
Abstract
Diet-related chronic diseases are highly prevalent among indigenous populations in the Canadian Arctic. A community-based, multi-institutional nutritional and lifestyle intervention—Healthy Foods North—was implemented to improve food-related psychosocial factors and behaviors among Inuit and Inuvialuit in four intervention communities (with two comparison communities) in Nunavut and the Northwest Territories, Canada, in 2008. The 12-month program was developed from theory (social cognitive theory and social ecological models), formative research, and a community participatory process. It included an environmental component to increase healthy food availability in local stores and activities consisting of community-wide and point-of-purchase interactive educational taste tests and cooking demonstrations, media (e.g., radio ads, posters, shelf labels), and events held in multiple venues, including recreation centers and schools. The intervention was evaluated using pre- and postassessments with 246 adults from intervention and 133 from comparison communities (311 women, 68 men; mean age 42.4 years; 78.3% retention rate). Outcomes included psychosocial constructs (healthy eating knowledge, self-efficacy, and behavioral intentions), frequency of healthy and unhealthy food acquisition, healthiness of commonly used food preparation methods, and body mass index (kg/m2). After adjustment for demographic, socioeconomic status, and body mass index variables, respondents living in intervention communities showed significant improvements in food-related self-efficacy (β = 0.15, p = .003) and intentions (β = 0.16, p = .001) compared with comparison communities. More improvements from the intervention were seen in overweight, obese, and high socioeconomic status respondents. A community-based, multilevel intervention is an effective strategy to improve psychosocial factors for healthy nutritional behavior change to reduce chronic disease in indigenous Arctic populations.
Keywords
Inuit and Inuvialuit indigenous populations living in Nunavut and the Northwest Territories (NWT), Canada, have increasing rates of obesity and chronic diseases and disproportionately high incidence of several cancers (Bjerregaard, Young, Dewailly, & Ebbesson, 2004; Circumpolar Inuit Cancer Review Working Group et al., 2008; Friborg & Melbye, 2008). This developing public health problem is largely attributable to the rapid nutrition and lifestyle transition that has occurred over the past few decades, specifically the transition from an active, subsistence-based lifestyle to one that is more sedentary and dependent on market foods (Bjerregaard et al., 2004; Friborg & Melbye, 2008; Kuhnlein, Receveur, Soueida, & Egeland, 2004; Popkin, 1998, 2006; Sharma, 2010). Inuit and Inuvialuit have a high chronic disease risk factor profile, including high prevalence of smoking, obesity, low levels of physical activity, and low dietary quality (Bjerregaard et al., 2004; Deering, Lix, Bruce, & Young, 2009; Erber, Beck, De Roose, & Sharma, 2010; Erber, Hopping, et al., 2010; Hopping, Erber, Beck, De Roose, & Sharma, 2010; Hopping, Erber, Mead, Roache, & Sharma, 2010; Hopping, Mead, et al., 2010). Inuit and Inuvialuit populations in the Canadian Arctic are at a critical point for nutritional and physical activity intervention for chronic disease prevention and improvement of dietary adequacy.
Diet and physical activity are important modifiable risk factors that have been successfully targeted in numerous intervention trials to reduce risk of chronic disease (Roberts & Barnard, 2005). Psychosocial factors, such as self-efficacy and intentions to perform healthy behaviors in the future, are significant predictors of consuming a healthy diet and engaging in physical activity, and can be targeted by intervention programs to produce lasting dietary and activity improvements that reduce risk of obesity and chronic disease (Abdulla & Gruber, 2000; Glanz et al., 1995; Langlois, Garriguet, & Findlay, 2009; Rovniak, Anderson, Winett, & Stephens, 2002; Watters & Satia, 2009). Prior work in Inuit and Inuvialuit communities showed only moderate levels of healthy eating knowledge, self-efficacy, and intentions to engage in healthier food-related behaviors in these populations (Mead, Gittelsohn, De Roose, & Sharma, 2010; Mead, Gittelsohn, Roache, & Sharma, 2010). In addition, unhealthy foods were acquired (e.g., white bread, potato chips) for their households two to three times more frequently than healthier options and there was infrequent use of food preparation methods that minimize fat content (Mead, Gittelsohn, De Roose, et al., 2010; Mead, Gittelsohn, Roache, et al., 2010). Community-based interventions targeting food-related psychosocial factors are needed to improve dietary behaviors and ultimately reduce the chronic disease burden.
Interventions that combine environmental approaches with behavior change strategies are promising advances in public health programming (Glanz et al., 1995; Kumanyika, 2001). Successfully implemented community-based nutritional and physical activity programs among Canadian First Nations and American Indian populations have had some success in improving psychosocial factors and dietary behaviors (Caballero et al., 2003; Ho et al., 2008; Saksvig et al., 2005; Stevens et al., 2003; Thompson et al., 2008). Key components of successful interventions with indigenous populations included community ownership of the program, cultural sensitivity, inclusion of community health workers, empowerment, and integration into multilevel efforts (Huffman & Galloway, 2010).
To date, health promotion programs targeting Inuit and Inuvialuit populations in Arctic Canada have been largely mass media initiatives or programs based in local health and wellness centers that would benefit from following standard research protocol for evidence-based development, rigorous evaluation, and working in other community institutions. To the best of the authors’ knowledge, despite significant investment of resources, no nutritional and physical intervention programs combining community-based and multi-institutional approaches with rigorous research methodologies have been previously implemented in these populations.
