
Abstract
Objectives. To explain vaccine confidence as it related to parents’ decisions to vaccinate their children with recommended vaccines, and to develop a confidence measure to efficiently and effectively predict parents’ self-reported vaccine behaviors. Method. A sample of parents with at least one child younger than 6 years (n = 376) was analyzed using data from the HealthStyles 2010 survey. Questions were grouped into block variables to create three confidence constructs: value, safety, and efficacy. Regression equations controlling for demographic characteristics were used to identify the confidence construct(s) that best predicted parents’ self-reported vaccination decisions (accept all, some, or none of the recommended childhood vaccines). Results. Among the three constructs evaluated, confidence in the value of vaccines, that is the belief that vaccines are important and vaccinating one’s children is the right thing to do, was the best predictor of parents’ vaccine decisions, F(2, 351) = 119.199, p < .001. When combined into a block variable for analysis, two survey items measuring confidence in the value of vaccines accounted for 40% of the variance in parents’ self-reported vaccine decisions. Confidence in the safety or efficacy of vaccines failed to account for additional significant variance in parent-reported vaccination behavior. Conclusions. Confidence in the value of vaccines is a helpful predictor of parent-reported vaccination behavior. Attitudinal constructs of confidence in the safety and efficacy of vaccines failed to account for additional significant variance in parents’ vaccination behaviors. Future research should assess the role of vaccine knowledge and tangible barriers, such as access and cost, to further explain parents’ vaccination behaviors.
In the past decade, there has been increasing concern about parents’ hesitancy to vaccinate their children according to the recommended schedule (Freed, Clark, Butchart, Singer, & Davis, 2010). Most parents are vaccinating their children, however most also have questions or concerns about childhood vaccines (A. Kennedy, LaVail, Nowak, Basket, & Landry, 2011). Measures have been developed to identify vaccine-hesitant parents, as well as their questions, concerns, and perceived barriers to vaccination (Opel, Mangione-Smith, et al., 2011; Opel, Taylor, et al., 2011). A key area of focus for those interested in vaccine hesitancy has been vaccine confidence; however, what the term represents has not been well defined. “Vaccine confidence” as a term has been used to represent a variety of different concepts, such as safety, necessity, and efficacy, limiting our understanding of the impact of different components related to vaccine confidence and vaccine hesitancy. It may not be helpful to think of vaccine confidence as part of vaccine hesitancy, but rather as its reverse, or the positive attitudes parents may have that help explain their choice to accept vaccination for their child.
This research sought to determine how different constructs related to vaccine confidence might predict vaccination behavior. A review of extant literature suggested three main interpretations of confidence: confidence in the safety of vaccines, confidence in the efficacy of vaccines, and confidence in the value of vaccines.
Safety
The reduced perception of threat from vaccine-preventable diseases (VPDs) has, in part, propagated an increased focus on the safety of vaccines themselves (Chen, 1999; Covello & Sandman, 2001; Salmon, Moulton, & Halsey, 2004). Real safety issues, such as the suspension of the first rotavirus vaccine approved for use in the United States after reported cases of intussusception, have created room for doubt in the safety of vaccines (Iskander, Haber, Murphy, Chen, & Sabin, 2004). Likewise, misconceptions, such as the unsubstantiated link between the MMR vaccine and autism, have fueled doubt in the safety of childhood vaccines (Poland & Spier, 2010). The proliferation of vaccine information on the Internet can both provide answers and raise doubts, and it can be difficult for parents to determine the trustworthiness of online sources (Zimmerman et al., 2005). Such doubts could erode public confidence in vaccine safety.
Efficacy
Confidence in the efficacy of childhood vaccines has also been an issue affecting parents’ feelings toward vaccinating their children (Cooper, Larson, & Katz, 2008). Vaccines are not 100% effective in preventing VPDs (Thomas & Moridani, 2010), and evidence of such limitations erodes confidence in parents’ assessments of their importance. This may be compounded by widely reported limitations of the seasonal flu vaccine for the general population (May, 2005; Imperato, 2005). Parents who doubt the ability of vaccines to provide protection from disease are unlikely to see the benefits of immunization as outweighing the perceived risks.
