
Abstract
Parents play a fundamental role in teaching their children safe driving skills to reduce risk of motor vehicle crashes, the leading cause of death for teens. Steering Teens Safe is a new parent-based intervention that equips parents with communication skills to talk about, demonstrate, and practice safe driving behaviors and skills with their teens. This implementation evaluation focuses on a sample of 83 parents who delivered Steering Teens Safe to their teens. One-, 2- and 3-month follow-up assessments were conducted with intervention parents to evaluate the self-reported quantity and quality of talking about, demonstrating, and practicing safe driving goals with teens; perceived success and benefit of the program; and barriers to implementation. Over 3 months of follow-up, parents discussed driving goals with their teens for a median of 101.5 minutes. The most frequently addressed topics were general safety principles, including distracted driving, driving in bad weather, wearing a seat belt, and being a safe passenger. Parents spent a median of 30 minutes practicing safe driving skills such as changing lanes. Sixty-seven percent of parents talked to their children about rural road safety, but just 36% demonstrated and half practiced these skills with their teens. Barriers to implementation include time and opportunity barriers and resistant attitudes of their teens. However, barriers neither affected frequency of engagement nor parents’ perceived benefit and comfort in delivering the program. Parents with time/opportunity barriers also had higher practice and demonstration times than parents without these barriers. Findings indicate high acceptability among parent implementers and promise for real-world delivery. Future studies are needed to assess intervention impact.
Motor vehicle crashes are the leading cause of death for teenagers in the United States, accounting for more than 4,000 deaths in 2008 (National Highway Traffic Safety Administration, Department of Transportation, 2009). More than 350,000 teens receive medical care each year because of injuries sustained in crashes (Centers for Disease Control and Prevention, 2010). Driving errors such as distraction, tailgating, and speeding account for more than 95% of the most severe crashes (Curry, Hafetz, Kallan, Winston, & Durbin, 2011). Reducing the risk of crashes among teens is a public health priority, and a critical window for intervention is the first year of unsupervised driving when crash rates for teens are highest (Insurance Institute for Highway Safety, 2009; Simons-Morton & Ouimet, 2006).
Parents play a fundamental role in training their teens to adopt safe driving behaviors and reduce driving errors. This is particularly important during the pre- and provisional licensure period. Parents equipped with knowledge and skills can successfully teach their teens safe driving skills (Beck, Hartos, & Simons-Morton, 2002, 2006; Hartos, Beck, & Simons-Morton, 2004; Hartos, Shattuck, Simons-Morton, & Beck, 2004; Simons-Morton & Hartos, 2002; Simons-Morton, Hartos, & Beck, 2003; Simons-Morton, Ouimet, & Catalano, 2008). For example, parents may encourage their teen’s use of specific safety behaviors, such as seat belt use and not driving while distracted. Since these choices are often made when parents are not in the car with their teens, effective communication to motivate safe choices by the teen is important.
Despite their influential role, parents generally exhibit poor monitoring and control of their teen’s risky driving behaviors and fail to clearly define driving rules and expectations (Beck, Shattuck, & Raleigh, 2001; Hartos, Beck, et al., 2004; Hartos, Eitel, & Simons-Morton, 2001, 2002). The most common driving rules implemented by parents regard permission to use the car, where the teen was going, and when the teen will be home (Hartos, Shattuck, et al., 2004), none of which directly involve driving safety. In addition, rules are poorly communicated and understood between parents and teens. In a survey of teens and parents, only half the driving rules were in agreement and nearly a third were “understood” rather than explicitly stated or in writing (Hartos, Shattuck, et al., 2004). To address this discordance, intervention approaches that consider parental influence through parent–adolescent communication are needed (Jaccard & Turrisi, 1999).
Steering Teens Safe is a parent-based teen driving program grounded in health behavior and family communication theory. In this study, we describe the components of this intervention and conduct an implementation evaluation of parents who delivered this program to their teens. These findings will ascertain how implementers (i.e., parents) accept and engage in this new teen driving intervention program.
Theoretical Framework
Steering Teens Safe was developed using social cognitive theory (Bandura, 1986) and family communication theory and literature on parent involvement and teen safe driving behavior. Accordingly, teens’ safe driving behaviors are influenced by individual determinants (e.g., the teen’s own knowledge, attitudes, and driving skills), environmental determinants (e.g., their parents’ belief, values, and safe driving behaviors), and the interactions between parents and teens (e.g., parents’ communicating about, demonstrating, and practicing safe driving with their teens). As such, parents are instructed to be a role model for their teens in how they demonstrate safe driving skills. Because effective family communication is an avenue through which parents could positively influence teen behaviors, we developed a program that provides instructions and strategies on effective parent–teen communication about safe driving guided by motivational interviewing (MI) techniques. MI is a communication-based behavioral approach applied to smoking cessation, improving diet, and reducing sexual risk taking among teens (Berg-Smith et al., 1999; Heckman, Egleston, & Hofmann, 2010; Karofsky, Zeng, & Kosorok, 2001; Miller, Levin, Whitaker, & Xu, 1998; Suarez & Mullins, 2008). Our final intervention program contained had two main components: (a) driving topics (presented as safe driving goals) that parents addressed with their teens and (b) effective communication styles for parents.
