys with points redeemable for cash or free access to the Internet if not already available in the household. Additional details on sampling methodology are available on the Knowledge Networks website (http://www.knowledgenetworks.com/knpanel/index.html).
The Knowledge Networks KnowledgePanel consists of about 50,000 adult members aged 18 years and older. The overall recruitment rate for the whole panel is only 4.17%, but the demographic profile of respondents corresponds to that of the U.S. general population as measured by the June 2011 CPS survey (http://www.knowledgenetworks.com/knpanel/docs/GfK-KnowledgePanel(R)-Demographic-Profile.pdf). With regard to the smoking population, approximately 17% were current smokers, which is in line with the smoking prevalence in the United States. This study sampled current and former smokers from the panel members and oversampled by race/ethnicity and in three states with varying strength of tobacco control policy (n = 339). The state oversamples, however, were removed for this analysis but are described below to clarify the methodology. Smoking status on panelists was obtained from a health profile survey that all panelists must fill out. A current smoker was defined as someone smoking at least 100 cigarettes in his or her lifetime and endorsing current “everyday” or “someday” smoking. A former smoker was defined as having smoked at least 100 cigarettes in his or her lifetime and endorsing no current smoking. The sample for this study was selected from those in the health profile survey who indicated they had ever smoked 100+ cigarettes. For African Americans and Hispanics, Knowledge Networks randomly selected enough sample, assuming a 50% response rate, to obtain 150 current and 150 former smokers for each respective racial/ethnic group. For the remainder of the sample (non-African American and non-Hispanics), they randomly selected enough sample, assuming a 60% response rate, to obtain 900 current and 900 former smokers. For the state oversamples they randomly selected enough of the remaining sample, assuming a 60% response rate, to obtain 100 completes from each of the three states of interest. Using this methodology, 5,306 panelists were contacted for participation. Of these, 3,585 (67.6%) completed the screening, and 3,146 were deemed eligible for the study (n = 1,373 current smokers and n = 1,773 former smokers). Poststratification weights were constructed on this sample to adjust for the study’s sample design and for survey nonresponse. As stated above, the state oversamples (n = 339) were removed from the sample, and an additional four individuals were removed since they refused to answer the main outcome variable in this study (nondisclosure of smoking status). This left a final sample size of 2,803 current (n = 1,296) and former smokers (n = 1,507). This study was exempted from requiring institutional review board review and approval by Independent Investigational Review Board, Inc.
Measures
The dependent variable for this analysis was response to the question, “Have you ever kept your smoking status a secret from a health care provider (a health care provider could be a medical doctor, nurse, nurse practitioner, dentist, pharmacist, or physician assistant)?” If yes, respondents were asked how and why the nondisclosure occurred in order to determine the context of nondisclosure. Nondisclosure that occurred because “My HCP did not ask and I did not bring it up” was classified as “passive,” whereas the responses “I checked ‘no’ while filling out a paper or online form from my HCP that asked about my smoking status,” and “I answered ‘no’ in response to my health care provider asking whether or not I smoked” were classified as “active” nondisclosure events. Current and former smokers were also asked questions about their tobacco use, cessation behavior, and other potential behavioral and attitudinal correlates of concealing smoking from an HCP.
Tobacco use items included cigarettes per day, nicotine dependence as measured by the Fagerstrom Test for Nicotine Dependence item “Time to First Cigarette” of the day (T. B. Baker et al., 2007), motivation to quit, and intention to quit (Prochaska & DiClemente, 1983). Past-12-month quit attempts was measured for current smokers, along with a number of cessation methods used in their last (if current smoker) or final (if former smoker) quit attempt.
Seven items measuring perceived social unacceptability of smoking were taken from Stuber and Galea (2009). First, to measure their normative environment, respondents were asked “How do most of your close friends and family feel about cigarette smoking among adults?” Response options included “acceptable, unacceptable, or don’t care one way or the other.” Second, an item measuring household smoking rules asked, “Which statement best describes smoking in your home?” Response options included “people smoke anywhere inside your home,” “people smoke in some rooms or at some times,” and “people do not smoke anywhere inside your home.” Next, two items were used to create a “smoker-related stigma scale”: “Most people believe that smoking is a sign of personal failure” and “Most people think less of a person who smokes.” Response options fell along a Likert-type scale from 1 (strongly disagree) to 4 (strongly agree). Summary scores ranged from two to eight; a tertile scale was created representing low, medium, and high stigma. Finally, three items were used to create a measure of perceived differential treatment due to smoking: “Have you had difficulty renting an apartment or finding housing because of your smoking?” “Were you turned down for a job for which you were qualified because of your smoking?” and “Were you refused or charged more for health insurance because of your smoking?” “Yes” to any of these items constituted perceiving differential treatment due to smoking.