Value
Confidence in the value of vaccines is an area of increasing attention because the salience of many VPDs has decreased. Vaccination programs have been effective to their own detriment, as a drop in the number of cases of VPDs also means that parents may presume that vaccines are no longer necessary (A. M. Kennedy, Brown, & Gust, 2005). Many parents today cannot remember a time when people contracted VPDs such as polio. The absence of such memories has decreased fear of disease that may motivate parents to vaccinate their children (Smith, Kennedy, Wooten, Gust, & Pickering, 2006). Reduced perceptions of the value of vaccines could influence whether parents see vaccination as a priority for their child’s health and whether they take the time and effort to get their child vaccinated.
The relationship of these three constructs was compared with parents’ reported vaccination behaviors to determine which aspects of the larger issue of confidence were the strongest predictors of deviation from the recommended vaccination schedule, and which variables might best be able to predict such behavior. Given this stratification of vaccine confidence, we hoped an efficient, valid, and reliable measure of the construct of vaccine confidence as it predicts parents’ childhood vaccination decisions would emerge. The development of such a measure would improve researchers’ insight into the role of confidence in predicting behavior, and provide a tool for pursuing additional explanations that may drive the decision process and by extension, childhood vaccination behaviors.
Method
To assess the nature of vaccine confidence, block variables (variables composed of more than one measurement item but measured as a single variable) related to confidence in safety, efficacy, and value of vaccines were developed, with the expectation that they would each explain incrementally less variance in parents’ childhood vaccination behaviors. Our a priori assumption was that the block variable of confidence in the safety of childhood vaccines would be the most important predictor of parental behavior.
Survey
Data from the 2010 HealthStyles survey were used for analysis. HealthStyles is an annual mail-panel survey of adults living in the United States. It is a follow-up survey to the ConsumerStyles survey conducted by Porter Novelli. ConsumerStyles was mailed to a stratified random sample of 20,000 households from April through May 2010. The response rate was 52% (10,328). Of respondents who returned the ConsumerStyles survey, a random sample of 6,253 households were sent the HealthStyles survey between September and October, 2010. The response rate was 67% (4,198). The overall response rate for our sample was 34%. The data were weighted to the 2009 Current Population Survey of the U.S. Census (http://www.census.gov/cps/) on five demographic variables (gender, age, income, race/ethnicity, and household size) creating a nationally representative sample that accounts for nonresponse bias among participants. Responses from parents with children 6 years and younger (n = 376) were selected for analysis to examine the reported attitudes and behaviors of parents who had made recent vaccination decisions for their children. A validity assessment of the HealthStyles survey has shown a high correlation with answers to questions from probability-based sample surveys, such as the Behavioral Risk Factor Surveillance System (Pollard, 2002). HealthStyles data have been used previously in several areas of health research to analyze knowledge, attitudes, and behaviors of the U.S. population (A. M. Kennedy et al., 2005).
Outcome Variable
The outcome variable used in the analysis was a survey question asking parents to report their vaccination behaviors for their children. Specifically, parents were asked to “indicate the answer that best described their plans for vaccinating your youngest child.” The options were “My child has already received all of the recommended vaccines,” “I intend to have my child receive all of the recommended vaccines,” “I intend to have my child receive some but not all of the recommended vaccines,” and “I intend to have my child receive none of the recommended vaccines.” The variable was re-coded into three groups, combining responses from the first two groups of parents who reported having already had and intended to have their child vaccinated with all the recommended vaccines, those who would allow their child to receive some but not all the recommended vaccines, and those who would not allow their child to receive any of the recommended vaccines. When conducted, the survey included responses from parents with children from 0 through 6 years of age. Thirty-three respondents declined to answer the question and were removed from further analysis.
Demographic Characteristics and Attitudinal Variables
Eight 5-point and one 10-point Likert-type scale variables related to three components of the construct of vaccine confidence were included in the initial analysis along with demographic variables (see Table 1). Additional variables that were included in further analyses were related to health engagement and health care provider relationship, as described below. All variables included in the study were analyzed for covariance; all levels of covariance were acceptable except for one variable, which was removed from further analysis.