Intervention Content: Safe Driving Goals
The intervention contained four modules: General Driving Skills, Safe Driving Behaviors, Special Driving Situations, and Rural Roads. General Driving Skills included driving goals for judging distance to follow another car, safely making left turns, changing lanes, and how to drive in unfavorable conditions such as poorly maintained roadways. Safe Driving Behavior goals included wearing a seat belt, avoiding alcohol while driving, never riding in a car with an intoxicated driver, avoiding distractions (e.g., texting/talking on cell phone, loud music, talking with passengers) while driving, maintaining a safe speed, remaining vigilant while driving, and avoiding aggressive driving. Special Driving Situations included avoiding collisions with animals, driving safely in bad weather, and using emergency maneuvers. A special module on Rural Roads was developed, with goals for negotiating uncontrolled intersections, blind curves, narrow rural roads, gravel roads, and slow-moving farm vehicles. Driving goals were developed from literature on teen crashes and materials from the Iowa Department of Transportation. Parents were encouraged to cover all these driving goals but could choose which goals to prioritize and how much time to devote to each goal. This allowed for tailoring of the program to what parents believed to most important driving safety issues for their child.
Intervention Content: Communication Strategies
Parents were taught three steps to address each driving goal with their teen: talk about the goal, demonstrate the goal (e.g., modeling seat belt use), and practice the goal while the teen was driving with the parent. Parents learned to use MI techniques to deliver their messages.
For the talking phase, parents were instructed against lecturing, and were taught MI skills for interacting with their teens. First, they learned to use “OARS” (open-ended questions, affirmations, reflection, summary),” a mnemonic used to remind parents of these MI techniques. Parents also learned “rolling with resistance” to help address teen attitudes about driving safety.
For the demonstration phase, parents were instructed to discuss driving goals while actively demonstrating them. For example, while changing lanes, a parent could question his or her teen about appropriate methods for safely completing this skill. The teen was encouraged to consider the skills required for changing lanes (e.g., maintaining safe speed, scanning, signaling, and maneuvering safely to the next lane). For safe behaviors, a parent was instructed to ask questions about the behavior (e.g., wearing a seat belt) while driving. The parent could then ask, “Do you think that if I crashed right now, I would benefit from having my seat belt on? Why or why not?” In the practice phase, the parent supervised the teen while practicing a skill. The parent reinforced messages by asking teens about what they were doing and why it was important.
Intervention Delivery and Materials
Parents received a guidebook with driving goals and talking points, worksheets for tracking progress, a video with sample conversations between a parent and teen, a pocket guide describing the OARS skills, and an information pamphlet designed by the Iowa Department of Transportation called “You’re the Coach: Guide for Parents of New Drivers.”
Parents were trained on Steering Teens Safe by a Traffic Safety Specialist who reviewed contents of the guidebook and video and demonstrated and role-played MI for driving safety goals. Trainings lasted approximately 1 hour.
Traffic Safety Specialists conducted follow-up phone calls with parents at 1, 2, and 3 months after trainings to assess progress on the driving goals, provide a booster training, and address challenges reported by parents.
Method
Study Participants
This implementation evaluation includes parent randomized to the intervention wing of a randomized controlled trial testing the effectiveness of Steering Teens Safe in improving parent–teen communications about safe driving. The source population was composed of parents from eight Iowa high schools located in and around the Des Moines and Iowa City areas and parents employed by the two hospitals located in the same geographic region. There were no significant differences in the demographics (age, gender, marital status, race, education, and employment) of parents from the two settings. Eligible participants were parents of a teen (or teens) at least 15 years of age anticipating an intermediate license within the next 3 months, which in Iowa represents the first opportunity for unsupervised driving. Subjects were recruited and enrolled into the study from 2007 to 2010 all year round.
Using passive recruitment methods, information about the program was sent home by mail to parents of freshmen and sophomores in the study high schools and by e-mail distribution to parents employed by the hospitals. Recruitment letters and e-mails included a phone number and e-mail address that parents could contact for enrollment. One parent was recruited for participation along with the new driver. Parental consent and teen assent were required. This study was approved by the University of Iowa Institutional Review Board.
Each enrolled parent was randomly assigned to the intervention or control group. Parents in the intervention group were the focus of this implementation evaluation study.
Implementation Evaluation
Often a missed step in evaluation studies, implementation evaluations are essential to determine how an intervention program was carried out (Sleet, Hopkins, & Olson, 2003). One approach recommended for process evaluations involves analysis of the characteristics and activities of the persons delivering the program (Linnan & Steckler, 2002; Saunders, Evans, & Joshi, 2005). Accordingly, in this study, we focused on parents (targeted implementers) and measured indicators to determine the quality and quantity of the intervention delivered to teens. Using a logic model, we identified process indicators for this implementation evaluation (Figure 1). The implementation process was first measured as the successful training provided to parents during by Traffic Safety Specialists. Immediately after completing their training, parents were asked to report their agreement with the following statements using a 5-point Likert-type scale where 1 = not agree at all and 5 = highly agree: “I understood the driving goals discussed by the Traffic Safety Specialist,” “The Traffic Safety Specialist assisted me in identifying challenges to meet driving goals,” “The Traffic Safety Specialist assisted in generating ideas to overcome these difficulties,” and “The session with the Traffic Safety Specialist increased my motivation to work on driving goals with my teen.”
