
Abstract
Objective. To further conceptualize and operationalize patient activation (PA), using measures from patient, physician, and researcher perspectives. Data Source/Study Setting. Multimethod observation in 2010 within a family medicine clinic. Study Design. Part of an intervention with 130 patients with type 2 diabetes, this observational study further looked at PA in 19 physician–patient dyads. Data Collection. Observations occurred in a teaching hospital, which served as recruiting and study site. Principal Findings. PA correlated with knowledge, self-efficacy, promotion orientation, and exercise intent. Patient-reported PA did not correlate with researcher-observed or physician-reported PA behavior. Researcher-observed PA correlated with physician-observation items. Conclusions. Results provide evidence for measuring different perspectives in studies of PA. When patients report they are activated in self-management, behavior does not indicate they are active in clinical communication, a critical component of collaborative decision making.
The chronic care model proposes that positive clinical outcomes are the result of an informed, activated patient (Wagner et al., 2001), who believes that his or her role as a patient is important, who has the confidence and knowledge necessary to take action, and who enacts behaviors to maintain and improve his or her health, even under stress (Hibbard, 2009a, 2009b; Hibbard, Greene, & Tusler, 2009; Hibbard, Mahoney, Stockard, & Tusler, 2005; Williams et al., 2005). These patients take action, ask questions of the provider, and participate in decisions about treatment (Cortes, Mulvaney-Day, Fortuna, Reinfeld, & Alegria, 2009; Griffin et al., 2004). Cortes et al. (2009) emphasize this conceptualization of patient activation as a skill-building process (Cortes et al., 2009). Hence, activated patients are collaborative partners with the provider in their health care (Hibbard, Mahoney, Stock, & Tusler, 2007). Patient activation is especially critical in chronically ill patients as they follow complex treatment regimens, monitor their conditions, and make lifestyle changes (Hibbard et al., 2005).
Proposed by Hibbard et al. (2004), the Patient Activation Measure (PAM) intends to capture an individual’s level of activation (Hibbard, 2009a, 2009b; Hibbard et al., 2005; Hibbard et al., 2009; Hibbard, Stockard, Mahoney, & Tusler, 2004; Williams et al., 2005). The self-reported PAM is associated with self-management behaviors, medication adherence, patient satisfaction, and quality of life (Harvey, Fowles, Xi, & Terry, 2012; Mosen et al., 2007). Within a diabetes-specific population, PAM is not related to knowledge regarding glycosylated hemoglobin (A1c—the standard measure of average blood glucose level; Rask et al., 2009) but is associated with better glycemic control (Rogvi, Tapager, Almdal, Schiøtz, & Willaing, 2012).
Although most clinicians are less familiar with the formal concept of patient activation, they have long seen presumed correlates of patient activation as significant factors in effective management of chronic disease (DiMatteo, 2004), issues such as medication compliance (Bell et al., 2011; Muntner et al., 2011), follow-up care (Mirotznik, Ginzler, Zagon, & Baptiste, 1998), and poor communication have been well documented as impediments in the care of chronic disease states. Specifically in the context of clinic communication, physicians communicate differently with patients who they perceive to be more active in clinic interactions (Street, Gordon, & Haidet, 2007). Bodenheimer (2005) recommends “pre-activating” patients prior to clinical encounters. Here, the concept of pre-activation tangibly includes rigorous follow-up and active, targeted communication from the health care team (Bodenheimer, 2005). Numerous interventions to include educational programs (Li et al., 2011), care coaching (Lin et al., 2012), and motivational interviewing (Linden, Butterworth, & Prochaska, 2010) have been attempted to improve this perceived activation with varied success. However, these efforts have rarely been tailored to potential intrinsic differences in how the patients approach their disease state.
Related Theoretical Concepts
Defined briefly as knowledge, skills, and confidence to self-manage health, patient activation is expected to associate with other similar concepts, specifically self-efficacy and promotion orientation.