Questions/Statements Comprising Confidence in Value, Efficacy, and Safety Block Variables and Questions/Statements Comprising Health Engagement and Health Care Provider Relationship Block Variables
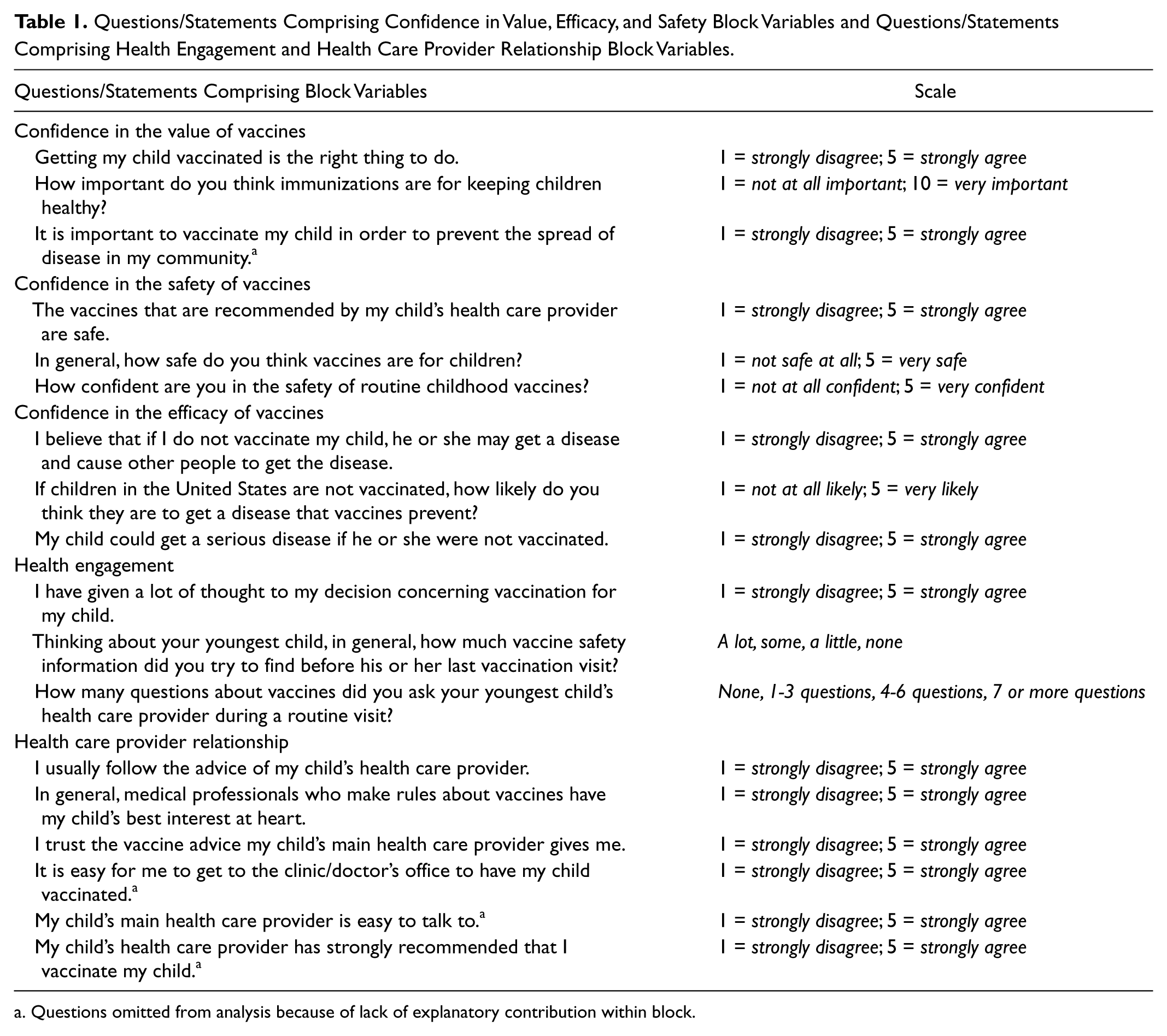
Questions omitted from analysis because of lack of explanatory contribution within block.
Statistical Analyses
We analyzed the frequencies and descriptive data for each response to the demographic, attitudinal, and behavioral questions collected in the survey. We then created a block variable for each of the three components of vaccine confidence being studied (safety, efficacy, and value). The safety and efficacy block variables were each created by combining the scores to the three attitude questions that represented those constructs, whereas the value block variable was created by combining the scores to two attitude questions that represented that construct (Table 1). In creating the value block, the question of the importance of vaccines for keeping children healthy was divided by 2 to reduce the weight of the scale used in the HealthStyles survey, a 10-point scale, and provide equal weight to both questions in the block. The two items’ different scales were the result of when and where they were added to the HealthStyles survey rather than any meaningful difference for the purpose of the study. Confidence in vaccine value was calculated as = [Getting my child vaccinated is the right thing to do + (how important do you think vaccines are for keeping children healthy/2)]/2. Scores ranged from 0.75 to 5 with 0.75 indicating low vaccine value and 5 indicating high vaccine value (M = 4.388, SD = 0.833). The scales were adjusted so that the block would be easier to interpret if it was incorporated into the final measure of vaccine confidence. Follow-up analyses were conducted to ensure that this did not alter the results of the analysis, since the other block variables did not need to be adjusted in this way.