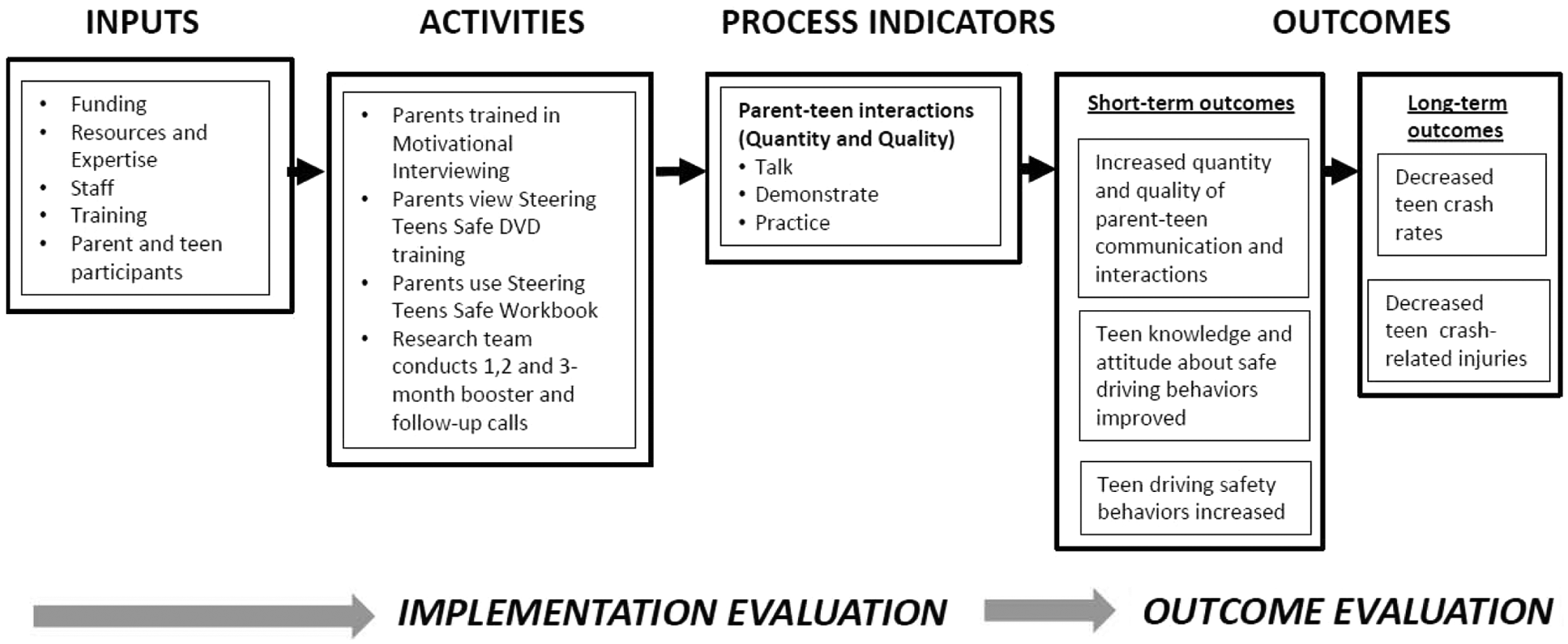
Logic model for evaluating Steering Teens Safe.
Another implementation indicator was the quantity of intervention sessions parents delivered to their teens related to 19 specific driving topics (5 topics on Safety Principles, 6 topics on General Driving Skills, 4 topics on Safe Driving Behavior, and 4 topics on Driving Skills on Rural Roads). Parents were asked to report how many sessions and minutes they engaged in three steps (talking, demonstrating and/or practicing) for each individual driving topic at 1-, 2- and 3-month follow-ups. Because talking, demonstrating, and practicing may not be mutually exclusive, sessions and minutes were not additive. This allowed us to monitor longitudinally the progress of each intervention parent in meeting programmatic goals (i.e., increased engagement with their teens).
The next implementation outcome was the quality of the intervention sessions parents delivered to their teens. During follow-up, parents were asked to report the success of each topic-specific conversation with their teen using a scale of 1 to 10 where 1 = not at all successful and 10 = very successful. Parents were also asked to provide an overall perceived benefit of and comfort in using MI skills using a similar 1 to 10 rating scale. Finally, parents responded to an open-ended question about any barriers encountered while talking, demonstrating, and/or practicing.
Traffic Safety Specialist used a Driving Goals Inventory Form to collect these data from parents at 1-, 2- and 3-month follow-ups.
Analysis
Implementation data reported for each of the 19 driving topics were graphed and then summed across 1-, 2- and 3-month follow-ups. Programmatic barriers, collected in open-ended format, were first coded using content analysis. As such, themes that emerged from analysis of text responses were developed into distinct categories. Simple descriptive statistics (frequency and percent) were used to describe the distribution of categorical data (e.g., types of barriers reported), and means and medians were reported for continuous measures (e.g., minutes and success ratings). Minutes of engagement and success ratings were compared between parents with and without reported barriers using a t test or Wilcoxon rank–sum test depending on the normality of the data.