Respondents were also asked whether they were a caretaker of dependents younger than 21 years, their perceived health status, and their comfort discussing smoking with an HCP. To assess respondents’ characterization of smoking, definitions of “habit,” “addiction,” and “lifestyle” were given before the question, “How would you characterize smoking? (a) Habit, (b) Addiction, (c) Lifestyle choice, (d) Other (Please specify).” Definitions were as follows: Habit: a routine behavior that is repeated regularly and tends to occur subconsciously, without one’s directly thinking about them; Addiction: compulsive need for, dependence on, and use of a substance that the user knows is harmful; Lifestyle: the way a person lives. Norms about quitting were measured using 14 agree/disagree statements (e.g., “People who smoke can easily quit if they have will power”). Finally, all current and former smokers were asked if they ever concealed their smoking in a variety of other situations, such as in order to rent an apartment or get a specific job.
Statistical Analysis
Bivariate logistic regression was used to examine the relationship between nondisclosure of smoking to an HCP (dependent variable) with each of the independent variables already described. All variables significantly related (p < .05) to nondisclosure in bivariate logistic regression were included in the multivariate logistic regression model, which additionally adjusted for gender, age, race, marital status, and education. In our analysis, estimates were weighted to adjust for the sample design and nonresponse. All statistical analyses were performed in June 2011 using Stata statistical software, version 11.2 (StataCorp LP, n.d.).
Results
Sociodemographic and tobacco use information about the study population of smokers and former smokers are presented in Table 1. Most of the respondents were non-Hispanic White (70.4%), followed by non-Hispanic Black (12.5%), Hispanic (11.4%), and those of other race/ethnicity (5.6%). There was a roughly even distribution of males (54%) and females (46%), and the majority were at least 35 years of age (85.8%) and had at least a high school education (89.2%). More than one fourth (26.8%) were a parent or caretaker of a child aged 21 years and younger, and 63.4% reported being married or living with a partner. One quarter of the sample (25.5%) describe their overall health as fair or poor.
Predictors of Nondisclosure of Smoking to a Health Care Provider Among Current and Former Smokers.
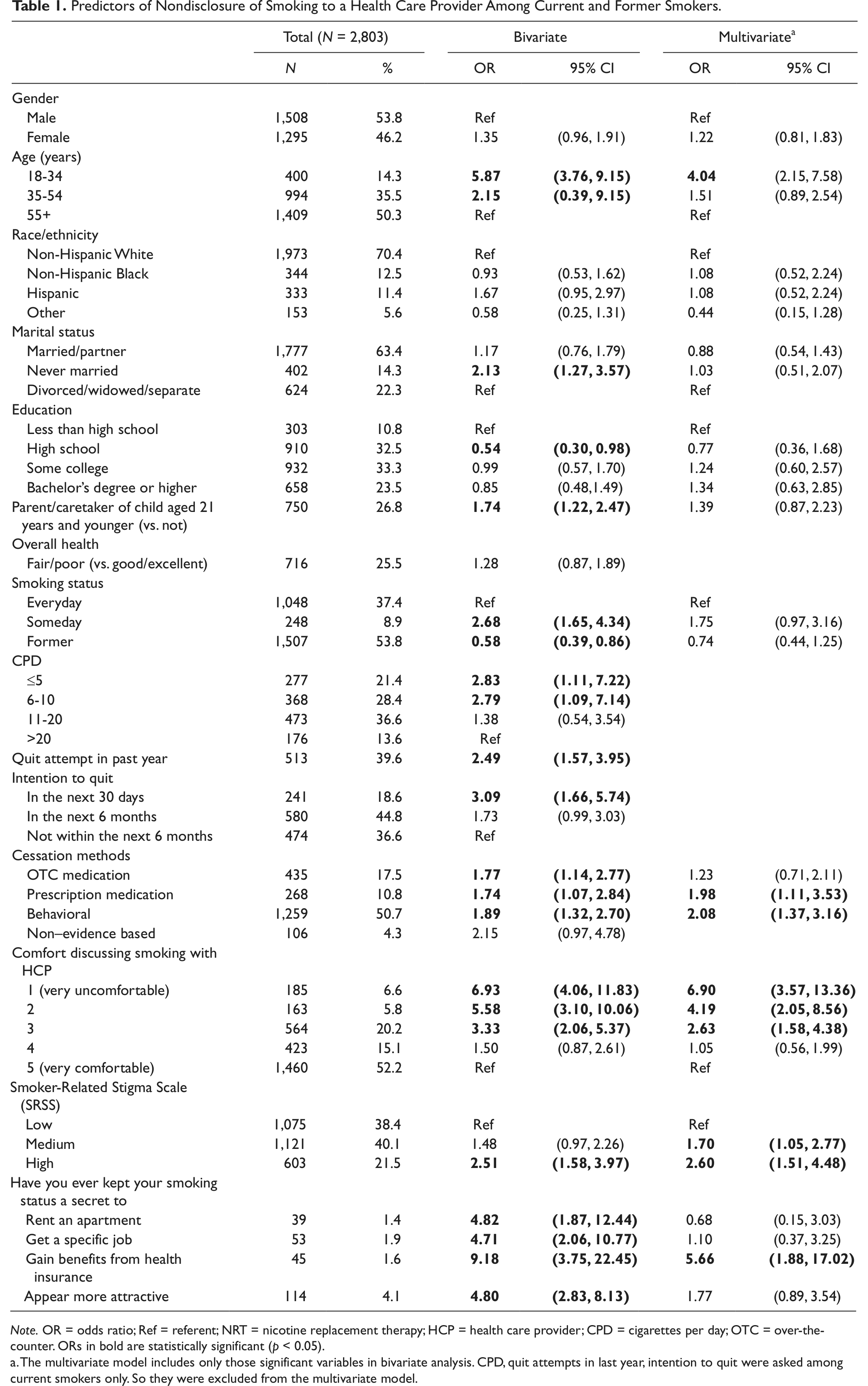
