
Abstract
Research suggests that testimonials, or first-person narratives, influence health behavior and health-related decision making, but few studies have examined conceptual factors that may be responsible for these effects. In the current study, older adults who were due for colorectal cancer screening read a message about screening that included a testimonial from a similar other who had previously made the screening decision. We assessed participants’ identification with the testimonial character and the degree to which they found the message to be vivid. We explored associations between these factors and participants’ knowledge following the message, mood, certainty about screening, and their behavioral intentions to look for more information about screening and to have a test in the next year. In bivariate analyses, identification and vividness were both significantly, positively associated with knowledge and behavioral intentions to have screening in the next year. However, multivariate analyses revealed that only vividness remained significantly associated with knowledge and intentions to be screened.
A testimonial is an account of an individual’s personal experience provided from the first-person perspective (Winterbottom, Bekker, Conner, & Mooney, 2008). Testimonials have also been called first-person narratives (Winterbottom et al., 2008), narratives (Green & Brock, 2000), exemplars (Brosius, 1999), anecdotal evidence (Slater & Rouner, 1996) and case histories (Sherer & Rogers, 1984). Testimonials have been used in a handful of studies to communicate risk and to persuade individuals to engage in particular health behaviors. For example, in one study, Rothman, Kelly, Weinstein, and O’Leary (1999) used testimonials to increase students’ perceived vulnerability to HIV, which was associated with HIV testing 1 month later. To encourage colorectal cancer screening, Lipkus, Green, and Marcus (2003) presented testimonials to older adults who had not been screened. The testimonials, which were from cancer patients, increased perceptions of the severity of colon cancer, which was associated with having a screening test 6 months later. Recently, Dillard, Fagerlin, Dal Cin, Zikmund-Fisher, and Ubel (2010) increased older adults’ intentions to have a colon cancer screening test by giving them testimonials that reduced negative emotions associated with screening such as the anticipated pain.
Testimonials have also been used to help individuals make informed decisions about medication or other treatment. In these medical decision making–interventions, patient testimonials are one of a number of tools to encourage an informed decision-making process. Testimonials are common in these interventions as it has been estimated that up to three quarters of all decision aids include them (Feldman-Stewart et al., 2006). Their use has been controversial with some researchers arguing they bias rather than inform decision making (e.g., Butow, Fowler, & Ziebland, 2005; for reviews, see Khangura, Bennett, Stacey, & O’Connor, 2008, Winterbottom et al., 2008). Ubel, Jepson, and Baron (2001) provided some evidence of this bias. They asked participants to imagine that they had heart disease and they had to decide whether to have bypass surgery. They provided both statistical information and testimonials from similar others to help with their decision. Despite not providing any new information, the testimonials changed participants’ decisions (also see Fagerlin, Wang, & Ubel, 2005).
Although much of the above research has found that exposure to testimonials tends to be associated with planning to take or taking preventive action and treatment preferences or decisions, little is known about why testimonials have these effects. In other words, what specific factors within testimonials may make them so influential? Older reviews of possible mediators and moderators of testimonials such as source credibility, vividness, and information format (e.g., narrative vs. statistical) have found few consistent patterns (e.g., Allen & Preiss, 1997; Reinard, 1988; Taylor & Thompson, 1982). For example, some studies may show a strong effect of a characteristic such as vividness whereas other studies find null effects of this characteristic (Thompson & Taylor, 1982). Winterbottom et al. (2008) recently argued the current state of research “. . . highlight[s] the need for more robust studies to examine narratives, their impact on judgments and decision making, and the associated moderating and/or mediating mechanisms” (p. 2081). Because testimonials from study to study often differ by content and other attributes such as source or length, it is particularly important to examine factors that may be common to them and their associations with message outcomes such as knowledge and behavior intentions.
One factor that may be important to the effects of testimonials is identification with a character, which has its roots in social cognitive theory (Bandura, 1986). According to this theory, people gain confidence in their ability to perform a new behavior when they observe another individual perform the behavior successfully. People will be likely to model this behavior if they identify with the individual. Bandura (2002) defined identification as relating to how much an individual perceives similarity between themselves and a character they observe. Although researchers have defined identification in different ways (e.g., liking a character or wanting to be like a character; see Murphy, Frank, Moran, & Patnoe-Woodley, 2011 for a review), most definitions emphasize perceived similarity. Experiments that test identification have often operationalized the concept in terms of perceived similarity. In one experiment, for example, Fox and Bailenson (2009) manipulated identification by creating virtual models that were either very similar or dissimilar to participants. They found that participants were more likely to model the virtual model’s behavior when it was a similar rather than dissimilar other. Other experiments examining identification have manipulated perceived similarity to a character, finding the former to be more likely to produce intentions to change behavior (e.g., Andsager, Bemker, Choi, & Torwel, 2006).