Results
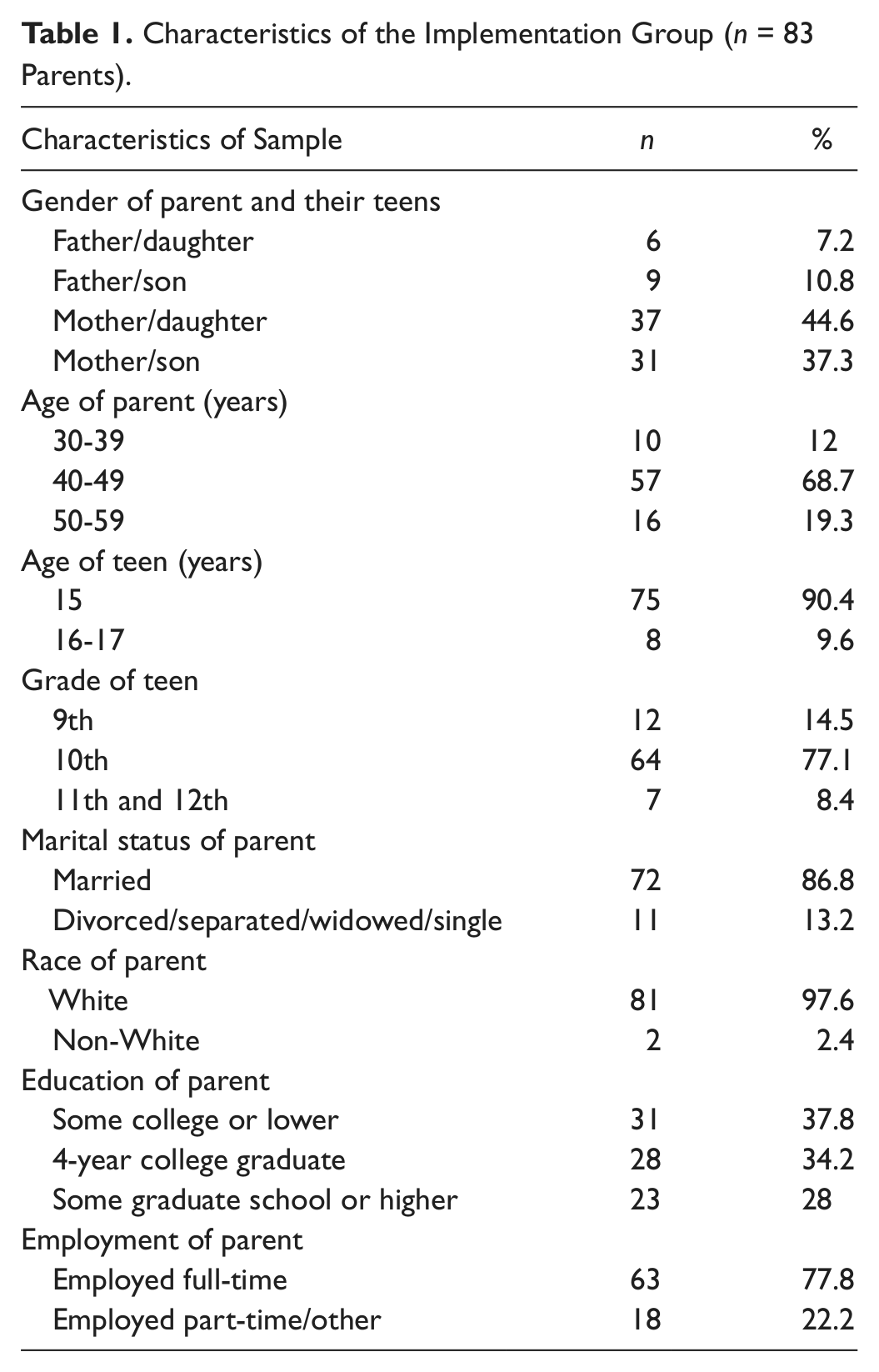
A total of 83 parents received the Steering Teens Safe intervention (Table 1). Intervention parents were mostly mothers (81.9%), married (86.8%), and White (97.6%), with some college education and employed full-time (77.8%). We also collected information about the teens targeted to receive the intervention from their parents. About half the participating teens were male, and the majority were 15 years old (90%.4) and in 10th grade (77.1%).
Characteristics of the Implementation Group (n = 83 Parents).