To determine which blocks to include in the final confidence measure, we then conducted stepwise logistic regression analyses to determine if there was statistically significant variance explained by each block and how useful the blocks were in explaining parents’ reported vaccination behaviors or intentions to vaccinate their children with all, some, or none of the recommended vaccines (p < .05). Effroymson’s stepwise regression was used to select the most influential block or blocks for predicting vaccine behavior (Effroymson, 1960; King, 1967), and eliminate blocks with little explanatory capacity (Beale, Kendall, & Mann, 1967) while accounting for the polytomous dependent variable of vaccination behavior (Wright, 1995). The analysis controlled for demographic variables of gender, race/ethnicity, age, household income, and education (see Table 2).
Sociodemographic and Behavioral Characteristics of Parents With at Least One Child Aged 6 Years and Younger, HealthStyles, 2010 (n = 376)

Note. Data were weighted to reflect the 2009 U.S. Census Current Population Survey. Percentages and numbers have been rounded.
Follow-up analyses were also conducted on responses from parents with children 6 years and younger from the 2009 HealthStyles survey (n = 544) to determine if the findings were consistent between sample groups over time. Information regarding the 2009 survey is available on request. The variables in both 2010 and 2009 data sets were normally distributed, a linear relationship was observed between the dependent and independent variables, and the independent variable data were homoscedastic in nature. The use of Effroymson’s (1960) stepwise regression, although valuable for selecting influential variables, is noted to inflate the potential for Type I error. To account for this, variable order was systematically rotated in an effort to discover any abnormalities. All analyses were computed using SPSS.
Results
Of the eight items used in analyzing vaccine confidence, all were individually significant predictors of parents’ reported vaccine behaviors. A stepwise logistic regression was calculated to predict parents’ reported childhood vaccine decisions or intentions based on the three block variables: safety, efficacy, and value, controlling for demographics. Univariate results are provided in Table 3. The block related to confidence in vaccine value was found to be significantly predictive of reported vaccination behavior, F(2, 351) = 119.199, p < .001, ΔR2 = .397, or almost 40% of the variance in reported parental vaccination behaviors, controlling for demographics (Table 4). The same analysis was repeated on the 2009 data set. The block related to confidence in vaccine value was found to be significantly predictive of reported vaccination behavior, F(2, 535) = 262.738, p < .001), ΔR2 = .489, or almost 49% of the variance in reported parental vaccination behaviors, controlling for demographic information. As parents’ confidence in vaccine value score increased, so did the likelihood that parents had vaccinated or intended to vaccinate their child according to the recommended schedule. Although the block variables for confidence in vaccine safety and confidence in vaccine efficacy were statistically significant predictors of vaccine behavior, neither accounted for additional significant variance beyond confidence in vaccine value in reported vaccine behaviors. This was the case for both the 2010 and 2009 data sets.