Note. OR = odds ratio; Ref = referent; NRT = nicotine replacement therapy; HCP = health care provider; CPD = cigarettes per day; OTC = over-the-counter. ORs in bold are statistically significant (p < 0.05).
The multivariate model includes only those significant variables in bivariate analysis. CPD, quit attempts in last year, intention to quit were asked among current smokers only. So they were excluded from the multivariate model.
Former smokers constituted 53.8% of the sample; of the remaining sample, 37.4% were everyday and 8.9% were someday smokers. Overall, 8.9% of respondents reported ever keeping their smoking status a secret from an HCP. Nondisclosure was higher among current smokers (12.9%) as compared with former smokers during the time they smoked (5.8%). Self-reported reasons for nondisclosure included not wanting a lecture from the HCP (59.1%), feeling ashamed about smoking (45.6%), not being ready to quit at the time (32.8%), and being scared to admit to smoking (21.6%). Incidences of nondisclosure occurred in a few different contexts: answering “no” in response to the HCP asking whether or not the respondent smoked (49.8%), not bringing it up if the respondent was not asked by their HCP (42.5%), and checking “no” while filling out a paper or online form that asked about smoking status (34.0%).
Bivariate analyses revealed that respondents who were younger and those who were never married, had less than high school education, and were the parent or caretaker of a dependent aged 21 years and younger were significantly more likely to have ever kept their smoking status a secret from an HCP as compared with their comparison groups (Table 1). Someday smokers, those who smoke less than five cigarettes a day, respondents who had made a quit attempt in the past year, those who intended to quit in the next 30 days, and those who had used all but two of the cessation methods on their last or final quit attempt were also more likely to report concealing their smoking than their comparison groups. Smoker-related stigma, comfort discussing smoking with an HCP, and having ever kept smoking a secret in other situations, such as to rent an apartment or appear more attractive, were also significantly related to nondisclosure. None of the items measuring norms about quitting or the characterization of smoking were statistically significantly related to nondisclosure (data not shown). Three of the four measures of social acceptability of smoking (perceived differential treatment, friends and family view of smoking, and home smoking rules) were also statistically unrelated to nondisclosure.