Implementation Indicators
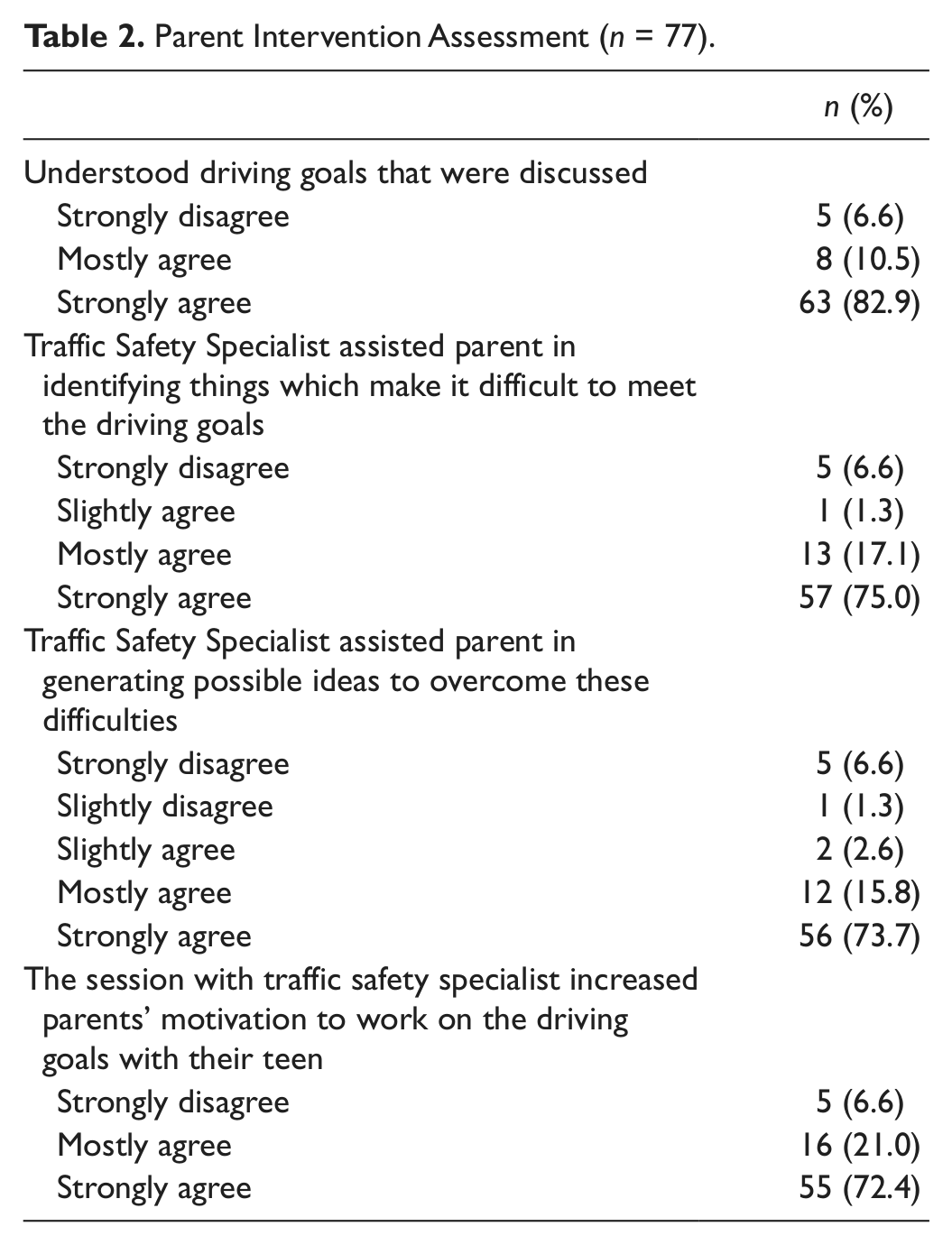
Of the 83 enrolled parents, 77 completed assessments about their Steering Teens Safe training sessions. More than 93% strongly agreed that they understood the driving goals. Almost all parents (93%) reported that the Traffic Safety Specialist increased parental motivation to work on the driving goals with their teen (Table 2).
Parent Intervention Assessment (n = 77).
Parents reported engaging in a median of 55 minutes of talking, 26 minutes of demonstrating, and 40 minutes of practicing during the first month (Figure 2). Minutes of talking, showing, and practicing decreased slightly through follow-up, but the number of sessions of interaction remained relatively stable. During the first month, parents spent more time talking (median = 55 minutes; nine sessions) than demonstrating (median = 25.5 minutes; six sessions) or practicing driving goals with their teen (median = 40 minutes; eight sessions). By the third month, parents were equally talking, demonstrating, and practicing driving goals, with a median range of 22 to 25 minutes. Anecdotally, parents indicated that after 3 months, they often talked while demonstrating or while the teen was practicing. Thus, these minutes are not additive.