Recently, Dal Cin, Gibson, Zanna, Shumate, and Fong (2007) conceptualized identification as the extent to which individuals felt they shared the same thoughts and feelings that a character they were exposed to was experiencing. Their operationalization of identification went beyond perceived similarity. They asked about identification explicitly and also conceptualized the construct on a deeper level, as cognitive and emotional perspective taking (e.g., Cohen, 2001, 2006). Like others testing identification with perceived similarity (e.g., Andsager et al., 2006), they also found that greater levels of identification were associated with more behavior change. Given that testimonials provide a vicarious experience and often come from a similar other, they may lead an individual to identify with a character which then subsequently affects the individual’s behavior or intentions to behave (see Hinyard & Kreuter, 2007). In the present study, older participants read a health message about colon cancer that included a testimonial from a similar other. Using Dal Cin et al.’s (2007) comprehensive measure of identification, we examined associations between this factor and message outcomes of knowledge about colon cancer and plans to have a screening test.
In addition to identification, testimonials may also influence knowledge and behavior by increasing the vividness of a message. Nisbett and Ross (1980) argued that vivid information is “likely to attract and hold our attention . . .” (p. 45), and conceptualized vividness as emotionally interesting, concrete or imagery provoking, and proximate. Unfortunately, unlike identification, the concept of vividness has been mostly atheoretical. In their review of the literature, Taylor and Thompson (1982) claimed that the vividness hypothesis—that vivid information is more persuasive and influential than abstract information—has been more self-evident (i.e., based on assumption and intuition) than empirically driven. They argued that instead of defining and validating the construct, researchers have, for the most part, assumed that particular types of information (e.g., detailed information, pictures or videos, or case histories) are vivid rather than actually testing their vividness. This research has compared this assumed vivid information with abstract information to examine its effects on knowledge and behavior.
Of studies comparing abstract information with vivid information, the vivid information appears to have a greater influence on behavior and in some cases knowledge. For example, in one study, researchers gave individuals either abstract information about osteoporosis or a case history of a woman who experienced osteoporosis (i.e., labeled as a more vivid account). The latter was rated more persuasive and had a stronger effect on behavioral intentions to reduce the risk of osteoporosis (Rook, 1986, 1987). Researchers have found similar results regarding information about polio (Wilson, Mills, Norman, & Tomlinson, 2005). Vividness has also been found to relate to greater knowledge following a health message (e.g., Sherer & Rogers, 1984) and others have hypothesized (but not always found) an information recall effect of vividness (Taylor & Thompson, 1982).
Like identification, vividness may also be connected to perceived similarity. In a study by Sherer and Rogers, (1984), researchers had problem drinkers read about either a similar other or a dissimilar other. Those who read about the similar other rated the message as more vivid (i.e., specifically emotionally interesting). Vividness in turn was associated with greater intentions to limit alcohol use.
In summary, both identification with a character and vividness of information may be important to testimonials’ downstream effects on knowledge and behavior following a health message. Although no studies to date have examined both factors in a single study, this examination is important because of their conceptual overlap: Previous research has connected them both to perceived similarity. Theoretically, identification has been defined as perceived similarity, but very little is known about the concept of vividness. Although one study has correlated vividness with similarity, most studies on vividness have been concerned with testing its effects rather than attempting to define it or connect it to related constructs. In an effort to understand these two constructs, the present study also examines their associations with perceived similarity.
In the present study, older adults were reading a health message about colon cancer and screening for this cancer. Within the message, individuals were exposed to a testimonial from a similar other, and we examined the degree to which participants’ reported identification with the testimonial character and their perceived vividness of the message. We examined associations between these two factors and participants’ perceived similarity to the character, knowledge, and behavioral intentions related to screening.
Method
Overview and Hypotheses
Older adult individuals who were due for colorectal cancer screening read an educational message about screening for the disease. Within the message, a testimonial was presented from a similar-age, -race, and -sex individual who had recently decided about screening. Following the message, participants reported their identification with the testimonial and rated the vividness of the information they read. They also reported their behavioral intentions to look for more information about screening, talk to their doctor about it, and have a test in the next year. They then completed knowledge questions, reported their certainty about the decision to screen, and their current mood.
Based on previous research, we hypothesized that both identification with the testimonial character and perceived vividness of the information would be significantly associated with perceived similarity of the testimonial character. Given its theoretical framework (i.e., social cognitive theory; Bandura, 1986), we expected that identification may be more strongly related to similarity than vividness. Based on previous research described above (e.g., Dal Cin et al., 2007; Wilson et al., 2005), we also hypothesized that both greater identification and greater vividness would be associated with greater intentions to seek more information about screening and to have a screening test in the future. Although both have been associated with health behavior and intentions in previous work, they have not been compared before. Finally, consistent with one previous finding (Sherer & Rogers, 1984), we hypothesized that greater vividness may also be associated with higher knowledge scores but we were uncertain about how identification would relate to this variable. In addition to these hypotheses, we explored associations between identification and vividness and decision certainty and mood. We explored these variables simply to gain more insight into the constructs of identification and vividness.
To examine these hypotheses, we first examined bivariate correlations between identification, vividness, and the primary outcomes. To examine their independent associations with outcomes, which would provide insight into the two factors’ relative importance to the different outcomes, we then examined them in multivariate analyses.