Results From Univariate Stepwise Regression of HealthStyles 2010 Data Evaluating the Predictive Strength of Confidence in Vaccine Value, Efficacy, and Safety on Reported Childhood Vaccination Behavior
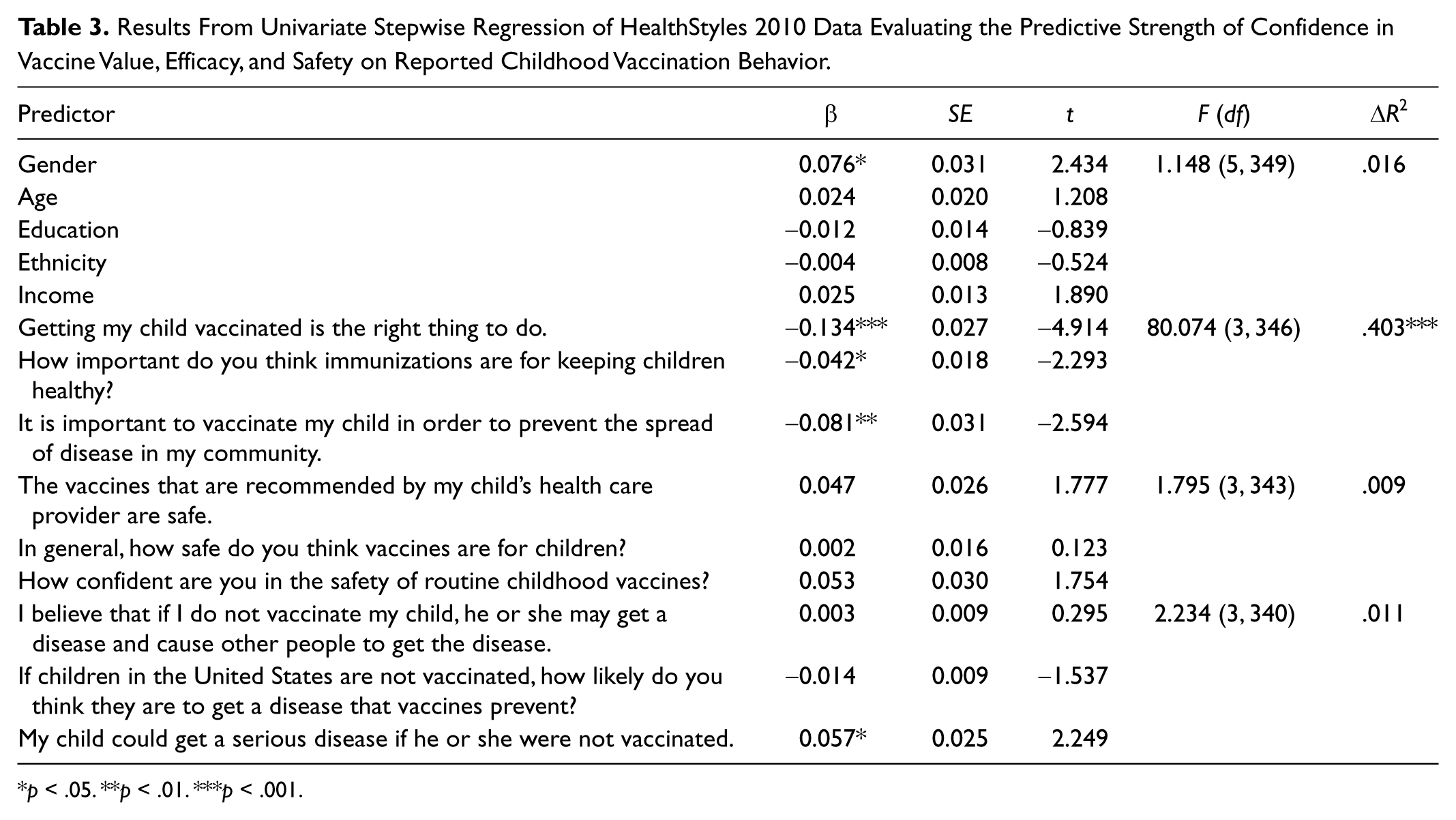
p < .05. **p < .01. ***p < .001.
Results From Effroymson’s Stepwise Regression Conducted on HealthStyles 2009 and 2010 Data Evaluating the Predictive Strength of Confidence in Vaccine Value, Efficacy, and Safety on Reported Childhood Vaccination Behavior

Includes gender, age, education, ethnicity, and income.
p < .001.
Discussion and Practice Implications
After further refining the construct of vaccine confidence, the focus of this research was to develop an effective and efficient measure of the attitudinal component of parents’ childhood vaccination decisions. All the variables included in the analysis significantly predicted parents’ behaviors when examined separately. This is important to illustrate that although the two-item confidence in vaccine value block may be superior in measuring behavioral variance, it does not suggest that the other variables are irrelevant in vaccine decisions. Furthermore, it is critical to emphasize that these results do not suggest that confidence in vaccine safety or efficacy are not real concerns that drive parents’ reported vaccination behaviors or intentions. Rather, the two-item block assessing parents’ confidence in the value of childhood vaccinations is an efficient tool for broadly measuring the attitudinal components that drive vaccination behavior. Researchers looking for a short measure of vaccine attitudes may find use in the value measure, and practitioners may better tailor their vaccine-related interactions with parents based on quickly gathered insights into their attitudes and predicted behaviors. When possible, we recommend consideration of issues related to vaccine value, efficacy, and safety, as they are all relevant to vaccine confidence.