Healthy Foods North
Healthy Foods North (HFN) was a 12-month community-based, multilevel, multi-institutional nutritional and physical activity intervention program that was developed using formative research, current dietary data, and a community participatory approach to ensure a basis in scientific evidence, cultural acceptability, and community ownership (Gittelsohn, Roache, et al., 2010; Sharma, Gittelsohn, Rosol, & Beck, 2010). In the formative research phase, community members and representatives from local community organizations, health and social services, and the stores were recruited using purposive sampling and interviewed about their perspectives on health and diet (Gittelsohn, Roache, et al., 2010). They also participated in community workshops to develop the intervention plan and materials, such as key messages, promotional strategies, and the selection of healthier foods, beverages, and preparation methods to promote (Gittelsohn, Roache, et al., 2010). Cultural norms and values identified from formative research were incorporated into the intervention, such as an emphasis on traditional foods and family life, to ensure that it would be culturally acceptable and relevant. Multiple stakeholders were partners, such as local stores, national food retailers, a local research institute, local and national nongovernmental organizations (e.g., local Hunters and Trappers organizations, Inuit Tapiriit Kanatami), and multiple levels of government (Sharma et al., 2010). Community collaboration and ownership continued throughout the length of the intervention through regular presentation of research results and study progress to the stakeholders and incorporating their feedback on an ongoing basis. Moreover, local community members were hired and trained to deliver the intervention, and their comments were incorporated into the intervention design (Gittelsohn, Roache, et al., 2010).
Employing a behavioral change strategy drawn from social cognitive theory (SCT) and social ecological models (SEM), HFN’s primary aims were to improve dietary adequacy, increase physical activity, and reduce risk of chronic disease among Inuit in Nunavut and Inuvialuit in the NWT. The objectives were to increase consumption of traditional foods (e.g., caribou, fish) and nutrient-dense store-bought foods low in fat and sugar (e.g., fruits, vegetables), decrease consumption of non–nutrient-dense, high-fat, high-sugar foods (e.g., soda, chips), and increase engagement in moderate and vigorous physical activity while reducing sedentary activity. The intervention was divided into seven phases, including tea/coffee/healthy breakfast, healthy snacks, healthy home eating/traditional foods, healthy beverages, healthier cooking/meal planning, and consuming sufficient vitamins and minerals (Sharma et al., 2010; Sharma, Mead, Gittelsohn, Beck, & Roache, 2011).
SCT emphasizes reciprocal determinism in the interaction between individual-level and environmental-level factors, and key concepts include self-efficacy, observational learning, outcome expectations, self-regulation, and facilitation (McAlister, Perry, & Parcel, 2008). In SEM, the social and physical environments are seen as highly influential of behaviors, and factors interact across multiple levels to affect behavior (Sallis, Owen, & Fisher, 2008). Following these theories, the intervention worked on an environmental level with local food stores, retailers, and other partners to increase the availability and accessibility of healthier food options and opportunities for engaging in physical activity (Sharma et al., 2010). The store component was a collaboration with store managers to stock healthier options, such as whole wheat bread, skim milk powder, and high-fiber low-sugar cereals. In addition, interactive taste test sessions and cooking demonstrations took place in the stores to educate community members about healthier cooking skills, healthy meal planning/shopping, and healthier alternatives to commonly consumed foods and beverages, such as skim milk powder as an alternative to high fat whitener for coffee. The aim of the sessions was to provide opportunities for observational learning, building self-efficacy, and increasing positive outcome expectations, which are theoretical constructs of SCT. Point-of-purchase media, such as shelf labels and posters, were displayed in the store to identify healthy choices (e.g., “High in Fiber” label on the whole wheat bread shelf) and to reinforce intervention messages.
The community component consisted of radio and television media and community-wide activities in recreational centers, health and wellness centers, worksites, schools, and other venues. Activities included cooking classes, taste tests, community feasts that featured promoted foods and cooking methods, walking clubs, and pedometer challenges. Where available, intervention messages were displayed on the local television channel, and stories that featured a family learning how to improve their diet and increase activity were broadcast on the local radio. At the individual level, the intervention aimed to increase healthy eating knowledge, self-efficacy, and intentions to engage in both healthy food-related behaviors and physical activity through the media and participation in intervention activities. The HFN intervention has been described in detail previously (Sharma et al., 2010).
This present study evaluates the impact of the HFN intervention on the psychosocial determinants of diet (i.e., healthy eating knowledge, self-efficacy, and intentions), food-related behaviors (i.e., frequency of healthy and unhealthy food acquisition, and healthfulness of food preparation methods), and body mass index (BMI).
Method
The study was a quasi-experimental pre-/postevaluation of HFN conducted in three Inuit communities in one region of Nunavut and three Inuvialuit communities in one region of the NWT. Two remote communities in Nunavut received the intervention from October 2008 to November 2009, and one semiremote and one remote community in the NWT received it from May 2008 to August 2009. One remote community in each territory served as the comparison (“delayed intervention”) community and received the intervention postevaluation. Communities were assigned to the intervention or comparison arm based on a range of population sizes, percentages of the population who were Inuit or Inuvialuit, percentages of the population engaged in the wage economy, and percentages of the population engaged in traditional hunting and fishing practices. This study was licensed by the Aurora Research Institute in the NWT and the Nunavut Research Institute and was approved by the Committee on Human Studies at the University of Hawaii, Office of Human Research Ethics at the University of North Carolina at Chapel Hill, and Beaufort Delta Health and Social Services Authority Ethics Review Committee. All respondents signed written consent forms (in English or the local language) and were compensated with a gift card for $25 CDN to a local store.