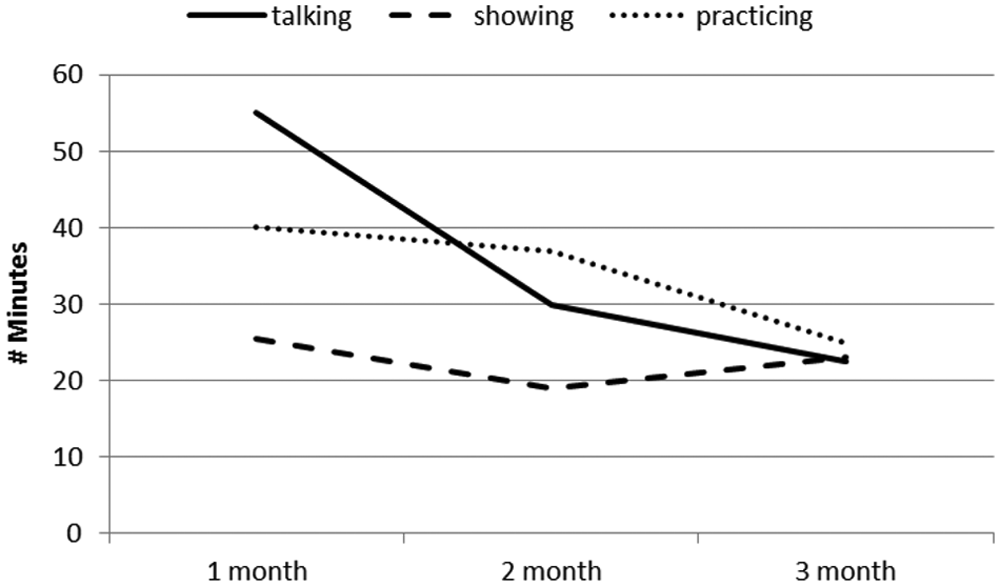
Median number of minutes parents talked, showed, and practiced with their teen.
Table 3 shows how frequently specific driving goals were talked about, demonstrated, and practiced aggregated across 1-, 2- and 3-month follow-ups. The median number of minutes that parents spent discussing all driving goals over the entire 3 months was 101.5 minutes. Goals related to safety principles were most frequently discussed by 89.6% of parents within a median of 39 minutes. Safety topics included avoiding distractions (84.4%), wearing a seat belt (53.2%), and being a safe passenger (54.5%). The 83% of parents who talked about special driving situations spent a median of 24 minutes doing so; the most common topic was driving in bad weather (62.3%) and the least common topic was emergency maneuvers (e.g., avoiding work zone crashes or moving out of the way for emergency vehicles; 24.7%). Complex driving goals such as taking the job of driving seriously (median = 12.5 minutes) and driving in bad weather (13.0 minutes) were discussed more frequently than safety behaviors such as wearing a seat belt or changing lanes (median = 6 minutes).
Average Number of Minutes Parents Talked, Demonstrated, and Practiced Driving Lessons With Their Teens (Across 3 Months; n = 77).
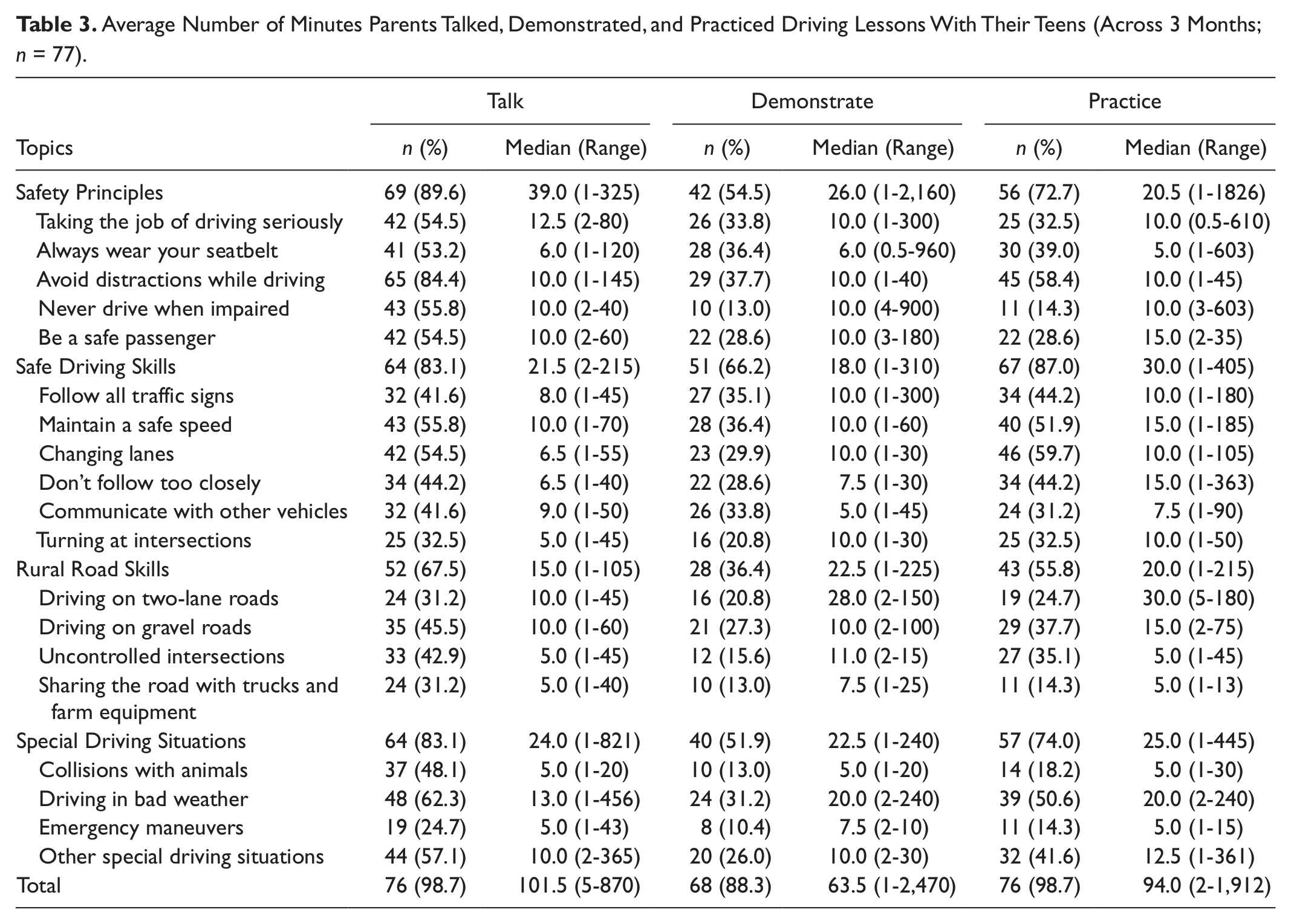
Parents spent the most time throughout the intervention practicing safe driving skills (median = 30.0 minutes), compared with showing (median = 18.0 minutes) and talking (median = 21.5 minutes). About 87% of parents practiced safe driving skills with their teen, and more than 66% demonstrated these skills. Changing lanes was the most commonly practiced skill (60%), with a median of 10 minutes practice time. Communicating with other vehicles (turn signals, break lights, eye contact) was least frequently practiced (31.2%), with a median of 7.5 minutes of practice time.