Self-efficacy
Within social cognitive theory (Bandura, 2004), self-efficacy along with knowledge, outcome expectations, health goals, facilitators, and impediments are determinants of health behavior. Self-efficacy refers to a person’s belief of being capable to successfully perform a behavior (Bandura, 1986). In this study, the patient needs to believe that he/she can walk as exercise to help manage his/her diabetes. This concept relates to the PAM’s intended capture of a patient’s confidence level in self-management.
Regulatory focus
From a personality-trait perspective, individuals are either pervasively focused on hopes and aspirations and pursue goals that seek advantages (promotion oriented) or focused on duties and obligation and pursue goals that avoid disadvantages (prevention oriented; Higgins, 1997; Rothman, Bartels, Wlaschin, & Salovey, 2006). Promotion-oriented individuals aspire to an ideal self and are motivated by accomplishments, hopes, and aspirations, whereas prevention-oriented individuals are concerned with safety, duties, and obligations (Higgins, Idson, Freitas, & Molden, 2003). In the context of health behavior, promotion-focused individuals perform health behaviors in pursuit of an ideal self, whereas the prevention-focused individual performs health behaviors to prevent negative consequences. Using the language of social cognitive theory (Bandura, 2004), activated patients here may pursue management of their diabetes as a goal, reflecting a promotion orientation.
As components of patient activation, the following conceptual relationships are hypothesized. One hypothesis addresses the knowledge component of patient activation.
Hypothesis 1: PAM will positively correlate with knowledge of the benefits of walking on diabetes management.
Two hypotheses address the skills component of patient activation.
Hypothesis 2: PAM will positively correlate with self-reported baseline exercise behavior.
Hypothesis 3: PAM will positively correlate with intent to adhere to physician’s exercise recommendation.
Three hypotheses address the confidence component of patient activation.
Hypothesis 4: PAM will positively correlate with self-efficacy regarding diabetes self-management.
Hypothesis 5: PAM will positively correlate with self-efficacy regarding walking exercise.
Hypothesis 6: PAM will positively correlate with individual promotion orientation (regulatory focus).
Furthermore, this study explored the concept of patient activation from two others’ perspectives, focusing on verbal behaviors to capture patients’ role in information exchange, control, support, and decision making (Street, 2001). We examined how the patient-reported activation measure corresponds with physician perception and researcher perception of patient activation, asking the following research questions:
Research Question 1: How does the patient (self-reported) activation measure compare with physician perceptions of patient activation?
Research Question 2: How does the patient (self-reported) activation measure compare with a third-person (researcher) perception of patient activation?
Research Question 3: How do physician perceptions of patient activation compare with a third-person (researcher) perception of patient activation?
This multimethod investigation approaches the phenomenon of the activated patient with triangulation (Erzberger & Prein, 1997) of quantitative and qualitative data, of observed and self-report data, and of the three perspectives.
Method
Data collection was part of a larger prospective intervention study, which targeted patients with type 2 diabetes and their walking behavior (Ledford, 2012). The single-site, prospective intervention study used a 2 × 3 factorial, nonequivalent comparison group quasi-experiment to evaluate two message design variables—gain/loss framing and presentation mode—as potential influencers of communication and adoption success, considering patient activation as an influencer of behavior adoption. Institutional review board approval was received through the intervention project.
Participants
This study focused on male and female patients with type 2 diabetes. Additional inclusion criteria were age (between 40 and 80 years of age) and absence of contraindications for exercise. The intervention was delivered on-site as part of regular primary health care at a metropolitan training hospital.
Sixteen licensed family medicine physicians participated in the study. Pairing with patient participants was random, though researchers purposely reassigned patients who were paired with their primary care physician. Physicians included 11 males and 5 females, who had provided an average of 8.50 years of patient care (SD = 6.53). Of these, 11 were staff and 5 were resident physicians.
Sampling for the audio-recorded data collection was random, inviting the third patient appointment of each day to participate. All patients invited to participate in audio-recording consented.