Data Collection
All the participating communities were located above the Arctic Circle (Sharma, 2010). The four intervention communities range in size from 800 to 3,500 residents (Statistics Canada, 2007a, 2007b). Three communities had two food stores, and one community had three food stores and three convenience stores. The intervention was implemented in all of the food stores. The two comparison communities had a population size of 400 and 1,000 and two small food stores (Statistics Canada, 2007a, 2007b).
Data collectors consisted of community members and research staff who were trained by the second author (JG) and principal investigator (SS) on administration of the questionnaires at baseline and follow-up. For non-English speaking respondents, either a data collector fluent in the local language conducted the interview or an interpreter was used. At baseline, households were randomly selected using government housing maps. One Inuit/Inuvialuit adult (≥19 years) per household was selected if she or he was a main food shopper or preparer in the household, was not pregnant or breastfeeding, had lived in the community for at least 6 months, and intended to remain in the community for at least another year. Baseline data were collected for 4 months in 2008 in Nunavut and 9 months from 2007-2008 in the NWT (Sharma, 2010). The intervention started within 1 month after baseline data collection completion. Sample size was calculated using a two-sided paired t test, a significance level of 5%, and a power of 80%, which showed that a sample size of 50 per community was required. Postintervention data collection occurred from October to December 2009, starting 1 month after intervention completion. At follow-up, data collectors were able to contact 91.5% of the 494 baseline respondents. Those who were not contacted had moved out of the community, were traveling outside of the community during the time of follow-up, or were deceased. Sixty-four refused to participate at follow-up. The overall retention rate was 78.3%.
Conducted at baseline and follow-up, the Adult Impact Questionnaire (AIQ) measured food-related knowledge, self-efficacy and intentions, frequency of healthy and unhealthy foods acquisition, and healthfulness of commonly used food preparation methods in the 30-day recall period. AIQ scales were based on constructs from SCT and theory of planned behavior, and the questions were developed and refined during community workshops and pilot testing in the intervention communities (Mead, Gittelsohn, De Roose, et al., 2010; Mead, Gittelsohn, Roache, et al., 2010; Sharma, 2010). Scales were evaluated for internal reliability using Cronbach’s α and for content, face, and cultural validity with a representative sample of Inuit and Inuvialuit adults during the workshops and pilot testing (Mead, Gittelsohn, De Roose, et al., 2010; Mead, Gittelsohn, Roache, et al., 2010). The AIQ also collected information on demographic and socioeconomic variables and the Material Style of Life (MSL) score, which was an additive scale of ownership of 20 items in working condition used to approximate socioeconomic status (SES; baseline Cronbach’s α = .83; follow-up Cronbach’s α = .84). Trained staff measured heights to the nearest centimeter using a stadiometer and weights to the nearest 0.10 pound using a digital scale.
Descriptions of the scales and baseline results have been reported previously (Mead, Gittelsohn, De Roose, et al., 2010; Mead, Gittelsohn, Roache, et al., 2010). In brief, the food knowledge score (baseline Cronbach’s α = .55; follow-up Cronbach’s α = .55) was the sum of correct answers for eight multiple-choice questions related to a healthy diet. The healthy eating self-efficacy score (baseline Cronbach’s α = .69; follow-up Cronbach’s α = .69) was based on eight questions assessing how easy or hard it would be for the respondent to perform certain healthy behaviors regularly on a 4-point Likert-type response scale, ranging from very easy (assigned 4 points) to impossible (assigned 1 point). The healthy eating intentions score (baseline Cronbach’s α = .61; follow-up Cronbach’s α = .64) was composed of seven questions concerning how often the respondent intended to engage in dietary practices in the next 30 days using a 5-point Likert-type scale, ranging from always (assigned 5 points) to never (assigned 1 point).
Two frequency of food acquisition scores were calculated, one for the summed frequency of acquisition of 24 healthier food choices promoted by the HFN program (baseline Cronbach’s α = .72; follow-up Cronbach’s α = .71) and one for the summed frequency of acquisition of nine unhealthy food choices (baseline Cronbach’s α = .69; follow-up Cronbach’s α = .63). Community members and other key stakeholders selected the foods during community planning workshops (Gittelsohn, Roache, et al., 2010). The term acquisition was inclusive of the following food usage strategies: store purchase, receipt from a food bank or family/friends, hunting and gathering, purchased while travelling, the individual Food Mail (government-subsidized airfreight food transportation to Northern communities, now known as Nutrition North Canada), or barge/sealift order. For the healthfulness of food preparation score, the preparation methods reported for eight different foods (i.e., bannock [fried bread], chicken, pork or beef, fish, seal, musk ox or caribou, potatoes, and eggs) were assigned a negative, zero, or positive point if the method added, had no impact on, or reduced fat content (baseline Cronbach’s α = .48; follow-up Cronbach’s α = .50), respectively.
Data Analyses
Differences between pre- and postpsychosocial and behavioral constructs and BMI by intervention assignment were analyzed using a two-sample t test for normally distributed variables and a Wilcoxon Mann–Whitney test for skewed variables. A p value of ≤.05 in a two-sided test was used as the level of significance for all analyses.