Procedure
The data presented in this article were collected as part of a study to examine the effects of different types of testimonials within a colon cancer screening message. The study varied two factors of testimonials for which there were no significant effects. 1 Nonetheless, all analyses reported in the current article control for these factors.
Participants were recruited from Survey Sampling International (SSI), a survey research company that maintains a demographically diverse pool of more than 1 million individuals recruited via Internet banner advertisements and online digit dialing. All SSI members complete a demographic questionnaire, which enables use of a stratified random sampling process that ensures demographic diversity with regard to gender, age, race, and ethnicity (for more information, see www.surveysampling.com).
American individuals between the ages of 49 and 60 years were invited to participate via e-mails sent by SSI. The age range is consistent with current screening guidelines (Levin et al., 2008), and includes individuals who may be starting to consider screening as well as those who may take more time before considering screening. The e-mail invitations included a link to the survey website and when individuals came to the website, they completed one eligibility question, “Have you ever had any of the following screening tests for colorectal cancer?” Five possible colorectal cancer screening tests were listed. Because prior screening could influence how participants responded to the message, only individuals who reported “No” were allowed to participate in the study.
Before viewing the screening message, participants reported their demographic characteristics including their age, race, and sex. The testimonial that participants read in the screening message was matched to these self-reported characteristics. Following the message, participants reported their identification with the testimonial character and they rated the vividness of the message. They also reported their behavioral intentions to seek more information about screening and have a test in the next year, completed a knowledge test of information they had read, reported their certainty about the decision to have screening and their current mood. After completing the measures, participants were debriefed. In exchange for their participation, they were entered into a drawing for modest cash prizes.
Measures
Identification with the testimonial
Four statements assessed participants’ identification with the character in the testimonial (from Dal Cin et al., 2007; Dal Cin, Zanna, & Fong, 2004). On a 7-point scale (from not at all to very much), participants indicated their agreement with, “I found that I could easily take the perspective of the person I read about,” “I found myself thinking what {he, she} might have been thinking,” “I found myself feeling what {he, she} might have been feeling,” and “I easily identified with this person.” We averaged the four items (α = .95).
Vividness of message
To assess vividness of the screening message, we asked participants five questions. Our definition of vividness was based on Nisbett and Ross’s (1980) conceptualization of vivid information as emotionally interesting, imagery provoking, and proximal. To measure the component of imagery, we used questions from the Narrative Transportation Scale (Green & Brock, 2000), which is a measure of cognitive engagement in a story, experience of mental imagery, and emotional reactions. We used three items from this scale that related specifically to mental imagery: “While you were reading information about Colonoscopy, to what extent could you picture yourself having one?” “To what extent did you have vivid images of colonoscopy including the preparation and the test procedure?” and “To what extent could you easily imagine the preparation and the test procedure?” Responses were on a 7-point scale from not at all to very much. To assess the components of interest and proximity, we asked participants the questions, “In your opinion, how interesting was the information we gave you in this study?” and “How personally relevant (related to you and your health) did the information we presented feel?” Responses were on a 7-point scales from not at all to extremely. The five items were averaged (α = .88).
Perceived similarity
A one-item measure was used to assess perceived similarity to the testimonial individual. We asked participants, “How closely did this person’s thoughts resemble your own thinking about colon cancer screening?” Participants responded on a 9-point scale from “{His, Her} thoughts were not at all similar to my own” to “{His, Her} thoughts were extremely similar to my own.”
Screening behavioral intentions
Prior to assessing screening behavioral intentions, participants read, “As you answer these questions, you may start to think about the cost of a screening test. However, we would like you to answer the questions as if there were NO out-of-pocket costs to you associated with getting screened.” Three questions then assessed their behavioral intentions: “Given what you know right now, how interested are you in getting a Colonoscopy?” “How interested are you in looking for more information about Colonoscopy (for example, by using the Internet or talking to others)?” and “How interested are you in talking to your doctor about Colonoscopy?” Responses were on a 7-point scales from not at all interested to extremely interested.
Knowledge
To assess knowledge of information presented in the message about both colon cancer and colonoscopy, we asked nine questions, including multiple choice and true/false items. These questions were developed based on the factual information presented in the message. For example, we asked participants, “Which of the following has
Certainty
We used three items from Lipkus et al. (2003) to assess certainty about screening. The items were, “I have mixed feelings about whether I should get screened for colon cancer,” “I feel torn over getting screened for colon cancer,” and “I have conflicting thoughts about screening.” Participants indicated their agreement on a 6-point scales from strongly disagree to strongly agree. We reverse coded the items so higher numbers represented greater certainty. The three items were averaged (α = .92).
Mood
We asked participants to “Please indicate the extent to which you are experiencing the following emotions: happy, joyful, fun/enjoyment, depressed/blue, unhappy, frustrated, angry/hostile, and worried/anxious” (Diener & Iran-Nejad, 1986). For each item, they responded on a 7-point scale, from not at all (0) to extremely (6). To create positive and negative affect scores, the three positive emotions and the five negative emotions were averaged (α = .96 and α = .91, respectively).