Many of the statistically significant associations mentioned above were retained in a multivariable logistic regression model. Age was negatively associated with nondisclosure: as compared with those aged 55+ years, respondents 18 to 34 years were more than four times as likely to report keeping their smoking a secret (odds ratio [OR] = 4.04, 95% confidence interval [CI] = 2.15, 7.58). Use of prescription medication and evidence-based behavioral therapy during a prior or final quit attempt was also significantly related to concealment of smoking status (OR = 1.98, 95% CI = 1.11, 3.53, and OR = 2.08, 95% CI = 1.37, 3.16, respectively). When analyzed by smoking status, however, this association was only statistically significant within former smokers. Comfort discussing smoking with an HCP was inversely related to nondisclosure, with the highest level of discomfort associated with the highest rates of nondisclosure (OR = 6.90, 95% CI = 3.57, 13.36). Only one of the four measures of perceived social unacceptability was significantly related to nondisclosure. Respondents who perceived either medium or high smoker-related stigma were more likely to report ever concealing their smoking from an HCP compared with respondents who perceived low smoker-related stigma (OR = 1.70, 95% CI = 1.05, 2.77 and OR = 2.60, 95% CI = 1.51, 4.48, respectively). Finally, those who reported keeping smoking a secret to gain benefits from health insurance were significantly more likely to have concealed their smoking from an HCP (OR = 5.66, 95% CI = 1.88, 17.02).
Because quit attempts and intention to quit could not be put into the multivariable model for the full sample (since former smokers did not answer these items), the analysis was replicated in a restricted sample, which included only current smokers (n = 1,296). Quit attempts and intention to quit were significant predictors of nondisclosure in the bivariate analysis of current smokers (OR = 2.49, 95% CI = 1.57, 3.95 and OR = 3.09, 95% CI = 1.66, 5.74, respectively); however, they were not significant in the multivariable model.
Finally, we analyzed three groups separately to see if context of nondisclosure affected predictors or nondisclosure. Predictors did not differ by disclosure type (i.e., active, passive, both active and passive).
Discussion
This study indicates that approximately 1 in 10 smokers (12.9%) has withheld their smoking status from HCPs. Projected to the population of smokers in the United States, this amounts to more than 6 million smokers nationwide not revealing to their HCP that they smoke (Centers for Disease Control and Prevention, 2010). This finding is similar to a previous study conducted on 835 current smokers in New York City where 8% of respondents reported concealing their smoking from an HCP (Stuber & Galea, 2009). Although nondisclosure of smoking status to an HCP may represent a different construct than endorsement of nondisclosure in a survey, the prevalence of nondisclosure reported in this study within female smokers (11%) is consistent, if slightly higher, than biochemically verified nondisclosure among female smokers in another nationally representative study, which found 9% of nonpregnant female smokers did not disclose their smoking status to survey interviewers (compared with 23% of pregnant smokers; Dietz et al., 2011).
Nondisclosure endorsed by former smokers, when they smoked, was half the rate of nondisclosure reported by current smokers. This could be because of recall bias, as former smokers may be less likely to remember incidents of nondisclosure, especially those who may have quit years prior to this survey. Since former smokers were not asked about the length of time since they quit, this cannot be assessed in these data. Increased rates of nondisclosure in current smokers may also reflect the increasing stigma surrounding smoking, due in large part to the enactment of tobacco control policies. The effect of stigma in this study was evident as medium or high smoking-related stigma was associated with nondisclosure, which is in agreement with past research (Stuber & Galea, 2009). Smokers may be responding to this stigma by providing a socially desirable response, which is to either avoid bring up their smoking status or deny it, if asked. Respondents even indicated that they had kept their smoking a secret in other areas of their lives, such as to appear more attractive, supporting the idea that these smokers feel social pressure to present themselves as nonsmokers.
Although this study produced results comparable to some prior research, there were several findings that were not replicated. For example, unlike a 1978 study, which documented small increases in “deception” among married trial participants, this study found no relationship with marital status (Murray et al., 1993). This may be related to the vast differences in the social construct of marriage today as compared with decades ago. This study also found no association with race/ethnicity and nondisclosure, contrary to a previous study conducted in Chicago (Fendrich et al., 2005). These samples, though, are not directly comparable as the social environment and tobacco control policies of Chicago in 2005 may differ from that assessed in this nationally representative sample in 2011.
Several results of this study are novel: younger smokers, former smokers who had used prescription medication or behavioral therapy in their final quit attempt, and those who have kept their smoking a secret in order to gain benefits from health insurance were more likely to have ever concealed their smoking from an HCP than their comparisons. Past research has found that desire to stop smoking is associated positively with age, but confidence in the ability to stop smoking is associated negatively with age (Kviz, Clark, Crittenden, Warnecke, & Freels, 1995). If younger smokers are more confident in their ability to quit but have less desire to do so, it follows that they may not find it necessary to report their smoking to an HCP. This study was also the first to document an association between nondisclosure and health insurance. More research is needed to identify reasons underlying this association as it has obvious clinical ramifications, but it is possible that smokers may be afraid of being denied medical coverage if their smoking status is revealed to an HCP. This might be an unintended consequence of insurance companies instating policies that increase premiums for smokers.