A concern related to the statistical tests used involves the somewhat subjective nature of variable selection, as repeated F tests typically inflate significance, which would lead to increased variable inclusion in the confidence measure (Forsythe, Engleman, Jennrich, & May, 1973). Partial correlations were calculated holding constant the other predictor variables to ensure that the selected block of variables was the strongest predictor of reported behavior. It was concluded that the two-item confidence in vaccine value block was the best predictor variable of all the attitudinal block variables examined in predicting parents’ reported vaccination behaviors or intentions for their children. As the score measuring parents’ confidence in the value of vaccines increased, so did the likelihood that respondents had or intended to vaccinate their child with all the recommended vaccinations. Moreover, the same analysis was repeated with data from the HealthStyles 2009 poll, producing similarly patterned results and greater explained variance. The same analyses were conducted with ConsumerStyles 2011 data, a larger, online poll, and similar results were found suggesting that the results were not because of Type I error. This block can serve as a tool for researchers intending to account for attitudinal variance in parents’ vaccine decisions. However, the decision to vaccinate is one that is made repeatedly at each medical visit, and it is influenced by any number of factors. More work is needed to develop a comprehensive measure that predicts vaccination behavior. At this stage, the vaccine value measure should be considered as a tool for researchers looking to account for attitudinal variance among other variables, or practitioners looking to quickly assess parental attitudes and prepare accordingly, perhaps by allowing more time to discuss vaccination questions and concerns.
Once parents’ overarching value of childhood immunizations has been assessed, it may be prudent to look beyond attitudes in explaining the basis for their decisions. This is consistent with most health behavior models, such as the theory of planned behavior, theory of reasoned action (Montano & Kasprzyk, 2002), and the health belief model (Janz, Champion, & Strecher, 2002), which consider attitudinal components as only partial influences in health behaviors. In seeking to better understand vaccine decision making, we must consider not only attitudes but also the perceived and tangible barriers (i.e., transportation to doctors’ offices), facilitators (i.e., school requirements), and knowledge (i.e., knowledge of the vaccine schedule) that contribute to the decision to adopt a behavior (Hochbaum, 1958; Rosenstock, 1974).
This study has a number of limitations. The panel survey method may introduce some bias in answers, as respondents by definition have indicated an interest in taking part in survey research and nonrespondents may differ systematically from those who returned surveys. The data were weighted in part to address these potential biases. In addition, vaccination behavior and intention were self-reported by respondents; however, the proportion of parents who had or planned to fully vaccinate their youngest child is similar to national vaccination coverage estimates reported at school entry (Centers for Disease Control and Prevention, 2007, 2011). Most notable is the small sample size of the study, and in particular the small sample of parents who do not intend to vaccinate their children at all. The statistical tests used in the analysis are valid despite these small numbers (Cohen, 1988). Furthermore, similar findings with the 2009 and 2011 data suggest that the results are not unique to the 2010 sample of respondents.
The two-item confidence in vaccine value block variable represents a potentially valuable tool for health and public health professionals to efficiently assess the role of confidence in vaccine decisions. Such measures have been used to assess the impact that attitudinal variables have on patient assessment of health outcomes such as spine surgery (Mannion et al., 2009), as well as health care professionals’ assessments of patients’ multiple sclerosis prognosis (Khan, Pallant, Zhang, & Turner-Stokes, 2010). The measure could be especially useful in moving forward with the assessment of other factors that drive parents’ vaccine decisions. Confidence variables accounted for a little less than half of the variance in reported vaccine behaviors and intentions in this survey. We looked at other attitudinal variables, such as health engagement, and relationships and communication with health care providers, and they failed to improve on the predictive nature of the value block. This suggests that the variance accounted for by the two-item value block may be effectively measuring the attitudinal component in parents’ vaccine behaviors. These findings suggest that it would behoove us to return to other types of variables to account for further variance in the parents’ vaccination behaviors, such as knowledge related to vaccine exemptions and tangible barriers and facilitators to receiving vaccinations, such as cost and access to health care. Furthermore, our findings point to the importance of discussing not only the risks of vaccines but also their benefits with parents, as a more thorough understanding of VPDs may help reinforce the value of vaccines in protecting the health of children.
Footnotes
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.