Materials
The screening message and testimonial
The screening message that participants read was adapted, with permission, from the National Cancer Institute online booklet, “What You Need to Know about Cancer of the Colon and Rectum.” The message gave a general description of colon cancer and different screening methods, and then elaborated on colonoscopy. It included topics such as “What is colon cancer?” “Protecting yourself: Screening,” and “Who should get screened?”
Within the message, participants read a testimonial from an individual who recently made the screening decision. The testimonial content was divided into three parts, presented in three places in the screening message. A photo that matched participants’ self-reported age, race, and sex characteristics accompanied the testimonial. The photos were used, with permission, from the University of Michigan’s Center for Health Communications Research. They maintain an online database of photographs of males and females of various ages and races.
Different testimonial content appeared in three places in the screening message and placement was decided based on where this content would best correspond to message content. For example, in the beginning of the message, participants learned that the study would inform them about colon cancer and screening. On this website page, participants were first introduced to the individual in the testimonial who discussed feeling uncertain about screening and knowing little about the different tests. On the next website page, the message provided information about the different types of screening tests. On the following page, participants again saw the testimonial individual, who talked about the way he or she made the decision including some of the barriers he or she had thought about (e.g., inconvenience of the procedure including having to take the laxative) in considering whether to have a test. On the following page, participants were encouraged to think more about screening because of their age. They were also told that they should think about the advantages and disadvantages of screening, including talking about them with their physician so that they could ultimately make the best decision for themselves. Participants then saw the testimonial for the third and final time in which the individual reported having made the decision to have screening and believing the benefits had been worth the risks.
Results
Participants
A total of 1,297 individuals completed measures at baseline. Of these participants, 670 were female and the average age was 53 years (SD = 3.4). The majority of participants were White (85%; mostly non-Hispanic, 91%), followed by Black (9%), Asian (3%), and other (3%). Thirty-one participants (3%) dropped out of the study prior to completing the majority of outcome measures leaving a total of 1,266 participants.
Analytic Strategy
We first examined bivariate correlations between identification with the testimonial, perceived vividness of the information, perceived similarity, behavioral intentions, knowledge, decision certainty, and mood. We next examined identification and vividness in multivariate analyses in which we could test their independent associations with outcomes. For the multivariate analyses, we conducted hierarchical regressions in which original experimental factors were entered in Step 1, demographic variables (e.g., age, race, and gender) were entered in Step 2, and identification and perceived vividness were entered together in Step 3.