Procedures
Following informed consent, participants completed a pre-intervention survey, assessing relevant knowledge, attitudinal, and behavior variables. Then, physicians presented the standard of care exercise recommendations during a clinical appointment (American Diabetes Association, 2012). Appointments were structured to include the exercise recommendations for patients with type 2 diabetes, strategies for including exercise in daily life, patient education about the A1c measure, and goal setting. The physician also gave the patient a printed handout to take home.
Immediately after the appointment, the participant completed a postintervention survey, assessing knowledge, attitudinal, and intent measures. The physician also completed a survey, recording perception of patient’s appointment communication.
Measures
For all appointments, physician (gender, years practice, staff or resident) and patient (gender, age, ethnicity, and education) demographics were recorded. The length of the audio-recorded appointments (in minutes and seconds) was also documented. Patient physiological measures included body mass index (BMI) and A1c.
Patient activation
The licensed PAM, developed by Hibbard et al. (2004), determined to be a reliable, valid, and potentially clinically useful measure (Hung et al., 2012; Skolasky et al., 2011), was used to assess participants’ patient activation prior to intervention. A proprietary scoring system uses 13 items to create a continuous PAM on a scale of 0 to 100 (Hibbard et al., 2005).
Knowledge, self-efficacy, and regulatory focus
Four sets of measures were included to explore relationships with the self-reported PAM. Three Likert-type items combined for the knowledge scale. Items included “Walking helps my heart and bones get strong,” “Walking relieves stress,” and “Walking improves my blood circulation.” A self-efficacy measure (Naik, Kallen, Walder, & Street, 2008) was adapted to diabetes management behavior. Self-efficacy in relation to walking exercise was assessed using confidence items (Marcus, Selby, Niaura, & Rossi, 1992). Promotion orientation was measured using a previously validated regulatory focus promotion-orientation Likert-type scale (see Appendix for scale items; Lockwood, Jordan, & Kunda, 2002).
Intention and behavior
At the initial survey, patient exercise behavior was assessed with a self-reported item, recording minutes exercised each day of the previous week; this measure combined two physical activity measures used by the Health Information National Trends Survey (Oh et al., 2010). Following the intervention, two Likert-type items (“I plan to. . . ” and “I will. . . ”) addressed behavioral intention.
Physician-perceived activation
Following the appointment, the physician assessed patient activation in the appointment with two Likert-type items. The first item, “The patient ‘forced’ me to go off message, crossing gain/loss frame,” assessed how a patient challenged the intervention’s framing of the exercise messages. This included physician perception of patients’ request for a restatement or clarification of recommendations. The second item, “The patient was active in discussion and asking questions,” was less ambiguous, assessing the physician’s perception of patient communication behavior in the interaction.
Researcher-observed activation
The first and second authors used theoretically driven, inductive coding to develop a taxonomy of patient activation behaviors (Bradley, Curry, & Devers, 2007; Glaser, 2002; Glaser & Strauss, 1967). Investigators conducted an open coding process and analyzed transcripts line by line and recorded conceptual codes as they emerged (Strauss & Corbin, 1998). The unit of analysis for coding was each patient statement. Axial coding then related subcategories and further developed categories. The constant comparative method was used to saturate categories (Conrad, 1978; Glaser & Strauss, 1967; Morse, 1995).
The resulting taxonomy of patient activation behaviors included nine categories: Patient seeks information or asks questions, patient expresses preferences, patient presents patient-obtained medical information, patient engages in conversation (nonmedically related), patient states goal, patient teaches back, patient provides detailed health information, patient relays experience of a salient other, and patient reports therapeutic behaviors.
The first and second authors then recoded all data with this final code structure and resolved any disagreement by joint consensus (Bradley et al., 2007). Each activation statement was recorded as one point toward an activation score, resulting in a researcher-observed activation score for each patient.