BMI was calculated (kg/m2) and adjusted for clothing weight (light, 1 kg; medium, 1.5 kg; heavy, 2 kg; Hopping, Erber, Beck, et al., 2010; Hopping, Erber, Mead, et al., 2010). Program impact was assessed using multivariable linear regression models. Postintervention knowledge, self-efficacy, intentions, frequency of healthy and unhealthy food acquisition, and healthfulness of food preparation scores were regressed on baseline independent variables that included intervention assignment, baseline score of the dependent variable, age, gender, educational level (categorical), MSL score (categorical), baseline BMI group (categorical), and either household employment status (binary) or income support status (binary) depending on which explained more variance. In addition, the two food acquisition dependent variables were adjusted for the postintervention number of people eating regularly in the household in the 30-day recall period, and were square root transformed to account for nonnormally distributed residuals. Postintervention BMI (continuous variable log transformed to account for nonnormally distributed residuals) was regressed on the baseline value, age, gender, education, MSL, and employment status. Standardized (std) beta regression coefficients (i.e., measured in standard deviations) were also reported to enhance comparability of the regression coefficients. Post hoc analyses were conducted to examine the psychosocial and behavioral model results stratified by baseline BMI groups and the interaction between intervention assignment and independent variables for all models.
Respondents who moved from an intervention to a comparison community (or vice versa) and 10 respondents missing pre- or postpsychosocial and behavioral data were excluded from analysis. Data were analyzed using Stata/IC version 11.1 (StataCorp LP, College Station, TX).
Results
A total of 246 (199 women, 47 men) in the intervention communities and 133 (112 women, 21 men) in the comparison communities were included in the analysis. Mean ages were 42.4 years (SD = 13.1) for the women and 42.3 years (SD = 12.8) for the men. Communities did not differ in their baseline values of healthy eating knowledge and self-efficacy, healthy and unhealthy food acquisition, and food preparation scores, though comparison respondents had greater intentions to engage in healthier food-related behaviors than intervention respondents at baseline (mean score 22.02 vs. 20.58, p = .0027; Table 1). Without adjusting for other factors, intervention respondents had a greater increase in healthy eating intentions than the comparison group (change 2.14, p < .0001; Table 1). The intervention group significantly reduced their average frequency of unhealthy food acquisition compared with the comparison group (change = −5.28, p = .0019). Intervention respondents acquired 4.51 fewer unhealthy foods than they did at baseline while the comparison respondents acquired 0.77 more unhealthy foods, on average.
Unadjusted Psychosocial, Behavioral, and Body Mass Index (BMI) Outcomes for Intervention and Comparison Groups at Follow-up (Mean)
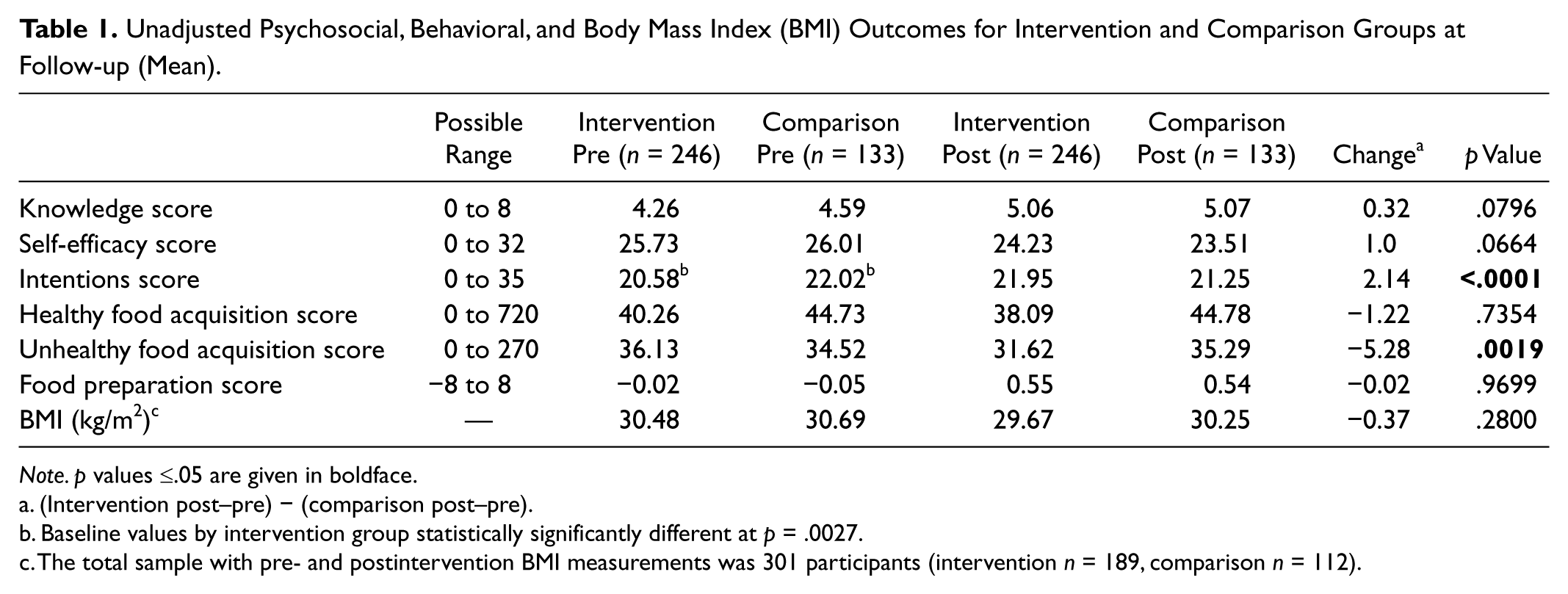
Note. p values ≤.05 are given in boldface.