Descriptives
Table 1 presents the means and standard deviations for all measures. The mean for perceived vividness of the information was somewhat higher than the mean for identification with the testimonial suggesting that participants were slightly more likely to find the message vivid than to identify with the testimonial character. Overall, participants were reporting moderate intentions to have a screening test in the next year, talk to their physician about screening, and look for more information. They scored better than chance on the knowledge questions and were reporting more positive than negative moods.
Means and Standard Deviations for Primary Measures
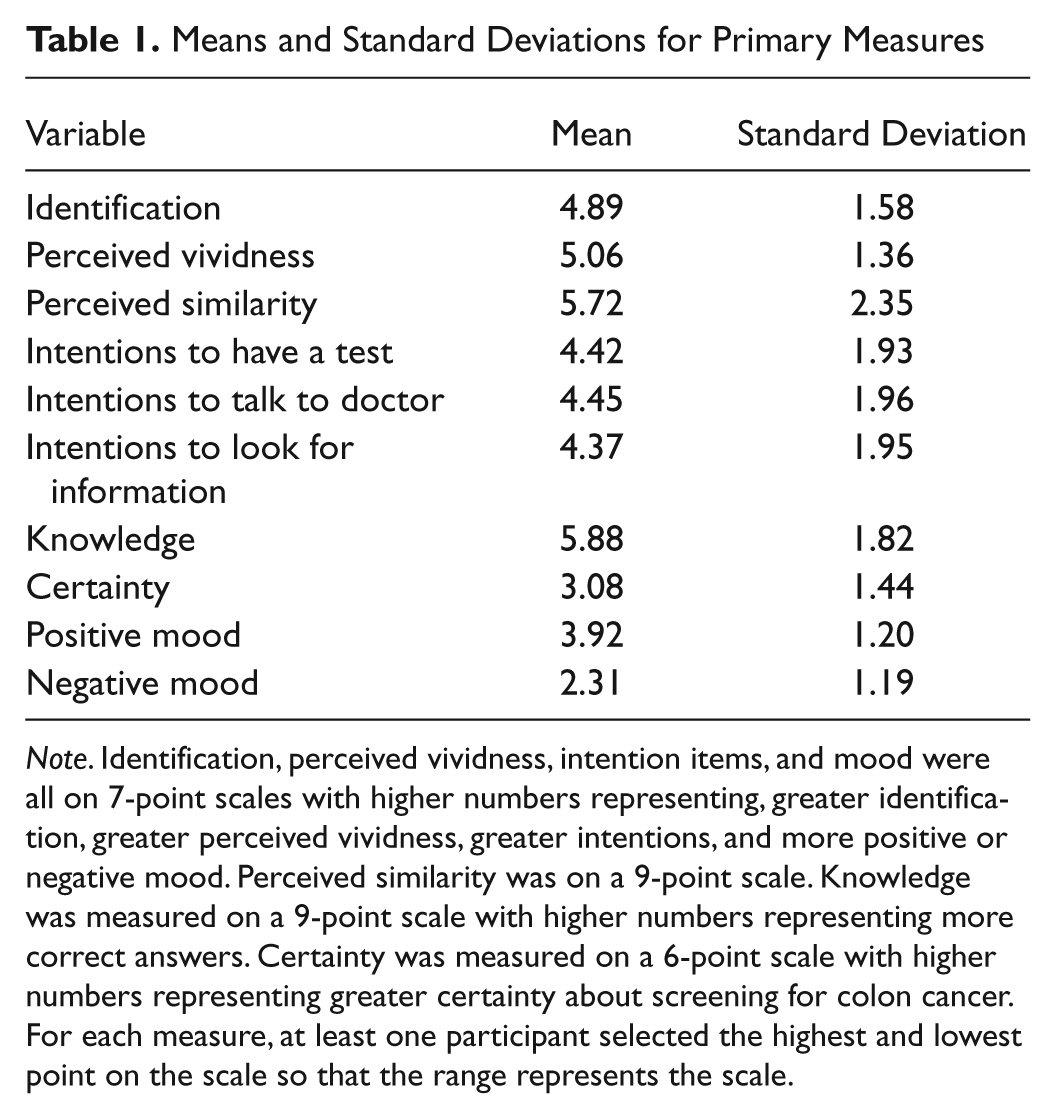
Note. Identification, perceived vividness, intention items, and mood were all on 7-point scales with higher numbers representing, greater identification, greater perceived vividness, greater intentions, and more positive or negative mood. Perceived similarity was on a 9-point scale. Knowledge was measured on a 9-point scale with higher numbers representing more correct answers. Certainty was measured on a 6-point scale with higher numbers representing greater certainty about screening for colon cancer. For each measure, at least one participant selected the highest and lowest point on the scale so that the range represents the scale.
We recorded time spent on each website page. Participants spent less time on testimonial pages compared with the informational pages. On the first, second, and third testimonial pages, participants spent an average of 24, 31, and 19 seconds, respectively, while across the six informational pages, the range was 31 to 55 seconds. These differences likely relate to differences in the amount of content as informational pages were somewhat longer in length than testimonial pages.
Recall that participants received a testimonial that was matched to their gender and ethnicity/race characteristics reported at baseline. We conducted analysis of variance (ANOVAs) to examine whether gender, race, or ethnicity was associated with perceived similarity of the testimonial character. Results showed that perceived similarity of the testimonial did not differ for males and females, F < 1. However, Whites (n = 1,094) were less likely than non-Whites (n = 187) to rate the testimonial character as similar to themselves, Ms = 5.65 (SD = 2.34) vs. 6.13 (SD = 2.33), respectively, F = 6.82, p < .01.
Primary Analyses
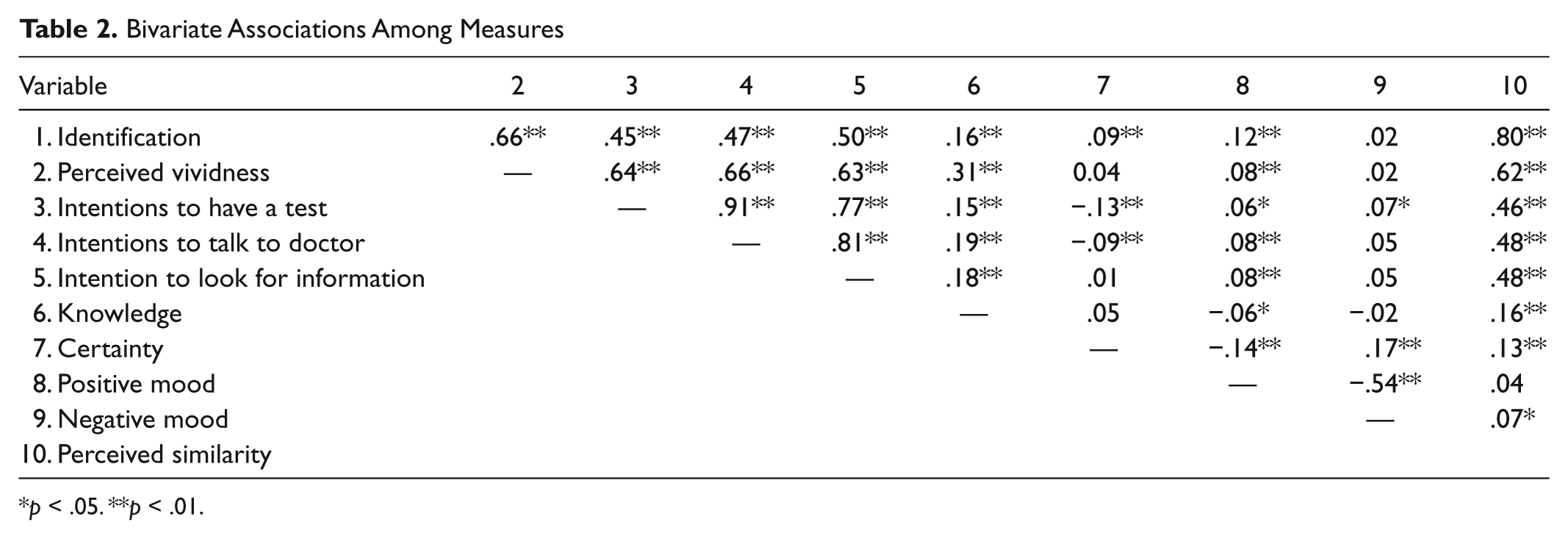
Table 2 presents the correlations among the measures. Several variables showed significant associations, but for the purpose of this article, we focus on the associations with identification and vividness. Identification and vividness were significantly, positively correlated (r = .66, p < .01), and both were significantly, positively correlated with perceived similarity. Both were also significantly associated with behavioral intentions related to screening. As hypothesized, the correlations showed that as identification and perceived vividness increased, participants had greater intentions to have a test in the next year, to talk with their doctor about screening, and to look for more information about it.