Results
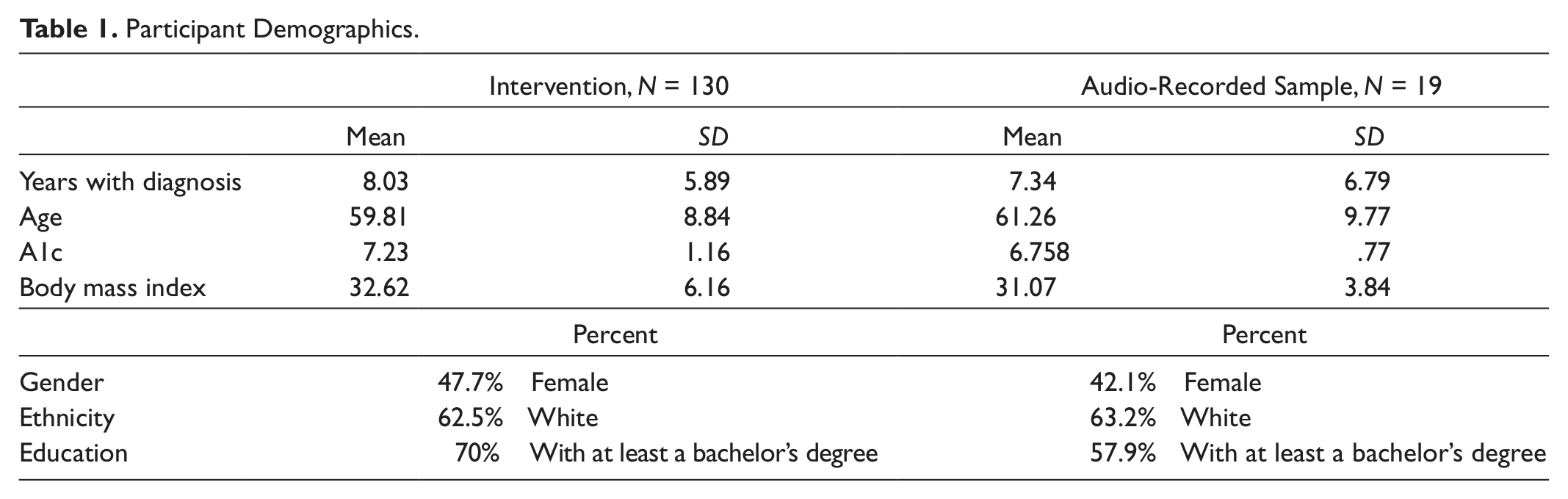
Recruitment letters were mailed to 1,520 patients with type 2 diabetes. Throughout recruitment, 142 patients volunteered to participate. Of these, 130 patients attended clinic appointments and completed pre- and postintervention surveys. Nineteen patient encounters were successfully recorded and transcribed. Table 1 presents patient demographics. Additionally, 92 patients (70.8%) reported other chronic medical concerns.
Participant Demographics.
Patient Activation
For this sample, the 13 item PAM had internal consistency, α = .851. The mean PAM score was 51.30 (SD = 11.41). PAM did not correlate to age, years with a diabetes diagnosis, or A1c at baseline. Cross-tabulation chi-squares also revealed no differences in gender, ethnicity, or education. However, PAM negatively correlated with BMI (r = −.203, n = 117, p < .05).
Hypothesis testing
Supporting Hypotheses 1, 3, 4, 5, and 6, PAM positively correlated with knowledge about walking’s benefits (r = .219, n = 128, p < .05), intent to walk (r = .297, n = 124, p < .001), self-efficacy regarding diabetes management (r = .275, n = 127, p < .005), self-efficacy regarding walking (r = .395, n = 126, p < .001), and promotion orientation (r = .267, n = 128, p < .005). However, results did not support the second hypothesis, which proposed a relationship between PAM and self-reported baseline exercise behavior. Table 2 presents PAM correlations.
Correlation Matrix of Hypothesized Patient-Reported Variables.

Correlation is significant at the .01 level (two-tailed). *Correlation is signification at the .05 level (two-tailed).