Research assessing physician–patient communication found that physicians felt smoking to be the least embarrassing topic to discuss (compared with diet and physical activity), required less time to discuss than other topics, and felt the most adequately trained to counsel about smoking cessation (Dolor et al., 2010). Results presented here, however, suggest that practitioners may be missing important opportunities to provide cessation-related resources and counsel to their patients who smoke. Almost half (42.5%) of those who reported nondisclosure were not asked about their smoking status. To minimize nondisclosure among smokers, all HCPs should at a minimum screen their patients for smoking according to the 2008 Update to the Clinical Practice Guidelines for Smoking Cessation (Fiore et al., 2008). Assessing smoking status in a nonjudgmental way might help lower the rate of concealment.
Limitations
Several factors may limit the generalizability of these findings. First, this study relies on self-report and may be a substantial underestimate of the true rate of nondisclosure in clinical settings. Because of social desirability bias, some respondents may not want to admit that they failed to disclose or lied about their smoking status to an HCP. Second, because of the cross-sectional nature of the report, causation cannot be determined for any of the significant relationships between variables. Third, the quality of data from online panels has been questioned (R. Baker et al., 2010). However, Knowledge Networks’ KnowledgePanel uses a probability-based recruitment design (address-based and previously RDD), reducing bias related to coverage and increasing accuracy of population estimates. Finally, because the recruitment rate for the overall panel was low, key motivational and psychosocial characteristics may significantly differ between respondents and nonrespondents. However, several methodological studies have demonstrated that the representativeness of the Knowledge Networks’ KnowledgePanel is similar to that of an RDD sample and that estimates did not differ significantly between the KnowledgePanel and other large probability RDD samples (Heeren et al., 2007; Yeager et al., 2011). Results from these and other articles discussing validity of the results from KnowledgePanel and the representativeness of the sample can be found at http://www.knowledgenetworks.com/ganp/reviewer-info.html.
Conclusion
This study provides a national prevalence estimate of nondisclosure of smoking among smokers and former smokers in the United States. In addition, we begin to identify correlates of nondisclosure that may be amenable to intervention, or at least require attention to prevent concealment of smoking at patient–provider interactions. Perceived stigma around smoking, an unintended consequence of the tobacco control movement, appears to be leading some smokers to conceal their smoking status in environments where admission is of utmost importance. Previous research has shown that contact with a physician or dentist is negatively associated with smoking (Kaplan, Newsom, & McFarland, 2002). In the current study, respondents who reported greater comfort discussing smoking with an HCP were less likely to have kept their smoking a secret. Since biochemical verification at HCP visits is not feasible, the solution lies with improving patient–provider communication. Clinicians and other providers can improve communication and encourage information sharing with patients by setting the right tone for the interaction: ensuring a quiet and nonthreatening physical environment, maximizing privacy and minimizing interruptions, and showing sensitivity, eye contact, active listening, and appropriate nonverbal cues (Teutsch, 2003).
Patient–provider confidentiality could also be stressed during the course of a visit. Research on high-risk behaviors has found that confidentiality concerns affect patients’ willingness to disclose information (Sankar, Moran, Merz, & Jones, 2003). Confidentiality protections are essential to preventing information from being withheld; health care settings often provide literature for patients to read on confidentiality. However, discussing, advertising, and reinforcing a confidentiality policy could go a long way toward creating a trusting environment and encouraging honesty (Shaw, Tomlinson, & Higginson, 1996). Additionally, alternative screening methods could be tested for their effect on rates of smoking disclosure; research in this area is needed.
Because smoking affects a variety of health conditions, contributes to overall poor health, and increased morbidity and mortality, this study has broad clinical implications. To promote better health and well-being and optimize treatment of all physical and mental health conditions, disclosure of smoking to HCPs is essential. Smokers should be encouraged to be forthright about their smoking so practitioners can offer treatment and services that increase cessation and reduce the burden of tobacco-related death and disease.
Footnotes
Authors’ Note
Laurel Erin Curry was affiliated with Legacy at the time of research and writing of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Data collection for this study was supported by a grant to Legacy from Pfizer, Inc. Laurel Curry, Amanda Richardson, and James Xiao received salary support from the grant for time spent on the project; however, Pfizer did not support the authors in the writing of this manuscript.