Bivariate Associations Among Measures
p < .05. **p < .01.
Both identification and vividness showed significant associations with participants’ knowledge following the message, suggesting that as perceptions of identification and vividness increased, participants learned more. Identification was also significantly associated with certainty about screening such that participants reporting greater identification reported greater certainty about screening. Vividness was not associated with certainty. Participants who perceived greater identification and vividness were also more likely to be reporting a positive mood but neither was associated with negative mood.
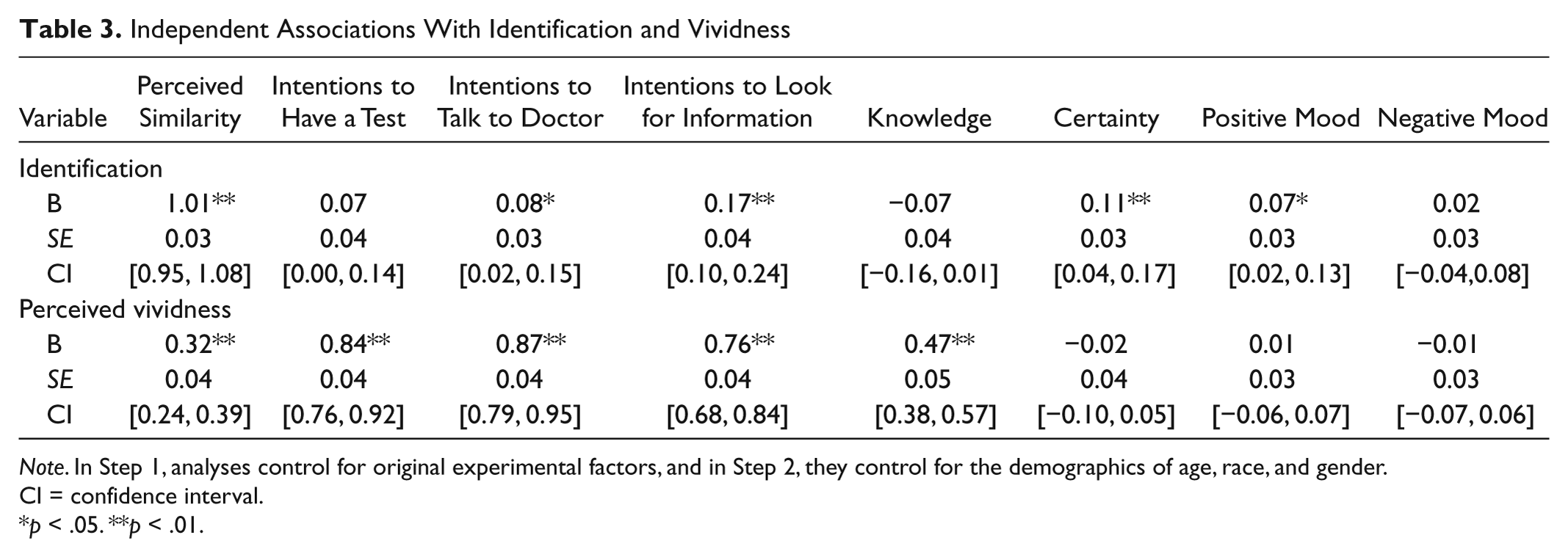
We next examined identification and vividness in hierarchical regressions in which we could test each factor’s unique associations with perceived similarity, behavioral intentions, knowledge, certainty, and mood. Controlling for original experimental factors in Step 1 and demographic variables in Step 2, identification and vividness were entered together in Step 3. Table 3 presents the coefficients for these regression analyses. Findings showed that both identification and vividness were significantly associated with perceived similarity, d = 1.20 and d = 0.33, respectively. Identification and vividness were also significantly associated with intentions to talk to their doctor about screening, d = 0.10 and d = 0.87, respectively, as well as intentions to look for more information about it, d = 0.19 and d = 0.73, respectively. However, only vividness was significantly associated with intentions to have a test in the next year, d = 0.82 with identification now marginally significant, d = 0.08. Vividness was also significantly positively associated with knowledge, d = 0.39, whereas identification was now marginally negatively associated with these scores, d = −0.07. Identification was significantly positively associated with certainty about the decision to have screening, d = 0.12, with vividness still not related to this variable. Identification was also significantly associated with a more positive mood, d = 0.10 whereas vividness was no longer significantly associated with mood.