Physician-Perceived Activation
For the restatement/clarification item, the mean response was 1.99 (SD = 1.31), where 1 = strongly disagree to 7 = strongly agree. There was no relationship with age, years with a diabetes diagnosis, BMI, or A1c at baseline. There were also no differences in ethnicity or education; however, physicians reported female patients asked for restatement/clarification significantly more than male patients, F(1, 124) = 3.970, p < .05.
For the patient communication behavior item, the mean response was 5.32 (SD = 1.41). There was no relationship with years with diagnosis or A1c; however, physician-perceived patient communication did correlate with age positively (r = .184, n = 126, p < .05) and BMI negatively (r = −.203, n = 115, p < .05). There were no differences in gender, ethnicity, or education.
Researcher-Observed Activation
The mean score for researcher-observed patient activation measure (ROPAM) was 4.00 (SD = 3.27). Table 3 summarizes scores within the PA taxonomy.
Researcher-Observed Patient Activation Taxonomy and Scores (From Most Frequent to Least; N = 19).

ROPAM was not related to years with a diabetes diagnosis, BMI, or A1c at baseline. However, ROPAM did correlate with age (r = .456, n = 19, p < .05). There were no differences in gender, ethnicity, or education.
Appointment length also correlated with researcher-observed PA (r = .549, n = 17, p < .05). For audio-recorded appointments, the average length was 6.91 minutes (SD = 2.75). This length seems appropriate considering average face-to-face patient care in family medicine appointments is 10.7 minutes (Gottschalk & Flocke, 2005).
Research Questions
Patient report and physician perception
A Pearson product–moment correlation coefficient was computed to assess the relationship between the patient-reported PAM and the two physician perception measures. Neither physician measure correlated with PAM.
Patient report and researcher observation
A Pearson product–moment correlation coefficient was computed to assess the relationship between the patient-reported PAM and researcher-observed PA. The variables did not correlate.
Physician perception and researcher observation
A Pearson product–moment correlation coefficient was computed to assess the relationship between physician perceptions and ROPAM. Researcher-observed PA correlated with each physician-observation item, restatement/clarification (r = .670, n = 15, p < .005), and patient communication (r = .572, n = 15, p < .05).
Conclusion
In the clinical setting, the PAM is a reliable, valid measure of knowledge and confidence related to promotive individual health behaviors. Results here also support the conceptualization of patient activation as related to self-efficacy and intention to comply with physician’s promotive messages.
Additionally, results extend previous findings that physicians communicate differently with activated patients (Street et al., 2007). However, results did not replicate findings that activation is related to the self-management behavior of interest here, exercise.
The PAM, however, is not capturing a subset of behaviors integral to clinical communication and decision making. More specifically, while we acknowledge that the PAM is associated with favorable clinical outcomes, its application to patient–provider interaction is not as readily apparent. Physicians are not inherently capable to reliably assess patient activation within the time constraints of a clinical encounter, based solely on the communication that occurs in that setting.
Although PAM is related to these other self-reported measures, results here identify a discrepancy between self-reported PAM and physician-perceived and researcher-observed PA. Results here provide evidence for measuring different perspectives in studies of PA. Although patients may report they are activated in chronic care management, behaviors do not indicate they are active in clinical communication, a critical component of collaborative decision making. More research is needed on the in-clinic profile of a patient, specifically and how PAM is enacted and perceived by the physician in both the acute clinic and long-term care settings.
Conversely, even activated patients can benefit from programs to increase physician–patient communication (Lu, Deen, Rothstein, Santana, & Gold, 2011), such as “Ask Me 3.” Efforts to increase patient activation need to reach beyond communication skills training to a wider set of attitudinal and behavior concepts.
Footnotes
Appendix
Acknowledgements
The authors would like to acknowledge Anthony Bennett for his expert direction of clinic workflow and patient relations.
Authors’ Note
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the U.S. Army, U.S. Air Force, the Uniformed Services University of the Health Sciences, or the Department of Defense at large.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.