Rural road safety, although the least frequently addressed topic, was still talked about by 67.5%, demonstrated by 36.4%, and practiced by 55.8% of parents. Of all rural road topics, sharing the road with trucks and farm equipment was practiced by only 14.3% teens. Parent–teen dyads also spent only a median of 5 minutes talking about and 7.5 minutes demonstrating how to share roads with trucks and farm equipment. However, the comparatively few parents (21% to 31%) who addressed driving on two-lane roads still spent a median of 28 minutes demonstrating and 30 minutes practicing with their teens; these were among the highest median demonstration and practice times.
Barriers to Implementation
Time/opportunity barriers were reported by more than half of all parents while talking (55.8%), demonstrating (70.1%), and practicing (70.1%; Table 4). One parent reported challenges in finding “time to show the different driving conditions,” because “activities at school take a lot of teen’s time.” Practicing skills such as driving on rural roads was hampered by lack of time and opportunity. “Opportunities to drive long distances are few,” indicated one parent. Another parent reported “not having had any experience with rural roads.” However, the most common barrier to talking about driving goals was the attitude of teens. One parent said, “My son is a great kid, but like many teens, thinks he knows all he needs to know about driving. I think he found the talking like an assignment and boring.” Despite these challenges, few parents indicated the program posed specific programmatic challenges. For example, only one parent reported difficulty remembering to refer to the parent guidebook.
Average Minutes and Success Ratings for Talk, Demonstrate, and Practice Questions by Barriers (Across 3 Months; n = 77).

Parents with time/opportunity barriers had a lower median number of talking minutes (98 minutes) than parents without time/opportunity barriers (108 minutes), but this difference was not statistically significant (p = .777). Interestingly, parents with time/opportunity barriers reported higher demonstration and even significantly higher practice times than parents without this type of barrier (Table 4). Parents with these barriers practiced driving goals for a median of 139 minutes, whereas those without barriers practiced only 34 minutes with their teens. Parents with attitude barriers did report lower median talking, demonstration, and practice times than parents without this barrier; however, these differences were not significant (p = .598). Median success ratings (8.2-9.0) for talking, showing, and practicing were mostly comparable between parents with and without any type of barriers. The only significant difference was found among parents when talking with their teens: Parents who encountered attitude barriers reported lower success rates in talking than parents without this type of barrier.
Despite encountering barriers, parents reported being very comfortable using MI to discuss driving goals with their teens (mean = 8.3, range = 1.0-10.0; Table 5). Furthermore, parents perceived MI to be beneficial in teaching their teens to drive safely (mean = 8.0, range = 2.0-10.0). In fact, parents with barriers had either slightly higher or similar ratings of comfort and benefit than parents without barriers (p = .106).
Benefit and Comfort Level in Using Motivational Interviewing Skills Reported Among Parents With and Without Barriers (Across 3 Months; n = 76).

Note. Scale from 1 to 10 (1 = not at all beneficial/comfortable, 10 = very beneficial/comfortable).
Discussion
An implementation evaluation is a first step in a comprehensive evaluation effort and aids in understanding the relationship between specific program elements and program outcomes (Saunders et al., 2005; Steckler & Linnan, 2002). In this study, we focused on whether the intervention components were acceptable and satisfactory by parents and how the intervention content was delivered to teens by parents
We learned that Steering Teens Safe was widely accepted by parent implementers, who were successfully trained and engaged in talking, demonstrating, and practicing safe driving skills with their teens. Coupling three teaching tools (i.e., talking, demonstrating, and practicing) with simple communication techniques is an innovate approach to safe teen driving. The few existing interventions traditionally provided during the prelicensure period have focused on supervised practice without talking and demonstrating and without guidance on specific driving skills and safety behaviors to target (Gregersen, Nyberg, & Berg, 2003; Page, Ouimet, & Cuny, 2004). Steering Teens Safe equips parents with communication skills, responding to a need for including parental communication to reduce teen risky driving (Beck, Hartos, & Simons-Morton, 2005; Ginsburg, Durbin, García-España, Kalicka, & Winston, 2009).