(Intervention post–pre) − (comparison post–pre).
Baseline values by intervention group statistically significantly different at p = .0027.
The total sample with pre- and postintervention BMI measurements was 301 participants (intervention n = 189, comparison n = 112).
After adjustment for demographic, socioeconomic, and BMI variables, all psychosocial factors significantly improved from baseline (p < .001), and the intervention was associated with increased self-efficacy and intentions (std β = 0.15, p = .003, and std β = 0.16, p = .001, respectively) compared with the comparison communities (Table 2). In other words, at follow-up, the increase in the average self-efficacy score from baseline was 0.13 SD greater in the intervention group than the comparison group (p = .009), and the increase in the intentions score was 0.16 SD greater (p = .001), after adjusting for participant characteristics. Across all communities, healthy and unhealthy food acquisition frequency significantly increased from baseline (std β = 0.23, p < .001, and std β = 0.34, p < .001, respectively), after adjusting for other factors (Table 3). However, the intervention was not associated with statistically significant changes in food acquisition frequency. The healthfulness of food preparation score did not significantly change from baseline, and the intervention was not associated with a significant change in food preparation. Adjusting for other characteristics, average BMI increased by 0.03 kg/m2 across all communities (std β = 0.91, p < .001), but the intervention had no significant impact on BMI (data not shown).
Impact of Healthy Foods North (HFN) on Post–Healthy Food Knowledge, Self-Efficacy, and Intentions, by Intervention Assignment
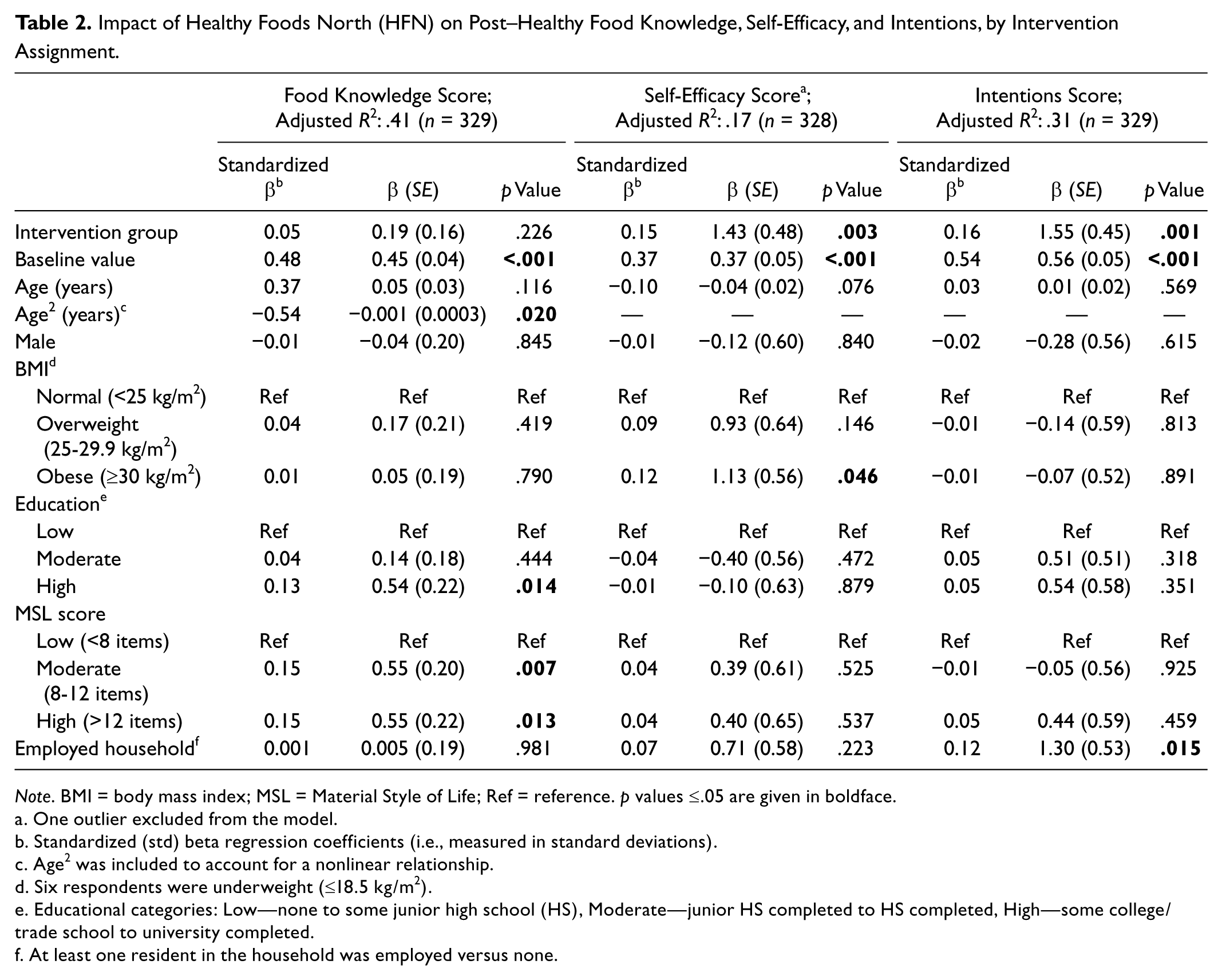
Note. BMI = body mass index; MSL = Material Style of Life; Ref = reference. p values ≤.05 are given in boldface.