Independent Associations With Identification and Vividness
Note. In Step 1, analyses control for original experimental factors, and in Step 2, they control for the demographics of age, race, and gender. CI = confidence interval.
p < .05. **p < .01.
Discussion
Testimonials have been found to influence decisions to engage in preventive behaviors, but it is unclear how specific factors of testimonials may relate to these effects. In the present study, individuals who had never been screened for colon cancer read a message about screening that included a testimonial from a similar other. We examined participants’ identification with the testimonial character and their perceived vividness of the information. Although both factors showed significant associations with behavioral intentions to seek more information about screening and have a screening test in the future, multivariate analyses showed that compared with identification, vividness had much stronger associations with these outcomes. Additionally, vividness was significantly, positively associated with knowledge following the message whereas identification was not associated with this outcome.
In addition to behavioral intentions and knowledge, we also examined associations with perceived similarity. Both the concepts of identification and vividness have been connected to perceived similarity in previous research. Identification has often been defined and operationalized in terms of perceived similarity (e.g., Bandura, 1986, 2002; Fox & Bailenson, 2009) and vividness has been significantly associated with it (Sherer & Rogers, 1984). Our findings showed that although both identification and vividness were significantly associated with perceived similarity, identification had the stronger connection. The finding supports social cognitive theory (Bandura, 2002) which views perceived similarity as a large part of identification. Of note, the bivariate associations between the one-item perceived similarity measure and behavioral intentions were as strong as those between identification and intentions. The findings suggest that research that has defined identification solely in terms of perceived similarity may not be all that different from research defining identification on a deeper level, at least in terms of effects on behavior. Regarding the association between vividness and perceived similarity, they continued to be significantly associated even after controlling for the strong effects of identification. The finding contributes to the limited empirical literature on what makes a message vivid—perceived similarity matters for vividness.
One question stemming from the present study’s findings is, after accounting for the shared association between identification and vividness, why was vividness more strongly associated with behavioral intentions? Although there is more theoretical support for identification to be associated with behavior and intentions, speculation about vividness can be offered to explain the strong association. Nisbett and Ross (1980) cited vividness as one of the many sources of the availability bias, a bias that leads to us to make judgments and decisions based not on probability but on the ease with which examples come to mind (Tversky & Kahneman, 1973). They argued that vividness leads to more readily available examples. In the present study, those who perceived the information to be more vivid may have had the screening message and testimonial more accessible in their minds as they were completing intentions items.
In the present study, identification and vividness showed differential associations with knowledge and mood. In multivariate analyses, viewing the message as vivid was associated with greater knowledge but not mood, whereas identification was marginally related to less knowledge but a more positive mood. Based on these associations, one could speculate that identification and vividness influence behavior via different mechanisms. According to the elaboration likelihood model (Petty & Cacioppo, 1986), there is a central route to behavior change associated with thinking deeply and analytically about information or a peripheral route to change associated with superficial influences such as mood. Given the pattern of associations, one possibility is that vividness encourages an elaborative process whereas identification promotes a more peripheral process. However, because the associations with identification were small, this is just speculative. A future experimental study should vary both identification and vividness and then examine effects on not only processing styles through measures of knowledge but also processing variables such as attention and argument scrutiny.
Another theory that could provide insight into the findings related to knowledge and intentions is narrative transportation theory (Green & Brock, 2000). According to this theory, “narrative transportation” is a state that one seeks when presented with a narrative and it occurs when an individual becomes completely engaged in a story (Green & Brock, 2000; Green, Brock, & Kaufman, 2004). Both identification and vividness are viewed as part of the process of narrative transportation. For example, the theory posits that an individual who is transported feels as if the narrative is a real experience (vividness) and strongly identifies with the character (identification). Theoretically, transportation leads to less scrutiny of the contents of the narrative but it is not necessarily a peripheral process (Green & Brock, 2000). Instead, narrative transportation is about becoming emerged in a text, focused on the narrative itself, rather than focused on its argument (i.e., central) or influenced by irrelevant cues (i.e., peripheral). Ultimately, narrative transportation will lead to belief and behavior change that is consistent with the narrative’s message (Green, 2004; Green & Brock, 2000; Green et al., 2004; Hinyard & Kreuter, 2007). In the present investigation, we were interested in the independent effects of identification and vividness. However, narrative transportation speaks to their interactive effects as well as other constructs (e.g., attention, cognitive ability) that may be at play when people are reading narratives. Future studies should consider narrative transportation theory as a framework for interpreting these interactive effects as well as developing different measures of knowledge.