During implementation of our intervention, parent and teens interacted to varying degrees. Talking and practicing were the most frequent intervention activities, lasting minutes to several hours. Over time, parents engaged in less minutes of talking, showing, and practicing; yet the number of talking sessions in particular remained relatively constant. These findings describe a natural progression—that conversations and demonstrations about driving behaviors are initially long and frequent but become shorter and perhaps more efficient as teens increase their practice trips and independent driving. These results also suggest that high levels of talking and demonstrating be delivered during the prelicensure period and especially before a teen begins practicing his or her driving skills. With time, we expect teens would begin to adopt safety skills and behaviors discussed and practiced well before independent driving.
This implementation evaluation identified the most and least common driving goals addressed by parents. In general, safety principles were most frequently discussed and demonstrated by parents, but safe driving skills were most frequently practiced by teens. Findings also suggest that more time is required to discuss complex and broad issues such as being a safe driver (e.g., taking the job of driving seriously, avoiding distractions while driving) and using emergency maneuvers. Certain driving skills and behaviors, such as emergency maneuvers and encountering animals, were often not shown and practiced unless natural opportunities arose. Surprisingly, less time was spent to discuss, demonstrate, and practice safety behaviors such as wearing a seat belt or skills such as not following too closely. The optimal amounts of discussions, demonstrations, and practice times and sessions are not yet known, and further assessments of this intervention must include outcome evaluations of effectiveness that accounts for differential deliveries of quantity, quality, and content.
Unlike existing teen driving programs, ours provides a unique teaching module on rural road skills. About half of the teens in our study received exposure to rural road safety instruction. However, 32% to 64% of our teens had no discussion, practice, or demonstration on rural road skills, although our sampling indicates that these teens will spend at least some time driving on rural roads. Qualitative results suggest that opportunities to drive on rural roads were few for some parents, with some indicating not having yet driven in the rural countryside. The long stretches of rural roads in Iowa and across the country are hard to avoid and without adequate parental instruction could be extremely dangerous for the novice driver (Peek-Asa, Britton, Young, Pawlovich, & Falb, 2010). Parents may not be aware of this increased risk and are not actively seeking opportunities to address these risks with their teen drivers. Future delivery of our intervention should therefore include focused encouragement of parents to discuss rural road issues and bring their teens on rural roads for demonstration and practice.
Parents reported other barriers to implementing programmatic activities, such as difficulty finding time to interact with teens and resistant attitudes of their teen. However, we learned that parents with barriers still engaged in relatively high frequencies of communication and driving with their teens and indicated high success rates in using MI communication techniques. In fact, parents who reported time barriers had significantly increased engagement with their teens. There are a number of possible reasons for this counterintuitive finding. First, it may be possible that the threshold amount of engagement is achieved at relatively lower frequencies of communication and driving. Second, the reporting of time barriers may have been more obvious to the parents who attempted to create more opportunities for interaction, implying that the time barrier may be a symptom of engagement rather than a barrier to implementation.
Our study has a number of limitations. Our small sample of parents who self-selected into this study were likely of higher socioeconomic status and more concerned about teen driving safety compared with all parents of teens as seen in previous literature (Simons-Morton, Hartos, Leaf, & Preusser, 2005). However, this first implementation of Steering Teens Safe in a rural state provides promising results for further work that may involve translation to other communities across the country. Only one parent participated as implementers, and another parent or family member could have affected the delivery of the intervention or, in some cases, provided conflicting messages to teens. All implementation data were self-reported by parents to our Traffic Safety Specialist, and thus, they are prone to possible underreporting and recall bias. Furthermore, because the objective of this study was to examine the ability of parents, the targeted implementers, to be trained and to deliver Steering Teens Safe, we did not focus on teen indicators. Given our results that parents were engaged implementers, the next steps in evaluation will involve examining the impact of the intervention in improving driving outcomes among teens and comparing teen–parent interactions in the randomized controlled trial.
Implications
In summary, this evaluation shows that parents can be taught communication approaches for teaching safe driving to their teens. Our intervention has promise as it engaged parents in delivering substantive minutes’ to hours’ worth of talking, showing, and practicing with their teens. These findings suggest important translatability for real-world implementation. Future studies are needed to effectively deliver Steering Teens Safe into practical settings. Also, the next steps are outcome evaluation studies that measure the intervention impact on teen-specific indicators such as decreased crash errors and increased safety behaviors.
Footnotes
Acknowledgements
We express our appreciation to collaborators at Blank Children’s Hospital, Des Moines, Iowa. We acknowledge the invaluable contributions of the school personnel, parents, and students in study schools who were involved in this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This research was funded by the National Center for Injury Prevention and Control at the Centers for Disease Control and Prevention (R49 CE000947).