One outlier excluded from the model.
Standardized (std) beta regression coefficients (i.e., measured in standard deviations).
Age2 was included to account for a nonlinear relationship.
Six respondents were underweight (≤18.5 kg/m2).
Educational categories: Low—none to some junior high school (HS), Moderate—junior HS completed to HS completed, High—some college/trade school to university completed.
At least one resident in the household was employed versus none.
Impact of Healthy Foods North (HFN) Intervention on Healthy Food Behaviors by Intervention Assignment
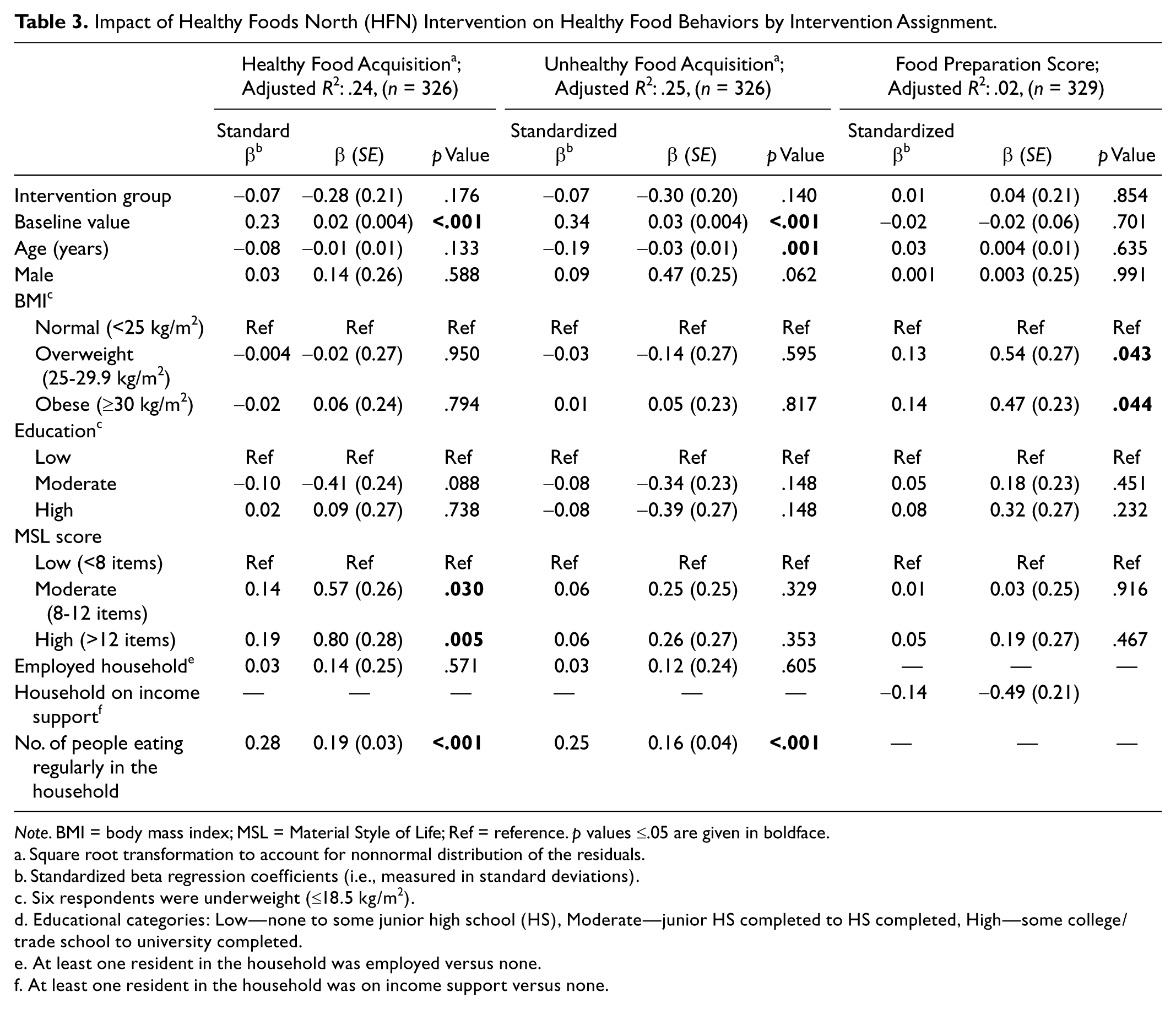
Note. BMI = body mass index; MSL = Material Style of Life; Ref = reference. p values ≤.05 are given in boldface.
Square root transformation to account for nonnormal distribution of the residuals.
Standardized beta regression coefficients (i.e., measured in standard deviations).
Six respondents were underweight (≤18.5 kg/m2).
Educational categories: Low—none to some junior high school (HS), Moderate—junior HS completed to HS completed, High—some college/trade school to university completed.
At least one resident in the household was employed versus none.
At least one resident in the household was on income support versus none.