The present study is the first to examine both identification and vividness in a single study. Most research on vividness has not examined the concept independently of other qualities that could also influence responses to a health message. Our findings show that identification is one of those qualities that relate to vividness and future research should examine other qualities. For example, how might audience characteristics such as age influence the association between vividness and behavior intentions (Rook, 1986)? At a fundamental level, more basic research needs to be conducted on vividness. As mentioned earlier, most research on vividness has compared assumed vivid information with abstract information (Taylor & Thompson, 1982), but what makes information vivid? We used Nisbett and Ross’s (1980) conceptualization of vividness which includes three components: emotional interest, detailed information, and proximity. It is possible that one of these components may be more important than the others in influencing knowledge and behavioral intentions. Finally, as discussed above, more research should be done to examine why vividness motivates behavioral intentions? We found that it increases knowledge, but there has been only mixed support for this idea (e.g., Sherer & Rogers, 1984 vs. Rook, 1986). A related question is how long might vividness affect behavior? Some research suggests that the effects are not stable (Rook, 1986), but in that study vividness was again assumed, not assessed. All these questions for future research will lend insight into the concept of vividness, which research (including the present study) shows, will be an important characteristic of health messages that aim to influence behavior.
The present findings have implications for risk communication and health behavior interventions. Health messages that include testimonials are becoming more widespread as a way to communicate information about personal risk and promote behavior change, but little is known about why. In the present study, we found that compared with identification with a character, vividness of the information was more strongly associated with knowledge and behavioral intentions following the message. These findings suggest that researchers and practitioners who use health messages to influence people’s knowledge and increase their health behaviors should be more concerned with making the messages vivid than including a character with whom the individual identifies with. By making messages vivid, perceived similarity will be captured and thus identification may naturally occur. Of course, it is also possible that perceived similarity drives both vividness and identification.
Our findings also have implications for research on the tailoring of health messages. Tailoring is, “Any combination of information or change strategies intended to reach one specific person, based on characteristics that are unique to that person, related to the outcome of interest, and have been derived from an individual assessment” (Kreuter & Skinner, 2000, p. 1). Compared with nontailored information, tailored information leads to greater attention, understanding, and behavior change (e.g., Kreuter & Holt, 2001; Skinner, Campbell, Rimer, Curry, & Prochaska, 1999; for a meta-analysis see Noar, Benac, & Harris, 2007). Although both identification and vividness may be intrinsic in tailored health messages, our findings would suggest the latter may have more to do with the beneficial effects of tailoring on knowledge and behavior.
The present study was limited in the following ways. First, the study was correlational and thus cannot inform any causal directions. In the future, an experimental study should be conducted that manipulates both identification and vividness to determine the effects on behavioral intentions, knowledge, and mood. Although they have been manipulated in separate experiments (e.g., Fox & Bailenson, 2009; Wilson et al., 2005), in an experiment in which they are both manipulated, researchers can compare them and examine their interactive effects. Experimental studies can also test whether elaborative, peripheral, or narrative transportation types of processing are prompted by vividness or identity. A related limitation is that we did not assess baseline knowledge and intentions related to colon cancer screening. One possibility is that participants who had more knowledge and greater intentions to start may have perceived the message as more vivid. Again, an experimental study could examine change in knowledge and intentions as a result of vividness or identification. A third limitation is that although the identification measure was specific to the testimonial (e.g., “I found myself feeling what {he, she} might have been feeling”), the vividness measure was more general (e.g., “While you were reading information about Colonoscopy, to what extent could you picture yourself having one?”). This difference in specificity of measures could have accounted for some of the larger associations with vividness. Fourth, in the present study, we examined behavioral intentions to screen not actual screening behavior. Although meta-analyses (e.g., Webb & Sheeran, 2006) have shown that intentions are predictive of behavior, prospective research that examines actual future behavior is needed. A final limitation relates to representativeness. The data in this study were collected via an Internet survey meaning participants needed to both have access to a computer and feel sufficiently comfortable to use one to participate in a research study. Given these stipulations, our participants may have been somewhat more educated and/or have had higher socioeconomic statuses than nonparticipants. However, previous studies using SSI panels have replicated results from nationally representative samples (e.g., Lacey, Smith, & Ubel, 2006).
Conclusion
Testimonials have been found to motivate preventive health behaviors and affect medical decisions and preferences. The factors of testimonials that may be most important to these effects have yet to be identified. In the present study, we found that identification with a character and vividness of information had differential associations with behavioral intentions, knowledge, and mood. Compared with identification, vividness was much more important to knowledge and behavioral intentions. Future studies should explore these two factors in experimental paradigms. Given that testimonials are often idiosyncratic to health messages, it is important to examine factors such as identification and vividness that may be common to them so that they are used most effectively in health messages.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This research was supported by a grant from the Foundation for Informed Medical Decision Making.