The multivariable linear regression models were also stratified by baseline BMI category (data not shown). Compared with the comparison communities, the intervention was significantly associated with increased healthy eating intentions (std β = 0.23, p = 0.021) and decreased frequency of unhealthy food acquisition (std β = −0.30, p = .008) among respondents who were overweight at baseline. Among obese respondents, the intervention was significantly associated with increased self-efficacy (std β = 0.16, p = .027) and healthy eating intentions (std β = 0.18, p = .010). No intervention effects were seen among the subset of respondents with normal weight at baseline.
Analysis of the interaction between the intervention assignment and independent variables revealed that the intervention was generally associated with improvements in healthy eating psychosocial factors and behaviors among higher SES respondents compared with low SES (data not shown). Compared with the comparison communities, the intervention was significantly associated with increased food knowledge (std β = 0.21, p = .032) and use of healthier preparation methods (std β = 0.27, p = .034) among respondents with a moderate MSL score compared with a low score. In addition, the intervention was significantly associated with increased self-efficacy among respondents with moderate (std β = 0.39, p = .001) and high MSL (std β = 0.28, p = .006) scores compared with low MSL, and among highly educated respondents compared with low education (std β = 0.23, p = .015). In contrast to the above trend, the intervention was significantly negatively associated with food knowledge in employed households compared with unemployed (std β = −0.24, p = .022).
Discussion
The present study reports on the impact on food-related psychosocial factors and behaviors of the first (to the authors’ knowledge) community-based, multi-institutional, evidence-based nutritional and physical activity program targeted toward Inuit and Inuvialuit populations in the Canadian Arctic. Following SEM and SCT, the intervention targeted environmental and psychosocial factors as important determinants of food-related behaviors. Intervention community respondents had significantly greater increases in healthy eating self-efficacy and intentions than comparison respondents. Baseline results showed that intention to perform the behavior in the future was the psychosocial factor most significantly associated with all three food-related behaviors of interest (Mead, Gittelsohn, De Roose, et al., 2010; Mead, Gittelsohn, Roache, et al., 2010). Prior research has shown that behavioral intentions are significantly related to increased healthy eating 6 years later, thus dietary changes—and subsequently BMI changes—in the intervention communities may be evident in the long-term (Conner, Norman, & Bell, 2002).
The effects of HFN were similar to other nutritional interventions in American Indian communities. The ZATPD (Zhiiwaapenewin Akino’maagewin: Teaching to Prevent Diabetes) nutritional and physical activity intervention in Ontario First Nations had store- and community-based components similar to HFN and found significant increases in healthy food knowledge and acquisition (Ho et al., 2008). In addition, a similar community- and store-based nutrition intervention on Apache reservations in the southwestern United States found increases in the psychosocial factors of healthy food knowledge and intentions as well as healthy food acquisition behaviors (Gittelsohn & Rowan, 2011). The positive impact of the HFN intervention on intentions and the other psychosocial constructs supports their potential as modifiable factors to affect positive change in food acquisition, food preparation, and dietary intake among Inuit and Inuvialuit. Without adjusting for other factors, a greater decrease in unhealthy food acquisition frequency was seen in the intervention communities than the comparison communities, suggesting the potential impact of HFN on food-related behavior.
Post hoc analysis revealed that the intervention was generally associated with healthier food-related psychosocial factors and behaviors among respondents with a higher SES and education. A systematic review of nutrition interventions found similar trends in greater intervention effects among high-SES participants compared with low-SES participants (Oldroyd, Burns, Lucas, Haikerwal, & Waters, 2008). Overall, strong evidence exists for a socioeconomic gradient in diet quality, and the high cost of healthy foods is a significant contributing factor (Darmon & Drewnowski, 2008). Although the HFN intervention attempted to promote healthy foods at the same or lower cost as the unhealthy alternatives (e.g., wheat bread in place of white bread), further exploration into how food costs affected the success of HFN and other nutrition interventions in low SES populations is warranted. For practitioners working with low SES populations to improve diet, the inclusion of local food cost data in the formative research phase may be useful in the selection of appropriate alternatives to promote. Last, SES may significantly moderate the relationship between the food-related psychosocial factors and behaviors (Sandvik, Gjestad, Samdal, Brug, & Klepp, 2010), which requires further study.
Significant differences in intervention effects on healthy eating self-efficacy, intentions, and unhealthy food acquisition frequency were seen among overweight and obese participants. These changes were significant given that 65% of the Inuvialuit and 72% of the Inuit study population were overweight or obese (Hopping, Erber, Beck, et al., 2010; Hopping, Erber, Mead, et al., 2010). The intervention was developed to target all community members, but the differences by SES and BMI show that further work may be needed to tailor the intervention to subgroups.
HFN is novel in its approach to community participation and capacity building at multiple stages, from intervention development through evaluation, making it integrable into other community organizations and programs. Community engagement and inclusion of community priorities in health promotion programs are essential for ethical, effective, and sustainable programs among indigenous populations (Canadian Institutes of Health Research, 2011; Macaulay et al., 1999; Merzel & D’Afflitti, 2003; Potvin, Cargo, McComber, Delormier, & Macaulay, 2003). In addition, HFN’s store- and community-based components, partnerships with multiple levels of government, nongovernmental organization, food retail, and community stakeholders, and environment-level impact on accessibility of healthier options make it highly likely to be an effective, sustainable program in the long-term (Sallis & Glanz, 2009). Multilevel approaches, partnerships with food stores, and multi-institutional integration are critical components of interventions to reduce the obesity epidemic in indigenous populations (Gittelsohn & Rowan, 2011).
Complex, multifaceted interventions such as HFN require a significant amount of preparation prior to implementation. Although the intervention itself was only 12 months in duration, the process to form collaborative partnerships, conduct formative research, design the intervention, and pilot intervention materials took 4 years prior to the start of preintervention data collection. The significant amount of preparation time helped ensure effective implementation of the intervention, and therefore investigators should build this time into the planning phase. However, challenges to implementation did arise, such as high community member staff turnover in the beginning of the intervention and difficulties in keeping some promoted foods stocked in the stores. The study team and partners worked together to address these challenges and adjust the intervention plan when needed. Future projects should allow for some flexibility and increased duration of intervention phases as needed. Despite the relatively short duration of an intervention of this magnitude, significant changes in several outcomes, and trends toward positive change in others, were seen, supporting the efficacy of the intervention.
To the best of the authors’ knowledge, no other systematic evidence-based nutritional and physical activity research and intervention programs have been implemented among Inuit and Inuvialuit adults in the Canadian Arctic. Other nutritional and physical activity intervention studies have been conducted with American Indian children, youth, and adults to reduce risk of diabetes, obesity, and other chronic diseases (Caballero et al., 2003; Ho et al., 2008; LeMaster & Connell, 1994; Potvin et al., 2003; Saksvig et al., 2005; Thompson et al., 2008). Successful components of these interventions have included using a multifaceted, integrative approach for the intervention, inclusion of cultural principles and practices in the intervention, community engagement, capacity building, and equal partnerships with the community and other stakeholders. The inclusion of these components in the HFN program is one of the keys to its success and should be considered by investigators (Sharma et al., 2010).
The results of the present study suggest that a community-based, multilevel intervention is a viable approach to improve diet within a population. Food stores and other community places are important venues for nutritional interventions (Gittelsohn & Rowan, 2011; Ho et al., 2008; Song et al., 2009). Future work should involve the food stores and other community partners in the planning process to develop an appropriate and effective multilevel intervention. Moreover, formative work was important to address the key diet-related issues in the community and develop relevant and strong materials. Messages were delivered from multiple sources in terms of educational sessions (e.g., taste tests, workplace demonstrations), materials (e.g., posters, flyers, shelf labels), media channels (e.g., print, television, radio), and venues (e.g., stores, workplaces, schools), which was critical to reach all community members and reinforce key messages.
The intervention had a small impact on food behaviors, which could be explained by food availability in the stores. Environmental changes in the stores were modest. First, the stores were relatively large in size, so they already carried some healthy foods. Similar store-based interventions in urban low-income communities have had a larger impact on changing the food environment by working with small stores (Gittelsohn, Suratkar, et al., 2010; Song et al., 2009). Second, the remoteness and climate where the study communities were located are fixed factors that significantly affect the food environment, beyond the control of the intervention (Mead, Gittelsohn, Kratzmann, Roache, & Sharma, 2010). Third, the stores were part of large-chain food retailers, and local store managers have some, though limited, decision-making ability about stocking foods. Investigators working in rural communities should build collaborative relationships with the central offices of the retail chain in the planning phase of the project to have a bigger impact on the food environment.
A significant strength of the study was the high retention rate, allowing for a representative assessment of intervention impact. In addition, the regression models were able to account for a modest amount of the variance (up to 41%), which is consistent with other studies (Backman, Haddad, Lee, Johnston, & Hodgkin, 2002; Gittelsohn et al., 2006; Ho et al., 2008; Robinson & Smith, 2002). Significant strengths of the intervention included the use of community-based participatory techniques during the development of the intervention to enhance cultural appropriateness; the use of the social ecological model to target multilevel determinants of diet in the communities; and implementation in all the food stores in the community to maximize exposure (Sharma et al., 2010).
Additional improvements in the food-related behaviors may have been seen with a longer implementation phase of the 12-month intervention. However, the intervention was designed as a pilot to identify components and strategies to further refine and disseminate the program to government partners. The evaluation design would have been strengthened by additional follow-up assessments (e.g., at 6 months or 1 year). Despite these limitations in duration and follow-up, the intervention had a significant positive impact on the psychosocial variables, which are well-established predictors of food consumption and nutrient intake (Glanz, Kristal, Tilley, & Hirst, 1998; Watters & Satia, 2009). The lack of significant changes in food knowledge and preparation scores may have been because of their low reliability scores and requires further measure refinement in this population. The small number of men in the sample limits generalizability to male Inuit and Inuvialuit in the study regions. However, the study selected the main food preparer/shopper in each household, who were largely women.
Results of this study of the impact of the HFN nutritional and physical activity program on food-related psychosocial factors and behaviors suggest the effectiveness of a culturally appropriate program with multi-institutional partnerships, community engagement, multilevel approaches, and capacity building on reducing risk of chronic disease and improving dietary adequacy among Inuit and Inuvialuit in the remote regions of Arctic Canada. Sustained, well-implemented, and well-evaluated program activities are needed to produce long-term dietary behavior change and to ensure informed policy and program decision making, particularly concerning equitable and informed allocation of resources.
Footnotes
Acknowledgements
We are very grateful to the local staff and the communities for their participation as well as the Aurora Research Institute for their support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
The project was supported by American Diabetes Association Clinical Research award 1-08-CR-57, the Government of Nunavut Department of Health and Social Services, the Government of the Northwest Territories Department of Health and Social Services, and Health Canada.